

Comparison of Early Postoperative Diaphragm Muscle Function after Lobectomy via VATS and Open Thoracotomy: A Sonographic Study
Abstract
1. Introduction
2. Materials and Methods
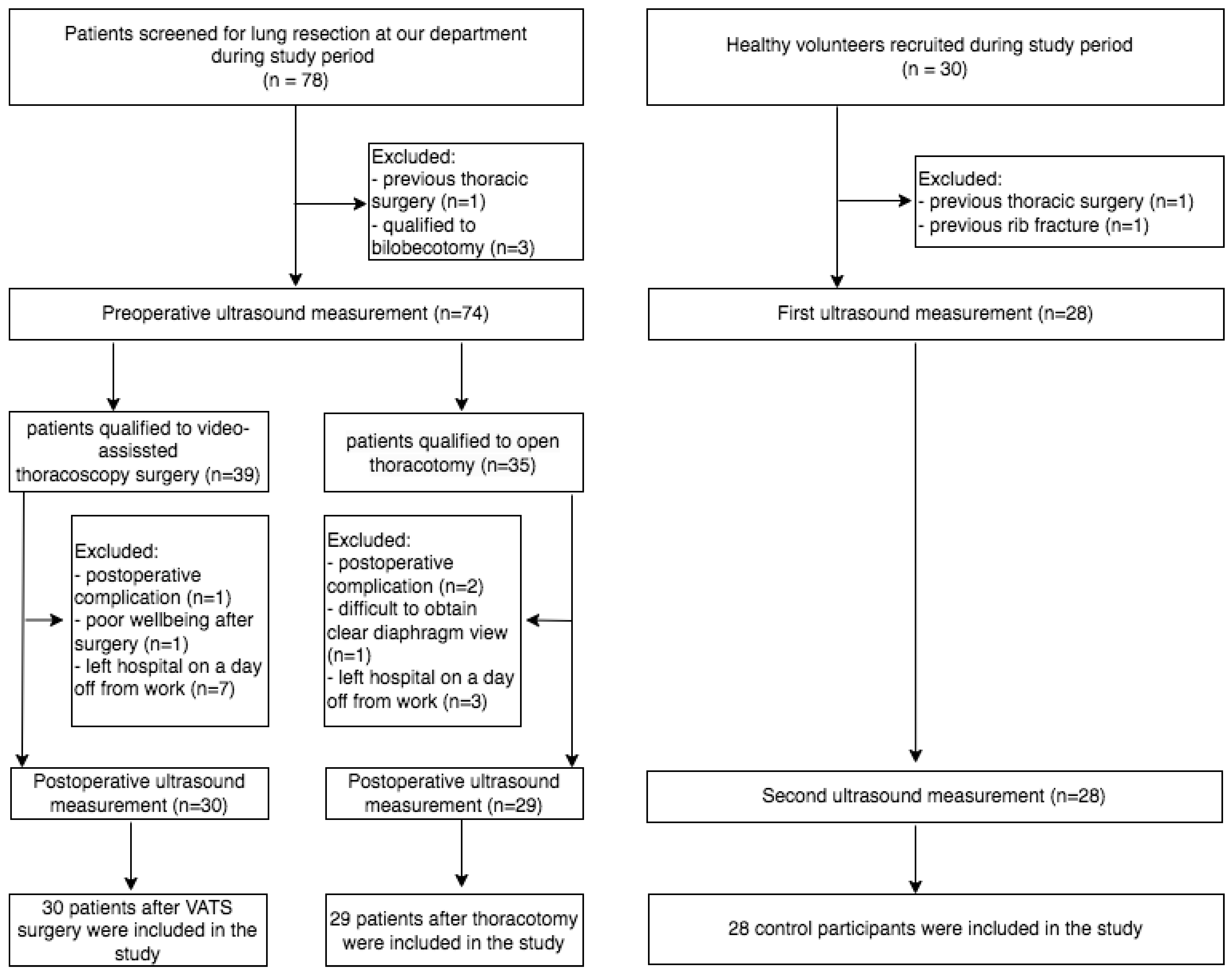
2.1. Participants Selection Process and Eligibility Criteria
2.2. Surgical Techniques
2.3. Diaphragm Muscle Ultrasound Assessment
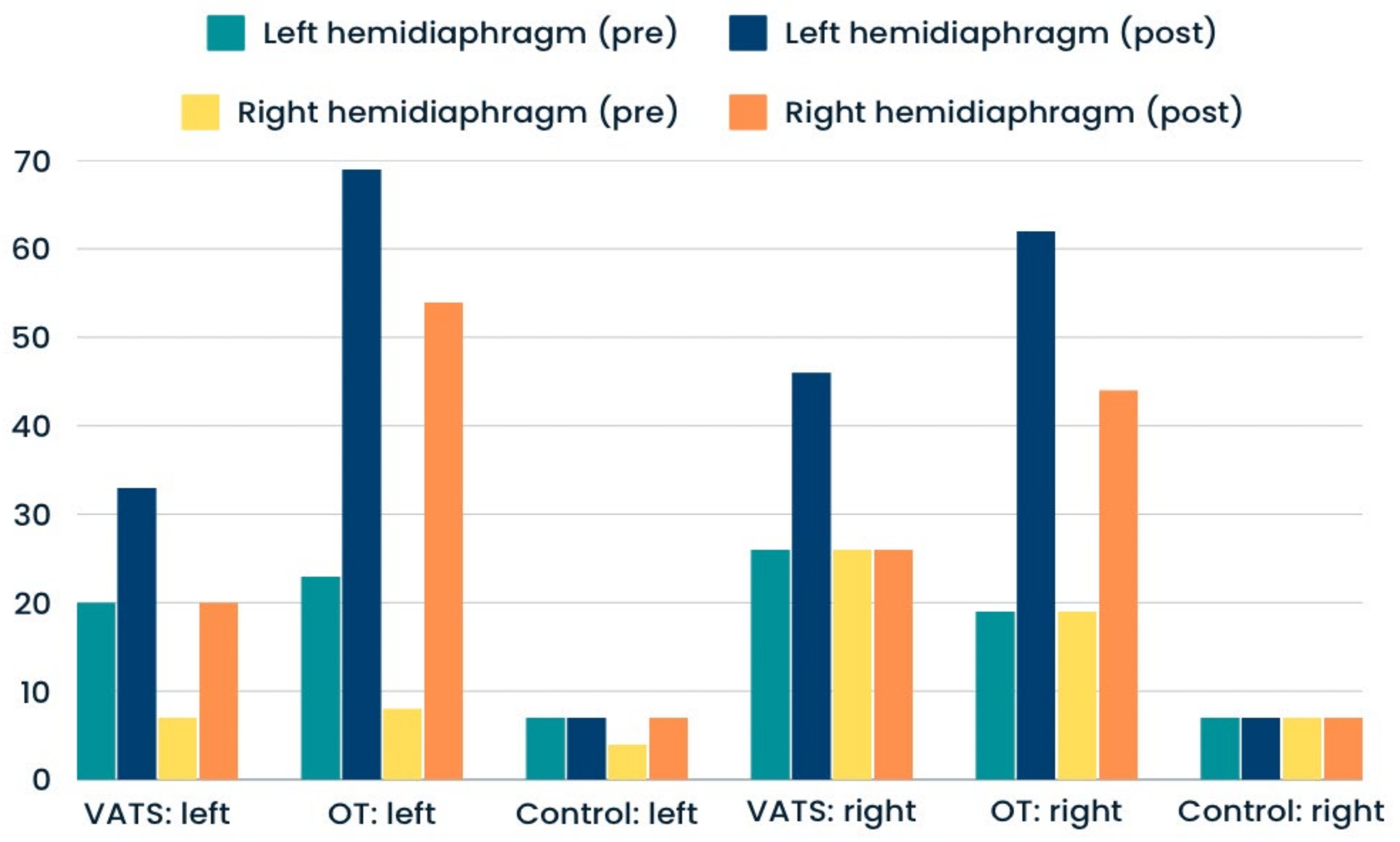
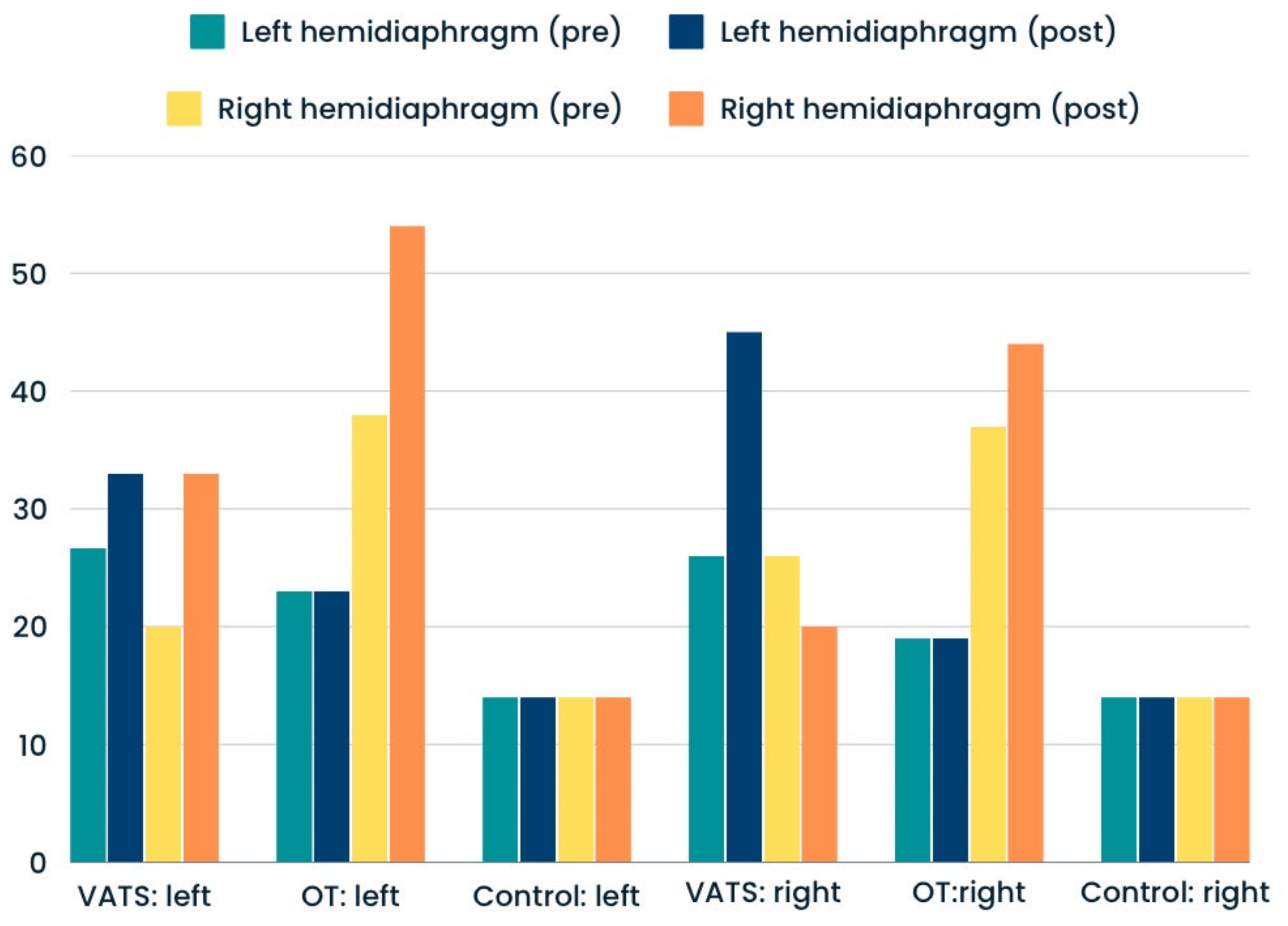
- DTF (Diaphragm Thickness Fraction), reflecting the magnitude of diaphragm effort. We used the following standardized formula: DTF = (ThIns − ThExp)/ThExp × 100%. The normal percentage for the supine position is more or equal to 65%. DTF values less than 20% are consistent with diaphragm muscle paralysis.
- DTR (Diaphragm Thickening Ratio), reflecting the diaphragm muscle strength. This index was calculated using the following formula: DTR = ThIns/ThExp. Higher values represent a better outcome. The normal value is between 1.7 to 2.0.
- Δ (Delta)—differences between preoperative (pre) and postoperative (post) values on each side were calculated using the following formulas: ΔThIns = ThIns (pre) − ThIns (post), ΔThExp = ThExp (pre) − ThExp (post), ΔDTF = DTF (pre) − DTF (post) and ΔDTR = DTR (pre) − DTR (post). For the precise comparative analysis, the differences between preoperative and postoperative values were also expressed as a percent of the preoperative amplitude: ΔThIns (%) = ΔThIns × 100/ThIns (pre), ΔThExp (%) = ΔThExp × 100/ThExp (pre), ΔDTF (%) = ΔDTF × 100/DTF (pre) and ΔDTR (%) = ΔDTR × 100/DTR (pre).
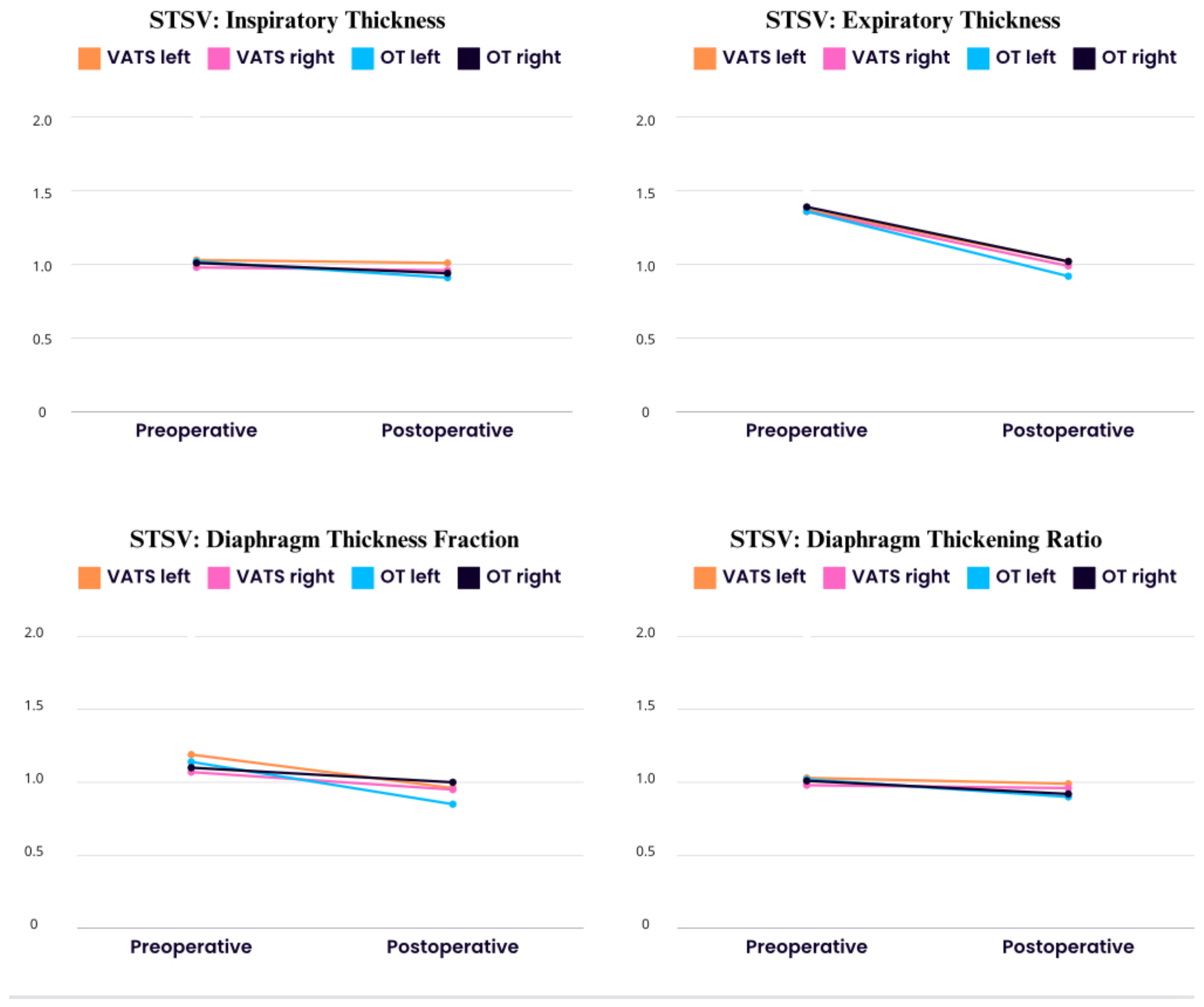
- Side-to-side variability (stsv)—differences between the left and right hemidiaphragm were calculated using the following formulas: ThIns (StSv) = ThIns (left) − ThIns (right), ThExp (StSv) = ThExp (left) − ThExp (right), DTF (StSv) = DTF (left) − DTF (right) and DTR (StSv) = DTR (left) − DTR (right). The obtained results are given as absolute values.
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
- Generally, greater diaphragm impairment was observed after lobectomy via conventional thoracotomy compared to VATS.
