

Evaluation of Absolute Neutrophil, Lymphocyte and Platelet Count and Their Ratios as Predictors of Thrombotic Risk in Patients with Prefibrotic and Overt Myelofibrosis

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and the Methodology
2.2. Statistical Methods
3. Results
3.1. Patients’ Characteristics
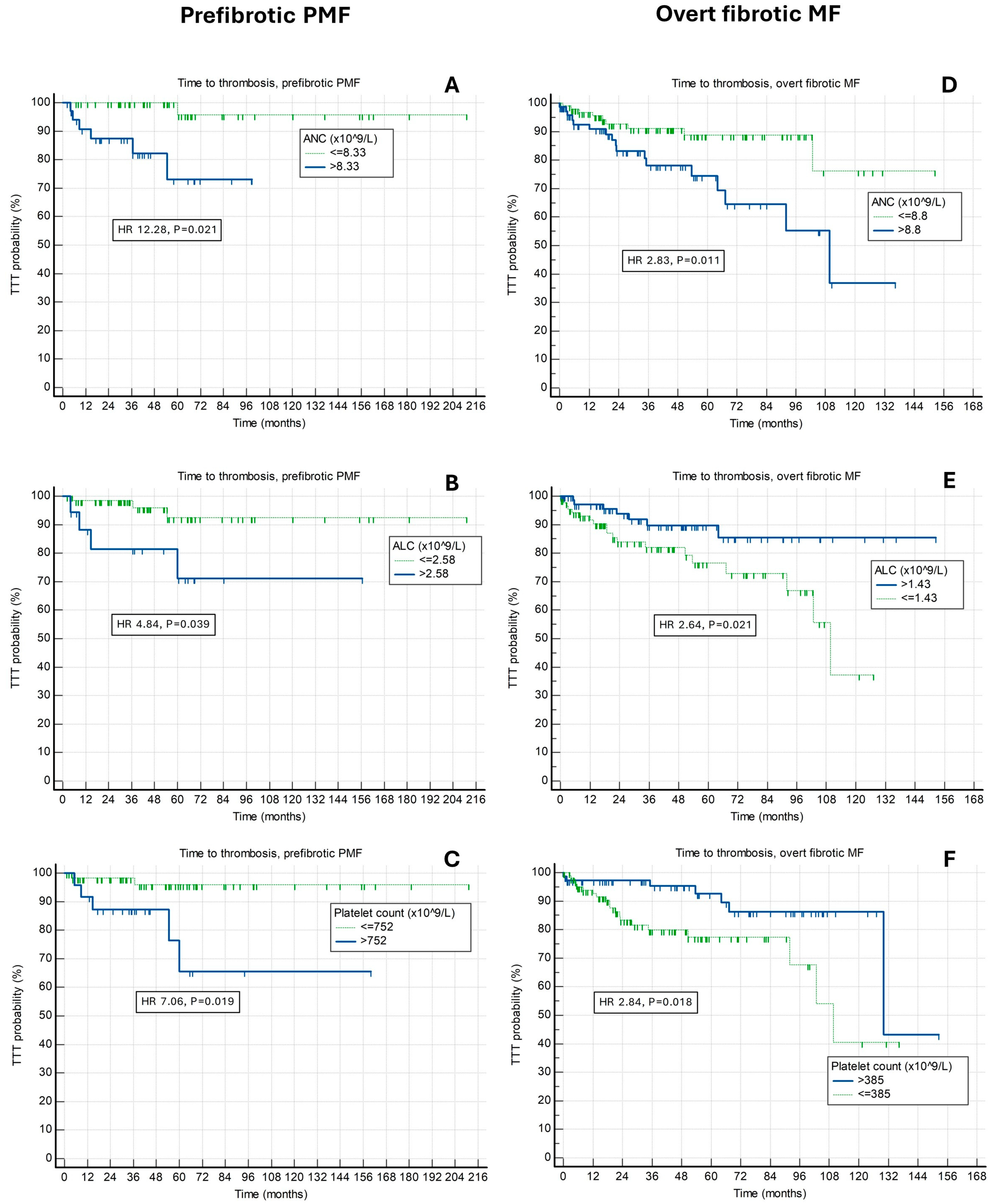
3.2. Relationship of Absolute Neutrophil, Absolute Lymphocyte, Platelet Count, Neutrophil-to-Lymphocyte and Platelet-to-Lymphocyte Ratios with Future Risk of Thrombosis in Prefibrotic PMF Patients

3.3. Relationship of Absolute Neutrophil, Absolute Lymphocyte, Platelet Count, Neutrophil-to-Lymphocyte and Platelet-to-Lymphocyte Ratios with Future Risk of Thrombosis in Overt Fibrotic MF Patients

{kind=link}
| Prefibrotic PMF | Overall Characteristics | ANC | ALC | Platelet Count |
|---|---|---|---|---|
| Age (years) | 66 IQR (56–73) | p = 0.008 * ↑ | p = 0.432 | p = 0.473 |
| Male sex | 57/85 (67.1%) | p = 0.771 | p = 0.050 * ↓ | p = 0.042 * ↑ |
| BM fibrosis Grade 0 Grade I | 13/85 (15.3%) 72/85 (84.7%) | p = 0.669 | p = 0.802 | p = 0.017 * ↑ |
| JAK2 mutated | 57/84 (67.9%) | p = 0.022 * ↑ | p = 0.081 | p = 0.688 |
| CALR mutated | 10/64 (15.6%) | p = 0.002 * ↓ | p = 0.882 | p = 0.913 |
| Constitutional symptoms | 19/85 (22.4%) | p = 0.011 * ↑ | p = 0.883 | p = 0.044 * ↓ |
| Transfusion dependency | 10/85 (11.8%) | p = 1.000 | p = 0.758 | p = 0.037 * ↓ |
| Massive splenomegaly | 5/80 (6.3%) | p = 0.314 | p = 0.432 | p = 0.001 * ↓ |
| Spleen size under left costal margin (cm) | 0 IQR (0–4) | p = 0.213 | p = 0.445 | p < 0.001 * ↓ |
| WBC (×109/L) | 10.9 IQR (8.4–16.4) | p < 0.001 * ↑ | p < 0.001 * ↑ | p = 0.758 |
| Circulatory blasts ≥ 1% | 17/85 (20%) | p = 0.668 | p = 0.821 | p < 0.001 * ↓ |
| ANC (×109/L) | 7.5 IQR (5.5–12.08) | - | p = 0.002 * ↑ | p = 0.687 |
| ALC (×109/L) | 1.8 IQR (1.3–2.5) | p = 0.002 * ↑ | - | p = 0.092 |
| Abs. mono. (×109/L) | 0.6 IQR (0.4–0.91) | p < 0.001 * ↑ | p < 0.001 * ↑ | p = 0.054 |
| Abs. basophils (×109/L) | 0.1 IQR (0.1–0.2) | p < 0.001 * ↑ | p = 0.007 * ↑ | p = 0.344 |
| Hemoglobin (g/L) | 132 IQR (117–148) | p = 0.689 | p = 0.062 | p = 0.054 |
| Platelet count (×109/L) | 550 IQR (297–780) | p = 0.687 | p = 0.092 | - |
| LDH (U/L) | 322 IQR (224.5–510.5) | p < 0.001 * ↑ | p = 0.802 | p = 0.106 |
| CRP (mg/L) | 1.9 IQR (0.8–5.4) | p = 0.085 | p = 0.307 | p = 0.007 * ↓ |
| Albumin (g/L) | 45 IQR (41.15–47.3) | p = 0.641 | p = 0.903 | p = 0.996 |
| Uric acid (mmol/L) | 380 IQR (301–450) | p = 0.001 * ↑ | p = 0.730 | p = 0.247 |
| Charlson comorbidity index | 3 IQR (2–4) | p = 0.032 * ↑ | p = 0.927 | p = 0.225 |
| CV risk factors | 60/83 (72.3%) | p = 0.538 | p = 0.131 | p = 0.348 |
| Chronic kidney disease | 15/82 (18.3%) | p = 0.035 * ↑ | p = 0.648 | p = 0.325 |
| Arterial hypertension | 49/83 (59%) | p = 0.752 | p = 0.301 | p = 0.876 |
| Diabetes mellitus | 12/83 (14.5%) | p = 0.835 | p = 0.876 | p = 0.478 |
| Hyperlipoproteinemia | 15/82 (18.3%) | p = 0.228 | p = 0.536 | p = 0.171 |
| Obesity | 9/62 (14.5%) | p = 0.771 | p = 0.496 | p = 0.335 |
| Active smoking | 10/72 (13.9%) | p = 0.980 | p = 0.750 | p = 0.352 |
| History of thrombosis | 15/85 (17.7%) | p = 0.828 | p = 0.861 | p = 0.071 |
| Cytoreductive therapy | 52/83 (62.7%) | p = 0.025 * ↑ | p = 0.099 | p = 0.006 * ↑ |
