

Associations of Ultrasound Findings with Serum Iron and Ferritin Levels in Children with Obesity

 , ,
, ,  , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Children Assessment
2.6. Measurements
2.7. Laboratory Tests
2.8. Imagistic Result
2.9. Statistical Analysis
2.10. Ethical Principles
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| COVID-19 | Coronavirus disease 2019 |
| TNF-α | Tumor necrosis factor |
| IL-6 | Interleukin-6 |
| NAFLD | Non-alcoholic fatty liver disease |
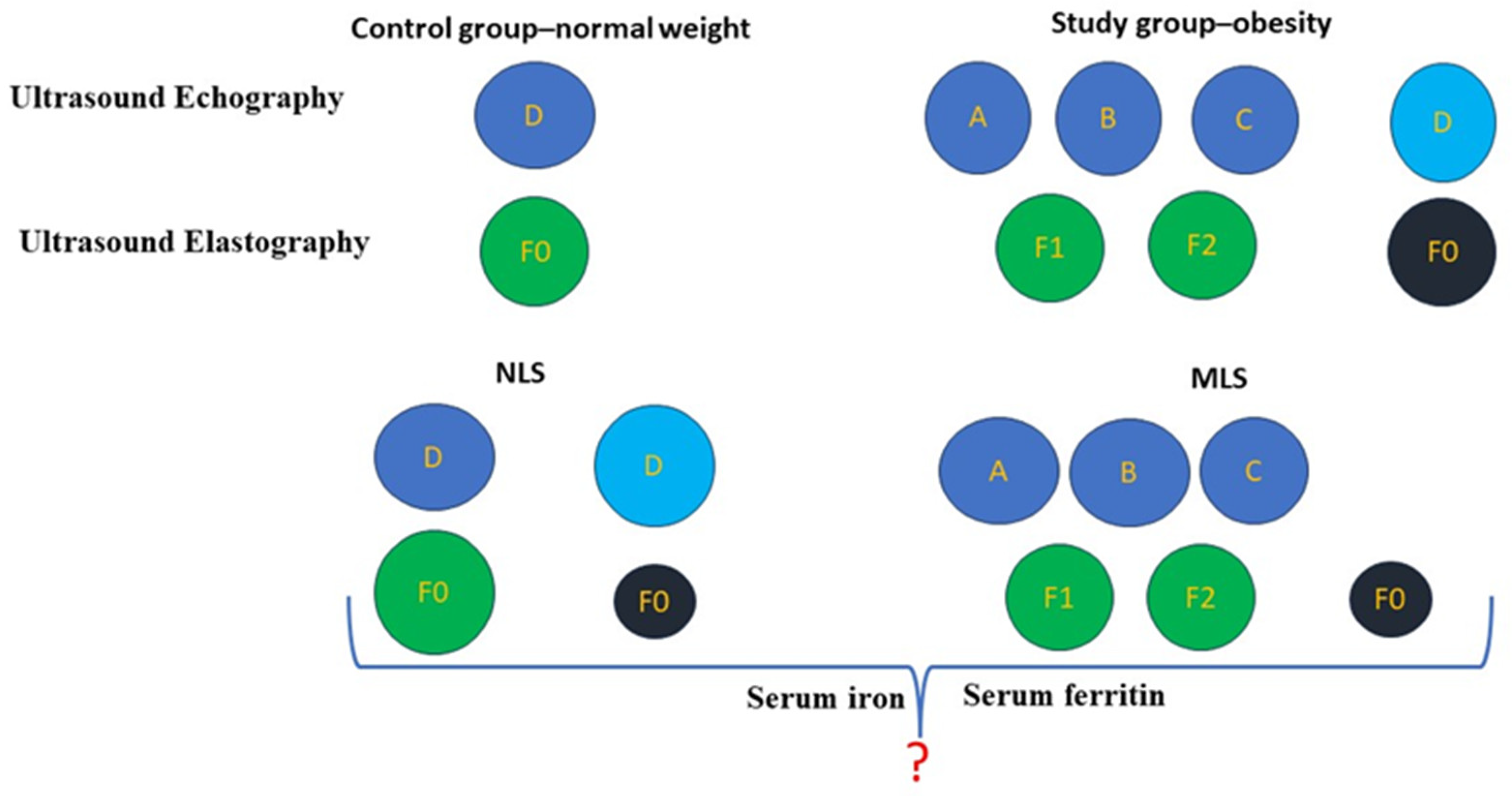
| NLS | Normal Liver Structure |
| MLS | Modified Liver Structure |
| BMI | Body mass index |
| WHO | World Health Organization |
| NASH | Non-Alcoholic Steatohepatitis |
| MRI | Magnetic Resonance Imaging |
References
- Jebeile, H.; Kelly, A.S.; O’Malley, G.; Baur, L.A. Obesity in children and adolescents: Epidemiology, causes, assessment, and management. Lancet Diabetes Endocrinol. 2022, 10, 351–365. [Google Scholar] [CrossRef]
- Kozioł-Kozakowska, A.; Januś, D.; Stępniewska, A.; Szczudlik, E.; Stochel-Gaudyn, A.; Wójcik, M. Beyond the Metabolic Syndrome: Non-Obvious Complications of Obesity in Children. Children 2023, 10, 1905. [Google Scholar] [CrossRef]
- Horesh, A.; Tsur, A.M.; Bardugo, A.; Twig, G. Adolescent and childhood obesity and excess morbidity and mortality in young adulthood—A systematic review. Curr. Obes. Rep. 2021, 10, 301–310. [Google Scholar] [CrossRef]
- Mihuta, M.S.; Paul, C.; Borlea, A.; Roi, C.M.; Velea-Barta, O.-A.; Mozos, I.; Stoian, D. Unveiling the Silent Danger of Childhood Obesity: Non-Invasive Biomarkers Such as Carotid Intima-Media Thickness, Arterial Stiffness Surrogate Markers, and Blood Pressure Are Useful in Detecting Early Vascular Alterations in Obese Children. Biomedicines 2023, 11, 1841. [Google Scholar] [CrossRef]