- Inspiratory Thickness, Diaphragm Thickness Fraction (DTF) reflecting the magnitude of diaphragm effort and the Diaphragm Thickening Ratio (DTR) reflecting diaphragm muscle strength were significantly reduced after lobe resection in both groups, but the percentage of deterioration was greater after thoracotomy compared to VATS.
- The percentage of hemidiaphragm paralysis was significantly higher after thoracotomy compared to VATS. Other types of diaphragm dysfunction (atrophy, weakness) were at similar levels after surgery compared to preoperative data.
- The degree of diaphragm impairment differed according to the location of the resected lobe. Left-upper and right-upper resection was associated with greater diaphragm impairment compared to the case of resection of other lobes
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global Burden of Disease Cancer Collaboration; Fitzmaurice, C.; Abate, D.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdel-Rahman, O.; Abdelalim, A.; Abdoli, A.; Abdollahpour, I.; et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2017: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2019, 5, 1749–1768. [Google Scholar] [PubMed]
- Kim, J.; Lee, H.; Huang, B.W. Lung Cancer: Diagnosis, Treatment Principles, and Screening. Am. Fam. Physician 2022, 105, 487–494. [Google Scholar] [PubMed]
- Batihan, G.; Ceylan, K.C.; Usluer OKaya, S. Video-Assisted Thoracoscopic Surgery vs Thoracotomy for Non-Small Cell Lung Cancer Greater Than 5 cm: Is VATS a feasible approach for large tumors? J. Cardiothorac. Surg. 2020, 15, 261. [Google Scholar] [CrossRef] [PubMed]
- Kirby, T.J.; Mack, M.J.; Landreneau, R.J.; Rice, T.W. Lobectomy—Video-assisted thoracic surgery versus muscle-sparing thoracotomy. A randomized trial. J. Thorac. Cardiovasc. Surg. 1995, 109, 997–1001. [Google Scholar] [CrossRef]
- Flores, R.M.; Park, B.J.; Dycoco, J.; Aronova, A.; Hirth, Y.; Rizk, N.P.; Bains, M.; Downey, R.J.; Rusch, V.W. Lobectomy by video-assisted thoracic surgery (VATS) versus thoracotomy for lung cancer. J. Thorac. Cardiovasc. Surg. 2009, 138, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Landreneau, R.J.; Mack, M.J.; Hazelrigg, S.R.; Naunheim, K.; Dowling, R.D.; Ritter, P.; Magee, M.J.; Nunchuck, S.; Keenan, R.J.; Ferson, P.F. Prevalence of chronic pain after pulmonary resection by thoracotomy or video-assisted thoracic surgery. J. Thorac. Cardiovasc. Surg. 1994, 107, 1079–1086. [Google Scholar] [CrossRef] [PubMed]