| DIPSS (PMF) Low risk Intermediate-1 risk Intermediate-2 risk High risk | 26/85 (30.6%) 40/85 (47.1%) 17/85 (20%) 2/85 (2.4%) | p = 0.412 | p = 0.204 | p = 0.071 |
| Overt Fibrotic Myelofibrosis | Overall Characteristics | ANC | ALC | Platelet Count |
|---|---|---|---|---|
| Age (years) | 68 IQR (61.5–76) | p = 0.223 | p = 0.494 | p = 0.185 |
| Male sex | 98/171 (57.3%) | p = 0.639 | p = 0.578 | p = 0.041 * ↑ |
| Etiology of myelofibrosis PMF Post PV SMF Post ET SMF | 93/171 (54.4%) 39/171 (22.8%) 38/171 (22.2%) | p = 0.055 | p = 0.133 | p = 0.116 |
| BM fibrosis Grade II Grade II | 113/171 (66.1%) 58/171 (33.9%) | p = 0.184 | p = 0.892 | p = 0.017 * ↓ |
| JAK2 mutated | 120/164 (73.2%) | p = 0.002 * ↑ | p = 0.898 | p = 0.245 |
| CALR mutated | 12/135 (8.9%) | p = 0.103 | p = 0.486 | p = 0.052 |
| MPL mutated | 4/133 (3%) | p = 0.402 | p = 0.668 | p = 0.716 |
| Constitutional symptoms | 93/171 (54.4%) | p = 0.169 | p = 0.394 | p < 0.001 * ↓ |
| Transfusion dependency | 54/171 (31.6%) | p = 0.224 | p = 0.407 | p = 0.101 |
| Massive splenomegaly | 35/160 (21.9%) | p = 0.873 | p = 0.041 * ↓ | p = 0.150 |
| Spleen size under left costal margin (cm) | 4 IQR (1–10) | p = 0.200 | p = 0.448 | p = 0.007 * ↓ |
| WBC (×109/L) | 10.4 IQR (6.05–19.15) | p < 0.001 * ↑ | p < 0.001 * ↑ | p < 0.001 * ↑ |
| Circulatory blasts ≥ 1% | 85/171 (49.7%) | p = 0.360 | p = 0.002 * ↑ | p = 0.073 |
| ANC (×109/L) | 7.3 IQR (3.5–13.43) | - | p < 0.001 * ↑ | p < 0.001 * ↑ |
| ALC (×109/L) | 1.4 IQR (1–2.13) | p < 0.001 * ↑ | - | p = 0.148 |
| Abs. mono. (×109/L) | 0.4 IQR (0.21–0.8) | p < 0.001 * ↑ | p < 0.001 * ↑ | p < 0.001 * ↑ |
| Abs. basophils (×109/L) | 0.1 IQR (0.06–0.3) | p < 0.001 * ↑ | p < 0.001 * ↑ | p = 0.022 * ↑ |
| Hemoglobin level (g/L) | 101 IQR (87.5–121.5) | p < 0.001 * ↑ | p = 0.072 | p = 0.002 * ↑ |
| Platelets (×109/L) | 300 IQR (173–525.5) | p < 0.001 * ↑ | p = 0.148 | - |
| LDH (U/L) | 485.5 IQR (343.25–729) | p = 0.008 * ↑ | p = 0.002 * ↑ | p = 0.667 |
| CRP (mg/L) | 6.7 IQR (2.3–13.4) | p = 0.931 | p = 0.567 | p < 0.001 * ↓ |
| Albumin (g/L) | 42 IQR (39–44.05) | p = 0.873 | p = 0.368 | p = 0.100 |
| Uric acid (mmol/L) | 381 IQR (318.75–467.25) | p = 0.004 * ↑ | p = 0.014 * ↑ | p = 0.018 * ↑ |
| Charlson comorbidity index | 3 IQR (2–4.25) | p = 0.258 | p = 0.983 | p = 0.910 |
| CV risk factors | 111/165 (67.3%) | p = 0.387 | p = 0.209 | p = 0.402 |
| Chronic kidney disease | 27/165 (16.4%) | p = 0.063 | p = 0.601 | p < 0.001 * ↑ |
| Arterial hypertension | 96/164 (58.5%) | p = 0.565 | p = 0.661 | p = 0.352 |
| Diabetes mellitus | 22/165 (13.3%) | p = 0.842 | p = 0.641 | p = 0.036 * ↓ |
| Hyperlipoproteinemia | 26/161 (16.1%) | p = 0.603 | p = 0.104 | p = 0.011 * ↑ |
| Obesity | 8/141 (5.7%) | p = 0.728 | p = 0.731 | p = 0.262 |
| Active smoking | 21/148 (14.2%) | p = 0.518 | p = 0.149 | p = 0.528 |
| History of thrombosis | 33/171 (19.3%) | p = 0.264 | p = 0.615 | p = 0.725 |
| Cytoreductive therapy | 116/167 (69.5%) | p < 0.001 * ↑ | p = 0.394 | p = 0.009 * ↑ |
| DIPSS (PMF) Low risk Intermediate-1 risk Intermediate-2 risk High risk | 4/93 (4.3%) 25/93 (26.9%) 52/93 (55.9%) 12/93 (12.9%) | p = 0.793 | p = 0.094 | p = 0.009 * ↓ |
| MYSEC-PM (SMF) Low risk Intermediate-1 risk Intermediate-2 risk High risk | 13/135 (9.6%) 42/135 (31.1%) 40/135 (29.6%) 40/135 (29.6%) | p = 0.165 | p = 0.208 | p = 0.005 * ↓ |
