
Early Detection of Hearing Loss among the Elderly

 , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Population
- -
- Group A comprised individuals aged 55 years and older with normal hearing and balance abilities, characterized by a pure-tone average of 0 to 20 dB across frequencies of 500, 1000, 2000, and 4000 Hz, and demonstrating good static and dynamic balance control.
- -
- Group B consisted of individuals aged 55 years and older who have been diagnosed with a hearing and/or balance disorder but have not undergone treatment, regardless of the reason.
- -
- Group C included individuals aged 55 years and older who have been diagnosed with a hearing and/or balance disorder and have received treatment: with hearing aids (HA), active middle ear implants (AMEIs), bone conduction implants (BCIs), cochlear implants (CIs), or vestibular rehabilitation.
2.2.1. Inclusion Criteria
- -
- The inclusion criteria for Group A required individuals to be aged 55 years or older, possess normal hearing in both ears, exhibit normal balance, demonstrate fluency in the Spanish language for clinical assessment, express willingness to engage in and adhere to all study protocols, and have the capacity to independently consent to participation.
- -
- The inclusion criteria for Group B mandated individuals to be aged 55 years or older, present with abnormal hearing in either ear and/or abnormal balance without receiving appropriate treatment, demonstrate fluency in the Spanish language for clinical evaluation, demonstrate a willingness to engage in and adhere to all study procedures, and have the capacity to independently consent to participation.
- -
- The inclusion criteria for Group C specified the inclusion of individuals aged 55 years or older who are unilateral or bilateral users of HA-BCI-AMEI-CI devices with bilateral hearing loss, received treatment when aged 55 years or older, meet the criteria for hearing aid treatment in one ear and for BCI-AMEI-CI treatment in the other ear, express a willingness to engage in and adhere to all study protocols, demonstrate fluency in the Spanish language for clinical evaluation, and have the capacity to independently consent to participation.
2.2.2. Exclusion Criteria
2.3. Study Measures: Assessment Tools
- -
- Unassisted pure-tone air-conduction audiometry (PTA): This assessment was conducted in soundproof chambers using the Interacoustics brand audiometer, model AC40. Unaided hearing thresholds, measured in decibel hearing level (dBHL) for pure-tone stimuli via air conduction, were assessed using headphones (TDH-39) following standard clinical procedures. Frequencies ranging from 250 to 4000 Hz were evaluated (250–500–1000–2000–4000 Kz), and a pure-tone average was calculated. This routine assessment typically takes around 5 min and involves both the clinician and the participant.
- -
- Speech discrimination assessment in quiet: This assessment was carried out in the participant’s typical listening environment, whether aided binaurally, aided monaurally, unaided in one ear, or unaided bilaterally (i.e., without hearing aid and cochlear implant availability). Standard speech materials were presented at various intensity levels in the sound field to establish the score–intensity function curve, including the presentation of a 65 dB sound pressure level (SPL). Recorded speech stimuli were presented from a loudspeaker at 00 Azimuth, at a distance of 1 m at head level. Disyllabic word lists in Spanish were utilized for this assessment. Results included the percentage of correctly identified speech items at 65 dB SPL and the speech reception threshold level (SRT50%). This evaluation typically lasts 10 to 15 min and involves both the clinician and the participant.
- -
- Routine speech discrimination assessment in noise: This evaluation involves assessing the ability to recognize speech in noisy environments, reflecting the subject’s everyday listening scenario, such as with bilateral hearing aids, one aided ear plus one unaided ear, or entirely unaided (without a hearing aid or cochlear implant). This evaluation is typically conducted for individuals who can accurately comprehend at least 50% of speech in quiet conditions. Testing occurs within a soundproof booth with added background noise. Depending on local protocols, speech materials are either presented adaptively in the sound field to determine the speech reception threshold (SRT) at 50% intelligibility in noise or fixed at a 65-decibel sound pressure level (dBSPL) while varying the background noise (e.g., pink noise) across presentation lists to ascertain the SRT at 50%. Speech samples and background noise are emitted from a speaker located directly ahead at a distance of 1 m from the subject’s head level. The test content typically comprises sentences or words commonly encountered in everyday listening situations in the native aided binaurally. This standard assessment procedure is typically conducted collaboratively by the clinician and the individual being assessed, lasting approximately 10 to 15 min.
- -
- Speech Spatial Qualities (SSQ12): SSQ12 serves as a self-evaluation tool for gauging hearing prowess and communication effectiveness in everyday settings, which is administered to patients [28]. It comprises twelve queries categorized into the following three sections: speech comprehension, spatial hearing (perception of sound in space), and quality (clarity of speech and other sounds), suitable for adults of all age groups and children aged nine and above [29]. Each query employs a rating scale ranging from 0 to 10, with higher scores indicating better proficiency. Typically, the scores are presented as mean ratings for each section, though they can also be analyzed individually or grouped differently, allowing for comparison between two time points. Clinically relevant disparities are identified by a rating shift of 1.0 for each subsection between testing sessions, a commonly observed discrepancy in evaluations of both unaided and aided hearing aid or implant users [30]. The completion of this form generally takes around 10 min for the candidate or recipient. Once completed, the questionnaire was reviewed by an audiology specialist.
- -
- Hearing Handicap Inventory in the Elderly Screening test (HHIE-S): The HHIE-S test is a concise self-evaluation tool tailored to measure the emotional and social impact of hearing loss on the daily lives of older individuals, both before and after receiving hearing-related interventions. It consists of ten questions, split evenly between emotional and social/situational aspects [31]. The total HHIE-S score ranges from 0 (minimal) to 100 (maximum). Scores below 16 in each subsection indicate no significant handicap, while scores falling between 17 and 42 denote a mild to moderate level of handicap, and scores exceeding 43 signify severe handicap. A higher HHIE-S score correlates with a greater degree of handicap caused by hearing impairment. Typically, candidates or recipients can complete this assessment in approximately 5 min. Once completed, the questionnaire was also reviewed by an audiology specialist.
