


Correlation between the Capillary Blood Flow Characteristics and Endothelium Function in Healthy Volunteers and Patients Suffering from Coronary Heart Disease and Atrial Fibrillation: A Pilot Study
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
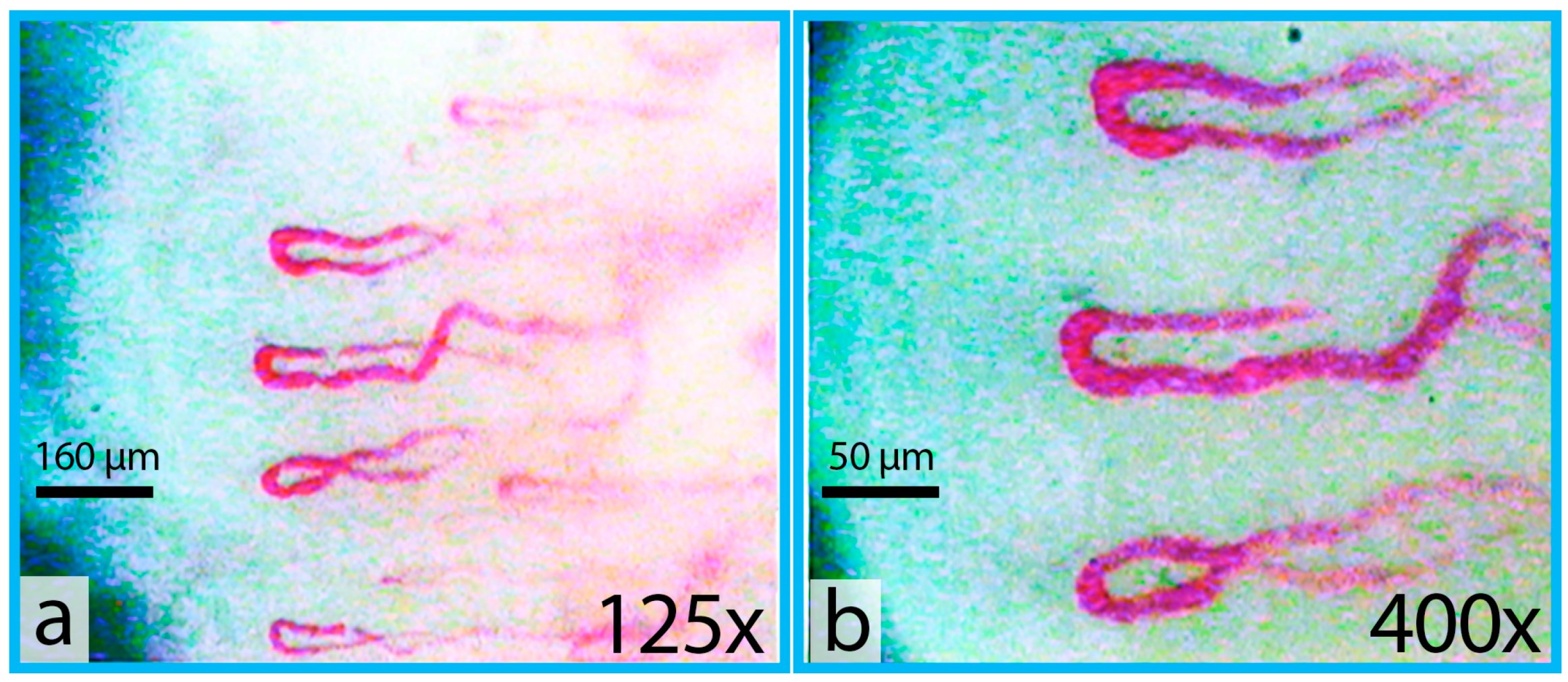
2.2. Vital Digital Capillaroscopy
- Size of RBC aggregates—the average area of RBC aggregate in μm2.
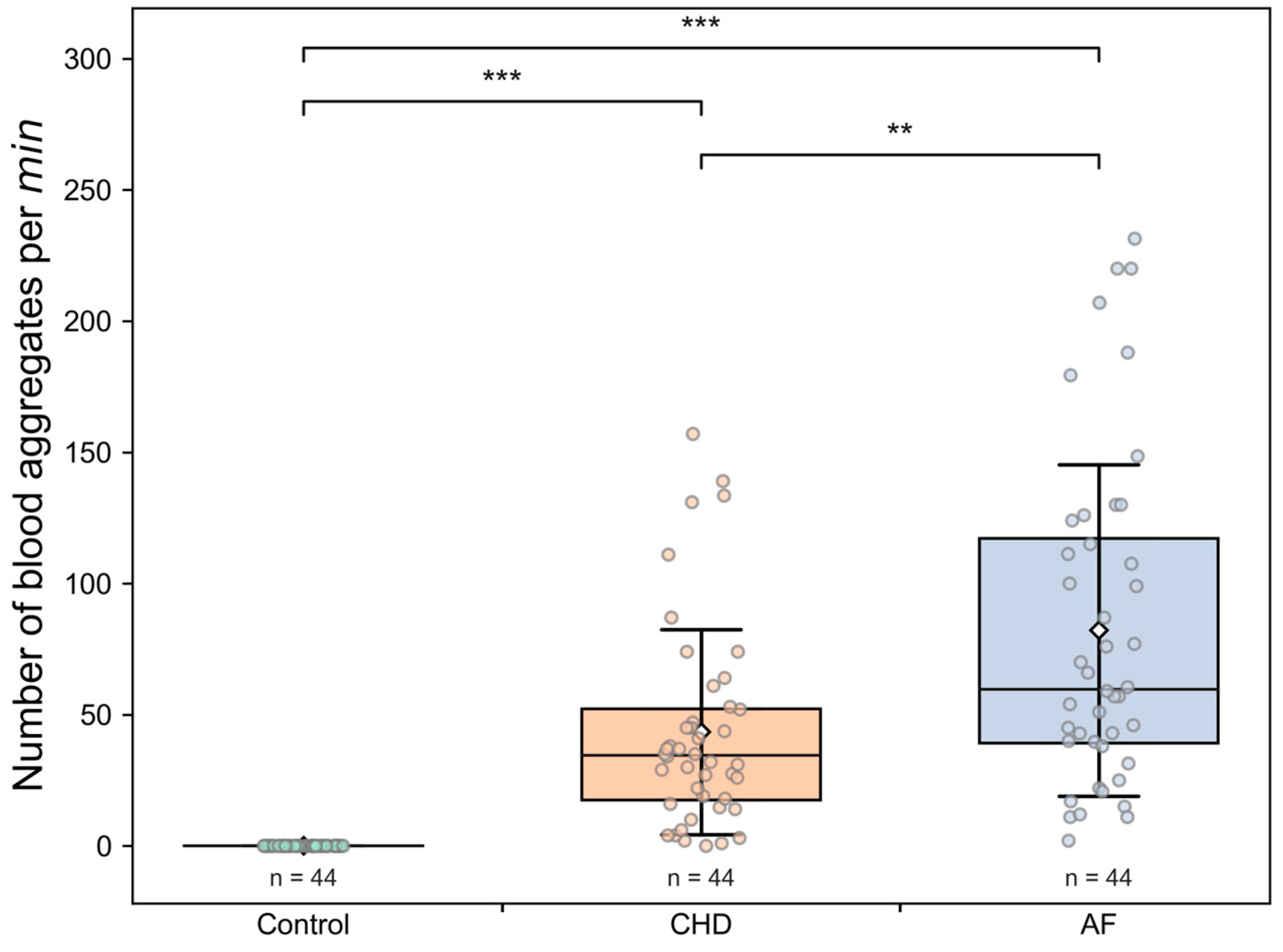
- Number of aggregates per min—ratio of the number of observed aggregates in a capillary per measuring interval. The aggregate count is calculated by the number of crossings of a fixed capillary cross section.