| Prefibrotic PMF | Time to Thrombosis (Composite) | Time to Arterial Thrombosis | Time to Venous Thrombosis |
|---|---|---|---|
| ANC (×109/L) ROCc defined cut-off Proportion of patients Associated risk Harrell’s C | >8.33 35 (41.2%) HR 12.28, p = 0.021 * 0.790 | >8.33 35 (41.2%) HR 23.6, p = 0.011 * 0.840 | >14.19 15 (17.6%) HR 11.29, p = 0.012 * 0.919 |
| ALC (×109/L) ROCc defined cut-off Proportion of patients Associated risk Harrell’s C | >2.58 19 (22%) HR 4.84, p = 0.039 * 0.703 | >4 3 (3.5%) HR -, p < 0.001 * 0.728 | >2.6 18 (21.2%) HR 21.28, p = 0.036 * 0.739 |
| Platelet count (×109/L) ROCc defined cut-off Proportion of patients Associated risk Harrell’s C | >752 25 (28.4%) HR 7.06, p = 0.019 * 0.709 | >574 41 (46.6%) HR 14.9, p = 0.029 * 0.799 | Not adequate > 752 - p = 0.156 0.682 |
| NLR ROCc defined cut-off Proportion of patients Associated risk Harrell’s C | >6.33 24 (28.2%) HR 4.87, p = 0.040 * 0.726 | Not adequate > 4.86 - p = 0.299 0.583 | >6.33 24 (28.2%) HR 35.5, p = 0.005 * 0.871 |
| PLR ROCc defined cut-off Proportion of patients Associated risk Harrell’s C | >498 13 (15.3%) HR 5.41, p = 0.027 * 0.634 | >498 13 (15.3%) HR 14.92, p = 0.027 * 0.718 | Not adequate ≤ 291 - p = 0.357 0.631 |
| Variables | Prefibrotic PMF | Overt Fibrotic Myelofibrosis |
|---|---|---|
| ANC (×109/L) | Cut-off >8.33; p = 0.036 * HR 13.08, 95% CI (1.18–144.94) | Cut-off >8.8; p = 0.004 * HR 4.49, 95% CI (1.62–12.45) |
| ALC(×109/L) | Cut-off >2.58; p = 0.049 * HR 20.63, 95% CI (1.01–420.74) | Cut-off ≤1.43; p = 0.003 * HR 4.15, 95% CI (1.65–10.47) |
| Platelet count (×109/L) | Cut-off >752; p = 0.043 * HR 10.5, 95% CI (1.07–103.11) | Cut-off ≤385; p = 0.004 * HR 4.68, 95% CI (1.61–13.66) |
| Age ≥ 60 years | p = 0.184 HR 6.94, 95% CI (0.39–121.71) | p = 0.846 HR 1.11, 95% CI (0.36–3.44) |
| History of thrombosis | p = 0.431 HR 0.17, 95% CI (0.0–13.41) | p = 0.231 HR 1.81, 95% CI (0.68–4.80) |
| Male sex | p = 0.441 HR 3.11, 95% CI (0.17–56.23) | p = 0.477 HR 0.72, 95% CI (0.29–1.77) |
| JAK2 mutated | p = 0.735 HR 1.48, 95% CI (0.14–14.75) | p = 0.919 HR 1.06, 95% CI (0.30–3.68) |
| Classic CV risk factors | p = 0.491 HR 2.82, 95% CI (0.14–54.62) | p = 0.747 HR 1.16, 95% CI (0.45–2.96) |
| CKD | p = 0.569 HR 1.9, 95% CI (0.21–17.41) | p < 0.001 * HR 9.07, 95% CI (3.26–25.18) |
| Overt Fibrotic Myelofibrosis | Time to Thrombosis (Composite) | Time to Arterial Thrombosis | Time to Venous Thrombosis |
|---|---|---|---|
| ANC (×109/L) ROCc defined cut-off Proportion of patients Associated risk Harrell’s C | >8.8 75 (43.9%) HR 2.83, p = 0.011 * 0.612 | >8.8 75 (43.9%) HR 2.43, p = 0.048 * 0.579 | Not adequate < 9.9 - p = 0.223 0.619 |
| ALC (×109/L) ROCc defined cut-off Proportion of patients Associated risk Harrell’s C | ≤1.43 90 (52.6%) HR 2.64, p = 0.021 * 0.604 | Not adequate ≤ 1.5 - p = 0.142 0.562 | Not adequate ≤ 1.43 - p = 0.112 0.664 |
| Platelet count (×109/L) ROCc defined cut-off Proportion of patients Associated risk Harrell’s C | ≤385 105 (58%) HR 2.84, p = 0.018 * 0.624 | ≤385 105 (58%) HR 4.32, p = 0.009 * 0.651 | Not adequate > 226 - p = 0.282 0.559 |
| NLR ROCc defined cut-off Proportion of patients Associated risk Harrell’s C | >8 46 (26.9%) HR 2.68, p = 0.012 * 0.592 | Not adequate > 8 46 (26.9%) p = 0.150 0.535 | >9.67 37 (21.6%) HR 6.53, p = 0.015 * 0.708 |