- -
- Digit Symbol Substitution Test (DSST): The DSST is a neurological assessment tool renowned for its sensitivity in detecting brain injury, aging-related cognitive decline, and symptoms of depression, while also evaluating working memory [32]. It comprises a series of digit–symbol pairs (e.g., 1/-, 2/┴, … 7/Λ, 8/X, 9/=) followed by a list of digits. The task for the subject is to match each digit with its corresponding symbol as swiftly as possible. The score is determined by the number of correct symbol matches achieved within the allotted time frame, typically 120 s. Notably, a decline in symbol copying performance exhibits a robust correlation with advancing age. This assessment typically requires around 2 min to complete and is usually administered by a clinician alongside the candidate or recipient. Within the Wechsler Adult Intelligence Scale, this test is referred to as “Digit Symbol” (WAIS-R) or “Digit–Symbol-Coding” (WAIS-IV). An audiology specialist helped the subjects to perform this test.
2.4. Statistical Analysis
3. Results
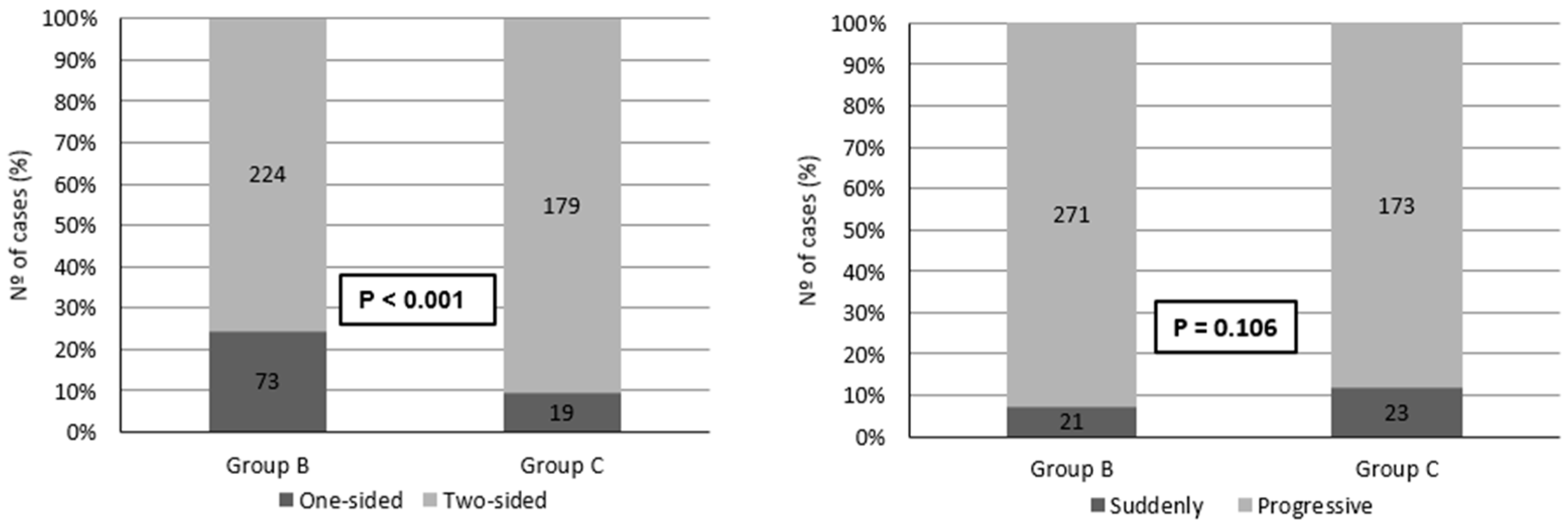
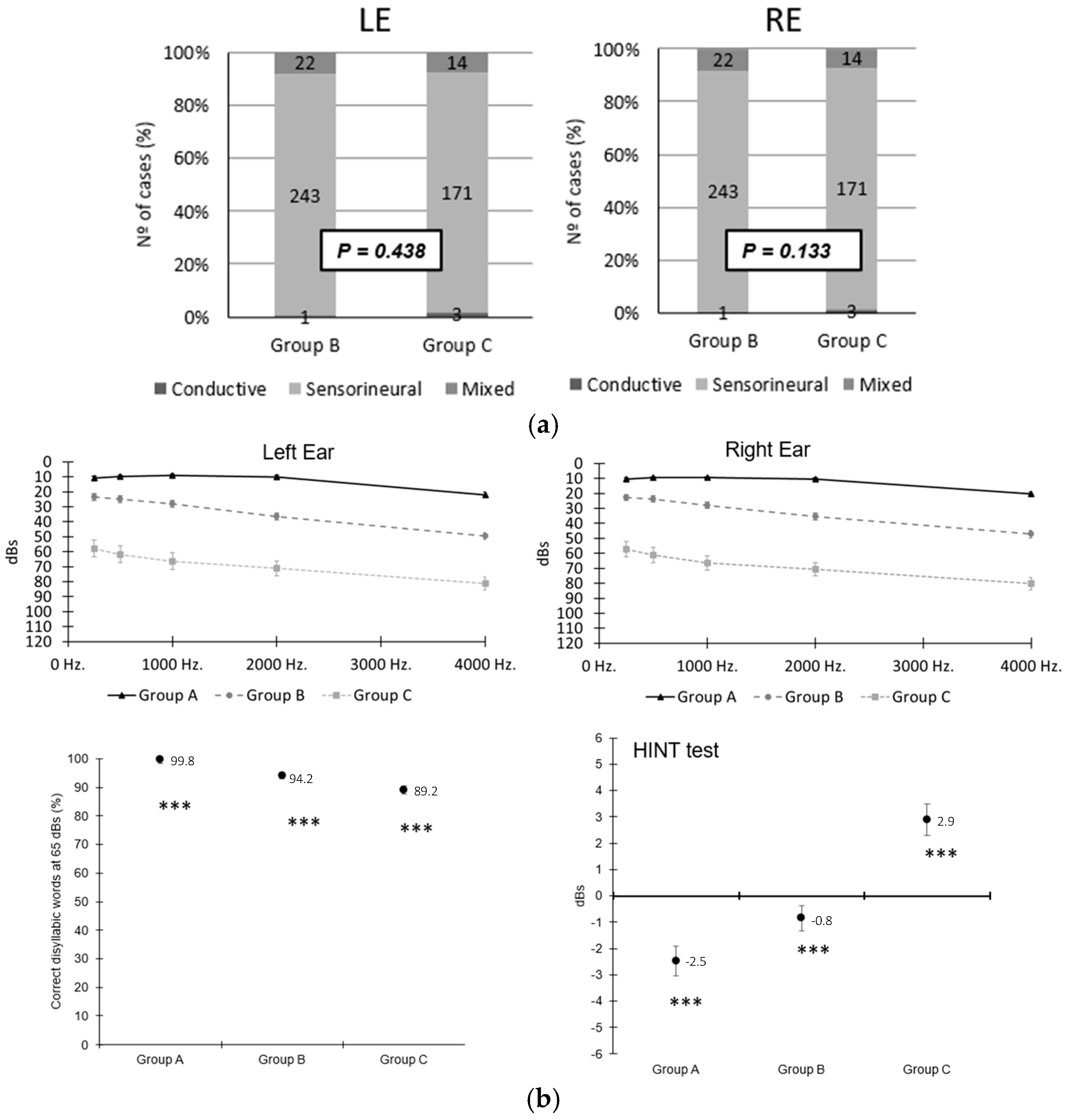
3.1. Auditory Profile of Each Population Group
3.2. Results of Questionnaires
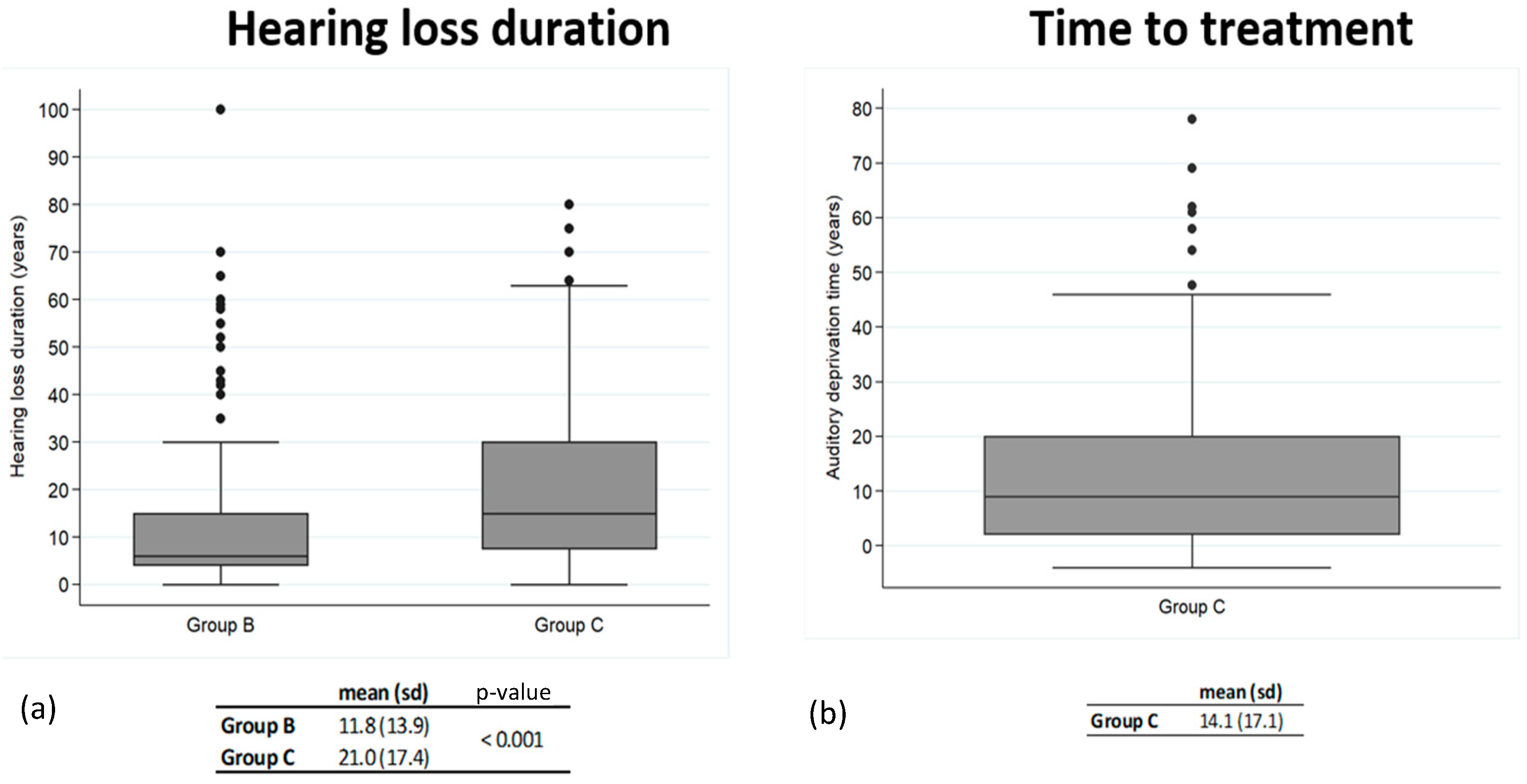
3.3. Correlation between Time-to-Treatment in Group C and Audiometry and Questionnaire Outcomes
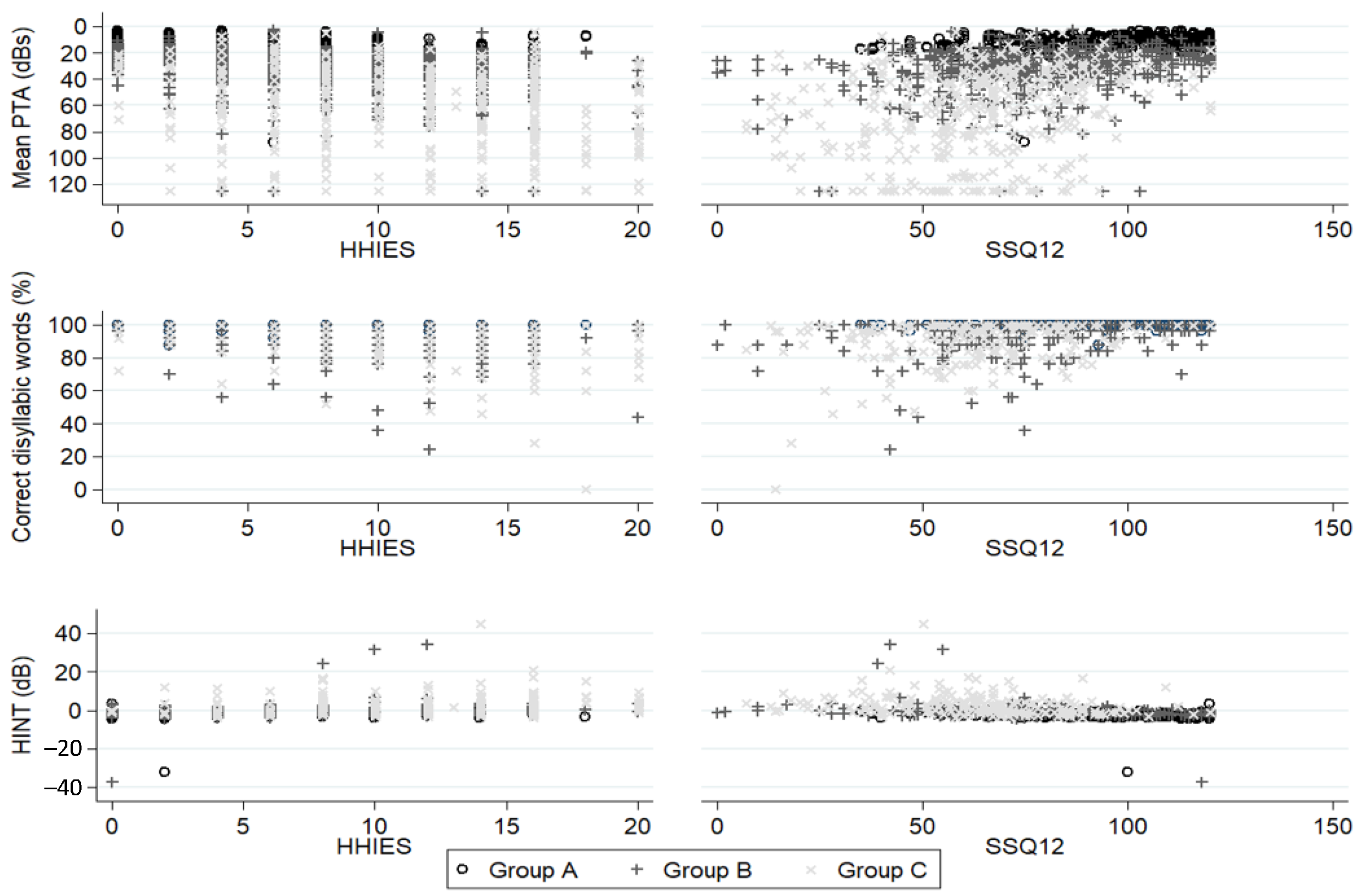
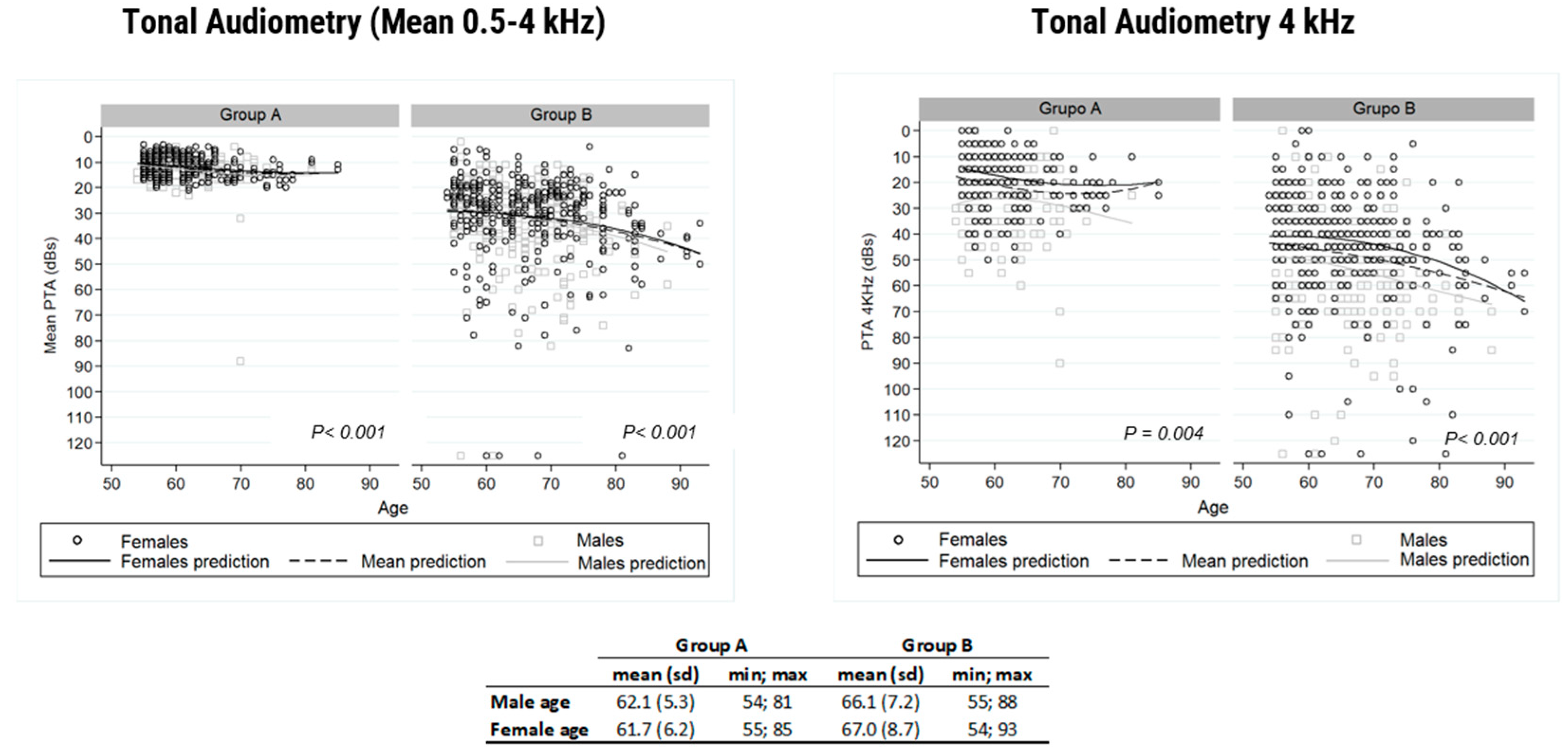
3.4. Correlation between Standard Audiometries, Questionnaires, and Liminar Tone Audiometry at 4 kHz
3.5. Sensitivity and Specificity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roth, T.N.; Hanebuth, D.; Probst, R. Prevalence of age-related hearing loss in Europe: A review. Eur. Arch. Oto-Rhino-Laryngol. 2011, 268, 1101–1107. [Google Scholar] [CrossRef] [PubMed]
