
In-Hospital Mortality of COVID-19 Patients Treated with High-Flow Nasal Oxygen: Evaluation of Biomarkers and Development of the Novel Risk Score Model CROW-65

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Considerations
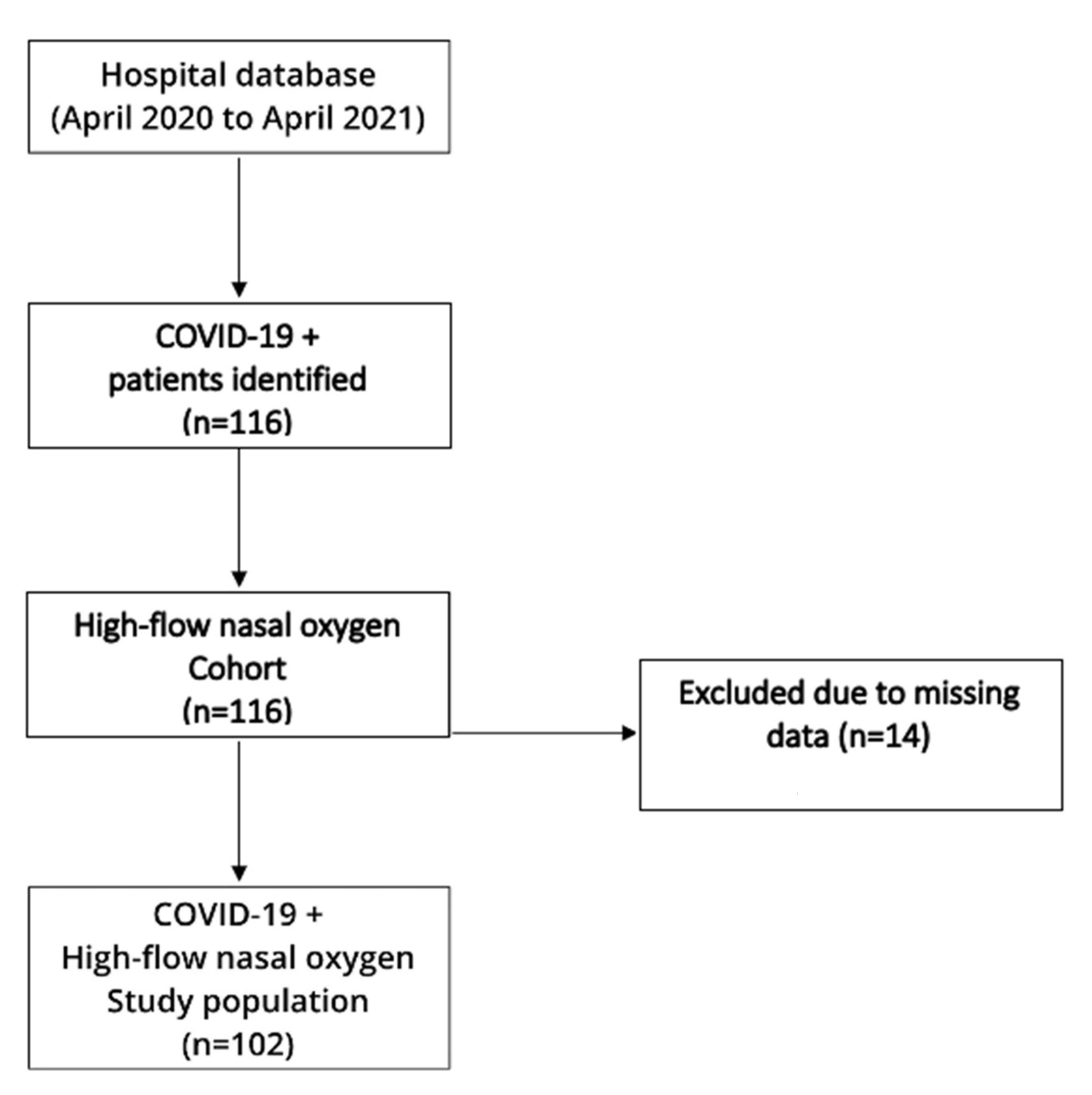
2.2. Subjects and Inclusion/Exclusion Criteria
2.3. Clinical and Laboratory Evaluations
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hajjar, L.A.; Costa, I.B.S.D.S.; Rizk, S.I.; Biselli, B.; Gomes, B.R.; Bittar, C.S.; de Oliveira, G.Q.; de Almeida, J.P.; Bello, M.V.D.O.; Garzillo, C.; et al. Intensive Care Management of Patients with COVID-19: A Practical Approach. Ann. Intensiv. Care 2021, 11, 1–17. [Google Scholar] [CrossRef]
- Cesari, M.; Proietti, M. COVID-19 in Italy: Ageism and Decision Making in a Pandemic. J. Am. Med. Dir. Assoc. 2020, 21, 576–577. [Google Scholar] [CrossRef] [PubMed]
- Solnica, A.; Barski, L.; Jotkowitz, A. Allocation of Scarce Resources during the COVID-19 Pandemic: A Jewish Ethical Perspective. J. Med. Ethic. 2020, 46, 444–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vergano, M.; Bertolini, G.; Giannini, A.; Gristina, G.R.; Livigni, S.; Mistraletti, G.; Riccioni, L.; Petrini, F. Clinical Ethics Recommendations for the Allocation of Intensive Care Treatments in Exceptional, Resource-Limited Circumstances: The Italian Perspective during the COVID-19 Epidemic. Crit. Care 2020, 24, 1–3. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Yang, X.; Huang, C.; Zou, X.; Zhou, T.; Pan, S.; Yang, L.; Wu, Y.; Ouyang, Y.; Wang, Y.; et al. A Novel Risk-Stratification Models of the High-Flow Nasal Cannula Therapy in COVID-19 Patients with Hypoxemic Respiratory Failure. Front. Med. 2020, 7, 607821. [Google Scholar] [CrossRef] [PubMed]
- Klein, A. Who will Get Ventilators in a Covid-19 Crisis? New Sci. 2020, 245, 12. [Google Scholar] [CrossRef]
- Hall, H. The Effect of the COVID-19 Pandemic on Healthcare Workers’ Mental Health. J. Am. Acad. Phys. Assist. 2020, 33, 45–48. [Google Scholar] [CrossRef] [PubMed]
- De Wit, E.; Van Doremalen, N.; Falzarano, D.; Munster, V.J. SARS and MERS: Recent Insights into Emerging Coronaviruses. Nat. Rev. Microbiol. 2016, 14, 523–534. [Google Scholar] [CrossRef] [PubMed]
- Peeri, N.C.; Shrestha, N.; Rahman, M.S.; Zaki, R.; Tan, Z.; Bibi, S.; Baghbanzadeh, M.; Aghamohammadi, N.; Zhang, W.; Haque, U. The SARS, MERS and Novel Coronavirus (COVID-19) Epidemics, the Newest and Biggest Global Health Threats: What Lessons have we Learned? Int. J. Epidemiol. 2020, 49, 717–726. [Google Scholar] [CrossRef] [Green Version]