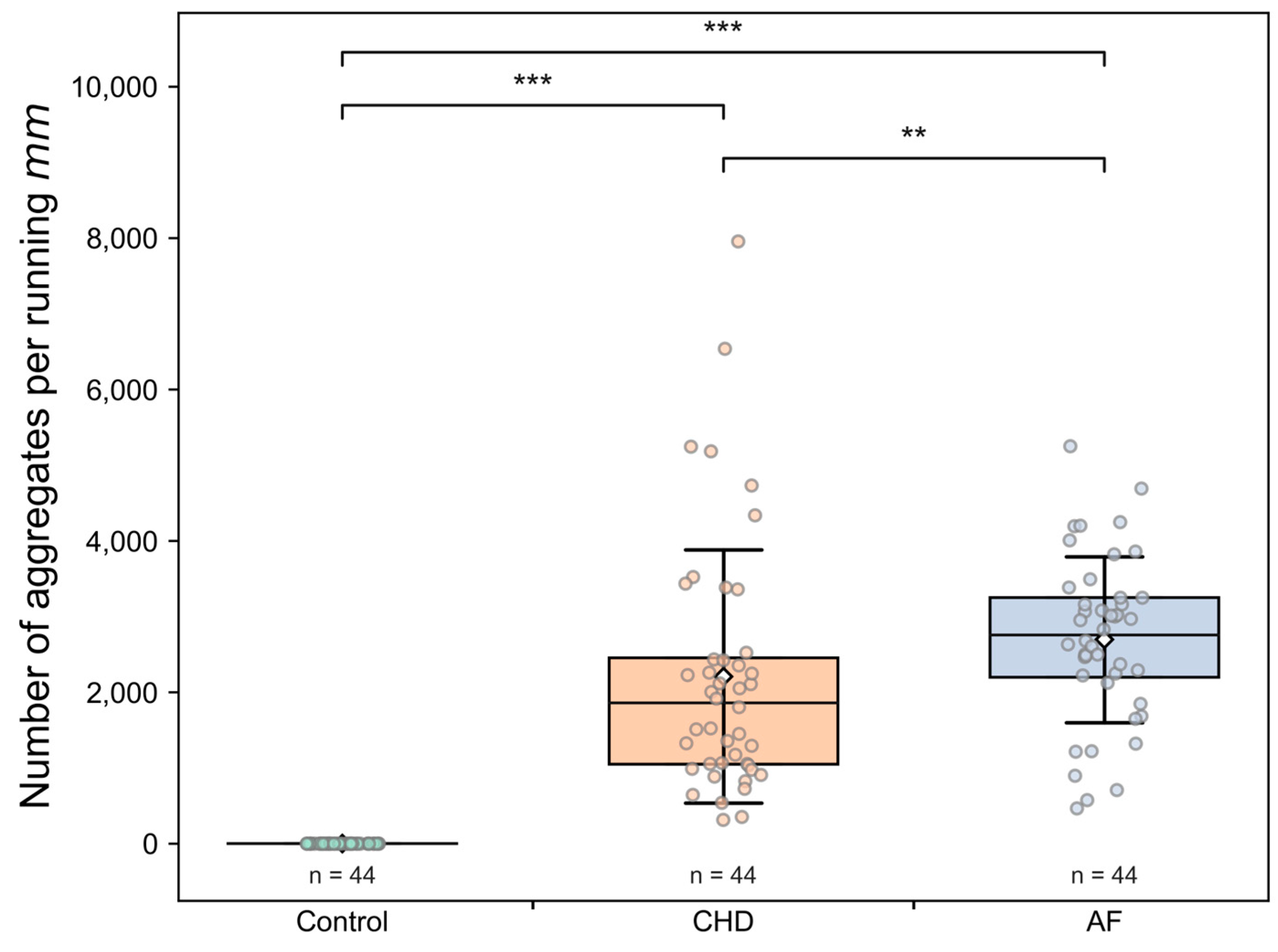
- Number of aggregates per running mm—the average number of observed aggregates in a capillary over the linear dimension of the capillary during measuring interval.
- Capillary blood flow velocity—the averaged velocity of moving single RBCs and RBC aggregates determined in the observed capillary during measuring interval in μm/s.