- Paul, S.; Altorki, N.K.; Sheng, S.; Lee, P.C.; Harpole, D.; Onaitis, M.W.; Stiles, B.M.; Port, J.L.; D’Amico, T.A. Thoracoscopic lobectomy is associated with lower morbidity than open lobectomy: A propensity-matched analysis from the STS database. J. Thorac. Cardiovasc. Surg. 2010, 139, 366–367. [Google Scholar] [CrossRef] [PubMed]
- Nagahiro, I.; Andou, A.; Aoe, M.; Sano, Y.; Date, H.; Shimizu, N. Pulmonary function, postoperative pain, and serum cytokine level after lobectomy: A comparison of VATS and conventional procedure. Ann. Thorac. Surg. 2001, 72, 362–365. [Google Scholar] [CrossRef] [PubMed]
- Demmy, T.L.; Nwogu, C. Is video-assisted thoracic surgery lobectomy better? Quality of life considerations. Ann. Thorac. Surg. 2008, 85, S719–S728. [Google Scholar] [CrossRef]
- von Meyenfeldt, E.M.; Marres, G.M.H.; van Thiel, E.; Damhuis, R.A.M. Variation in length of hospital stay after lung cancer surgery in the Netherlands. Eur. J. Cardiothorac. Surg. 2018, 54, 560–564. [Google Scholar] [CrossRef]
- Nath, T.S.; Mohamed, N.; Gill, P.K.; Khan, S.; Nath, T.S. A Comparative Analysis of Video-Assisted Thoracoscopic Surgery and Thoracotomy in Non-Small-Cell Lung Cancer in Terms of Their Oncological Efficacy in Resection: A Systematic Review. Cureus 2022, 14, e25443. [Google Scholar] [CrossRef] [PubMed]
- Fratacci, M.D.; Kimball, W.R.; Wain, J.C.; Kacmarek, R.M.; Polaner, D.M.; Zapol, W.M. Diaphragmatic shortening after thoracic surgery in humans. Effects of mechanical ventilation and thoracic epidural anesthesia. Anesthesiology 1993, 79, 654–665. [Google Scholar] [CrossRef] [PubMed]
- Maeda, H.; Nakahara, K.; Ohno, K.; Kido, T.; Ikeda, M.; Kawashima, Y. Diaphragm function after pulmonary resection: Relationship to postoperative respiratory failure. Am. Rev. Respir. Dis. 1988, 137, 678–861. [Google Scholar] [CrossRef] [PubMed]