| PLR ROCc defined cut-off Proportion of patients Associated risk Harrell’s C | Not adequate ≤ 477 - p = 0.633 0.508 | Not adequate ≤ 477 - p = 0.129 0.577 | >397 42 (24.6%) HR 4.1, p = 0.070 0.659 |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thiele, J.; Kvasnicka, H.M.; Orazi, A.; Gianelli, U.; Gangat, N.; Vannucchi, A.M.; Barbui, T.; Arber, D.A.; Tefferi, A. The international consensus classification of myeloid neoplasms and acute Leukemias: Myeloproliferative neoplasms. Am. J. Hematol. 2023, 98, 166–179. [Google Scholar] [CrossRef] [PubMed]
- Krecak, I.; Lucijanic, M.; Verstovsek, S. Advances in Risk Stratification and Treatment of Polycythemia Vera and Essential Thrombocythemia. Curr. Hematol. Malig. Rep. 2022, 17, 155–169. [Google Scholar] [CrossRef] [PubMed]
- Barbui, T.; Thiele, J.; Gisslinger, H.; Kvasnicka, H.M.; Vannucchi, A.M.; Guglielmelli, P.; Orazi, A.; Tefferi, A. The 2016 WHO classification and diagnostic criteria for myeloproliferative neoplasms: Document summary and in-depth discussion. Blood Cancer J. 2018, 8, 15. [Google Scholar] [CrossRef] [PubMed]
- Sankar, K.; Stein, B.L.; Rampal, R.K. Thrombosis in the Philadelphia Chromosome-Negative Myeloproliferative Neoplasms. Cancer Treat. Res. 2019, 179, 159–178. [Google Scholar] [CrossRef]
- Hultcrantz, M.; Björkholm, M.; Dickman, P.W.; Landgren, O.; Derolf, Å.R.; Kristinsson, S.Y.; Andersson, T.M.L. Risk for Arterial and Venous Thrombosis in Patients With Myeloproliferative Neoplasms: A Population-Based Cohort Study. Ann. Intern. Med. 2018, 168, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Casini, A.; Fontana, P.; Lecompte, T.P. Thrombotic complications of myeloproliferative neoplasms: Risk assessment and risk-guided management. J. Thromb. Haemost. 2013, 11, 1215–1227. [Google Scholar] [CrossRef]
- Krecak, I.; Verstovsek, S.; Lucijanic, M. Reappraisal of cardiovascular risk factors in patients with chronic myeloproliferative neoplasms. Clin. Adv. Hematol. Oncol. 2023, 21, 541–548. [Google Scholar] [PubMed]
- Lucijanic, M.; Krecak, I.; Soric, E.; Sabljic, A.; Galusic, D.; Holik, H.; Perisa, V.; Moric Peric, M.; Zekanovic, I.; Kusec, R. Patients with post polycythemia vera myelofibrosis might experience increased thrombotic risk in comparison to primary and post essential thrombocythemia myelofibrosis. Leuk. Res. 2022, 119, 106905. [Google Scholar] [CrossRef]
- Lucijanic, M.; Krecak, I.; Soric, E.; Sabljic, A.; Galusic, D.; Holik, H.; Perisa, V.; Morić Perić, M.; Zekanović, I.; Kusec, R. Atrial Fibrillation in Patients with Myelofibrosis. Blood 2023, 142, 6437. [Google Scholar] [CrossRef]
- Zimran, E.; Hoffman, R.; Kremyanskaya, M. Current approaches to challenging scenarios in myeloproliferative neoplasms. Expert. Rev. Anticancer. Ther. 2018, 18, 567–578. [Google Scholar] [CrossRef]
- Harrison, C.N.; Nangalia, J.; Boucher, R.; Jackson, A.; Yap, C.; O’Sullivan, J.; Fox, S.; Ailts, I.; Dueck, A.C.; Geyer, H.L.; et al. Ruxolitinib Versus Best Available Therapy for Polycythemia Vera Intolerant or Resistant to Hydroxycarbamide in a Randomized Trial. J. Clin. Oncol. 2023, 41, 3534–3544. [Google Scholar] [CrossRef] [PubMed]
- Guglielmelli, P.; Gangat, N.; Coltro, G.; Lasho, T.L.; Loscocco, G.G.; Finke, C.M.; Morsia, E.; Sordi, B.; Szuber, N.; Hanson, C.A.; et al. Mutations and thrombosis in essential thrombocythemia. Blood Cancer J. 2021, 11, 77. [Google Scholar] [CrossRef] [PubMed]