2.3. Characterization of the Endothelium Function
2.4. Statistical Analysis of the Data
3. Results
3.1. Microcirculation in Studied Groups
3.1.1. Microcirculation Parameters
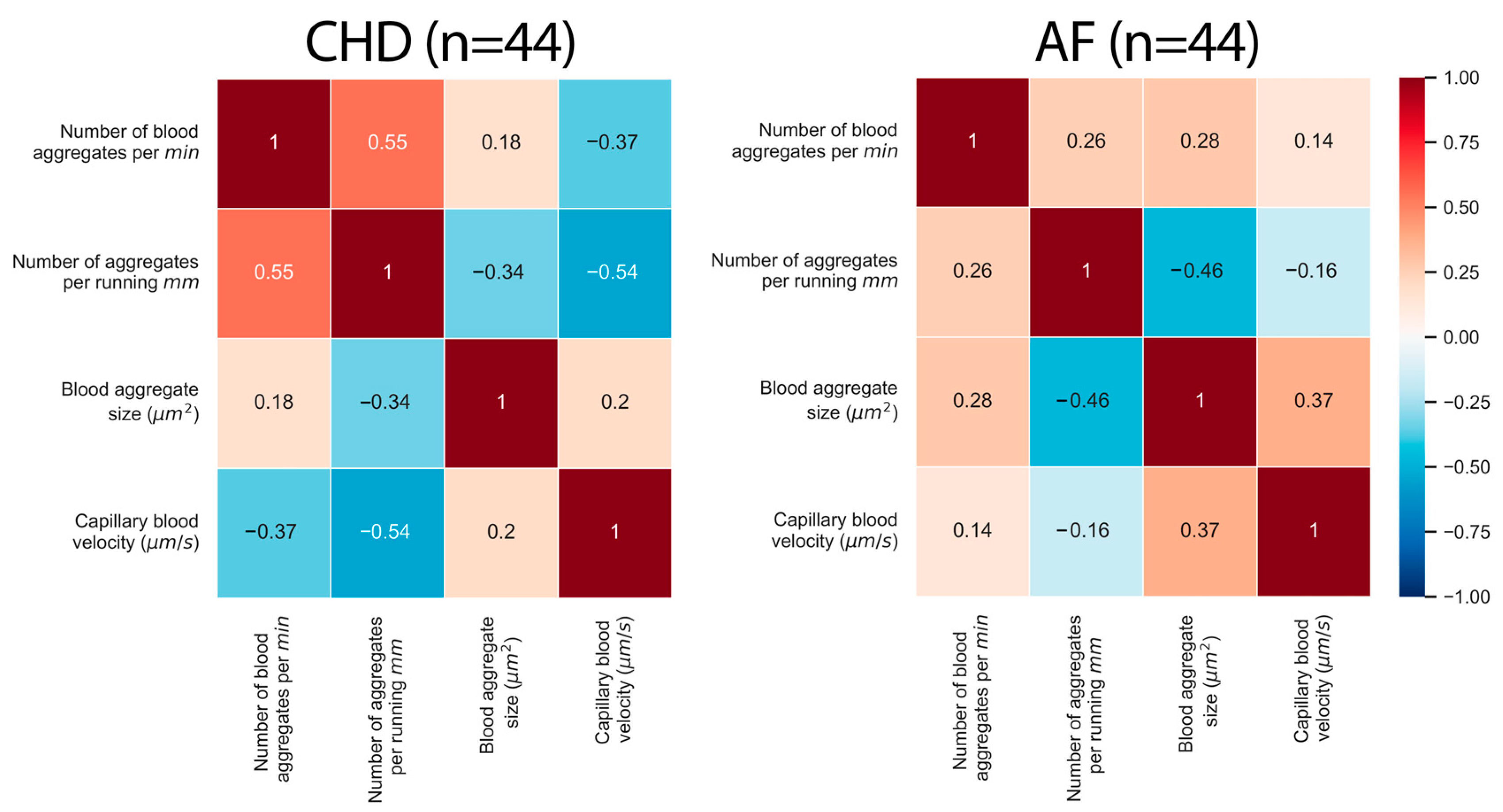
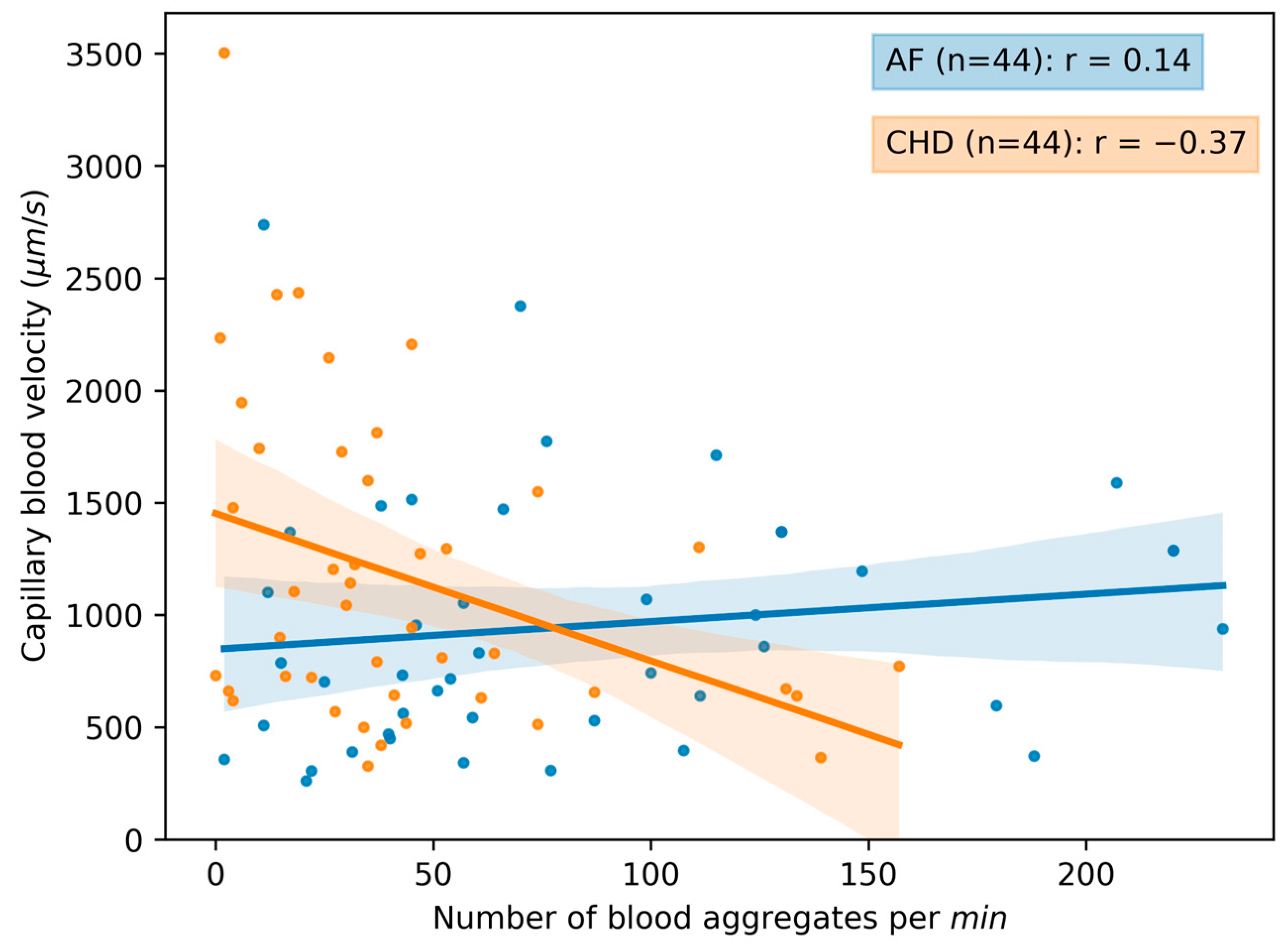
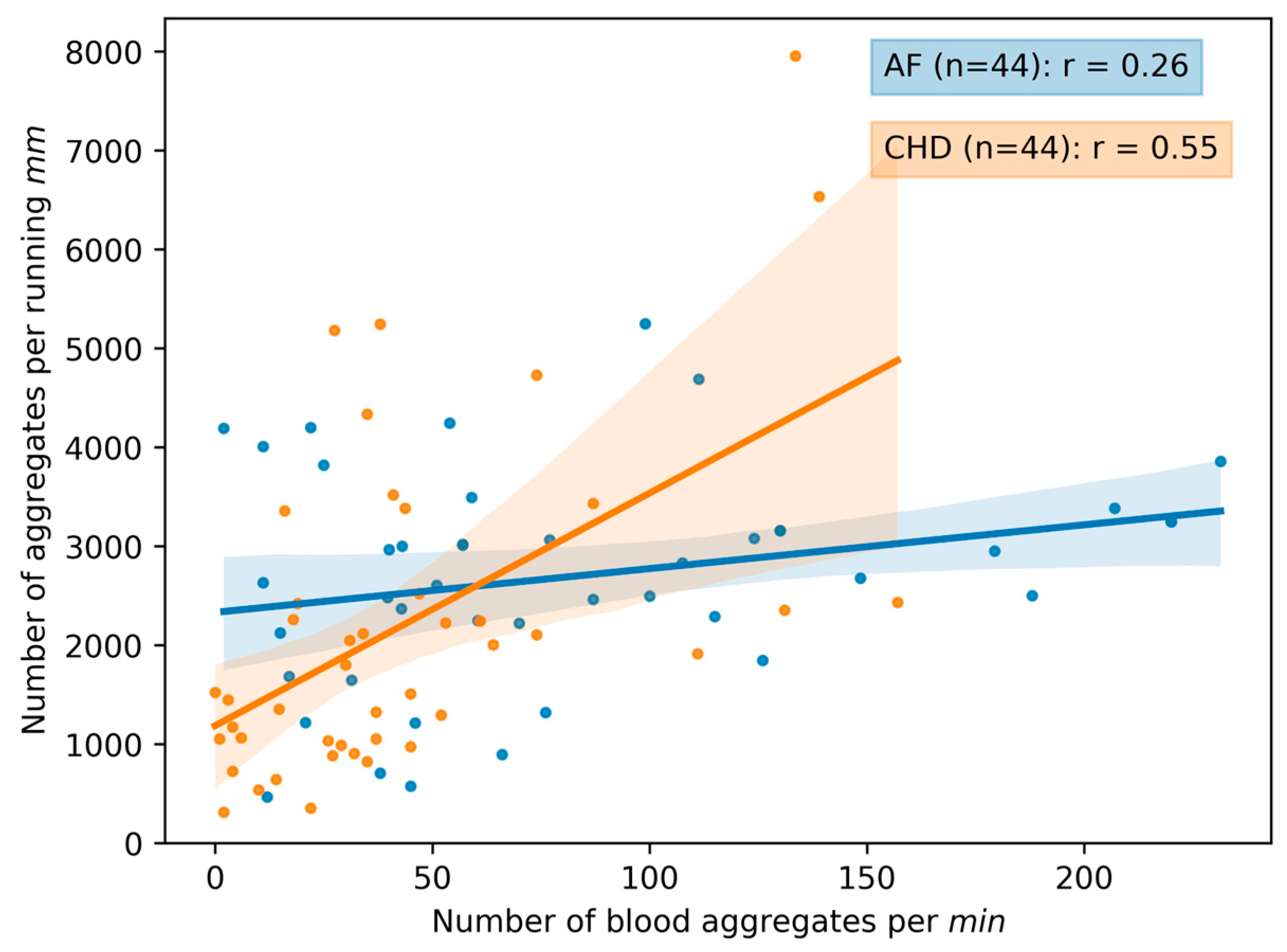
3.1.2. Correlations between the Parameters of Microcirculation
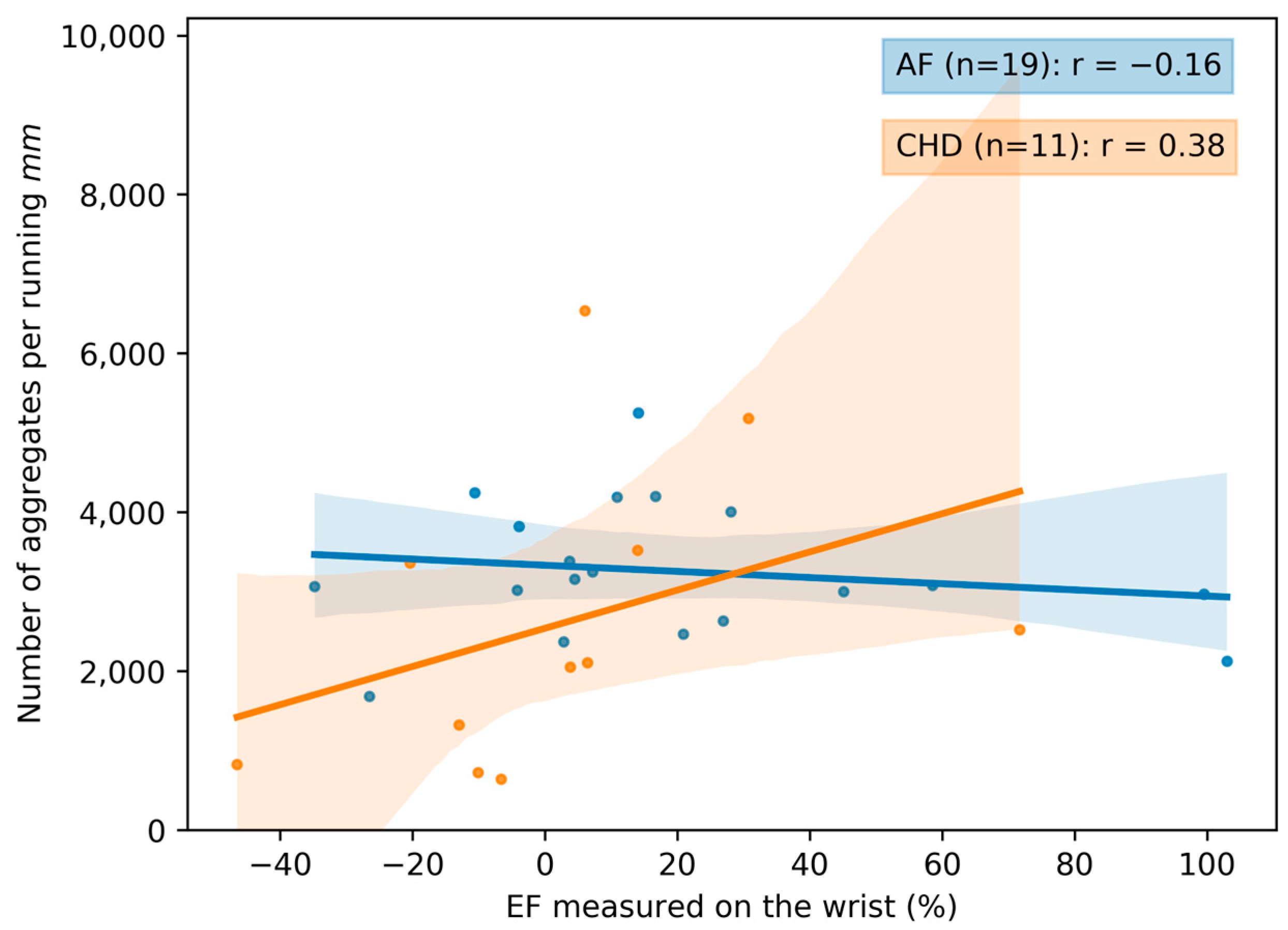
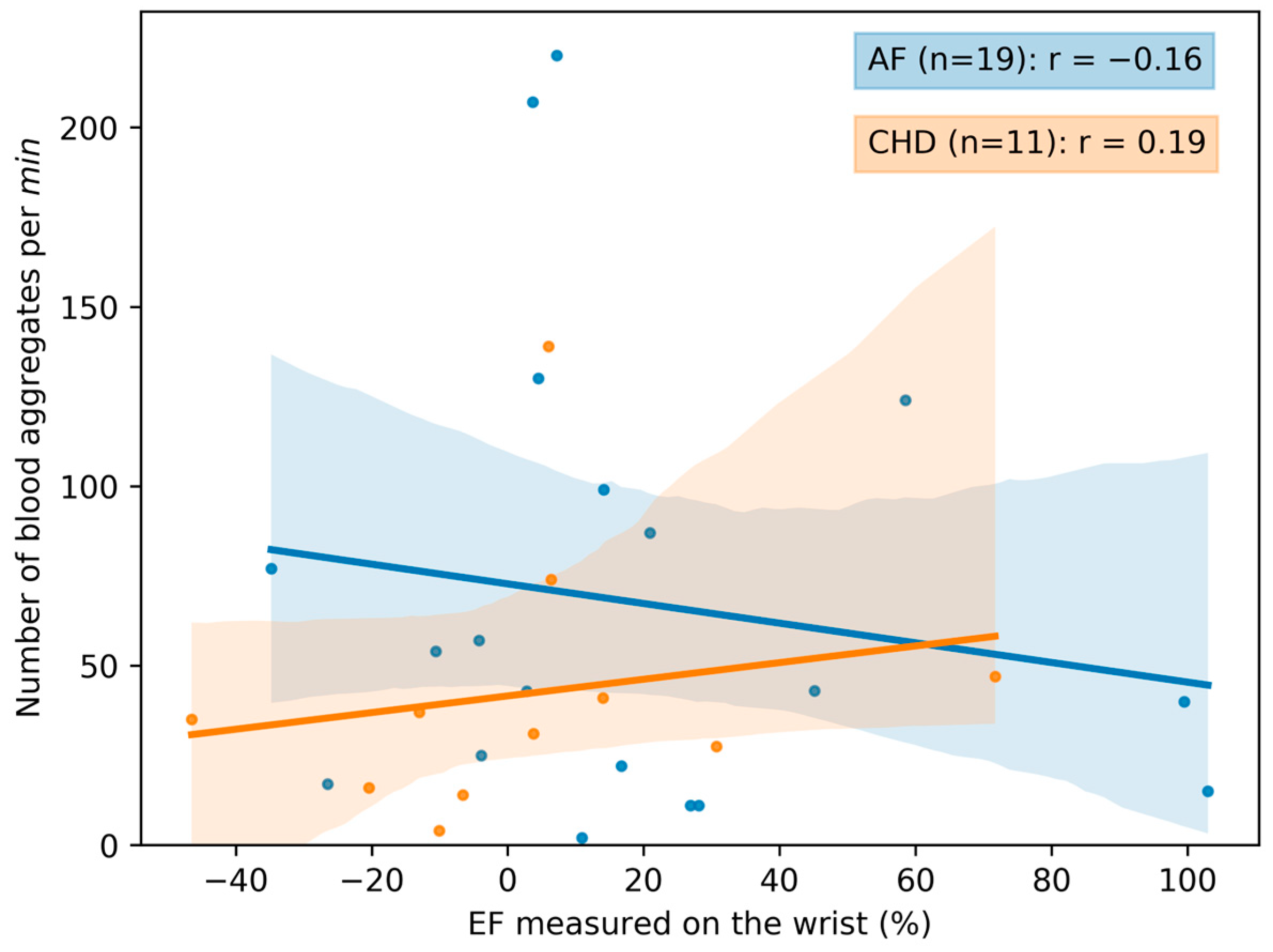
3.2. The Correlation between Microcirculation Parameters and the Endothelial Function
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lowe, G.D.O.; Lee, A.J.; Rumley, A.; Price, J.F.; Fowkes, F.G.R. Blood Viscosity and Risk of Cardiovascular Events: The Edinburgh Artery Study. Br. J. Haematol. 1997, 96, 168–173. [Google Scholar] [CrossRef]
- Slovinski, A.P.; Hajjar, L.A.; Ince, C. Microcirculation in Cardiovascular Diseases. J. Cardiothorac. Vasc. Anesth. 2019, 33, 3458–3468. [Google Scholar] [CrossRef]
- Agabiti-Rosei, E.; Heagerty, A.M.; Rizzoni, D. Microcirculation in Cardiovascular Diseases; Springer International Publishing: Cham, Switzerland, 2020; ISBN 978-3-030-47800-1. [Google Scholar]
- Félétou, M. The Endothelium, Part I: Multiple Functions of the Endothelial Cells—Focus on Endothelium-Derived Vasoactive Mediators. In Colloquium Series on Integrated Systems Physiology: From Molecule to Function; Morgan & Claypool: Kentfield, CA, USA, 2011; Volume 3, pp. 1–306. [Google Scholar] [CrossRef]
- Van De Graaff, K.M. Human Anatomy; McGraw-Hill Higher Education: Sydney, Australia, 2001; Volume 1. [Google Scholar]
- Baskurt, O.; Neu, B.; Meiselman, H.J. Red Blood Cell Aggregation; CRC Press: Boca Raton, FL, USA, 2011; ISBN 9781439841815. [Google Scholar]
- Barshtein, G. Biochemical and Biophysical Properties of Red Blood Cells in Disease. Biomolecules 2022, 12, 923. [Google Scholar] [CrossRef]
- Maslianitsyna, A.; Ermolinskiy, P.; Lugovtsov, A.; Pigurenko, A.; Sasonko, M.; Gurfinkel, Y.; Priezzhev, A. Multimodal Diagnostics of Microrheologic Alterations in Blood of Coronary Heart Disease and Diabetic Patients. Diagnostics 2021, 11, 76. [Google Scholar] [CrossRef]
- Wolf, P.A.; Abbott, R.D.; Kannel, W.B. Atrial Fibrillation: A Major Contributor to Stroke in the Elderly. The Framingham Study. Arch. Intern. Med. 1987, 147, 1561–1564. [Google Scholar] [CrossRef]