- Stevens, G.; Flaxman, S.; Brunskill, E.; Mascarenhas, M.; Mathers, C.D.; Finucane, M.; Global Burden of Disease Hearing Loss Expert Group. Global and regional hearing impairment prevalence: An analysis of 42 studies in 29 countries. Eur. J. Public Health 2013, 23, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Chia, E.-M.; Wang, J.J.; Rochtchina, E.; Cumming, R.R.; Newall, P.; Mitchell, P. Hearing impairment and health-related quality of life: The Blue Mountains Hearing Study. Ear Hear. 2007, 28, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Lin, F.R.; Ferrucci, L. Hearing loss and falls among older adults in the United States. Arch. Intern. Med. 2012, 172, 369–371. [Google Scholar] [CrossRef] [PubMed]
- Hyams, A.V.; Hay-McCutcheon, M.; Scogin, F. Hearing and quality of life in older adults. J. Clin. Psychol. 2018, 74, 1874–1883. [Google Scholar] [CrossRef] [PubMed]
- Jansen, L.A.; van Wier, M.F.; Vernimmen, F.P.J.; Goderie, T.; van de Berg, R.; Lemke, U.; Lissenberg-Witte, B.I.; Kramer, S.E. Ten-year association between change in speech-in-noise recognition and falls due to balance problems: A longitudinal cohort study. BMC Public Heal 2024, 24, 1–14. [Google Scholar] [CrossRef]
- Gopinath, B.; McMahon, C.M.; Burlutsky, G.; Mitchell, P. Hearing and vision impairment and the 5-year incidence of falls in older adults. Age Ageing 2016, 45, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Bigelow, R.T.; Reed, N.S.; Brewster, K.K.; Huang, A.; Rebok, G.; Rutherford, B.R.; Lin, F.R. Association of Hearing Loss With Psychological Distress and Utilization of Mental Health Services Among Adults in the United States. JAMA Netw. Open 2020, 3, e2010986. [Google Scholar] [CrossRef] [PubMed]
- West, J.S. Hearing impairment, social support, and depressive symptoms among U.S. adults: A test of the stress process paradigm. Soc. Sci. Med. 2017, 192, 94–101. [Google Scholar] [CrossRef]
