Abstract
Objectives: To evaluate the feasibility and safety of low energy X-ray photon intraoperative radiotherapy (IORT) as an adjuvant therapy for recurrent gynecological cancer.Methods: Medical records of all recurrence gynecological cancer patients who underwent IORT were reviewed. Results: Between January 2018 and December 2021, five women (including cervical cancer (n = 2), endometrial cancer (n = 2), and uterine leiomyosarcoma (n = 1)), who underwent IORT and surgical resection for recurrent gynecologic cancer were reviewed. A median dose of 15.62 Gy (range, 12 to 20 Gy) was used for IORT. Repeated IORT and surgical resection was performed in two women. Three women experienced local recurrence, and three women died during follow-up. The 1-year local control rate was 60%. The 2-year overall survival rate was 30%. There was no Clavien–Dindo classification grade III–V complication. Conclusion: IORT using low energy X-ray photon therapy seems to be feasible and safe as an adjuvant therapy in women who underwent salvage surgery for recurrent gynecologic cancer. However, large-scale prospective studies are needed to confirm our findings and evaluate its efficacy.
1. Introduction
The management of recurrent cervical and endometrial cancers can be challenging for the gynecologic oncologist. For resectable lesions, surgery is the first-line therapy for cancer recurrence. Post-operative radiation therapy has the role of prevention of local tumor recurrence or local control of the tumor, especially for R1 or R2 resection. However, those patients with tumor recurrence frequently have histories of previous irradiation with either external beam radiation or brachytherapy as their primary frontline treatment or adjuvant treatment in women with cervical cancer or endometrial cancer. Thus, the issue of re-irradiation for the recurrence disease to achieve disease control and avoid surrounding normal structure injury is a problem to be overcome. Intraoperative radiation therapy (IORT) is a special useful technique to deliver high doses to a focused region, especially for recurrent disease within the prior irradiation area. Owing to its nature of direct contact radiation to the tumor [1] and the ability of protection after proper packing, IORT allows maximal tumor control with irradiation and minimizing the radiation exposure of surrounding normal structures [1].
IORT can be delivered via different techniques, including intraoperative electron beam radiotherapy (IOERT) [2,3], high-dose-rate intraoperative brachytherapy (HDR-IORT) [4], and low energy X-ray photon IORT with cone (spherical), balloon, or catheter applicators of variable sizes implanted during the surgery to match the defined tumor bed or region at risk. Each technique has its unique method and suitable indication.
For IOERT, from when it was introduced in the 1960s, patients need to be transported from the operation room to the radiation department [5]. In addition, the mobile linear accelerator machine and the less self-shielding demanded of IOERT provide a more flexible use for intraoperative electron radiotherapy [1,2,3,6,7,8]; however, the cone applicator of IOERT is rigid and might be difficult to fit to the irregular shape or narrow cavity of the tumor bed or region at risk in the pelvic site. Thus, the use of IOERT for the treatment of recurrent gynecological malignancies is limited.
The issue of shielding demanded in the operation room is not solved for HDR-IORT, and the relatively prolonged treatment time is also another problem for HDR-IORT.
The Axxent Electronic Brachytherapy System (Xoft Inc., Fremont, CA, USA) [9,10,11,12] and Intrabeam (Carl Zeiss AG, Jena, Germany) [13] are both commonly used with low energy X-ray photon IORT. The mobile machines and less shielding requirement in the operation room have made them popular in IORT applications. They have different sized balloon (Figure 1A) and cone (Figure 1B) applicators that can be suited for a wide range of target volumes and shapes. They have the advantage of dose distribution with steep dose gradients. The limited dose penetration within 0.5–1 cm can provide safe treatment without excessive surrounding normal tissue damage and can prevent related toxicity.
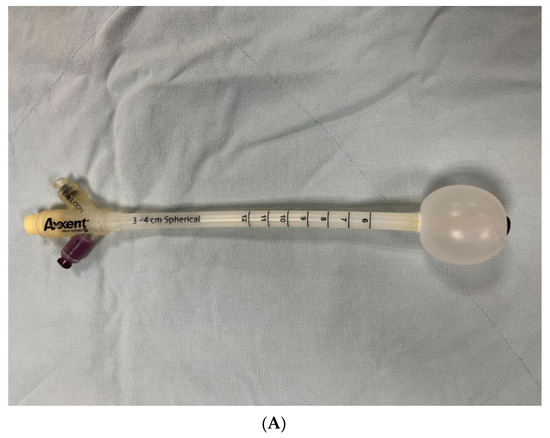
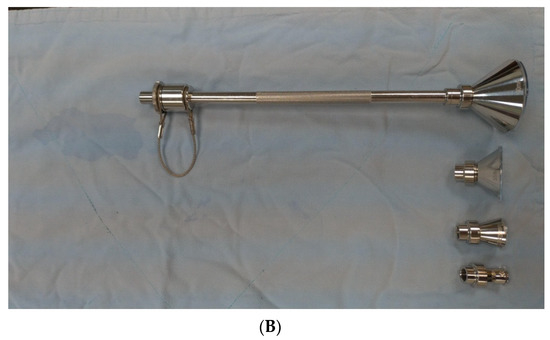
Figure 1.
(A) Balloon and (B) cone applicators.