- Wolf, P.A.; Abbott, R.D.; Kannel, W.B. Atrial Fibrillation as an Independent Risk Factor for Stroke: The Framingham Study. Stroke 1991, 22, 983–988. [Google Scholar] [CrossRef] [PubMed]
- Lamassa, M.; Di Carlo, A.; Pracucci, G.; Basile, A.M.; Trefoloni, G.; Vanni, P.; Spolveri, S.; Baruffi, M.C.; Landini, G.; Ghetti, A.; et al. Characteristics, Outcome, and Care of Stroke Associated with Atrial Fibrillation in Europe. Stroke 2001, 32, 392–398. [Google Scholar] [CrossRef]
- Go, A.S.; Hylek, E.M.; Phillips, K.A.; Chang, Y.; Henault, L.E.; Selby, J.V.; Singer, D.E. Prevalence of Diagnosed Atrial Fibrillation in Adults. JAMA 2001, 285, 2370. [Google Scholar] [CrossRef] [PubMed]
- Zherebtsov, E.A.; Zharkikh, E.V.; Loktionova, Y.I.; Zherebtsova, A.I.; Sidorov, V.V.; Rafailov, E.U.; Dunaev, A.V. Wireless Dynamic Light Scattering Sensors Detect Microvascular Changes Associated with Ageing and Diabetes. IEEE Trans. Biomed. Eng. 2023, 1–8. [Google Scholar] [CrossRef]
- Dunaev, A. Wearable Devices for Multimodal Optical Diagnostics of Microcirculatory-Tissue Systems: Application Experience in the Clinic and Space. J. Biomed. Photonics. Eng. 2023, 9, 020201. [Google Scholar] [CrossRef]
- Abdurashitov, A.S.; Lychagov, V.V.; Sindeeva, O.A.; Semyachkina-Glushkovskaya, O.V.; Tuchin, V.V. Histogram Analysis of Laser Speckle Contrast Image for Cerebral Blood Flow Monitoring. Front. Optoelectron. 2015, 8, 187–194. [Google Scholar] [CrossRef]
- Timoshina, P.A.; Zinchenko, E.M.; Tuchina, D.K.; Sagatova, M.M.; Semyachkina-Glushkovskaya, O.V.; Tuchin, V.V. Laser Speckle Contrast Imaging of Cerebral Blood Flow of Newborn Mice at Optical Clearing. In Proceedings of the Saratov Fall Meeting 2016: Optical Technologies in Biophysics and Medicine XVIII, Saratov, Russia, 27–30 September 2016; SPIE: Bellingham, WA, USA, 2017; Volume 10336, p. 1033610. [Google Scholar]
- Gurfinkel, Y.I.; Sasonko, M.L.; Kuznetzov, M.I.; Priezzhev, A.V. Importance of Image Processing in Digital Optical Capillaroscopy for Early Diagnostics of Arterial Hypertension. In Proceedings of the 2015 International Conference on BioPhotonics (BioPhotonics), Florence, Italy, 20–22 May 2015; IEEE: Piscataway, NJ, USA; pp. 1–4. [Google Scholar]