- Takazakura, R.; Takahashi, M.; Nitta, N.; Sawai, S.; Tezuka, N.; Fujino, S.; Murata, K. Assessment of diaphragmatic motion after lung resection using magnetic resonance imaging. Radiat. Med. 2007, 25, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Sekine, Y.; Iwata, T.; Chiyo, M.; Yasufuku, K.; Motohashi, S.; Yoshida, S.; Suzuki, M.; Iizasa, T.; Saitoh, Y.; Fujisawa, T. Minimal alteration of pulmonary function after lobectomy in lung cancer patients with chronic obstructive pulmonary disease. Ann. Thorac. Surg. 2003, 76, 356–361. [Google Scholar] [CrossRef]
- Spadaro, S.; Grasso, S.; Dres, M.; Fogagnolo, A.; Dalla Corte, F.; Tamburini, N.; Maniscalco, P.; Cavallesco, G.; Alvisi, V.; Stripoli, T.; et al. Point of Care Ultrasound to Identify Diaphragmatic Dysfunction after Thoracic Surgery. Anesthesiology 2019, 131, 266–278. [Google Scholar] [CrossRef] [PubMed]
- Nomori, H.; Horio, H.; Naruke, T.; Suemasu, K. What is the advantage of a thoracoscopic lobectomy over a limited thoracotomy procedure for lung cancer surgery? Ann. Thorac. Surg. 2001, 72, 879–884. [Google Scholar] [CrossRef] [PubMed]
- Sarwal, A.; Walker, F.O.; Cartwright, M.S. Neuromuscular ultrasound for evaluation of the diaphragm. Muscle Nerve 2013, 47, 319–329. [Google Scholar] [CrossRef]
- Boussuges, A.; Rives, S.; Finance, J.; Chaumet, G.; Vallée, N.; Risso, J.J.; Brégeon, F. Ultrasound Assessment of Diaphragm Thickness and Thickening: Reference Values and Limits of Normality When in a Seated Position. Front. Med. 2021, 27, 742703. [Google Scholar] [CrossRef]
- Bernard, A.; Brondel, L.; Arnal, E.; Favre, J.P. Evaluation of respiratory muscle strength by randomized controlled trial comparing thoracoscopy, transaxillary thoracotomy, and posterolateral thoracotomy for lung biopsy. Eur. J. Cardiothorac. Surg. 2006, 29, 596–600. [Google Scholar] [CrossRef]
- Nomori, H.; Horio, H.; Fuyuno, G.; Kobayashi, R.; Yashima, H. Respiratory muscle strength after lung resection with special reference to age and procedures of thoracotomy. Eur. J. Cardiothorac. Surg. 1996, 10, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Brocki, B.C.; Westerdahl, E.; Langer, D.; Souza, D.S.; Andreasen, J.J. Decrease in pulmonary function and oxygenation after lung resection. ERJ Open Res. 2018, 4, 00055–02017. [Google Scholar] [CrossRef] [PubMed]