- Jiang, F.; Kuper, H.; Zhou, C.; Qin, W.; Xu, L. Relationship between hearing loss and depression symptoms among older adults in China: The mediating role of social isolation and loneliness. Int. J. Geriatr. Psychiatry 2022, 37. [Google Scholar] [CrossRef]
- Bowl, M.R.; Dawson, S.J. Age-Related Hearing Loss. Cold Spring Harb. Perspect. Med. 2018, 9, a033217. [Google Scholar] [CrossRef] [PubMed]
- Powell, D.S.; Brenowitz, W.D.; Yaffe, K.; Armstrong, N.M.; Reed, N.S.; Lin, F.R.; Gross, A.L.; Deal, J.A. Examining the Combined Estimated Effects of Hearing Loss and Depressive Symptoms on Risk of Cognitive Decline and Incident Dementia. J. Gerontol. B Psychol. Sci. Soc. Sci. 2021, 77, 839–849. [Google Scholar] [CrossRef] [PubMed]
- Uchida, Y.; Sugiura, S.; Nishita, Y.; Saji, N.; Sone, M.; Ueda, H. Age-related hearing loss and cognitive decline — The potential mechanisms linking the two. Auris Nasus Larynx 2018, 46, 1–9. [Google Scholar] [CrossRef]
- Mazlan, R.; Raman, K.; Abdullah, A. A 10-year retrospective analysis of newborn hearing screening in a tertiary hospital in Malaysia. Egypt. J. Otolaryngol. 2022, 38, 1–8. [Google Scholar] [CrossRef]
- Lima Pozzi, R.S.; Pinheiro, M.M.C.; Haas, P.; Hillesheim, D.; de Paiva, K.M. Universal newborn hearing screening program and perinatal and congenital infections in neonates attended in South Brazil. Int. J. Pediatr. Otorhinolaryngol. 2021, 147, 110773. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.Y.; Park, S.-K.; Choi, S.; Chang, J. Analysis of Newborn Hearing Screening Results in South Korea after National Health Insurance Coverage: A Nationwide Population-Based Study. Int. J. Environ. Res. Public Heal 2022, 19, 15052. [Google Scholar] [CrossRef] [PubMed]
- CODEPEH; Núñez, F.; et al. Update of early detection programmes for pediatric hearing loss: 2019 CODEPEH recommendations (Diagnosis, Treatment and Follow-up). In FIAPAS Journal, 171. Special Supplement, 2nd ed.; FIAPAS: Madrid, Spain, 2020. [Google Scholar]