- Fagrell, B.; Intaglietta, M. Microcirculation: Its Significance in Clinical and Molecular Medicine. J. Intern. Med. 1997, 241, 349–362. [Google Scholar] [CrossRef]
- Lugovtsov, A.E.; Gurfinkel, Y.I.; Ermolinskiy, P.B.; Fabrichnova, A.A.; Priezzhev, A.V. The Use of Capillaroscopy and Aggregometry Methods to Diagnose the Alterations of Microcirculation and Microrheology in Diabetes. In Biomedical Photonics for Diabetes Research; CRC Press: Boca Raton, FL, USA, 2022; pp. 57–79. [Google Scholar]
- Lugovtsov, A.E.; Gurfinkel, Y.I.; Ermolinskiy, P.B.; Maslyanitsina, A.I.; Dyachuk, L.I.; Priezzhev, A.V. Optical Assessment of Alterations of Microrheologic and Microcirculation Parameters in Cardiovascular Diseases. Biomed. Opt. Express 2019, 10, 3974. [Google Scholar] [CrossRef]
- Hardeman, M.R.; Dobbe, J.G.; Ince, C. The Laser-Assisted Optical Rotational Cell Analyzer (LORCA) as Red Blood Cell Aggregometer. Clin. Hemorheol. Microcirc. 2001, 25, 1–11. [Google Scholar] [PubMed]
- Priezzhev, A.V.; Lee, K.; Firsov, N.N.; Lademann, J. Optical Study of RBC Aggregation in Whole Blood Samples and Single Cells. In Handbook of Optical Biomedical Diagnostics, 2nd ed.; SPIE Press Bellingham: Bellingham, WA, USA, 2016; Volume 2: Methods; pp. 5–13. [Google Scholar]
- Shin, S.; Yang, Y.; Suh, J.-S. Measurement of Erythrocyte Aggregation in a Microchip Stirring System by Light Transmission. Clin. Hemorheol. Microcirc. 2009, 41, 197–207. [Google Scholar] [CrossRef]
- Ruaro, B.; Smith, V.; Sulli, A.; Pizzorni, C.; Tardito, S.; Patané, M.; Paolino, S.; Cutolo, M. Innovations in the Assessment of Primary and Secondary Raynaud’s Phenomenon. Front. Pharmacol. 2019, 10, 360. [Google Scholar] [CrossRef]
- Lambova, S.N.; Kurteva, E.K.; Dzhambazova, S.S.; Vasilev, G.H.; Kyurkchiev, D.S.; Geneva-Popova, M.G. Capillaroscopy and Immunological Profile in Systemic Sclerosis. Life 2022, 12, 498. [Google Scholar] [CrossRef]
- D’Oria, M.; Gandin, I.; Riccardo, P.; Hughes, M.; Lepidi, S.; Salton, F.; Confalonieri, P.; Confalonieri, M.; Tavano, S.; Ruaro, B. Correlation between Microvascular Damage and Internal Organ Involvement in Scleroderma: Focus on Lung Damage and Endothelial Dysfunction. Diagnostics 2022, 13, 55. [Google Scholar] [CrossRef]
- Edwards, G.; Félétou, M.; Weston, A.H. Endothelium-Derived Hyperpolarising Factors and Associated Pathways: A Synopsis. Pflug. Arch. 2010, 459, 863–879. [Google Scholar] [CrossRef]