- Skov, V. Next Generation Sequencing in MPNs. Lessons from the Past and Prospects for Use as Predictors of Prognosis and Treatment Responses. Cancers 2020, 12, 2194. [Google Scholar] [CrossRef] [PubMed]
- Gu, W.; Zhang, Y.; Sun, T.; Ju, M.; Liu, X.; Xue, F.; Chen, Y.; Liu, W.; Li, H.; Wang, W.; et al. Prediction of thrombosis in polycythemia vera: Development and validation of a multiple factor-based prognostic score system. Res. Pract. Thromb. Haemost. 2023, 7, 100132. [Google Scholar] [CrossRef]
- Mascarenhas, J.; Gleitz, H.F.E.; Chifotides, H.T.; Harrison, C.N.; Verstovsek, S.; Vannucchi, A.M.; Rampal, R.K.; Kiladjian, J.J.; Vainchenker, W.; Hoffman, R.; et al. Biological drivers of clinical phenotype in myelofibrosis. Leukemia 2023, 37, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Nasillo, V.; Riva, G.; Paolini, A.; Forghieri, F.; Roncati, L.; Lusenti, B.; Maccaferri, M.; Messerotti, A.; Pioli, V.; Gilioli, A.; et al. Inflammatory Microenvironment and Specific T Cells in Myeloproliferative Neoplasms: Immunopathogenesis and Novel Immunotherapies. Int. J. Mol. Sci. 2021, 22, 1906. [Google Scholar] [CrossRef] [PubMed]
- Krecak, I.; Verstovsek, S.; Lucijanic, M. Optimization of cardiovascular risk factor management in patients with BCR::ABL1 negative chronic myeloproliferative neoplasms, current knowledge, and perspectives. Ann. Hematol. 2023, 103, 1513–1523. [Google Scholar] [CrossRef] [PubMed]
- Bartels, S.; Faisal, M.; Büsche, G.; Schlue, J.; Hasemeier, B.; Schipper, E.; Vogtmann, J.; Westphal, L.; Lehmann, U.; Kreipe, H. Mutations associated with age-related clonal hematopoiesis in PMF patients with rapid progression to myelofibrosis. Leukemia 2020, 34, 1364–1372. [Google Scholar] [CrossRef]
- Barosi, G.; Mesa, R.A.; Thiele, J.; Cervantes, F.; Campbell, P.J.; Verstovsek, S.; Dupriez, B.; Levine, R.L.; Passamonti, F.; Gotlib, J.; et al. Proposed criteria for the diagnosis of post-polycythemia vera and post-essential thrombocythemia myelofibrosis: A consensus statement from the International Working Group for Myelofibrosis Research and Treatment. Leukemia 2008, 22, 437–438. [Google Scholar] [CrossRef]
- Barosi, G.; Rosti, V.; Gale, R.P. Myelofibrosis-type megakaryocyte dysplasia (MTMD) as a distinct category of BCR::ABL-negative myeloproliferative neoplasms. Challenges and perspectives. Leukemia 2023, 37, 725–727. [Google Scholar] [CrossRef]
- Leiva, O.; Hobbs, G.; Ravid, K.; Libby, P. Cardiovascular Disease in Myeloproliferative Neoplasms: JACC: CardioOncology State-of-the-Art Review. JACC CardioOncol. 2022, 4, 166–182. [Google Scholar] [CrossRef] [PubMed]
- Aviv, A.; Levy, D. Hemothelium, Clonal Hematopoiesis of Indeterminate Potential, and Atherosclerosis. Circulation 2019, 139, 7–9. [Google Scholar] [CrossRef] [PubMed]
- Said, S.M.; Leung, N.; Sethi, S.; Cornell, L.D.; Fidler, M.E.; Grande, J.P.; Herrmann, S.; Tefferi, A.; D’Agati, V.D.; Nasr, S.H. Myeloproliferative neoplasms cause glomerulopathy. Kidney Int. 2011, 80, 753–759. [Google Scholar] [CrossRef] [PubMed]
- Holik, H.; Krečak, I.; Lucijanić, M.; Samardžić, I.; Pilipac, D.; Vučinić Ljubičić, I.; Coha, B.; Kitter Pipić, A.; Miškić, B.; Zupančić-Šalek, S. Hip and Knee Osteoarthritis in Patients with Chronic Myeloproliferative Neoplasms: A Cross-Sectional Study. Life 2023, 13, 1388. [Google Scholar] [CrossRef] [PubMed]