The Axxent Electronic Brachytherapy System has been used for breast cancer patients [9,10,11,12]. It delivers a single high dose to the focused area and has a limited depth with a low energy 50 kv X-ray to perform effective IORT treatment, reduces exposure to surrounding normal tissue, and minimizes side effects. The Axxent Electronic Brachytherapy System has been used as adjuvant brachytherapy for early stage endometrial cancer in women with a high risk for recurrence [14]. A total of 15 patients with stage I or II endometrial cancer were enrolled. There were only four grade I and 2 grade II brachytherapy-related adverse events. The grade I adverse events included dysuria, vaginal dryness, mucosal atrophy, and rectal bleeding. The grade II adverse events included dysuria and vaginal pain. There were no grade III or IV adverse events. The Axxent Electronic Brachytherapy System seemed to perform well and was associated with limited toxicity [14].
To our knowledge, clinical use of the Axxent Electronic Brachytherapy System in the treatment of recurrent gynecologic cancers has never been reported. Thus, this retrospective study aims to evaluate the feasibility and safety of low energy X-ray photon IORT with the Axxent Electronic Brachytherapy System as an adjuvant therapy in women who have undergone salvage surgery for recurrent gynecologic cancer.
2. Materials and Methods
Medical records of women with recurrence of cervical cancer, endometrial cancer, or uterine leiomyosarcoma, and undergoing salvage surgery and low energy X-ray photon IORT in a tertiary referral hospital, were reviewed. The study was approved by the Research Ethics Review Committee of the hospital (No.110259-E).
IORT with 50 kv X-ray photons (Axxent Electronic Brachytherapy System, Xoft Inc., Fremont, CA, USA) was delivered by variable sized cone or balloon applicators limited to the at-risk region and depth to maximize dose to the target and minimize exposure to the surrounding normal tissues. The commonly used radiation dose of IORT was ranged within 10–20 Gy in a single fraction. The actual delivering dose depended on the treatment site, surrounding tissue/organ tolerance, margin status of gross residual or microscopic residual disease, and the treatment goals of adjuvant, salvage, or palliative settings. The use of cone or balloon applicators depended on the shape of the treatment regions. The cone applicators were for the relatively flat region, and the balloon applicators were for the spherical region. Many different sizes of applicators can be used for different treatment volumes. The aim was to match the tumor bed or region at risk volume to the applicators without attenuation radiation dose in the gap. Thus, the curative high dose IORT was delivered to the surface with limited penetration depth to obtain the therapeutic effect. Concurrently, the use of several applicators were allowed dependent on the physician’s choice. Cancer recurrence was assessed according to the appearance of abnormal radiological findings or histological proof from biopsy analyses, whichever occurred first. Recurrence-free survival was measured from the date of primary surgery, completion of definitive radiotherapy or salvage surgery to the date of clinically defined recurrence, disease progression, or the last follow-up visit. Overall survival was calculated from the date of salvage surgery to the date of death from any cause or the last follow-up visit. Stata version 11.0 (Stata Corp, College Station, TX, USA) was used for statistical analyses. Survival curves were generated using the Kaplan–Meier method.
3. Results
Between January 2018 and December 2021, there were five women who underwent eight procedures of IORT for recurrent gynecologic cancers including cervical cancer, endometrial cancer, and uterine leiomyosarcoma. Baseline data were shown in Table 1.The IORT procedure was performed after salvage debulking surgery for cancer recurrence. Doses of IORT ranged from 12 to 20 Gy (median, 15.62 Gy) using 50 kv photons (Table 2). Dosage was prescribed at the surface of the cone or balloon applicator on the pelvic side wall, pelvic lymph node region, abdominal wall, or vaginal stump, respectively.

Table 1.
Baseline data of cancer patients (n = 5).
Table 2.
Clinical outcome of women who underwent intraoperative radiotherapy (n = 5).
Three women experienced local recurrence (Figure 2A), and three women died during follow-up (Figure 2B). The overall local control rate was 40% (2/5), and the overall survival rate was 40% (2/5). The median recurrence-free survival was 13.8 months (95% confidence interval (CI) = 1.6 months to infinity), and the median overall survival was 16.4 months (95% CI = 4.7 months to infinity). The 1-year local control rate was 60% (95% CI = 13% to 88%). The 2-year overall survival rate was 30% (95% CI = 1% to 72%). However, there was no Clavien–Dindo classification grade III–V complication.

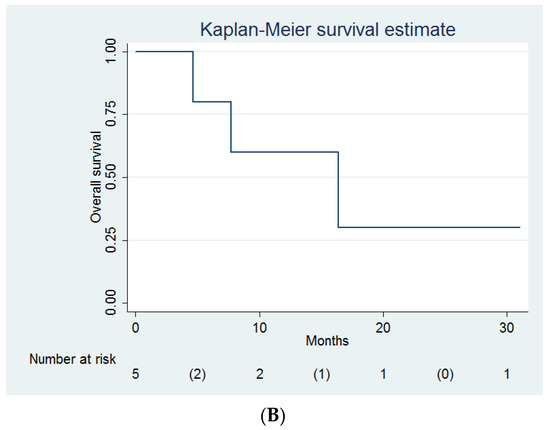
Figure 2.
(A) Recurrence-free survival and (B) overall survival of women undergoing intraoperative radiotherapy (n = 5).
Both endometrial cancer patients were treated with optimal debulking surgery and IORT, and both women did not have any local recurrence after treatment. However, one woman with endometrial cancer died owing to lung and liver metastasis (Table 2).
Repeated IORT procedures were performed in two women (Patients no. 2 and 5, Table 3). The woman who underwent pelvic exenteration and IORT for recurrent cervical cancer, experienced vaginal stump recurrence 17 months after exenteration. The woman with recurrent uterine leiomyosarcoma experienced repeated recurrence and died from recurrence despite repeated optimal debulking surgeries and IORT; however, the recurrent sites did not locate at prior IORT sites.