- Pizov, A.V.; Pizov, N.A.; Skachkova, O.A.; Pizova, N.V. Endothelial Function in Normal and Pathological Conditions. Med. Counc. 2019, 6, 154–159. [Google Scholar] [CrossRef]
- Furchgott, R.F.; Zawadzki, J.V. The Obligatory Role of Endothelial Cells in the Relaxation of Arterial Smooth Muscle by Acetylcholine. Nature 1980, 288, 373–376. [Google Scholar] [CrossRef]
- Zeiher, A.M.; Drexler, H.; Wollschlaeger, H.; Saurbier, B.; Just, H. Coronary Vasomotion in Response to Sympathetic Stimulation in Humans: Importance of the Functional Integrity of the Endothelium. J. Am. Coll. Cardiol. 1989, 14, 1181–1190. [Google Scholar] [CrossRef]
- Simmonds, M.J.; Detterich, J.A.; Connes, P. Nitric Oxide, Vasodilation and the Red Blood Cell. Biorheology 2014, 51, 121–134. [Google Scholar] [CrossRef] [PubMed]
- Osipov, A.N.; Borisenko, G.G.; Vladimirov, Y.A. Biological Activity of Hemoprotein Nitrosyl Complexes. Biochemistry 2007, 72, 1491–1504. [Google Scholar] [CrossRef] [PubMed]
- Vanin, A.F. Nitric Oxide and Its Detection in Biological Systems by the Electron Paramagnetic Resonance Technique. Phys.-Uspekhi 2000, 43, 415–417. [Google Scholar] [CrossRef]
- Muravyov, A.V. The Role of Gaseous Mediators (CO, NO and H2S) in the Regulation of Blood Circulation: Analysis of the Participation of Blood Cell Microrheology. Reg. Blood Circ. Microcirc. 2021, 20, 91–99. [Google Scholar] [CrossRef]
- Shabrov, A.V.; Apresyan, A.G.; Dobkes, A.L.; Ermolov, S.U.; Ermolova, T.V.; Manasyan, S.G.; Serdyukov, S.V. Current Methods of Endothelial Dysfunction Assessment and Their Possible Use in the Practical Medicine. Ration. Pharmacother. Cardiol. 2016, 12, 733–742. [Google Scholar] [CrossRef]
- Vita, J.A.; Keaney, J.F. Endothelial Function. Circulation 2002, 106, 640–642. [Google Scholar] [CrossRef]
- Bonetti, P.O.; Lerman, L.O.; Lerman, A. Endothelial Dysfunction. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 168–175. [Google Scholar] [CrossRef]
- Deanfield, J.E.; Halcox, J.P.; Rabelink, T.J. Endothelial Function and Dysfunction. Circulation 2007, 115, 1285–1295. [Google Scholar] [CrossRef]