- Becheanu, C.A.; Smădeanu, R.E.; Ţincu, I.F. Effect of a Symbiotic Mixture on Fecal Microbiota in Pediatric Patients Suffering of Functional Abdominal Pain Disorders. Processes 2021, 9, 2157. [Google Scholar] [CrossRef]
- Močnik, M.; Marčun Varda, N. Ultrasound Elastography in Children. Children 2023, 10, 1296. [Google Scholar] [CrossRef]
- Mentzel, H.J.; Glutig, K.; Gräger, S.; Krüger, P.C.; Waginger, M. Ultrasound elastography in children—Nice to have for scientific studies or arrived in clinical routine? Mol. Cell. Pediatr. 2022, 9, 11. [Google Scholar] [CrossRef]
- Mörwald, K.; Aigner, E.; Bergsten, P.; Brunner, S.M.; Forslund, A.; Kullberg, J.; Ahlström, H.; Manell, H.; Roomp, K.; Schütz, S.; et al. Serum Ferritin Correlates with Liver Fat in Male Adolescents with Obesity. Front. Endocrinol. 2020, 11, 340. [Google Scholar] [CrossRef]
- Berton, P.F.; Gambero, A. Hepcidin and inflammation associated with iron deficiency in childhood obesity—A systematic review. J. Pediatr. 2023, 100, 124–131. [Google Scholar] [CrossRef]
- Alshwaiyat, N.M.; Ahmad, A.; Wan Hassan, W.; Al-Jamal, H.A. Association between obesity and iron deficiency (Review). Exp. Ther. Med. 2021, 22, 1268. [Google Scholar] [CrossRef]
- Zhang, J.; Cao, J.; Xu, H.; Dong, G.; Huang, K.; Wu, W.; Ye, J.; Fu, J. Ferritin as a key risk factor for nonalcoholic fatty liver disease in children with obesity. J. Clin. Lab. Anal. 2020, 35, e23602. [Google Scholar] [CrossRef] [PubMed]
- Sanad, M.; Osman, M.; Gharib, A. Obesity modulate serum hepcidin and treatment outcome of iron deficiency anemia in children: A case control study. Ital. J. Pediatr. 2011, 37, 34. [Google Scholar] [CrossRef]
- Peng, L.; Wu, S.; Zhou, N.; Zhu, S.; Liu, Q.; Li, X. Clinical characteristics and risk factors of nonalcoholic fatty liver disease in children with obesity. BMC Pediatr. 2021, 21, 122. [Google Scholar] [CrossRef]
- Kolodziejczyk, A.A.; Zheng, D.; Shibolet, O.; Elinav, E. The Role of the Microbiome in NAFLD and NASH. EMBO Mol. Med. 2019, 11, e9302. [Google Scholar] [CrossRef] [PubMed]