Table 3.
Clinical outcome of women who underwent repeated intraoperative radiotherapy (n = 2).
4. Discussion
In our study, all women underwent IORT procedures at the end of salvage surgery (Table 2 and Table 3). In our case series, with the aid of IORT cone and balloon applicators (Figure 1a,b), low energy X-ray photon IORT with the Axxent Electronic Brachytherapy system seemed to be feasible as an adjuvant therapy in women who had undergone salvage debulking surgery for recurrent gynecologic cancers, even in women with vaginal stump, pelvic side wall, and abdominal wall metastasis (Table 2 and Table 3).
Common treatment-related toxicities of IOERT and HDR-IORT include peripheral neuropathy, gastrointestinal fistula, gastrointestinal perforation, gastrointestinal obstruction, ureteral stricture, persistent pain, pelvic abscess, perioperative hemorrhage, delayed wound healing, and lymphedema [1,2,15,16,17,18,19,20,21]. In our study, there were no Clavien–Dindo classification grade III–V complications (Table 2), even in women who received repeated IORT (Table 3). Thus, the use of low energy X-ray photon IORT using 50 kv photons to the highly focused area seems to be safe for women who have undergone salvage surgery for recurrent gynecologic cancer patients.
In this study, women who underwent low energy X-ray photon IORT included those with recurrent cervical cancer, recurrent endometrial cancer, and recurrent uterine leiomyosarcoma (Table 2 and Table 3). IORT has been used as a boosting technique to deliver the irradiation directly to the resection bed. The technique is usually used in women with cervical cancer recurrence. The addition of IORT increases the local control rate of recurrent cervical cancer [22]. The role of IORT in endometrial cancer is less frequently reported. Both of our endometrial cancer patients underwent an optimal salvage debulking operation and had a good local control. Dowdy et al. also reported a local control rate of 84% in women with no residual tumor and 47% in women with residual tumors [18]. The amount of residual tumor is significantly associated with a local control rate after IORT [18,23]. Arians et al. reported that the 5-year overall survival rate was 50% in recurrent endometrial carcinoma [3]. Thus, IORT seems to be promising for the treatment of recurrent endometrial cancer patients.
In our patient, repeated recurrent uterine leiomyosarcoma was noted despite the use of IORT. However, the recurrent sites after IORT were not located at previous IORT sites (Table 1 and Table 2). The aggressive behavior of recurrent uterine leiomyosarcoma may increase the failure rate. Coelho et al. also reported that the overall survival was inferior in the sarcoma group compared with the epithelial group (i.e., the 2-year, 5-year, and 8-year overall survival rates were 60%, 20%, and 6% in the sarcoma group versus the 2-year, 5-year, and 8-year overall survival rates of 73%, 57%, and 40% in the epithelial tumor group, respectively, p = 0.005) [24]. However, many patients achieve long-term overall survival and local control without significant morbidity after salvage surgery and IORT, especially in the case of clear margins [24]. Barney et al. also reported a good local control rate in women with primary or locoregionally recurrent uterine sarcoma who received adjuvant IORT after surgical resection [25].
The initial clinical experience of IORT was for the treatment of cervical cancer. Nonetheless, most case series of IORT in gynecological cancer management were for recurrent cervical, endometrial, vaginal, vulvar, and ovarian cancer [2,3,8,15]. Considering the characteristic of IORT for delivering a large irradiation dose and limiting the irradiation exposure to the adjacent regions, IORT is especially suitable for tumors in abdominopelvic regions with much irradiation susceptibility and normal organs surrounding it.
Following the evolution of radiation techniques, the application of IORT has been developed and used for several tumors in different regions and various settings in recurrent or primary cancer management. This includes early breast cancer [26,27,28], recurrent head and neck cancer [29,30,31], locally advanced or recurrent colorectal cancer [32,33,34,35], extremity soft tissue sarcoma [36,37], retroperitoneal sarcoma [38,39], pediatric tumors [40], genitourinary cancers (such as bladder cancer [41], renal cell carcinoma [42], or prostate cancer [43]), gastric cancer [44,45], or pancreatic cancer [46,47,48]. Most of the reported data indicate the above cancer treatments were delivered with IOERT. Some of them were treated with HDR-IORT. The variety of clinical indications of IORT has provided a growing number of patients who have received this radiation modality.
According to the previously published clinical series of recurrent gynecological malignancies, IORT was delivered with electrons in the majority, and others were delivered with HDR-IORT. Surgical margin status plays an important role in the clinical outcome of recurrent gynecologic cancers treated with IORT. Dowdy et al. reported that salvage surgery with negative surgical margins combined with IORT could provide good long-term local control and survival (the 5-year overall survival rate was 71% in R0 surgical resection, compared with the 5-year overall survival rate of 47% in R1 surgical resection and the 5-year overall survival rate of 0% in R2 surgical resection) [18]. Similarly, Delara et al. reported that the 3-year progression-free survival rates were 51.8% in negative margins, 20.5% in the microscopic margin, and 0% in the macroscopic surgical margin [17]. Martínez-Monge et al. reported a poor local control rate in women with recurrent cervical cancer with positive lymph nodes, parametrial involvement, and/or incomplete resection despite the use of IORT [49].