- Ross, R. Atherosclerosis—An Inflammatory Disease. N. Engl. J. Med. 1999, 340, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Celermajer, D.S.; Sorensen, K.E.; Gooch, V.M.; Spiegelhalter, D.J.; Miller, O.I.; Sullivan, I.D.; Lloyd, J.K.; Deanfield, J.E. Non-Invasive Detection of Endothelial Dysfunction in Children and Adults at Risk of Atherosclerosis. Lancet 1992, 340, 1111–1115. [Google Scholar] [CrossRef]
- Joannides, R.; Haefeli, W.E.; Linder, L.; Richard, V.; Bakkali, E.H.; Thuillez, C.; Lüscher, T.F. Nitric Oxide Is Responsible for Flow-Dependent Dilatation of Human Peripheral Conduit Arteries In Vivo. Circulation 1995, 91, 1314–1319. [Google Scholar] [CrossRef] [PubMed]
- Corretti, M.C.; Anderson, T.J.; Benjamin, E.J.; Celermajer, D.; Charbonneau, F.; Creager, M.A.; Deanfield, J.; Drexler, H.; Gerhard-Herman, M.; Herrington, D.; et al. Guidelines for the Ultrasound Assessment of Endothelial-Dependent Flow-Mediated Vasodilation of the Brachial Artery. J. Am. Coll. Cardiol. 2002, 39, 257–265. [Google Scholar] [CrossRef]
- Mitchell, G.F.; Vita, J.A.; Larson, M.G.; Parise, H.; Keyes, M.J.; Warner, E.; Vasan, R.S.; Levy, D.; Benjamin, E.J. Cross-Sectional Relations of Peripheral Microvascular Function, Cardiovascular Disease Risk Factors, and Aortic Stiffness. Circulation 2005, 112, 3722–3728. [Google Scholar] [CrossRef]
- Hamburg, N.M.; Benjamin, E.J. Assessment of Endothelial Function Using Digital Pulse Amplitude Tonometry. Trends Cardiovasc. Med. 2009, 19, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Cutolo, M.; Sulli, A.; Secchi, M.E.; Paolino, S.; Pizzorni, C. Nailfold Capillaroscopy Is Useful for the Diagnosis and Follow-up of Autoimmune Rheumatic Diseases. A Future Tool for the Analysis of Microvascular Heart Involvement? Rheumatology 2006, 45, iv43–iv46. [Google Scholar] [CrossRef]
- Shah, R.; Petch, J.; Nelson, W.; Roth, K.; Noseworthy, M.D.; Ghassemi, M.; Gerstein, H.C. Nailfold Capillaroscopy and Deep Learning in Diabetes. J. Diabetes 2023, 15, 145–151. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Control | CHD 1 | AF 2 |
|---|---|---|---|
| Number of individuals | 44 | 44 | 44 |
| Number of females | 19 | 14 | 25 |
| Number of males | 25 | 30 | 19 |
| Mean age ± SD (years) | 36.5 ± 18.5 | 70.4 ± 8.7 | 73.3 ± 9.9 |
| Parameter | Control | CHD 1 | AF 2 |
|---|---|---|---|
| Number of individuals | 17 | 11 | 19 |
| Number of females | 6 | 2 | 9 |
| Number of males | 11 | 9 | 10 |