- Barchetta, I.; Cimini, F.A.; Cavallo, M.G. Vitamin D and Metabolic Dysfunction-Associated Fatty Liver Disease (MAFLD): An Update. Nutrients 2020, 12, 3302. [Google Scholar] [CrossRef]
- Lister, N.B.; Baur, L.A.; Felix, J.F.; Hill, A.J.; Marcus, C.; Reinehr, T.; Summerbell, C.; Wabitsch, M. Child and adolescent obesity. Nat. Rev. Dis. Primers 2023, 9, 24. [Google Scholar] [CrossRef] [PubMed]
- Orsini, F.; D’Ambrosio, F.; Scardigno, A.; Ricciardi, R.; Calabrò, G.E. Epidemiological Impact of Metabolic Syndrome in Overweight and Obese European Children and Adolescents: A Systematic Literature Review. Nutrients 2023, 15, 3895. [Google Scholar] [CrossRef]
- Lourenço, L.P.; Viola, P.C.A.F.; Franceschini, S.D.C.C.; Rosa, C.O.B.; Ribeiro, S.A.V. Metabolic syndrome and risk factors in children: A risk score proposal. Eur. J. Clin. Nutr. 2023, 77, 278–282. [Google Scholar] [CrossRef]
- Papachristodoulou, A.; Kavvadas, D.; Karamitsos, A.; Papamitsou, T.; Chatzidimitriou, M.; Sioga, A. Diagnosis and Staging of Pediatric Non-Alcoholic Fatty Liver Disease: Is Classical Ultrasound the Answer? Pediatr. Rep. 2021, 13, 312–321. [Google Scholar] [CrossRef]
- D’Hondt, A.; Rubesova, E.; Xie, H.; Shamdasani, V.; Barth, R.A. Liver fat quantification by ultrasound in children: A prospective study. AJR Am. J. Roentgenol. 2021, 217, 996–1006. [Google Scholar] [CrossRef]
- Chuang, Y.H.; Hsieh, C.S.; Lai, M.W.; Chen, C.C.; Chao, H.C.; Yeh, H.Y.; Lai, H.; Tsui, P.H. Detection of pediatric hepatic steatosis through ultrasound backscattering analysis. Eur. Radiol. 2021, 5, 3216–3225. [Google Scholar] [CrossRef] [PubMed]
- Ferraioli, G.; Calcaterra, V.; Lissandrin, R.; Guazzotti, M.; Maiocchi, L.; Tinelli, C.; De Silvestri, A.; Regalbuto, C.; Pelizzo, G.; Larizza, D.; et al. Noninvasive assessment of liver steatosis in children: The clinical value of controlled attenuation parameter. BMC Gastroenterol. 2017, 17, 61. [Google Scholar] [CrossRef] [PubMed]