- Bellani, G.; Laffey, J.G.; Pham, T.; Madotto, F.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; Bumbasirevic, V.; Piquilloud, L.; et al. Noninvasive Ventilation of Patients with Acute Respiratory Distress Syndrome. Insights from the Lung Safe Study. Am. J. Respir. Crit. Care Med. 2017, 195, 67–77. [Google Scholar] [CrossRef] [Green Version]
- Grasselli, G.; Pesenti, A.; Cecconi, M. Critical Care Utilization for the COVID-19 Outbreak in Lombardy, Italy. JAMA 2020, 323, 1545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pisano, A.; Yavorovskiy, A.; Verniero, L.; Landoni, G. Indications for Tracheal Intubation in Patients with Coronavirus Disease 2019 (COVID-19). J. Cardiothorac. Vasc. Anesthesia 2021, 35, 1276–1280. [Google Scholar] [CrossRef] [PubMed]
- Jiang, B.; Yao, W.; Wang, T.; Cook, T.M.; Behringer, E.; Wei, H. Tracheal Intubation in COVID-19 Patients: Update on Recommendations. Br. J. Anaesth. 2020, 125, e424–e426. [Google Scholar] [CrossRef]
- Wong, P.; Lim, W.Y. Aligning Difficult Airway Guidelines with the Anesthetic COVID-19 Guidelines to Develop a COVID-19 Difficult Airway Strategy: A Narrative Review. J. Anesth. 2020, 34, 924–943. [Google Scholar] [CrossRef]
- Siempos, I.I.; Xourgia, E.; Ntaidou, T.K.; Zervakis, D.; Magira, E.E.; Kotanidou, A.; Routsi, C.; Zakynthinos, S.G. Effect of Early vs. Delayed or No Intubation on Clinical Outcomes of Patients With COVID-19: An Observational Study. Front. Med. 2020, 7, 614152. [Google Scholar] [CrossRef]
- Cooper, A.; Joglekar, A.; Adhikari, N. A Practical Approach to Airway Management in Patients with SARS. CMAJ 2003, 169, 785–787. [Google Scholar] [CrossRef] [PubMed]
- Azoulay, E.; For the Efraim Investigators and the Nine-I Study Group; Pickkers, P.; Soares, M.; Perner, A.; Rello, J.; Bauer, P.R.; Van De Louw, A.; Hemelaar, P.; Lemiale, V.; et al. Acute Hypoxemic Respiratory Failure in Immunocompromised Patients: The Efraim Multinational Prospective Cohort Study. Intensiv. Care Med. 2017, 43, 1808–1819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perpiñan, C.; Bertran, L.; Terra, X.; Aguilar, C.; Lopez-Dupla, M.; Alibalic, A.; Riesco, D.; Camaron, J.; Perrone, F.; Rull, A.; et al. Predictive Biomarkers of COVID-19 Severity in SARS-CoV-2 Infected Patients with Obesity and Metabolic Syndrome. J. Pers. Med. 2021, 11, 227. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Mon, M.; Ortega, M.A.; Gasulla, Ó.; Fortuny-Profitós, J.; Mazaira-Font, F.A.; Saurina, P.; Monserrat, J.; Plana, M.N.; Troncoso, D.; Moreno, J.S.; et al. A Predictive Model and Risk Factors for Case Fatality of COVID-19. J. Pers. Med. 2021, 11, 36. [Google Scholar] [CrossRef]