- Hasselbalch, H.C.; Bjørn, M.E. MPNs as Inflammatory Diseases: The Evidence, Consequences, and Perspectives. Mediat. Inflamm. 2015, 2015, 102476. [Google Scholar] [CrossRef] [PubMed]
- Hasselbalch, H.C.; Kristiansen, M.H.; Kjær, L.; Skov, V.; Larsen, M.K.; Ellervik, C.; Wienecke, T. CHIP-JAK2V617F, chronic inflammation, abnormal megakaryocyte morphology, organ failure, and multimorbidties. Blood Adv. 2024, 8, 681–682. [Google Scholar] [CrossRef] [PubMed]
- Lucijanic, M.; Livun, A.; Tupek, K.M.; Stoos-Veic, T.; Aralica, G.; Gecek, I.; Pejsa, V.; Kusec, R. Heat shock protein 27 (HSP27/HSPB1) expression is increased in patients with primary and secondary myelofibrosis and may be affecting their survival. Leuk. Lymphoma 2017, 58, 2497–2500. [Google Scholar] [CrossRef] [PubMed]
- Inia, J.A.; O’Brien, E.R. Role of Heat Shock Protein 27 in Modulating Atherosclerotic Inflammation. J. Cardiovasc. Transl. Res. 2021, 14, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Lucijanic, M.; Krecak, I. The Complete Blood Count: Increasing Its Precision and Impact. Ann. Intern. Med. 2023, 176, eL230164. [Google Scholar] [CrossRef]
- Passamonti, F.; Cervantes, F.; Vannucchi, A.M.; Morra, E.; Rumi, E.; Pereira, A.; Guglielmelli, P.; Pungolino, E.; Caramella, M.; Maffioli, M.; et al. A dynamic prognostic model to predict survival in primary myelofibrosis: A study by the IWG-MRT (International Working Group for Myeloproliferative Neoplasms Research and Treatment). Blood 2010, 115, 1703–1708. [Google Scholar] [CrossRef]
- Lucijanic, M.; Livun, A.; Stoos-Veic, T.; Pejsa, V.; Jaksic, O.; Cicic, D.; Lucijanic, J.; Romic, Z.; Orehovec, B.; Aralica, G.; et al. High absolute basophil count is a powerful independent predictor of inferior overall survival in patients with primary myelofibrosis. Hematology 2018, 23, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Lucijanic, M.; Cicic, D.; Stoos-Veic, T.; Pejsa, V.; Lucijanic, J.; Fazlic Dzankic, A.; Vlasac Glasnovic, J.; Soric, E.; Skelin, M.; Kusec, R. Elevated Neutrophil-to-Lymphocyte-ratio and Platelet-to-Lymphocyte Ratio in Myelofibrosis: Inflammatory Biomarkers or Representatives of Myeloproliferation Itself? Anticancer. Res. 2018, 38, 3157–3163. [Google Scholar] [CrossRef] [PubMed]
- Lucijanic, M.; Veletic, I.; Rahelic, D.; Pejsa, V.; Cicic, D.; Skelin, M.; Livun, A.; Tupek, K.M.; Stoos-Veic, T.; Lucijanic, T.; et al. Assessing serum albumin concentration, lymphocyte count and prognostic nutritional index might improve prognostication in patients with myelofibrosis. Wien. Klin. Wochenschr. 2018, 130, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Krečak, I.; Holik, H.; Morić Perić, M.; Zekanović, I.; Coha, B.; Gverić-Krečak, V.; Lucijanić, M. High platelet-to-lymphocyte ratio may differentiate polycythemia vera from secondary polycythemia. Wien. Klin. Wochenschr. 2022, 134, 483–486. [Google Scholar] [CrossRef] [PubMed]
- Tefferi, A.; Loscocco, G.G.; Farrukh, F.; Szuber, N.; Mannelli, F.; Pardanani, A.; Hanson, C.A.; Ketterling, R.P.; De Stefano, V.; Carobbio, A.; et al. A globally applicable “triple A” risk model for essential thrombocythemia based on Age, Absolute neutrophil count, and Absolute lymphocyte count. Am. J. Hematol. 2023, 98, 1829–1837. [Google Scholar] [CrossRef] [PubMed]