- Pasini, E.; Corsetti, G.; Romano, C.; Aquilani, R.; Scarabelli, T.; Chen-Scarabelli, C.; Dioguardi, F.S. Management of Anaemia of Chronic Disease: Beyond Iron-Only Supplementation. Nutrients 2021, 13, 237. [Google Scholar] [CrossRef] [PubMed]
- Yan, J.; Guan, T.; Guo, M.; Liu, J. Serum Ferritin and Non-alcoholic Fatty Liver Disease: A Meta-analysis and Systematic Review. Turk. J. Gastroenterol. 2023, 34, 952–960. [Google Scholar] [CrossRef] [PubMed]
- Du, S.X.; Lu, L.L.; Geng, N.; Victor, D.W.; Chen, L.Z.; Wang, C.; Yue, H.Y.; Xin, Y.N.; Xuan, S.Y.; Jin, W.W. Association of serum ferritin with non-alcoholic fatty liver disease: A meta-analysis. Lipids Health Dis. 2017, 16, 228. [Google Scholar] [CrossRef] [PubMed]
- Aigner, E.; Feldman, A.; Datz, C. Obesity as an Emerging Risk Factor for Iron Deficiency. Nutrients 2014, 6, 3587–3600. [Google Scholar]
- Amato, A.; Santoro, N.; Calabro, P.; Grandone, A.; Swinkels, D.W.; Perrone, L.; del Giudice, E.M. Effect of body mass index reduction on serum hepcidin levels and iron status in obese children. Int. J. Obes. 2005, 34, 1772–1774. [Google Scholar]
- Huang, Y.-F.; Tok, T.-S.; Lu, C.-L.; Ko, H.-C.; Chen, M.-Y.; Chen, S.C.-C. Relationship between being overweight and iron deficiency in adolescents. Pediatr. Neonatol. 2015, 56, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Shattnawi, K.K.; Alomari, M.A.; Al-Sheyab, N.; Salameh, A.B. The relationship between plasma ferritin levels and body mass index among adolescents. Sci. Rep. 2018, 8, 15307. [Google Scholar] [CrossRef] [PubMed]
- Di Martino, M.; Koryukova, K.; Bezzi, M.; Catalano, C. Imaging Features of Non-Alcoholic Fatty Liver Disease in Children and Adolescents. Children 2017, 4, 73. [Google Scholar] [CrossRef]