- Ogawa, K.; Asano, K.; Ikeda, J.; Fujii, T. Non-Invasive Oxygenation Strategies for Respiratory Failure with COVID-19: A Concise Narrative Review of Literature in Pre and Mid-COVID-19 Era. Anaesth. Crit. Care Pain Med. 2021, 40, 100897. [Google Scholar] [CrossRef] [PubMed]
- Frat, J.-P.; Thille, A.W.; Mercat, A.; Girault, C.; Ragot, S.; Perbet, S.; Prat, G.; Boulain, T.; Morawiec, E.; Cottereau, A.; et al. High-Flow Oxygen through Nasal Cannula in Acute Hypoxemic Respiratory Failure. N. Engl. J. Med. 2015, 372, 2185–2196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthay, A.M.; Aldrich, J.M.; Gotts, E.J. Treatment for Severe Acute Respiratory Distress Syndrome from COVID-19. Lancet Respir. Med. 2020, 8, 433–434. [Google Scholar] [CrossRef] [Green Version]
- Mellado-Artigas, R.; Ferreyro, B.L.; Angriman, F.; Hernández-Sanz, M.; Arruti, E.; Torres, A.; Villar, J.; Brochard, L.; Ferrando, C. High-Flow Nasal Oxygen in Patients with COVID-19-Associated Acute Respiratory Failure. Crit. Care 2021, 25, 1–10. [Google Scholar] [CrossRef]
- Schmidt, M.; Hajage, D.; Demoule, A.; Pham, T.; Combes, A.; Dres, M.; Lebbah, S.; Kimmoun, A.; Mercat, A.; Beduneau, G.; et al. Clinical Characteristics and Day-90 Outcomes of 4244 Critically Ill Adults with COVID-19: A Prospective Cohort Study. Intensiv. Care Med. 2021, 47, 60–73. [Google Scholar] [CrossRef]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected with SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [Green Version]
- Zucman, N.; Mullaert, J.; Roux, D.; Roca, O.; Ricard, J.-D. Prediction of Outcome of Nasal High Flow Use during COVID-19-Related Acute Hypoxemic Respiratory Failure. Intensiv. Care Med. 2020, 46, 1924–1926. [Google Scholar] [CrossRef]
- Kang, B.J.; Koh, Y.; Lim, C.-M.; Huh, J.W.; Baek, S.; Han, M.; Seo, H.-S.; Suh, H.J.; Seo, G.J.; Kim, E.Y.; et al. Failure of High-Flow Nasal Cannula Therapy may Delay Intubation and Increase Mortality. Intensiv. Care Med. 2015, 41, 623–632. [Google Scholar] [CrossRef]
- Hemalkumar, B.M.; Vinay, M.; Cynthia, J.G.; Deepak, A.; Michael, L.J. Regression Coefficient–Based Scoring System should be Used to Assign Weights to the Risk Index. J. Clin. Epidemiol. 2016, 79, 22–28. [Google Scholar]
- Geng, S.; Mei, Q.; Zhu, C.; Yang, T.; Yang, Y.; Fang, X.; Pan, A. High Flow Nasal Cannula is a Good Treatment Option for COVID-19. Hear. Lung 2020, 49, 444–445. [Google Scholar] [CrossRef]