- Irace, A.L.; Sharma, R.K.; Reed, N.S.; Golub, J.S. Smartphone-Based Applications to Detect Hearing Loss: A Review of Current Technology. J. Am. Geriatr. Soc. 2020, 69, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Bauer, M.A.; Sales, A.; Teixeira, A.R.; Morsch, P.; Lessa, A.H.; Bós, Â.J.G. Development and accuracy of a hearing screening application. Braz. J. Otorhinolaryngol. 2020, 87, 711–717. [Google Scholar] [CrossRef]
- Manrique, M.; Batuecas, A.; Cenjor, C.; Ferrán, S.; Gómez, J.R.; Lorenzo, A.I.; Marco, J.; Matiñó, E.; Morant, A.; Morera, C.; et al. Presbiacusia y trastornos del equilibrio en personas mayores. Revisión de aspectos etiopatogénicos, consecuencias sobre calidad de vida y efectos positivos de su tratamiento. Act. Esp. Otorrinolaringol. 2022, 74, 124–132. [Google Scholar] [CrossRef]
- Liberman, M.C.; Kujawa, S.G. Cochlear synaptopathy in acquired sensorineural hearing loss: Manifestations and mechanisms. Hear. Res. 2017, 349, 138–147. [Google Scholar] [CrossRef]
- Mepani, A.M.; Verhulst, S.; Hancock, K.E.; Garrett, M.; Vasilkov, V.; Bennett, K.; de Gruttola, V.; Liberman, M.C.; Maison, S.F. Envelope following responses predict speech-in-noise performance in normal-hearing listeners. J. Neurophysiol. 2021, 125, 1213–1222. [Google Scholar] [CrossRef]
- Parthasarathy, A.; Kujawa, S.G. Synaptopathy in the Aging Cochlea: Characterizing Early-Neural Deficits in Auditory Temporal Envelope Processing. J. Neurosci. 2018, 38, 7108–7119. [Google Scholar] [CrossRef] [PubMed]
- Fischer, N.; Chacko, L.J.; Glueckert, R.; Schrott-Fischer, A. Age-Dependent Changes in the Cochlea. Gerontology 2019, 66, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Murphy, C.F.B.; Rabelo, C.M.; Silagi, M.L.; Mansur, L.L.; Bamiou, D.E.; Schochat, E. Auditory Processing Performance of the Middle-Aged and Elderly: Auditory or Cognitive Decline? J. Am. Acad. Audiol. 2018, 29, 005–014. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, T.D.; Lad, M.; Kumar, S.; Holmes, E.; McMurray, B.; Maguire, E.A.; Billig, A.J.; Sedley, W. How Can Hearing Loss Cause Dementia? Neuron 2020, 108, 401–412. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.C.S.; Marshall, C.R.; Weil, R.S.; Bamiou, D.-E.; Hardy, C.J.D. Hearing and dementia: From ears to brain. Brain 2020, 144, 391–401. [Google Scholar] [CrossRef] [PubMed]
- Noble, W.; Gatehouse, S. Interaural asymmetry of hearing loss, Speech, Spatial and Qualities of Hearing Scale (SSQ) disabilities and handicap. Int. J. Audiol. 2004, 43, 100–114. [Google Scholar] [CrossRef] [PubMed]
- Gatehouse, S.; Noble, W. The speech, spatial and qualities of hearing scale (SSQ). Int. J. Audiol. 2004, 43, 85–99. [Google Scholar] [CrossRef]
- Noble, W.; Gatehouse, S. Effects of bilateral versus unilateral hearing aid fitting on abilities measured by the Speech, Spatial, and Qualities of Hearing scale (SSQ). Int. J. Audiol. 2006, 45, 172–181. [Google Scholar] [CrossRef]
- Newman, C.W.; Jacobson, G.P.; Hug, G.A.; Weinstein, B.E.; Malinoff, R.L. Practical Method for Quantifying Hearing Aid Benefit in Older Adults. J. Am. Acad. Audiol. 1991, 2, 70–75. [Google Scholar]
- Jaeger, J. Digit Symbol Substitution Test: The Case for Sensitivity Over Specificity in Neuropsychological Testing. J. Clin. Psychopharmacol. 2018, 38, 513–519. [Google Scholar] [CrossRef] [PubMed]
- de Lima, J.P.; Manrique-Huarte, R.; Ferran, S.; Mallmann, F.; Gil, D.C.; Barrenechea, B.A.; Huarte, A.; Madrid, M.A.G.; Manrique, M. Hearing and Balance in Healthy Aging Project: Characterization of Hearing, Balance, and Other Associated Disorders in Three Population Groups Aged 55 and Over. Audiol. Neurotol. 2024; Epub ahead of print. 1–16. [Google Scholar] [CrossRef]
- WHO. Available online: http://www.who.int/mediacentre/news/releases/2017/vector-control-ncds-cancer/es/ (accessed on 3 January 2024).