- Andreetti, C.; Menna, C.; Ibrahim, M.; Ciccone, A.M.; D’Andrilli, A.; Venuta, F.; Rendina, E.A. Postoperative pain control: Videothoracoscopic versus conservative mini-thoracotomic approach. Eur. J. Cardiothorac. Surg. 2014, 46, 907–912. [Google Scholar] [CrossRef] [PubMed]
- Nakata, M.; Saeki, H.; Yokoyama, N.; Kurita, A.; Takiyama, W.; Takashima, S. Pulmonary function after lobectomy: Video-assisted thoracic surgery versus thoracotomy. Ann. Thorac. Surg. 2000, 70, 938–941. [Google Scholar] [CrossRef]
- Siafakas, N.M.; Mitrouska, I.; Bouros, D.; Georgopoulos, D. Surgery and the respiratory muscles. Thorax 1999, 54, 458–465. [Google Scholar] [CrossRef]
- Ventura, L.; Zhao, W.; Chen, T.; Wang, Z.; Feng, J.; Gu, Z.; Ji, C.; Fang, W. Significant diaphragm elevation suggestive of phrenic nerve injury after thoracoscopic lobectomy for lung cancer: An underestimated problem. Transl. Lung Cancer Res. 2020, 9, 1822–1831. [Google Scholar] [CrossRef]
- Piehler, J.M.; Pairolero, P.C.; Gracey, D.R.; Bernatz, P.E. Unexplained diaphragmatic paralysis: A harbinger of malignant disease? J. Thorac. Cardiovasc. Surg. 1982, 84, 861–864. [Google Scholar] [CrossRef] [PubMed]
- Tenling, A.; Joachimsson, P.O.; Tyden, H.; Hedenstierna, G. Thoracic epidural analgesia as an adjunct to general anesthesia for cardiac surgery: Effects on pulmonary mechanics. Acta Anaesthesiol. Scand. 2000, 44, 1071–1076. [Google Scholar] [CrossRef] [PubMed]
- Simonneau, G.; Vivien, A.; Sartene, R.; Kunstlinger, F.; Samii, K.; Noviant, Y.; Duroux, P. Diaphragm dysfunction induced by upper abdominal surgery. Role of postoperative pain. Am. Rev. Respir. Dis. 1983, 128, 899–903. [Google Scholar] [CrossRef]
- Pu, H.; Doig, G.S.; Lv, Y.; Wu, X.; Yang, F.; Zhang, S.; Liang, Z.; Zhou, Y.; Kang, Y. Modifiable risk factors for ventilator associated diaphragmatic dysfunction: A multicenter observational study. BMC Pulm. Med. 2023, 23, 343. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | VATS | OT | Control Group | p-Value |
|---|---|---|---|---|
| Number of subjects | 30 | 29 | 28 | - |
| Age: | ||||
| Mean (years) | 63.44 ± 12.02 | 65.07 ± 11.99 | 59.13 ± 11.46 | 0.334 |