- Wang, K.; Zhao, W.; Li, J.; Shu, W.; Duan, J. The Experience of High-Flow Nasal Cannula in Hospitalized Patients with 2019 Novel Coronavirus-Infected Pneumonia in Two Hospitals of Chongqing, China. Ann. Intensiv. Care 2020, 10, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Chandel, A.; Patolia, S.; Brown, A.W.; Collins, A.C.; Sahjwani, D.; Khangoora, V.; Cameron, P.C.; Desai, M.; Kasarabada, A.; Kilcullen, J.K.; et al. High-Flow Nasal Cannula Therapy in COVID-19: Using the ROX Index to Predict Success. Respir. Care 2021, 66, 909–919. [Google Scholar] [CrossRef]
- Hu, M.; Zhou, Q.; Zheng, R.; Li, X.; Ling, J.; Chen, Y.; Jia, J.; Xie, C. Application of High-Flow Nasal Cannula in Hypoxemic Patients with COVID-19: A Retrospective Cohort Study. BMC Pulm. Med. 2020, 20, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Goh, K.J.; Chai, H.Z.; Ong, T.H.; Sewa, D.W.; Phua, G.C.; Tan, Q.L. Early prediction of high flow nasal cannula therapy outcomes using a modified ROX index incorporating heart rate. J. Intensive Care 2020, 8, 41. [Google Scholar] [CrossRef]
- Duan, J.; Zeng, J.; Deng, P.; Ni, Z.; Lu, R.; Xia, W.; Jing, G.; Su, X.; Ehrmann, S.; Zhang, W.; et al. High-Flow Nasal Cannula for COVID-19 Patients: A Multicenter Retrospective Study in China. Front. Mol. Biosci. 2021, 8, 639100. [Google Scholar] [CrossRef]
- Fang, F.C.; Schooley, R.T. Treatment of Coronavirus Disease 2019—Evidence-Based or Personalized Medicine? Clin. Infect. Dis. 2020, ciaa996. [Google Scholar] [CrossRef] [PubMed]
- McEnery, T.; Gough, C.; Costello, R.W. COVID-19: Respiratory Support Outside the Intensive Care Unit. Lancet Respir. Med. 2020, 8, 538–539. [Google Scholar] [CrossRef]
- Stéphan, F.; Barrucand, B.; Petit, P.; Rézaiguia-Delclaux, S.; Médard, A.; Delannoy, B.; Cosserant, B.; Flicoteaux, G.; Imbert, A.; Pilorge, C.; et al. High-Flow Nasal Oxygen vs Noninvasive Positive Airway Pressure in Hypoxemic Patients After Cardiothoracic Surgery. JAMA 2015, 313, 2331–2339. [Google Scholar] [CrossRef] [Green Version]
- Frat, J.-P.; Ragot, S.; Girault, C.; Perbet, S.; Prat, G.; Boulain, T.; Demoule, A.; Ricard, J.-D.; Coudroy, R.; Robert, R.; et al. Effect of Non-Invasive Oxygenation Strategies in Immunocompromised Patients with Severe Acute Respiratory Failure: A Posthoc Analysis of a Randomised Trial. Lancet Respir. Med. 2016, 4, 646–652. [Google Scholar] [CrossRef]
- Tu, G.-W.; Liao, Y.-X.; Li, Q.-Y.; Dong, H.; Yang, L.-Y.; Zhang, X.-Y.; Fu, S.-Z.; Wang, R.-L. Prone Positioning in High-Flow Nasal Cannula for COVID-19 Patients with Severe Hypoxemia: A Pilot Study. Ann. Transl. Med. 2020, 8, 598. [Google Scholar] [CrossRef] [PubMed]
- Goury, A.; Moussanang, J.; Bard, M.; Champenois, V.; Julien, G.; Dupont, V.; Mourvillier, B. Predictive Factors Associated with High-Flow Nasal Cannula Success for COVID-19-Related Acute Hypoxemic Respiratory Failure. Health Sci. Rep. 2021, 4, e287. [Google Scholar] [CrossRef]