- Krecak, I.; Lekovic, D.; Arsenovic, I.; Holik, H.; Zekanovic, I.; Moric Peric, M.; Lucijanic, M. The triple A model (age, absolute neutrophil count, absolute lymphocyte count-AAA) predicts survival and thrombosis in polycythemia vera. Am. J. Hematol. 2024, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Lucijanic, M.; Krecak, I.; Galusic, D.; Holik, H.; Perisa, V.; Moric Peric, M.; Zekanovic, I.; Budimir, J.; Lekovic, D.; Kusec, R. Triple A score (AAA: Age, absolute neutrophil count and absolute lymphocyte count) and its prognostic utility in patients with overt fibrotic and prefibrotic myelofibrosis. Ann. Hematol. 2024. [Google Scholar]
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef]
- Thiele, J.; Kvasnicka, H.M.; Facchetti, F.; Franco, V.; van der Walt, J.; Orazi, A. European consensus on grading bone marrow fibrosis and assessment of cellularity. Haematologica 2005, 90, 1128–1132. [Google Scholar]
- Passamonti, F.; Giorgino, T.; Mora, B.; Guglielmelli, P.; Rumi, E.; Maffioli, M.; Rambaldi, A.; Caramella, M.; Komrokji, R.; Gotlib, J.; et al. A clinical-molecular prognostic model to predict survival in patients with post polycythemia vera and post essential thrombocythemia myelofibrosis. Leukemia 2017, 31, 2726–2731. [Google Scholar] [CrossRef]
- Lucijanic, M. Survival analysis in clinical practice: Analyze your own data using an Excel workbook. Croat. Med. J. 2016, 57, 77–79. [Google Scholar] [CrossRef] [PubMed]
- Barbui, T.; Carobbio, A.; Thiele, J.; Gangat, N.; Rumi, E.; Rambaldi, A.; Vannucchi, A.M.; Tefferi, A. The impact of thrombosis on probabilities of death and disease progression in polycythemia vera: A multistate transition analysis of 1,545 patients. Blood Cancer J. 2023, 13, 187. [Google Scholar] [CrossRef]
- Carobbio, A.; Vannucchi, A.M.; Rumi, E.; De Stefano, V.; Rambaldi, A.; Carli, G.; Randi, M.L.; Gisslinger, H.; Passamonti, F.; Thiele, J.; et al. Survival expectation after thrombosis and overt-myelofibrosis in essential thrombocythemia and prefibrotic myelofibrosis: A multistate model approach. Blood Cancer J. 2023, 13, 115. [Google Scholar] [CrossRef] [PubMed]
- Krečak, I.; Pivac, L.; Lucijanić, M.; Skelin, M. Polypharmacy, Potentially Inappropriate Medications, and Drug-to-Drug Interactions in Patients with Chronic Myeloproliferative Neoplasms. Biomedicines 2023, 11, 1301. [Google Scholar] [CrossRef] [PubMed]
- Marcellino, B.K.; Verstovsek, S.; Mascarenhas, J. The Myelodepletive Phenotype in Myelofibrosis: Clinical Relevance and Therapeutic Implication. Clin. Lymphoma Myeloma Leuk. 2020, 20, 415–421. [Google Scholar] [CrossRef]
- Chifotides, H.T.; Verstovsek, S.; Bose, P. Association of Myelofibrosis Phenotypes with Clinical Manifestations, Molecular Profiles, and Treatments. Cancers 2023, 15, 3331. [Google Scholar] [CrossRef] [PubMed]
- McLornan, D.P.; Psaila, B.; Ewing, J.; Innes, A.; Arami, S.; Brady, J.; Butt, N.M.; Cargo, C.; Cross, N.C.P.; Francis, S.; et al. The management of myelofibrosis: A British Society for Haematology Guideline. Br. J. Haematol. 2024, 204, 136–150. [Google Scholar] [CrossRef] [PubMed]
- Liu, A.; Naymagon, L.; Tremblay, D. Splanchnic Vein Thrombosis in Myeloproliferative Neoplasms: Treatment Considerations and Unmet Needs. Cancers 2022, 15, 11. [Google Scholar] [CrossRef] [PubMed]