The Memorial Sloan-Kettering Cancer Center has reported their experience of a combination of surgical resection and HDR-IORT for treating recurrent gynecologic cancers, including cervical (n = 9), uterine (n = 7), and vaginal cancer (n = 1) [50]. The 3-year local control rate was 67%, and the 3-year overall survival rate was 54%. However, the 3-year local control rate was only 25% in women with gross residual tumor, compared with 83% in women with complete gross resection (p< 0.01); thus, they emphasized that patient selection is very important for treating recurrent gynecological cancers with a combination of surgical resection and IORT [50]. In contrast to our report, gastrointestinal obstruction (n = 4), abscess (n = 3), peripheral neuropathy (n = 3), rectovaginal fistula (n = 2), and uretheral obstruction (n = 2) were observed in some patients [50].
According to the successful experience of low energy X-ray photon IORT for early breast cancer [9,10,11,12], an undetermined issue is the feasibility of low energy X-ray photon IORT for treating recurrent gynecologic cancers. Shielding in the operation room is demanded while performing IOERT or HDR-IORT. However, shielding is needed less for delivering low energy X-ray photon IORT (i.e., Axxent Electronic Brachytherapy System or Intrabeam System).In addition, the machine for delivering low energy X-ray photon IORT is easily moved and can be transported to different operation rooms or even to different hospitals. Its cost-effectiveness and feasibility have made the low energy X-ray photon IORT system increasingly popular in clinical practice.
The Axxent Electronic Brachytherapy System has been used for treating breast cancer patients [9,10,11,12]. In our institution, IORT was delivered with the Axxent Electronic Brachytherapy System. The local control when using the Axxent Electronic Brachytherapy System to treat early breast cancer was reported to be similar to the conventional external beam radiation therapy [9,10,11,12]. In our study, the use of the Axxent Electronic Brachytherapy System in the treatment of recurrent gynecological cancer is an innovative approach. Our data provide detailed experience and clinical outcomes of delivering IORT with the Axxent Electronic Brachytherapy System in patients with recurrent gynecological cancers, including cervical cancer, endometrial cancer, and uterine leiomyosarcoma. Thus, our results can be considered as an important reference for pretreatment consultation for those women scheduled for salvage surgical resection of the above gynecological cancers.
In addition to recurrent cervical cancer, IORT might have a role as the adjuvant therapy after primary surgical resection of stage IIB cervical cancer. A 5-year survival rate of 49–88%, a 5-year disease-free survival of 70%, and a local control rate of 79–100% have been reported in women with stage IIB cervical cancer receiving surgical resection and IORT [51,52,53]. Similarly, the 2-year disease-free survival in stage IIB cervical cancer treated by concurrent chemoradiotherapy is estimated as 75% [54]. Gao et al. reported the clinical outcome of adjuvant IORT in women with stage IIB cervical adenocarcinoma [52]. After a total dose of weekly intracavitary brachytherapy (total dose HDR 12–14 point A), an IORT dose of 18–20 Gy was delivered using a 12 MeV electron beam during hysterectomy. Adjuvant chemotherapy with 4–6 cycles of cisplatin and 5FU was also performed. The 5-year overall survival and disease-free survival rates were 77.8% and 70.4%, respectively. Local control in the field was 100% even with close/positive resection margins [52]. Gao et al. concluded that IORT was safe and feasible and appeared to confer a disease control benefit to surgical resection, especially for cervical adenocarcinoma [52]. Future researches may assess the effect of the Axxent Electronic Brachytherapy System as an adjuvant IORT after primary surgical resection in women with stage IIB cervical adenocarcinoma.
Gynecologic cancer is a very stressful experience for women and treatment can compromise fertility and reproductive capacity [55]. In addition, therapy for recurrent gynecologic cancers may have a detrimental effect on patients’ quality of life, psychological distress, and even sexual function [55,56]. For example, vaginal vault resection is an effective treatment for vaginal recurrence of cervical cancer; however, the complications of this resection procedure led to a reduced quality of life [57]. To our knowledge, there is no study mentioning about the impact of IORT on quality of life. Future researches can explore its detailed impact on quality of life.
Our study is limited due to its retrospective nature, small sample size, and heterogeneous cancer type. Future large-scale studies are needed to prove the efficacy and safety of low energy X-ray photon IORT for women undergoing salvage surgical resection of recurrent gynecologic cancers.
5. Conclusions
IORT using low energy X-ray photon therapy seems to be feasible and safe as an adjuvant therapy in women who have undergone salvage surgery for recurrent gynecologic cancer. However, large-scale prospective studies are needed to confirm our findings and evaluate its efficacy.
Author Contributions
Conceptualization, P.-W.S. and S.-M.H.; methodology, S.-M.H.; software, S.-M.H.; validation, P.-W.S. and S.-M.H.; formal analysis, S.-M.H.; investigation, S.-M.H.; resources, S.-M.H.; data curation, H.-H.C., W.-H.T. and P.-Y.H.; writing—original draft preparation, H.-H.C. and P.-Y.H.; writing—review and editing, S.-M.H.; visualization, S.-M.H.; supervision, P.-W.S.; project administration, S.-M.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Research Ethics Review Committee of Far Eastern Memorial Hospital (protocol code 110259-E and date of approval 17 November 2021).
Informed Consent Statement
Patient consent was waived due to the retrospective nature of this study and approved by the Research Ethics Review Committee of Far Eastern Memorial Hospital.