- Roca, O.; Caralt, B.; Messika, J.; Samper, M.; Sztrymf, B.; Hernández, G.; García-De-Acilu, M.; Frat, J.-P.; Masclans, J.R.; Ricard, J.-D. An Index Combining Respiratory Rate and Oxygenation to Predict Outcome of Nasal High-Flow Therapy. Am. J. Respir. Crit. Care Med. 2019, 199, 1368–1376. [Google Scholar] [CrossRef] [PubMed]
- Roca, O.; Messika, J.; Caralt, B.; de Acilu, M.G.; Sztrymf, B.; Ricard, J.-D.; Masclans, J.R. Predicting Success of High-Flow Nasal Cannula in Pneumonia Patients with Hypoxemic Respiratory Failure: The Utility of the ROX Index. J. Crit. Care 2016, 35, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, R.A.; Jurado, B.A.; Güeto, F.C.; Yuste, A.C.; García, I.D.; Delgado, F.G.; Pérez, J.G.; Obispo, M.L.; Del Río, I.Q.; Espinar, F.R.; et al. Predictors of success of high-flow nasal cannula in the treatment of acute hypoxemic respiratory failure. Med. Intensiva 2021, 45, 80–87. [Google Scholar] [CrossRef]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [Green Version]
- Ng, W.H.; Tipih, T.; Makoah, N.A.; Vermeulen, J.-G.; Goedhals, D.; Sempa, J.B.; Burt, F.J.; Taylor, A.; Mahalingam, S. Comorbidities in SARS-CoV-2 Patients: A Systematic Review and Meta-Analysis. mBio 2021, 12, e03647-20. [Google Scholar] [CrossRef]
- Atkins, J.L.; Masoli, J.A.H.; Delgado, J.; Pilling, L.C.; Kuo, C.-L.; Kuchel, A.G.; Melzer, D. Preexisting Comorbidities Predicting COVID-19 and Mortality in the UK Biobank Community Cohort. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2020, 75, 2224–2230. [Google Scholar] [CrossRef]
- Grau, C.M.; Bofill, C.B.; Picó-Plana, E.; Comí, G.R.; Terrón-Puig, M.; Paz, N.B.; Mateu, M.S.; Fornés, C.G. Use of Predictive Tools in the Management of COVID-19 Patients: A Key Role of Clinical Laboratories. Adv. Lab. Med. Av. En Med. De Lab. 2021, 2, 237–243. [Google Scholar] [CrossRef]
- Yang, A.-P.; Liu, J.-P.; Tao, W.-Q.; Li, H.-M. The Diagnostic and Predictive Role of NLR, d-NLR and PLR in COVID-19 Patients. Int. Immunopharmacol. 2020, 84, 106504. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Death Event | Total (n = 102) | p Value | |
|---|---|---|---|---|
| No (n = 60) | Yes (n = 42) | |||
| Age (years) | 63 (57–72) | 71 (66–77) | 66 (58–73) | <0.001 * |
| Male sex | 40 (66.7%) | 33 (78.6%) | 73 (71.6%) | 0.190 † |
| Disease duration at admission (days) | 9 (8–11) | 10 (7–11) | 9 (8–11) | 0.415 * |
| ROX index | 5.25 ± 1.26 | 2.90 ± 1.00 | 4.27 ± 1.64 | <0.001 ‡ |
| HFNO duration (days) | 9 (5–12) | 5 (4–8) | 7 (4–11) | 0.005 * |
| Disease duration at HFNO interruption (days) | 20 (16–24) | 18 (16–23) | 19 (16–24) | 0.283 * |