- Villani, R.; Lupo, P.; Sangineto, M.; Romano, A.D.; Serviddio, G. Liver Ultrasound Elastography in Non-Alcoholic Fatty Liver Disease: A State-of-the-Art Summary. Diagnostics 2023, 13, 1236. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameters% (No. Cases) (%) | Normal Weight | Obesity | p Value (x2 Test) | ||
|---|---|---|---|---|---|
| Age | 6–9 years | 14 (53.8%) | 34 (47.2%) | p > 0.05 | |
| 10–14 years | 12 (46.2%) | 38 (52.8%) | |||
| Gender | Female | 11 (42.3%) | 29 (40.3%) | p > 0.05 | |
| Male | 15 (57.7%) | 43 (59.7%) | |||
| Environment | Urban | 10 (38.5%) | 41 (56.9%) | p > 0.05 | |
| Rural | 16 (61.5%) | 31 (43.1%) | |||
| BMI | 16.7 ± 1.2 | 27 ± 3.8 | |||
| Ultrasound Elastography | kPa | 2.9 ± 0.5 | 5.1 ± 1.7 | p < 0.001 | |
| Fibrosis score | F0 | 26 (100%) | 42 (58.3%) | ||
| F1 | 0 | 13 (18.1%) | |||
| F2 | 0 | 17 (23.6%) | |||
| Ultrasound Echography | Score A | 0 | 8 (11.1%) | p < 0.001 | |
| Score B | 0 | 25 (34.7%) | |||
| Score C | 0 | 17 (23.6%) | |||
| Score D | 26 (100%) | 22 (30.6%) | |||
| Serum iron | μg/dL | 63.8 ± 20.5 | 14.5 ± 11.9 | p < 0.001 | |
| Deficit | 3 (11.5%) | 67 (93.1%) | |||
| Serum ferritin | ng/mL | 49.5 ± 29.5 | 187.2 ± 36.2 | p < 0.001 | |
| Increased | 2 (7.7%) | 69 (95.8%) | |||
| Parameters% (No. Cases) (%) | NLS | MLS | p Value | |
|---|---|---|---|---|
| Age (years) 6–9 years 10–14 years | 9.4 ± 2 | 9.8 ± 2.2 | p > 0.05 | |
| 23 (47.9%) | 25 (50%) | |||
| 25 (52.1%) | 25 (50%) | |||
| BMI | 20.7 ± 4.7 | 27.7 ± 4.2 | p < 0.001 | |
| Normal weight | 26 (26.5%) | 0 | ||
| Obesity | 22 (22.4%) | 50 (51.1%) | ||
| Serum Fe | μg/dL | 45.4 ± 27.6 | 10.5 ± 5.2 | p < 0.001 |
| Deficit | 22 (22.4%) | 48 (48.9%) | ||
| Serum Ferritin | ng/mL | 97.6 ± 60.8 | 201.7 ± 28 | p < 0.001 |
| Increased | 22 (22.4%) | 49 (50%) | ||
| Parameters% (No. Cases) (%) | Ultrasound Echography | p Value | |||||
|---|---|---|---|---|---|---|---|
| MSL | NSL | ||||||