Data Availability Statement
The data presented in this study are available on reasonable request to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Foley, O.W.; Rauh-Hain, J.A.; Del Carmen, M.G. The role of intraoperative radiation therapy in the management of recurrent and locally advanced gynecologic cancers. Int. J. Gynecol. Cancer 2013, 23, 9–15. [Google Scholar] [CrossRef]
- Barney, B.M.; Petersen, I.A.; Dowdy, S.C.; Bakkum-Gamez, J.N.; Klein, K.A.; Haddock, M.G. Intraoperative Electron Beam Radiotherapy (IOERT) in the management of locally advanced or recurrent cervical cancer. Radiat. Oncol. 2013, 8, 80. [Google Scholar] [CrossRef]
- Arians, N.; Foerster, R.; Rom, J.; Uhl, M.; Roeder, F.; Debus, J.; Lindel, K. Outcome of patients with local recurrent gynecologic malignancies after resection combined with intraoperative electron radiation therapy (IOERT). Radiat. Oncol. 2016, 11, 44. [Google Scholar] [CrossRef]
- Harrison, L.B.; Enker, E.W.; Anderson, L.L. High-dose-rate intraoperative radiation therapy for colorectal cancer. Oncology 1995, 9, 679–683. [Google Scholar]
- Abe, M.; Fukuda, M.; Yamano, K.; Matsuda, S.; Handa, H. Intra-operative irradiation in abdominal and cerebral tumours. Acta Radiol. Ther. Phys. Biol. 1971, 10, 408–416. [Google Scholar] [CrossRef]
- Pilar, A.; Gupta, M.; Ghosh Laskar, S.; Laskar, S. Intraoperative radiotherapy: Review of techniques and results. Ecancermedicalscience 2017, 11, 750. [Google Scholar] [CrossRef]
- Veronesi, U.; Orecchia, R.; Luini, A.; Gatti, G.; Intra, M.; Zurrida, S.; Ivaldi, G.; Tosi, G.; Ciocca, M.; Tosoni, A.; et al. A preliminary report of intraoperative radiotherapy (IORT) in limited-stage breast cancers that are conservatively treated. Eur. J. Cancer 2001, 37, 2178–2183. [Google Scholar] [CrossRef]
- Sole, C.V.; Calvo, F.A.; Lozano, M.A.; González-Bayón, L.; González-Sansegundo, C.; Alvarez, A.; Lizarraga, S.; García-Sabrido, J. External-beam radiation therapy after surgical resection and intraoperative electron beam radiation therapy for oligorecurrent gynecological cancer. Long-term outcome. Strahlenther. Onkol. 2014, 190, 171–180. [Google Scholar] [CrossRef]
- Chi, M.S.; Ko, H.L.; Chen, C.C.; Hsu, C.H.; Chen, L.K.; Cheng, F.T. Single institute experience of intraoperative radiation therapy in early-stage breast cancer. Medicine 2021, 100, e27842. [Google Scholar] [CrossRef]
- Kostova-Lefterova, D.; Vasileva-Slaveva, M.; Maslyankov, S.; Konsoulova, A.; Atanasova, M.; Paycheva, T.; Vlahova, A.; Genadieva-Yordanova, M.; Prodanova, G.; Zahariev, Z.; et al. Intraoperative radiotherapy with balloon-based electronic brachytherapy system-a systematic review and first bulgarian experience in breast cancer patients. Curr. Oncol. 2021, 28, 335. [Google Scholar] [CrossRef]
- Redler, G.; Templeton, A.; Zhen, H.; Turian, J.; Bernard, D.; Chu, J.C.; Griem, K.L.; Liao, Y. Dosimetric effects of saline- versus water-filled balloon applicators for IORT using the model S700 electronic brachytherapy source. Brachytherapy 2018, 17, 500–505. [Google Scholar] [CrossRef]
- Silverstein, M.J.; Epstein, M.S.; Lin, K.; Chen, P.; Khan, S.; Snyder, L.; Guerra, L.E.; De Leon, C.; Mackintosh, R.; Coleman, C.; et al. Intraoperative radiation using low-kilovoltage x-rays for early breast cancer: A single site trial. Ann. Surg. Oncol. 2017, 24, 3082–3087. [Google Scholar] [CrossRef]
- Alvarez, D.S.A.; Watson, P.G.F.; Popovic, M.; Heng, V.J.; Evans, M.D.C.; Seuntjens, J. Monte Carlo calculation of the relative TG-43 dosimetry parameters for the INTRABEAM electronic brachytherapy source. Phys. Med. Biol. 2020, 65, 245041. [Google Scholar] [CrossRef]
- Dickler, A.; Puthawala, M.Y.; Thropay, J.P.; Bhatnagar, A.; Schreiber, G. Prospective multi-center trial utilizing electronic brachytherapy for the treatment of endometrial cancer. Radiat. Oncol. 2010, 5, 67. [Google Scholar] [CrossRef]
- Foley, O.W.; Rauh-Hain, J.A.; Clark, R.M.; Goodman, A.; Growdon, W.B.; Boruta, D.M.; Schorge, J.O.; Del Carmen, M.G. Intraoperative radiation therapy in the management of gynecologic malignancies. Am. J. Clin. Oncol. 2016, 39, 329–334. [Google Scholar] [CrossRef]
- Jablonska, P.; Cambeiro, M.; Gimeno, M.; Aramendía, J.M.; Mínguez, J.A.; Alcázar, J.L.; Aristu, J.J.; Calvo, F.A.; Martínez-Monge, R. Intraoperative electron beam radiotherapy and perioperative high-dose-rate brachytherapy in previously irradiated oligorecurrent gynecological cancer: Clinical outcome analysis. Clin. Transl. Oncol. 2021, 23, 1934–1941. [Google Scholar] [CrossRef]