| Range (min–max) | (42–73) | (45–78) | (35–69) | - |
| Height (cm) | 168.15 ± 12.07 | 172.99 ± 15.26 | 173.01 ± 14.35 | |
| Weight (kg) | 76.95 ± 14.57 | 73.91 ± 16.18 | 75.64 ± 15.87 | 0.633 |
| BMI (kg/m2) | 27.59 ± 8.36 | 25.61 ± 9.19 | 25.84 ± 10.13 | 0.577 |
| Gender: | 0.213 | |||
| Male | 18 (60.0%) | 15 (51.7%) | 13 (46.4%) | |
| Female | 12 (40.0%) | 14 (48.3%) | 15 (53.6%) | |
| Involved side: | 0.426 | |||
| Left | 15 (50.0%) | 13 (44.8%) | - | |
| Right | 15 (50.0%) | 16 (55.2%) | - | |
| Control side: | ||||
| Left | - | - | 14 (50.0%) | 1.00 |
| Right | - | - | 14 (50.0%) | |
| Resected lobe: | 0.119 | |||
| Right-upper | 9 (30.0%) | 7 (24.1%) | - | |
| Right-middle | 2 (6.7%) | 2 (6.9%) | - | |
| Right-lower | 6 (20.0%) | 6 (20.7%) | - | |
| Left-upper | 7 (23.3%) | 6 (20.7%) | - | |
| Left-lower | 6 (20.0%) | 8 (27.6%) | - | |
| Complete radical | 1.00 | |||
| Lymphadenectomy: | ||||
| Yes | 30 (100.0%) | 30 (100.0%) | - | |
| No | 0 (0.0%) | 0 (0.0%) | - | |
| Lymph Nodes resection: | 0.144 | |||
| LNs 4 | 9 (30.0%) | 7 (24.1%) | - | |
| LNs 5 | 7 (23.3%) | 6 (20.7%) | - | |
| LNs 6 | 0 (0.0%) | 0 (0.0%) | - | |
| LNs 7 | 30 (100%) | 29 (100%) | - | |
| LNs 8 | 12 (40.0%) | 14 (48.2%) | - | |
| LNs 9 | 12 (40.0%) | 14 (48.2%) | - | |
| LNs 10 | 30 (100%) | 29 (100%) | - | |
| LNs 11 | 30 (100%) | 29 (100%) | - |
| Variables | Th Ins Left | Th Ins Right | Th Exp Left | Th Exp Right | ||
|---|---|---|---|---|---|---|
| Left Side Operated | VATS | Pre | 2.97 ± 0.47 (2.73–3.21) | 2.90 ± 0.54 (2.65–3.06) | 2.14 ± 0.39 (1.94–2.34) | 2.14 ± 0.41 (1.93–2.35) |
| Post | 2.59 ± 0.40 (2.35–2.76) | 2.57 ± 0.46 (2.31–2.78) | 1.95 ± 0.40 (1.74–2.15) | 1.98 ± 0.39 (1.78–2.18) | ||
| p-value | 0.12 | 0.019 | 0.113 | 0.126 | ||
| Δ | 0.38 * | 0.33 * | 0.19 | 0.16 | ||
| % Δ | 12.79 | 11.37 * | 8.87 * | 7.47 | ||
| OT | Pre | 3.11 ± 0.65 (2.74–3.38) | 3.05 ± 0.68 (2.67–3.41) | 2.32 ± 0.61 (1.98–2.66) | 2.32 ± 0.62 (1.98–2.67) | |
| Post | 2.61 ± 0.63 (2.23–2.98) | 2.59 ± 0.62 (2.24–2.99) | 2.23 ± 0.64 (1.85–2.61) | 2.22 ± 0.65 (1.83–2.60) | ||
| p-value | <0.001 | <0.001 | 0.531 | 0.506 | ||
| Δ | 0.50 * | 0.46 * | 0.09 | 0.10 | ||
| % Δ | 16.07 * | 15.08 * | 3.87 * | 4.31 | ||