| Mean age ± SD (years) | 39.3 ± 22.4 | 69.9 ± 6.9 | 74.1 ± 9.3 |
| Parameter | Control (N = 44) | CHD 1 (N = 44) | AF 2 (N = 44) |
|---|---|---|---|
| Capillary blood velocity | 1742 ± 884 | 1168 ± 694 | 949 ± 557 |
| Blood aggregate size µm2 | 0 ± 0 | 104 ± 35 | 111 ± 35 |
| Number of aggregates per running mm | 0 ± 0 | 2208 ± 1673 | 2696 ± 1096 |
| Number of blood aggregates per min | 0 ± 0 | 43 ± 39 | 82 ± 63 |
| Parameter | Control (N = 17) | CHD 1 (N = 11) | AF 2 (N = 19) |
|---|---|---|---|
| Capillary blood velocity (µm/s) | 1861 ± 1144 | 1143 ± 603 | 880 ± 601 |
| Blood aggregate size (µm2) | 0 ± 0 | 104 ± 30 | 100 ± 22 |
| Number of aggregates per running mm | 0 ± 0 | 2618 ± 1904 | 3259 ± 864 |
| Number of blood aggregates per min | 0 ± 0 | 42 ± 37 | 68 ± 64 |
| EF 3 measured on the wrist (%) | 38 ± 26 | 3 ± 30 | 19 ± 36 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ermolinskiy, P.; Gurfinkel, Y.; Sovetnikov, E.; Lugovtsov, A.; Priezzhev, A. Correlation between the Capillary Blood Flow Characteristics and Endothelium Function in Healthy Volunteers and Patients Suffering from Coronary Heart Disease and Atrial Fibrillation: A Pilot Study. Life 2023, 13, 2043. https://doi.org/10.3390/life13102043
Ermolinskiy P, Gurfinkel Y, Sovetnikov E, Lugovtsov A, Priezzhev A. Correlation between the Capillary Blood Flow Characteristics and Endothelium Function in Healthy Volunteers and Patients Suffering from Coronary Heart Disease and Atrial Fibrillation: A Pilot Study. Life. 2023; 13(10):2043. https://doi.org/10.3390/life13102043
Chicago/Turabian StyleErmolinskiy, Petr, Yury Gurfinkel, Egor Sovetnikov, Andrei Lugovtsov, and Alexander Priezzhev. 2023. "Correlation between the Capillary Blood Flow Characteristics and Endothelium Function in Healthy Volunteers and Patients Suffering from Coronary Heart Disease and Atrial Fibrillation: A Pilot Study" Life 13, no. 10: 2043. https://doi.org/10.3390/life13102043
APA StyleErmolinskiy, P., Gurfinkel, Y., Sovetnikov, E., Lugovtsov, A., & Priezzhev, A. (2023). Correlation between the Capillary Blood Flow Characteristics and Endothelium Function in Healthy Volunteers and Patients Suffering from Coronary Heart Disease and Atrial Fibrillation: A Pilot Study. Life, 13(10), 2043. https://doi.org/10.3390/life13102043