| Corticosteroid therapy (%) | 60 (100.0%) | 42 (100.0%) | 102 (100.0%) | / |
| Remdesivir therapy (%) | 57 (95.0%) | 35 (83.3%) | 92 (90.2%) | 0.051 † |
| Ventilator (%) | 9 (15.5%) | 32 (76.2%) | 41 (40.2%) | <0.001 † |
| Comorbidities | ||||
| Active smoking | 32 (53.3%) | 21 (50.0%) | 53 (52.0%) | 0.740 † |
| Obesity | 5 (8.3%) | 4 (9.5%) | 9 (8.8%) | 0.835 † |
| Arterial hypertension | 37 (61.7%) | 28 (66.7%) | 65 (63.7%) | 0.605 † |
| Diabetes mellitus | 19 (31.7%) | 8 (19.0%) | 27 (26.5%) | 0.155 † |
| COPD | 1 (1.7%) | 4 (9.5%) | 5 (4.9%) | 0.070 † |
| CCI | 2.43 ± 1.14 | 3.55 ± 1.95 | 2.89 ± 1.62 | <0.001 ‡ |
| Laboratory parameters | ||||
| SpO2 (%) | 81.95 ± 10.84 | 80.61 ± 11.57 | 81.40 ± 11.11 | 0.552 ‡ |
| pH (units) | 7.44 ± 0.06 | 7.43 ± 0.05 | 7.44 ± 0.06 | 0.694 ‡ |
| pO2 (kPa) | 6.15 ± 1.21 | 6.36 ± 1.31 | 6.23 ± 1.25 | 0.418 ‡ |
| pCO2 (kPa) | 4.35 ± 0.47 | 4.43 ± 0.65 | 4.38 ± 0.55 | 0.437 ‡ |
| HCO3− (mmol/L) | 25.85 ± 2.49 | 25.23 ± 3.31 | 25.60 ± 2.86 | 0.284 ‡ |
| Hemoglobin (g/L) | 140.57 ± 14.96 | 134.26 ± 15.66 | 137.97 ± 15.49 | 0.042 ‡ |
| RDW (%) | 13.99 ± 1.43 | 16.85 ± 18.09 | 15.17 ± 11.66 | 0.226 ‡ |
| Platelets (x109/L) | 236 (171–317) | 253 (165–311) | 250 (169–314) | 0.497 * |
| WBC (x109/L) | 10.78 ± 5.28 | 9.10 ± 4.29 | 10.09 ± 4.94 | 0.090 ‡ |
| Neutrophiles (%) | 81.99 ± 10.63 | 83.57 ± 8.49 | 82.64 ± 9.79 | 0.424 ‡ |
| Lymphocytes (%) | 12.08 ± 9.39 | 10.84 ± 7.69 | 11.57 ± 8.71 | 0.482 ‡ |
| Monocytes (%) | 4.52 ± 1.91 | 4.89 ± 1.96 | 4.67 ± 1.93 | 0.344 ‡ |
| Eosinophiles (%) | 0.29 ± 0.33 | 0.40 ± 0.53 | 0.33 ± 0.42 | 0.221 ‡ |
| CRP (mmol/L) | 152 (82–251) | 128 (90–199) | 146 (85–214) | 0.321 * |
| LDH (umol/L) | 451 (345–676) | 454 (387–614) | 453 (372–659) | 0.240 * |
| D-dimers (mmol/L) | 2 (1–4) | 4 (1–6) | 2 (1–5) | 0.449 * |
| Variables | Death Event | Total (n = 102) | p Value | |
|---|---|---|---|---|
| No (n = 60) | Yes (n = 42) | |||
| NLR ratio | 9 (5–16) | 9 (6–17) | 9 (6–16) | 0.285 * |
| Hemoglobin to RDW ratio | 10.15 ± 1.48 | 9.42 ± 2.01 | 9.85 ± 1.75 | 0.037 † |
| LDH to hemoglobin ratio | 3 (2–5) | 4 (3–5) | 3 (3–5) | 0.118 * |
| Eosinophile to lymphocyte ratio | 0.04 ± 0.06 | 0.10 ± 0.33 | 0.07 ± 0.22 | 0.166 † |
| CRP to lymphocyte ratio | 29.36 ± 4.99 | 42.56 ± 7.33 | 34.79 ± 8.06 | 0.459 † |
| D-dimer to CRP ratio | 0.06 ± 0.19 | 0.05 ± 0.07 | 0.06 ± 0.15 | 0.621 † |
| LDH to WBC ratio | 54.55 ± 5.65 | 79.44 ± 7.36 | 64.80 ± 5.50 | 0.022 † |
| Variables | HR (95% CI) | p Value * |
|---|---|---|
| Age | 1.04 (1.01–1.08) | 0.006 |
| Male sex | 1.50 (0.71–3.14) | 0.285 |
| Disease duration at admission | 1.08 (0.98–1.19) | 0.106 |