- Delara, R.; Yang, J.; Suárez-Salvador, E.; Vora, S.; Magriña, J.; Butler, K.; Magtibay, P. Radical extirpation with intraoperative radiotherapy for locally recurrent gynecologic cancer: An institutional review. Mayo Clin. Proc. Innov. Qual. Outcomes 2021, 5, 1081–1088. [Google Scholar] [CrossRef]
- Dowdy, S.C.; Mariani, A.; Cliby, W.A.; Haddock, M.G.; Petersen, I.A.; Sim, F.H.; Podratz, K.C. Radical pelvic resection and intraoperative radiation therapy for recurrent endometrial cancer: Technique and analysis of outcomes. Gynecol. Oncol. 2006, 101, 280–286. [Google Scholar] [CrossRef]
- Backes, F.J.; Billingsley, C.C.; Martin, D.D.; Tierney, B.J.; Eisenhauer, E.L.; Cohn, D.E.; O’Malley, D.M.; Salani, R.; Copeland, L.J.; Fowler, J.M. Does intra-operative radiation at the time of pelvic exenteration improve survival for patients with recurrent, previously irradiated cervical, vaginal, or vulvar cancer? Gynecol. Oncol. 2014, 135, 95–99. [Google Scholar] [CrossRef]
- Calvo, F.; Sole, C.; Lozano, M.; Gonzalez-Bayon, L.; Gonzalez-Sansegundo, C.; Alvarez, A.; Blanco, J.; Calín, A.; Lizarraga, S.; García-Sabrido, J.L. Intraoperative electron beam radiotherapy and extended surgical resection for gynecological pelvic recurrent malignancies with and without external beam radiation therapy: Long-term outcomes. Gynecol. Oncol. 2013, 130, 537–544. [Google Scholar] [CrossRef]
- Tran, P.T.; Su, Z.; Hara, W.; Husain, A.; Teng, N.; Kapp, D.S. Long-term survivors using intraoperative radiotherapy for recurrent gynecologic malignancies. Int. J. Radiat. Oncol. Biol. Phys. 2007, 69, 504–511. [Google Scholar] [CrossRef]
- Biete, A.; Oses, G. Intraoperative radiation therapy in uterine cervical cancer: A review. Rep. Pr. Oncol. Radiother. 2018, 23, 589–594. [Google Scholar] [CrossRef]
- Coelho, T.M.; Fogaroli, R.C.; Pellizzon, A.C.A.; De Castro, D.G.; Gondim, G.R.M.; Silva, M.L.G.; Chen, M.J.; Ramos, H. Intraoperative radiation therapy for the treatment of recurrent retroperitoneal and pelvic tumors: A single-institution analysis. Radiat. Oncol. 2018, 13, 224. [Google Scholar] [CrossRef]
- Barney, B.M.; Petersen, I.A.; Dowdy, S.C.; Bakkum-Gamez, J.N.; Haddock, M.G. Long-term outcomes with intraoperative radiotherapy as a component of treatment for locally advanced or recurrent uterine sarcoma. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, 191–197. [Google Scholar] [CrossRef]
- Vaidya, J.S.; Wenz, F.; Bulsara, M.; Tobias, J.S.; Joseph, D.J.; Keshtgar, M.; Flyger, H.L.; Massarut, S.; Alvarado, M.; Saunders, C.; et al. Risk-adapted targeted intraoperative radiotherapy versus whole-breast radiotherapy for breast cancer: 5-year results for local control and overall survival from the TARGIT-A randomised trial. Lancet 2014, 383, 603–613. [Google Scholar] [CrossRef]
- Vaidya, J.S.; Bulsara, M.; Baum, M.; Wenz, F.; Massarut, S.; Pigorsch, S.; Alvarado, M.; Douek, M.; Saunders, C.; Flyger, H.L.; et al. Long term survival and local control outcomes from single dose targeted intraoperative radiotherapy during lumpectomy (TARGIT-IORT) for early breast cancer: TARGIT-A randomised clinical trial. BMJ 2020, 370, m2836. [Google Scholar] [CrossRef]
- Veronesi, U.; Orecchia, R.; Maisonneuve, P.; Viale, G.; Rotmensz, N.; Sangalli, C.; Luini, A.; Veronesi, P.; Galimberti, V.; Zurrida, S.; et al. Intraoperative radiotherapy versus external radiotherapy for early breast cancer (ELIOT): A randomised controlled equivalence trial. Lancet Oncol. 2013, 14, 1269–1277. [Google Scholar] [CrossRef]
- Scala, L.M.; Hu, K.; Urken, M.L.; Schantz, S.; Harrison, L.B. Intraoperative high-dose-rate radiotherapy in the management of locoregionally recurrent head and neck cancer. Head Neck 2013, 35, 485–492. [Google Scholar] [CrossRef]
- Zeidan, Y.H.; Shiue, K.; Weed, D.; Johnstone, P.A.; Terry, C.; Freeman, S.; Krowiak, E.; Borrowdale, R.; Huntley, T.; Yeh, A. Intraoperative radiotherapy for parotid cancer: A single-institution experience. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 1831–1836. [Google Scholar] [CrossRef]
- Zeidan, Y.H.; Yeh, A.; Weed, D.; Terry, C.; Freeman, S.; Krowiak, E.; Borrowdale, R.; Huntley, T. Intraoperative radiation therapy for advanced cervical metastasis: A single institution experience. Radiat. Oncol. 2011, 6, 72. [Google Scholar] [CrossRef]