- Dobrow, M.J.; Hagens, V.; Chafe, R.; Sullivan, T.; Rabeneck, L. Consolidated principles for screening based on a systematic review and consensus process. Can. Med. Assoc. J. 2018, 190, E422–E429. [Google Scholar] [CrossRef] [PubMed]
- Feltner, C.; Wallace, I.F.; Kistler, C.E.; Coker-Schwimmer, M.; Jonas, D.E. Screening for hearing loss in older adults: Updated evidence reports and systematic review for the US Preventive Services Task Force. JAMA 2021, 325, 1202–1215. [Google Scholar] [CrossRef] [PubMed]
- Chien, W.; Lin, F.R. Prevalence of Hearing Aid Use Among Older Adults in the United States. Arch. Intern. Med. 2012, 172, 292–293. [Google Scholar] [CrossRef] [PubMed]
- Michels, T.C.; Duffy, M.T.; Rogers, D.J. Hearing Loss in Adults: Differential Diagnosis and Treatment. Am. Fam. Physician 2019, 100, 98–108. [Google Scholar] [PubMed]
- Manrique, M.; Batuecas, A.; Cenjor, C.; Ferrán, S.; Gómez, J.R.; Lorenzo, A.I.; Marco, J.; Matiñó, E.; Miralles, R.; Morant, A.; et al. Documento sobre fragilidad e hipoacusia. Com. Científico GAES-Amplifon 2021. [Google Scholar]
- Huddle, M.G.; Goman, A.M.; Kernizan, F.C.; Foley, D.M.; Price, C.; Frick, K.D.; Lin, F.R. The Economic Impact of Adult Hearing Loss: A Systematic Review. JAMA Otolaryngol. Head. Neck Surg. 2017, 143, 1040–1048. [Google Scholar] [CrossRef] [PubMed]
- Ye, X.; Zhu, D.; Chen, S.; He, P. Cost-Effectiveness Analysis of Hearing Aids for Middle-Aged and Older Adults in China: A Randomized Controlled Trial. Otol. Neurotol. 2023, 44, e456–e462. [Google Scholar] [CrossRef]
- Hsu, A.K.; Bassett, S.M.; O’dwyer, L.C.; McHugh, M.; Heinemann, A.W.; Jordan, N.; Dhar, S. Cost-Effectiveness of Hearing Screening in Older Adults: A Scoping Review. Res. Aging 2021, 44, 186–204. [Google Scholar] [CrossRef]
- Joore, M.A.; van der Stel, H.; Peters, H.J.M. The cost-effectiveness of hearing-aid fitting in the Netherlands. Arch. Otolaryngol.-Head Neck Surg. 2003, 129, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Chisolm, T.H.; Johnson, C.E.; Danhauer, J.L.; Portz, L.J.; Abrams, H.B.; Lesner, S.; McCarthy, P.A.; Newman, C.W. A systematic review of health-related quality of life and hearing aids: Final report of the American Academy of Audiology task force on the health-related quality of life benefits of amplification in adults. J. Am. Acad. Audiol. 2007, 18, 151–183. [Google Scholar] [CrossRef] [PubMed]
- Ciorba, A.; Bianchini, C.; Pelucchi, S.; Pastore, A. The impact of hearing loss on the quality of life of elderly adults. Clin. Interv. Aging 2012, 7, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Kochkin, S.; Rogin, C. Quantifying the obvious: The impact of hearing instruments on quality of life. Hear. Rev. 2000, 7, 6–34. [Google Scholar]
- Fisher, D.; Li, C.-M.; Chiu, M.S.; Themann, C.L.; Petersen, H.; Jónasson, F.; Jónsson, P.V.; Sverrisdottir, J.E.; Garcia, M.; Harris, T.B.; et al. Impairments in Hearing and Vision Impact on Mortality in Older People. AGES-Reyk. Study Age Ageing 2014, 43, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Contrera, K.J.; Betz, J.; Genther, D.J.; Lin, F.R. Association of Hearing Impairment and Mortality in the National Health and Nutrition Examination Survey. JAMA Otolaryngol. Head Neck. Surg. 2015, 141, 944–946. [Google Scholar] [CrossRef] [PubMed]
- Saito, H.; Nishiwaki, Y.; Michikawa, T.; Kikuchi, Y.; Mizutari, K.; Takebayashi, T.; Ogawa, K. Hearing handicap predicts the development of depressive symptoms after three years in older community-dwelling Japanese. J. Am. Geriatr. Soc. 2010, 58, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Amieva, H.; Ouvrard, C.; Giulioli, C.; Meillon, C.; Rullie, R.L.; Dartigues, J.F. Self-Reported Hearing Loss, Hearing Aids, and Cognitive Decline in Elderly Adults: A 25-Year Study. J. Am. Geriatr. Soc. 2015, 63, 2099–2104. [Google Scholar] [CrossRef] [PubMed]
- Mosnier, I.; Bebear, J.-P.; Marx, M.; Fraysse, B.; Truy, E.; Lina-Granade, G.; Mondain, M.; Sterkers-Artières, F.; Bordure, P.; Robier, A.; et al. Predictive factors of cochlear implant outcomes in the elderly. Audiol. Neurotol. 2014, 19 (Suppl. S1), 15–20. [Google Scholar] [CrossRef]
- Manrique, R.; Calavia, D.; Huarte, A.; Girón, L.; Manrique, M. Treatment for hearing loss among the elderly: Auditory outcomes and Impact on quality of life. Audiol. Neurotol. 2016, 21 (Suppl. S1), 26–35. [Google Scholar] [CrossRef]
- Huarte, A.; Lezaun, R.; Manrique, M. Quality of life outcomes for cochlear implantation in the elderly. Audiol. Neurotol. 2014, 19, 36–39. [Google Scholar] [CrossRef]