| Disease duration at HFNO initiation | 1.03 (0.97–1.10) | 0.324 |
| HFNO duration | 0.89 (0.83–0.96) | 0.003 |
| Remdesivir treatment | 0.53 (0.23–1.19) | 0.122 |
| Ventilator initiation | 5.74 (2.81–11.69) | <0.001 |
| CCI | 1.27 (1.12–1.45) | <0.001 |
| ROX index | 0.46 (0.35–0.60) | <0.001 |
| pO2 | 1.15 (0.90–1.48) | 0.274 |
| pCO2 | 1.32 (0.78–2.23) | 0.305 |
| HCO3− | 0.96 (0.87–1.05) | 0.370 |
| Hemoglobin | 0.98 (0.96–1.01) | 0.080 |
| RDW | 1.01 (0.99–1.03) | 0.108 |
| Platelets | 1.00 (0.99–1.01) | 0.229 |
| WBC | 0.93 (0.87–1.00) | 0.055 |
| Neutrophiles | 0.93 (0.86–1.00) | 0.061 |
| Lymphocytes | 0.74 (0.39–1.41) | 0.359 |
| Monocytes | 0.93 (0.32–2.72) | 0.900 |
| CRP | 1.00 (0.99–1.00) | 0.162 |
| LDH | 0.99 (0.98–1.01) | 0.866 |
| D-dimers | 1.00 (0.97–1.03) | 0.988 |
| Variables | Youden Index | Sensitivity/Specificity | AUC (95% CI) | p Value * |
|---|---|---|---|---|
| Age | ≤65 | 65.0%/76.2% | 0.705 (0.606–0.791) | <0.001 |
| LDH-to-WBC ratio | ≤42.75 | 48.33%/76.19% | 0.633 (0.532–0.726) | 0.017 |
| CCI | ≤3 | 83.3%/40.5% | 0.673 (0.573–0.763) | 0.002 |
| ROX index | >4.12 | 81.4%/92.9% | 0.892 (0.814–0.945) | <0.001 |
| Variables | Score |
|---|---|
| CCI >4 | 3 |
| ROX index ≤ 4.11 | 26 |
| LDH-to-WBC ratio | 7 |
| Age > 65 years | 5 |
| Total | 41 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kljakovic Gaspic, T.; Pavicic Ivelja, M.; Kumric, M.; Matetic, A.; Delic, N.; Vrkic, I.; Bozic, J. In-Hospital Mortality of COVID-19 Patients Treated with High-Flow Nasal Oxygen: Evaluation of Biomarkers and Development of the Novel Risk Score Model CROW-65. Life 2021, 11, 735. https://doi.org/10.3390/life11080735
Kljakovic Gaspic T, Pavicic Ivelja M, Kumric M, Matetic A, Delic N, Vrkic I, Bozic J. In-Hospital Mortality of COVID-19 Patients Treated with High-Flow Nasal Oxygen: Evaluation of Biomarkers and Development of the Novel Risk Score Model CROW-65. Life. 2021; 11(8):735. https://doi.org/10.3390/life11080735
Chicago/Turabian StyleKljakovic Gaspic, Toni, Mirela Pavicic Ivelja, Marko Kumric, Andrija Matetic, Nikola Delic, Ivana Vrkic, and Josko Bozic. 2021. "In-Hospital Mortality of COVID-19 Patients Treated with High-Flow Nasal Oxygen: Evaluation of Biomarkers and Development of the Novel Risk Score Model CROW-65" Life 11, no. 8: 735. https://doi.org/10.3390/life11080735
APA StyleKljakovic Gaspic, T., Pavicic Ivelja, M., Kumric, M., Matetic, A., Delic, N., Vrkic, I., & Bozic, J. (2021). In-Hospital Mortality of COVID-19 Patients Treated with High-Flow Nasal Oxygen: Evaluation of Biomarkers and Development of the Novel Risk Score Model CROW-65. Life, 11(8), 735. https://doi.org/10.3390/life11080735