- Kusters, M.; Valentini, V.; Calvo, F.; Krempien, R.; Nieuwenhuijzen, G.A.; Martijn, H.; Doglietto, G.B.; del Valle, E.; Roeder, F.; Buchler, M.W.; et al. Results of European pooled analysis of IORT-containing multimodality treatment for locally advanced rectal cancer: Adjuvant chemotherapy prevents local recurrence rather than distant metastases. Ann. Oncol. 2010, 21, 1279–1284. [Google Scholar] [CrossRef]
- Sole, C.V.; Calvo, F.A.; Serrano, J.; del Valle, E.; Rodriguez, M.; Muñoz-Calero, A.; Turégano, F.; García-Sabrido, J.L.; Garcia-Alfonso, P.; Peligros, I.; et al. Post-chemoradiation intraoperative electron-beam radiation therapy boost in resected locally advanced rectal cancer: Long-term results focused on topographic pattern of locoregional relapse. Radiother. Oncol. 2014, 112, 52–58. [Google Scholar] [CrossRef]
- Holman, F.A.; Haddock, M.G.; Gunderson, L.L.; Kusters, M.; Nieuwenhuijzen, G.A.; van den Berg, H.A.; Nelson, H.; Rutten, H.J. Results of intraoperative electron beam radiotherapy containing multimodality treatment for locally unresectable T4 rectal cancer: A pooled analysis of the Mayo Clinic Rochester and Catharina Hospital Eindhoven. J. Gastrointest. Oncol. 2016, 7, 903–916. [Google Scholar] [CrossRef]
- Haddock, M.G.; Miller, R.C.; Nelson, H.; Pemberton, J.H.; Dozois, E.J.; Alberts, S.R.; Gunderson, L.L. Combined modality therapy including intraoperative electron irradiation for locally recurrent colorectal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 143–150. [Google Scholar] [CrossRef]
- Holman, F.; Bosman, S.; Haddock, M.; Kusters, M.; Nieuwenhuijzen, G.A.; van den Berg, H.; Nelson, H.; Rutten, H.J. Results of a pooled analysis of IOERT containing multimodality treatment for locally recurrent rectal cancer: Results of 565 patients of two major treatment centres. Eur. J. Surg. Oncol. 2017, 43, 107–117. [Google Scholar] [CrossRef]
- Calvo, F.A.; Sole, C.V.; Polo, A.; Cambeiro, M.; Montero, A.; Álvarez, A.; Cuervo, M.; Julian, M.S.; Martínez-Monge, R. Limb-sparing management with surgical resection, external-beam and intraoperative electron-beam radiation therapy boost for patients with primary soft tissue sarcoma of the extremity. Strahlenther. Und Onkol. 2014, 190, 891–898. [Google Scholar] [CrossRef]
- Roeder, F.; Lehner, B.; Saleh-Ebrahimi, L.; Hensley, F.W.; Ulrich, A.; Alldinger, I.; Mechtersheimer, G.; Huber, P.E.; Krempien, R.; Bischof, M.; et al. Intraoperative electron radiation therapy combined with external beam radiation therapy and limb sparing surgery in extremity soft tissue sarcoma: A retrospective single center analysis of 183 cases. Radiother. Oncol. 2016, 119, 22–29. [Google Scholar] [CrossRef]
- Roeder, F.; Ulrich, A.; Habl, G.; Uhl, M.; Saleh-Ebrahimi, L.; Huber, P.E.; Schulz-Ertner, D.; Nikoghosyan, A.V.; Alldinger, I.; Krempien, R.; et al. Clinical phase I/II trial to investigate preoperative dose-escalated intensity-modulated radiation therapy (IMRT) and intraoperative radiation therapy (IORT) in patients with retroperitoneal soft tissue sarcoma: Interim analysis. BMC Cancer 2014, 14, 1–12. [Google Scholar] [CrossRef]
- Gronchi, A.; De Paoli, A.; Dani, C.; Merlo, D.F.; Quagliuolo, V.; Grignani, G.; Bertola, G.; Navarria, P.; Sangalli, C.; Buonadonna, A.; et al. Preoperative chemo-radiation therapy for localised retroperitoneal sarcoma: A phase I–II study from the Italian Sarcoma Group. Eur. J. Cancer 2014, 50, 784–792. [Google Scholar] [CrossRef]
- Sole, C.V.; Calvo, F.A.; Polo, A.; Cambeiro, M.; Gonzalez, C.; Desco, M.; Martinez-Monge, R. Intraoperative electron-beam radiation therapy for pediatric Ewing sarcomas and rhabdomyosarcomas: Long-term outcomes. Int. J. Radiat. Oncol. Biol. Phys. 2015, 92, 1069–1076. [Google Scholar] [CrossRef]
- Hallemeier, C.L.; Karnes, R.J.; Pisansky, T.M.; Davis, B.; Gunderson, L.L.; Leibovich, B.C.; Haddock, M.G.; Choo, R. Multimodality therapy including surgical resection and intraoperative electron radiotherapy for recurrent or advanced primary carcinoma of the urinary bladder or ureter. Am. J. Clin. Oncol. 2013, 36, 596–600. [Google Scholar] [CrossRef]
- Paly, J.J.; Hallemeier, C.L.; Biggs, P.J.; Niemierko, A.; Roeder, F.; Martínez-Monge, R.; Whitson, J.; Calvo, F.A.; Fastner, G.; Sedlmayer, F.; et al. Outcomes in a multi-institutional cohort of patients treated with intraoperative radiation therapy for advanced or recurrent renal cell carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 618–623. [Google Scholar] [CrossRef]