| Right Side Operated | VATS | Pre | 2.88 ± 0.31 (2.72–3.03) | 2.95 ±0.32 (2.79–3.11) | 2.14 ± 0.38 (1.95–2.33) | 2.14 ± 0.36 (1.96–2.33) |
| Post | 2.61 ± 0.45 (2.38–2.84) | 2.68 ± 0.41 (2.47–2.89) | 1.96 ± 0.47 (1.72–2.19) | 1.98 ± 0.47 (1.74–2.22) | ||
| p-value | 0.024 | 0.021 | 0.139 | 0.131 | ||
| Δ | 0.27 * | 0.27 * | 0.18 | 0.17 | ||
| % Δ | 9.37 * | 9.15 * | 8.41 | 7.94 | ||
| OT | Pre | 3.09 ± 0.45 (2.86–3.28) | 3.07 ± 0.46 (2.85–3.19) | 2.10 ± 0.47 (1.88–2.32) | 2.10 ± 0.45 (1.88–2.31) | |
| Post | 2.55 ± 0.49 (2.32–2.79) | 2.56 ± 0.50 (2.31–2.78) | 2.03 ± 0.42 (1.83–2.23) | 2.05 ± 0.41 (1.85–2.24) | ||
| p-value | <0.001 | <0.001 | 0.445 | 0.469 | ||
| Δ | 0.54 *** | 0.51 *** | 0.07 | 0.05 | ||
| % Δ | 17.47 *** | 16.61 *** | 3.33 | 2.38 | ||
| Variables | DTF Left | DTF Right | DTR Left | DTR Right | ||
|---|---|---|---|---|---|---|
| Left Side Operated | VATS | Pre | 36.24 ± 23.51 (24.34–48.14) | 32.60 ± 20.59 (22.18–43.02) | 1.36 ± 0.24 (1.23–1.49) | 1.32 ± 0.20 (1.22–1.43) |
| Post | 25.89 ± 18.00 (16.78–35.00) | 26.82 ± 16.28 (18.58–35.06) | 1.25 ± 0.18 (1.16–1.35) | 1.27 ± 0.16 (1.18–1.35) | ||
| p value | <0.001 | <0.001 | 0.492 | 0.786 | ||
| Δ | 10.35 *** | 5.78 * | 0.11 | 0.05 | ||
| % Δ | 28.55 *** | 17.73 *** | 8.08 | 3.78 | ||
| OT | Pre | 36.45 ± 22.71 (23.60–49.31) | 33.43 ± 23.57 (20.09–46.77) | 1.36 ± 0.22 (1.24–1.48) | 1.33 ± 0.23 (1.20–1.46) | |
| Post | 18.41 ± 16.01 (8.95–27.88) | 19.59 ± 16.18 (10.02–29.15) | 1.18 ± 0.16 (1.09–1.27) | 1.19 ± 0.16 (1.10–1.29) | ||
| p-value | <0.001 | <0.001 | 0.037 | 0.048 | ||
| Δ | 18.04 *** | 13.84 *** | 0.18 | 0.14 | ||
| % Δ | 49.41 *** | 41.39 *** | 13.23 | 10.52 | ||
| Right Side Operated | VATS | Pre | 42.20 ± 18.07 (27.06–45.35) | 45.57 ± 24.00 (28.42–52.72 | 1.38 ± 0.18 (1.27–1.46) | 1.41 ± 0.24 (1.28–1.52) |
| Post | 35.18 ± 23.00 (25.54–48.82) | 35.66 ± 19.36 (18.67–33.53) | 1.29 ± 0.23 (1.25–1.48) | 1.27 ± 0.47 (1.19–1.67) | ||
| p-value | 0.022 | 0.037 | 0.507 | 0.046 | ||
| Δ | 7.02 | 9.91 | 0.09 | 0.14 | ||
| % Δ | 16.63 *** | 21.74 *** | 6.52 | 9.92 | ||
| OT | Pre | 41.11 ± 23.12 (25.36–56.85) | 45.01 ± 27.04 (30.32–61.71) | 1.51 ± 0.34 (1.35–1.67) | 1.51 ± 0.33 (1.35–1.66) | |