- Crowson, M.G.; Semenov, Y.R.; Tucci, D.L.; Niparko, J.K. Quality of Life and Cost-Effectiveness of Cochlear Implants: A Narrative Review. Audiol. Neurotol. 2017, 22, 236–258. [Google Scholar] [CrossRef] [PubMed]
- Turchetti, G.; Bellelli, S.; Palla, I.; Berrettini, S. Systematic review of the scientific literature on the economic evaluation of cochlear implants in adult patients. ACTA Otorhinolaryngol. Ita. Lica. 2011, 31, 319–327. [Google Scholar]
- Campbell, J.; Sharma, A. Cross-Modal Re-Organization in Adults with Early Stage Hearing Loss. PLoS ONE 2014, 9, e90594. [Google Scholar] [CrossRef]
- Bisgaard, N.; Zimmer, S.; Laureyns, M.; Groth, J. A model for estimating hearing aid coverage world-wide using historical data on hearing aid sales. Int. J. Audiol. 2021, 61, 841–849. [Google Scholar] [CrossRef]
- Hall, D.A.; Kitterick, P.; Heffernan, E.; Fackrell, K.; Lucas, L.; Ferguson, M. How Do We Know That Our Patients Have Benefitted from Our ENT/Audiological Interventions? Presented at the Annual Meeting of ADANO 2016 in Berlin. Otol. Neurotol. 2019, 40, e474–e481. [Google Scholar] [CrossRef] [PubMed]
- Oremule, B.; Abbas, J.; Saunders, G.; Kluk, K.; Isba, R.; Bate, S.; Bruce, I. Mobile audiometry for hearing threshold assessment: A systematic review and meta-analysis. Clin. Otolaryngol. 2023, 49, 74–86. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Chracteristics | Group A (n = 210) | Group B (n = 302) | Group C (n = 198) | p-Value |
|---|---|---|---|---|
| Gender (M/F) | 61% F | 55% F | 44% F | p < 0.010 |
| Age | 61 y | 66 y | 68 y | p < 0.001 |
| Habitat (rural/urban) | 83% urban | 78% urban | 73% urban | NSD |
| Assistance (none/family) | 99% none | 97% none | 98% none | NSD |
| Education level | 50% university | 38% university | 28% university | p < 0.001 |
| Languages (mono/plurilingual) | 66% monolingual | 70% monolingual | 77% monolingual | p < 0.050 |
| Work activity | 53% yes | 34% yes | 29% yes | p < 0.001 |
| Tobacco | 55% no | 47% no | 45% no | NSD |
| Cardiovascular disease | 28% yes | 31% yes | 31% yes | NSD |
| Psychiatric disease | 18% yes | 21% yes | 18% yes | NSD |
| Neurological disease | 4% yes | 8% yes | 9% yes | NSD |
| Endocrine disease | 31% yes | 31% yes | 32 yes | NSD |
| Mobility (normal/assisted) | 1% assisted | 2% assisted | 5% assisted | NSD |
| PTA | 500 Hz | 1000 Hz | 2000 Hz | 4000 Hz | Total (dB) |
|---|---|---|---|---|---|
| Group A | 9.7 dB (6.6) (0; 90) | 9.3 dB (6.2) (0; 85) | 10.3 dB (8.0) (0; 85) | 21.2 dB (12.3) (0; 90) | 12.6 dB (5.9) (2.5; 87.5) |
| Group B | 24.2 dB (18.9) (0; 120) | 28.0 dB (19.1) (0; 120) | 35.9 dB (19.8) (0; 125) | 48.4 dB (20.5) (0; 120) | 34.1 dB (16.9) (1.2; 120) |
| Group C | 61.4 dB (38.2) (0; 120) | 66.4 dB (36.9) (5; 120) | 70.9 dB (33.8) (0; 125) | 80.8 dB (31.6) (0; 120) | 69.8 dB (33.5) (3.7; 120) |
| Speech Audiometry in Quiet | Speech Audiometry in Noise (Hint Test) | ||||
| Group A | 99.8% (1.1) (88; 100) | Group A | −2.5 dB (1.0) (−4.4; 3.2) | ||
| Group B | 94.2% (10.6) (24; 100) | Group B | −0.8 dB (3.6) (−4.2; 34.0) | ||
| Group C | 89.2% (14.1) (0; 100) | Group C | 2.9 dB (5.5) (−3.5; 45.0) | ||
| HHIE-S Total | Total (Range 0–120) 7.1 (5.7) (0; 20) | SSQ12 | Total (Range 0–120) 78.9 (25.0) (0; 120) | ||
| Group A | 2.9 (3.8) (0; 18) | Group A | 94.8 (19.7) (35; 120) | ||
| Group B | 7.3 (4.9) (0; 20) | Group B | 78.3 (23.4) (0; 120) | ||
| Group C | 11.5 (5.7) (0; 20) | Group C | 63.1 (22.1) (7; 120) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferrán, S.; Manrique-Huarte, R.; Lima, J.P.; Rodríguez-Zanetti, C.; Calavia, D.; Andrade, C.J.; Terrasa, D.; Huarte, A.; Manrique, M. Early Detection of Hearing Loss among the Elderly. Life 2024, 14, 471. https://doi.org/10.3390/life14040471
Ferrán S, Manrique-Huarte R, Lima JP, Rodríguez-Zanetti C, Calavia D, Andrade CJ, Terrasa D, Huarte A, Manrique M. Early Detection of Hearing Loss among the Elderly. Life. 2024; 14(4):471. https://doi.org/10.3390/life14040471
Chicago/Turabian StyleFerrán, Sol, Raquel Manrique-Huarte, Janaina P. Lima, Carla Rodríguez-Zanetti, Diego Calavia, Constanza Jimena Andrade, David Terrasa, Alicia Huarte, and Manuel Manrique. 2024. "Early Detection of Hearing Loss among the Elderly" Life 14, no. 4: 471. https://doi.org/10.3390/life14040471
APA StyleFerrán, S., Manrique-Huarte, R., Lima, J. P., Rodríguez-Zanetti, C., Calavia, D., Andrade, C. J., Terrasa, D., Huarte, A., & Manrique, M. (2024). Early Detection of Hearing Loss among the Elderly. Life, 14(4), 471. https://doi.org/10.3390/life14040471