- Krengli, M.; Terrone, C.; Ballarè, A.; Loi, G.; Tarabuzzi, R.; Marchioro, G.; Beldì, D.; Mones, E.; Bolchini, C.; Volpe, A.; et al. Intraoperative radiotherapy during radical prostatectomy for locally advanced prostate cancer: Technical and dosimetric aspects. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, 1073–1077. [Google Scholar] [CrossRef]
- Fu, S.; Lu, J.J.; Zhang, Q.; Yang, Z.; Peng, L.; Xiong, F. Intraoperative radiotherapy combined with adjuvant chemoradiotherapy for locally advanced gastric adenocarcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2008, 72, 1488–1494. [Google Scholar] [CrossRef]
- Zhang, Q.; Tey, J.; Peng, L.; Yang, Z.; Xiong, F.; Jiang, R.; Liu, T.; Fu, S.; Lu, J.J. Adjuvant chemoradiotherapy with or without intraoperative radiotherapy for the treatment of resectable locally advanced gastric adenocarcinoma. Radiother. Oncol. 2012, 102, 51–55. [Google Scholar] [CrossRef]
- Calvo, F.A.; Sole, C.V.; Atahualpa, F.; Lozano, M.A.; Gomez-Espi, M.; Calin, A.; García-Alfonso, P.; Gonzalez-Bayon, L.; Herranz, R.; García-Sabrido, J.L. Chemoradiation for resected pancreatic adenocarcinoma with or without intraoperative radiation therapy boost: Long-term outcomes. Pancreatology 2013, 13, 576–582. [Google Scholar] [CrossRef]
- Valentini, V.; Calvo, F.; Reni, M.; Krempien, R.; Sedlmayer, F.; Buchler, M.W.; Di Carlo, V.; Doglietto, G.B.; Fastner, G.; Garcia-Sabrido, J.L.; et al. Intra-operative radiotherapy (IORT) in pancreatic cancer: Joint analysis of the ISIORT-Europe experience. Radiother. Oncol. 2009, 91, 54–59. [Google Scholar] [CrossRef]
- Ogawa, K.; Karasawa, K.; Ito, Y.; Ogawa, Y.; Jingu, K.; Onishi, H.; Aoki, S.; Wada, H.; Kokubo, M.; Etoh, H.; et al. Intraoperative radiotherapy for resected pancreatic cancer: A multi-institutional retrospective analysis of 210 patients. Int. J. Radiat. Oncol. Biol. Phys. 2010, 77, 734–742. [Google Scholar] [CrossRef]
- Martínez-Mongem, R.; Jurado, M.; Aristu, J.J.; Moreno, M.; Cambeiro, M.; Pe’rez-Ochoa, A.; Lo´pez-Garcı´a, G.; Alcázar, J.; Martínez-Monge, R. Intraoperative electron beam radiotherapy during radical surgery for locally advanced and recurrent cervical cancer. Gynecol. Oncol. 2001, 82, 538–543. [Google Scholar] [CrossRef]
- Gemignani, M.L.; Alektiar, K.M.; Leitao, M.; Mychalczak, B.; Chi, D.; Venkatraman, E.; Barakat, R.R.; Curtin, J.P. Radical surgical resection and high-dose intraoperative radiation therapy (HDR-IORT) in patients with recurrent gynecologic cancers. Int. J. Radiat. Oncol. Biol. Phys. 2001, 50, 687–694. [Google Scholar] [CrossRef]
- Giorda, G.; Boz, G.; Gadducci, A. Multimodality approach in extra-cervical locally advanced cervical cancer: Chemoradiation, surgery and intra-operative radiation therapy. A phase II trial. EJSO 2011, 37, 442–447. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Gao, Y.; Liu, Z.; Gao, F.; Chen, X. Intraoperative radiotherapy in stage IIB adenocarcinoma of the uterine cervix: A retrospective study. Oncotargets Ther. 2013, 6, 1695–1700. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Liu, Z.; Chen, X. Preliminary results of intraoperative radiation therapy for cervical carcinoma IIB. Zhongua Fu Chan Ke Za Zhi 2002, 37, 553–555. [Google Scholar]
- Matsuzaki, S.; Klar, M.; Mikami, M.; Shimada, M.; Grubbs, B.H.; Fujiwara, K.; Roman, L.D.; Matsuo, K. Management of stage IIB cervical cancer: An overview of the current evidence. Curr. Oncol. Rep. 2020, 22, 28. [Google Scholar] [CrossRef]
- Laganà, A.S.; La Rosa, V.L.; Rapisarda, A.M.; Platania, A.; Vitale, S.G. Psychological impact of fertility preservation techniques in women with gynaecological cancer. Ecancermedicalscience 2017, 11, ed62. [Google Scholar] [CrossRef]
- Vitale, S.G.; La Rosa, V.L.; Rapisarda, A.M.C.; Laganà, A.S. Fertility preservation in women with gynaecologic cancer: The impact on quality of life and psychological well-being. Hum. Fertil. 2018, 21, 35–38. [Google Scholar] [CrossRef]
- Abe, A.; Matoda, M.; Okamoto, S.; Kondo, E.; Kato, K.; Omatsu, K.; Umayahara, K.; Utsugi, K.; Takeshima, N. Resection of the vaginal vault for vaginal recurrence of cervical cancer after hysterectomy and brachytherapy. World J. Surg. Oncol. 2015, 13, 137. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).