| Post | 27.85 ± 21.30 (17.72–37.97) | 25.00 ± 17.94 (16.47–33.53) | 1.27 ± 0.21 (1.17–1.38) | 1.25 ± 0.18 (1.16–1.34) | ||
| p-value | <0.001 | <0.001 | 0.008 | 0.003 | ||
| Δ | 13.26 *** | 20.01 *** | 0.24 | 0.26 | ||
| % Δ | 32.25 *** | 44.45 *** | 15.89 | 17.21 | ||
| Variables | ΔTh Ins Left | ΔTh Ins Right | ΔTh Exp Left | ΔTh Exp Right | ΔDTF Left | ΔDTF Right | ΔDTR Left | ΔDTR Right | |
|---|---|---|---|---|---|---|---|---|---|
| Upper-right Resection | VATS | 15.85 † | 17.58 | 6.99 * | 7.43 * | 26.39 | 30.72 †† | 7.47 | 9.23 |
| OT | 18.01 † | 19.24 † | 3.19 * | 3.26 * | 30.23 | 34.06 †† | 11.13 | 11.84 | |
| Upper-left Resection | VATS | 14.69 | 13.85 | 12.26 *† | 10.24 *† | 33.45 † | 23.61 | 10.13 | 8.77 |
| OT | 17.67 | 15.26 | 3.32 * | 3.27 * | 35.27 †† | 27.89 † | 11.82 | 10.67 | |
| Lower-right Resection | VATS | 6.23 † | 15.12 | 6.74 | 6.37 | 22.24 | 17.44 †† | 6.13 | 8.66 |
| OT | 13.78 | 14.89 | 3.28 | 3.40 | 25.65 | 19.88 †† | 9.27 | 10.18 | |
| Lower-left Resection | VATS | 11.87 | 9.11 | 6.02 | 5.25 | 20.95 † | 18.32 | 6.06 | 5.42 |
| OT | 14.34 | 13.75 | 3.63 | 3.39 | 21.54 †† | 19.37 † | 9.88 | 9.31 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kocjan, J.; Rydel, M.; Czyżewski, D.; Adamek, M. Comparison of Early Postoperative Diaphragm Muscle Function after Lobectomy via VATS and Open Thoracotomy: A Sonographic Study. Life 2024, 14, 487. https://doi.org/10.3390/life14040487
Kocjan J, Rydel M, Czyżewski D, Adamek M. Comparison of Early Postoperative Diaphragm Muscle Function after Lobectomy via VATS and Open Thoracotomy: A Sonographic Study. Life. 2024; 14(4):487. https://doi.org/10.3390/life14040487
Chicago/Turabian StyleKocjan, Janusz, Mateusz Rydel, Damian Czyżewski, and Mariusz Adamek. 2024. "Comparison of Early Postoperative Diaphragm Muscle Function after Lobectomy via VATS and Open Thoracotomy: A Sonographic Study" Life 14, no. 4: 487. https://doi.org/10.3390/life14040487
APA StyleKocjan, J., Rydel, M., Czyżewski, D., & Adamek, M. (2024). Comparison of Early Postoperative Diaphragm Muscle Function after Lobectomy via VATS and Open Thoracotomy: A Sonographic Study. Life, 14(4), 487. https://doi.org/10.3390/life14040487