| Total | Score A | Score B | Score C | Score D | |||
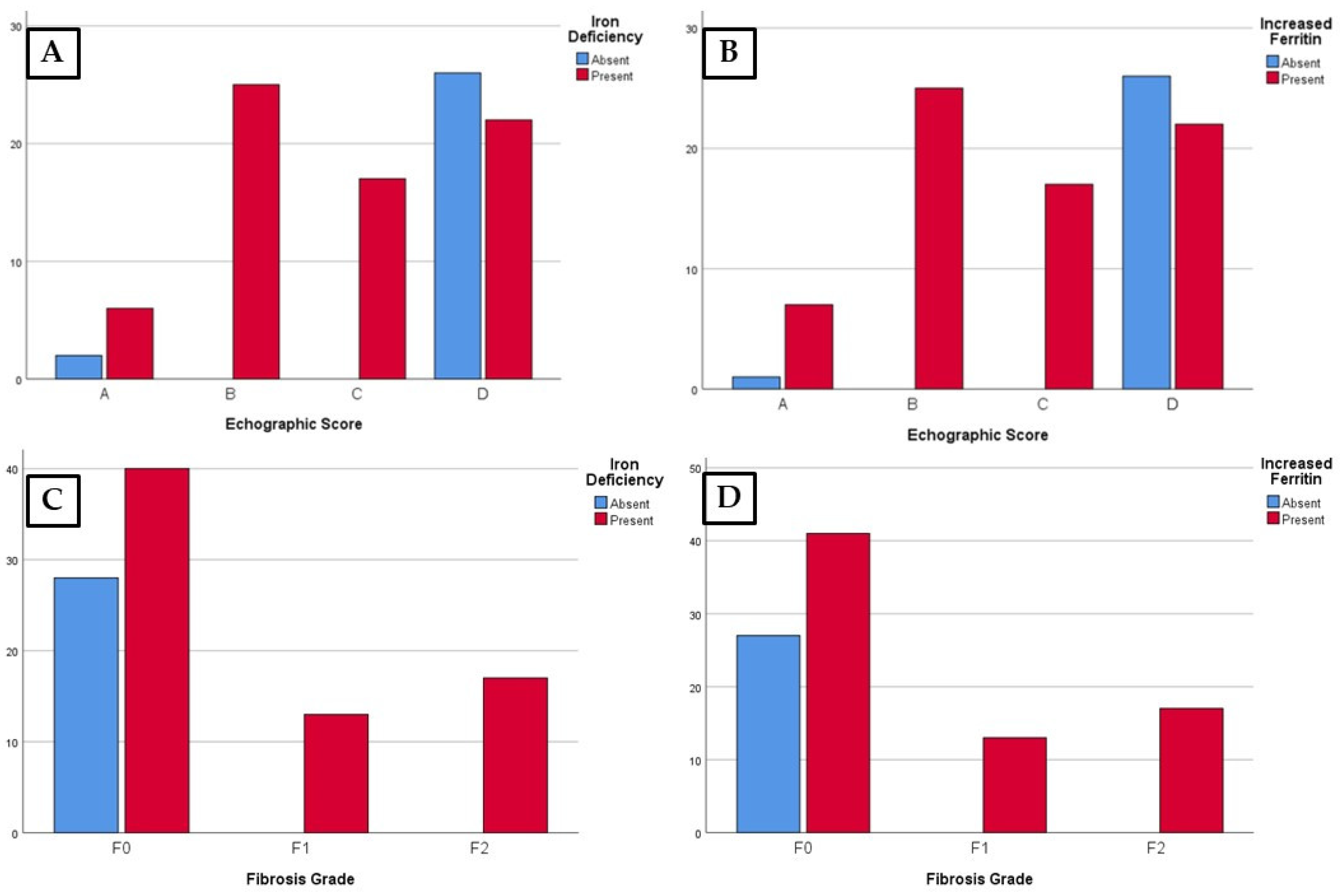
| Serum iron | Normal level | 28 (28.6%) | 2 (2.1%) | 0 | 0 | 26 (26.5%) | p < 0.001 |
| Deficit | 70 (71.4%) | 6 (6.1%) | 25 (25.5%) | 17 (17.3%) | 22 (22.5%) | ||
| Serum ferritin | Normal level | 27 (27.5%) | 1 (1%) | 0 | 0 | 26 (26.5%) | p < 0.001 |
| Increased | 71 (72.4%) | 7 (7.1%) | 25 (25.5%) | 17 (17.3%) | 22 (22.5%) | ||
| Parameters/% (No. Cases) (%) | Ultrasound Elastography | p Value | ||||
|---|---|---|---|---|---|---|
| Total | F0 | F1 | F2 | |||
| Serum iron | Normal level | 28 (28.6%) | 28 (28.6%) | 0 | 0 | p < 0.001 |
| Deficit | 70 (71.4%) | 40 (40.8%) | 13 (13.2%) | 17 (17.3%) | ||
| Serum ferritin | Normal level | 27 (27.5%) | 27 (27.5%) | 0 | 0 | p < 0.001 |
| Increased | 71 (72.4%) | 41 (41.8%) | 13 (13.2%) | 17 (17.3%) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stepan, M.D.; Vintilescu, Ș.B.; Ionele, C.M.; Dumitra, G.G.; Podeanu, M.A.; Bigea, C.C.; Sacerdoțianu, V.M.; Anastasescu, C.M.; Florescu, D.N. Associations of Ultrasound Findings with Serum Iron and Ferritin Levels in Children with Obesity. Life 2024, 14, 484. https://doi.org/10.3390/life14040484
Stepan MD, Vintilescu ȘB, Ionele CM, Dumitra GG, Podeanu MA, Bigea CC, Sacerdoțianu VM, Anastasescu CM, Florescu DN. Associations of Ultrasound Findings with Serum Iron and Ferritin Levels in Children with Obesity. Life. 2024; 14(4):484. https://doi.org/10.3390/life14040484
Chicago/Turabian StyleStepan, Mioara Desdemona, Ștefănița Bianca Vintilescu, Claudiu Marinel Ionele, Gheorghe Gindrovel Dumitra, Mihaela Andreea Podeanu, Camelia Cristiana Bigea, Victor Mihai Sacerdoțianu, Cătălina Mihaela Anastasescu, and Dan Nicolae Florescu. 2024. "Associations of Ultrasound Findings with Serum Iron and Ferritin Levels in Children with Obesity" Life 14, no. 4: 484. https://doi.org/10.3390/life14040484