- Guglielmelli, P.; Kiladjian, J.J.; Vannucchi, A.M.; Duan, M.; Meng, H.; Pan, L.; He, G.; Verstovsek, S.; Boyer, F.; Barraco, F.; et al. Efficacy and safety of ruxolitinib in patients with myelofibrosis and low platelet count (50 × 10(9)/L to <100 × 10(9)/L) at baseline: The final analysis of EXPAND. Ther. Adv. Hematol. 2022, 13, 20406207221118429. [Google Scholar] [CrossRef]
- Tremblay, D.; Winters, A.; Beckman, J.D.; Naymagon, L.; Patel, R.; Mascarenhas, J.; Schiano, T.D. Splanchnic vein thrombosis associated with myeloproliferative neoplasms. Thromb. Res. 2022, 218, 8–16. [Google Scholar] [CrossRef]
- Bankar, A.; Zhao, H.; Iqbal, J.; Coxford, R.; Cheung, M.C.; Mozessohn, L.; Earle, C.C.; Gupta, V. Healthcare resource utilization in myeloproliferative neoplasms: A population-based study from Ontario, Canada. Leuk. Lymphoma 2020, 61, 1908–1919. [Google Scholar] [CrossRef] [PubMed]
- Copher, R.; Kee, A.; Gerds, A. Treatment Patterns, Health Care Resource Utilization, and Cost in Patients with Myelofibrosis in the United States. Oncologist 2022, 27, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Tefferi, A. Primary myelofibrosis: 2023 update on diagnosis, risk-stratification, and management. Am. J. Hematol. 2023, 98, 801–821. [Google Scholar] [CrossRef]
- Sliwa, T.; Beham-Schmid, C.; Burgstaller, S.; Buxhofer-Ausch, V.; Gastl, G.; Geissler, K.; Krauth, M.; Krippl, P.; Lang, A.; Petzer, A.; et al. Austrian recommendations for the management of primary myelofibrosis, post-polycythemia vera myelofibrosis and post-essential thrombocythemia myelofibrosis: An expert statement. Wien. Klin. Wochenschr. 2017, 129, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Guglielmelli, P.; Carobbio, A.; Rumi, E.; De Stefano, V.; Mannelli, L.; Mannelli, F.; Rotunno, G.; Coltro, G.; Betti, S.; Cavalloni, C.; et al. Validation of the IPSET score for thrombosis in patients with prefibrotic myelofibrosis. Blood Cancer J. 2020, 10, 21. [Google Scholar] [CrossRef]
- Buxhofer-Ausch, V.; Gisslinger, H.; Thiele, J.; Gisslinger, B.; Kvasnicka, H.M.; Müllauer, L.; Frantal, S.; Carobbio, A.; Passamonti, F.; Rumi, E.; et al. Leukocytosis as an important risk factor for arterial thrombosis in WHO-defined early/prefibrotic myelofibrosis: An international study of 264 patients. Am. J. Hematol. 2012, 87, 669–672. [Google Scholar] [CrossRef] [PubMed]
- Lucijanic, M.; Galusic, D.; Krecak, I.; Sedinic, M.; Holik, H.; Perisa, V.; Moric Peric, M.; Zekanovic, I.; Stoos-Veic, T.; Kusec, R. Reduced renal function strongly affects survival and thrombosis in patients with myelofibrosis. Ann. Hematol. 2020, 99, 2779–2785. [Google Scholar] [CrossRef]
- Lucijanic, M.; Krecak, I.; Soric, E.; Sabljic, A.; Galusic, D.; Holik, H.; Perisa, V.; Peric, M.M.; Zekanovic, I.; Kusec, R. Higher estimated plasma volume status is associated with increased thrombotic risk and impaired survival in patients with primary myelofibrosis. Biochem. Med. 2023, 33, 020901. [Google Scholar] [CrossRef]
- Li, Q.; Nie, J.; Cao, M.; Luo, C.; Sun, C. Association between inflammation markers and all-cause mortality in critical ill patients with atrial fibrillation: Analysis of the Multi-Parameter Intelligent Monitoring in Intensive Care (MIMIC-IV) database. Int. J. Cardiol. Heart Vasc. 2024, 51, 101372. [Google Scholar] [CrossRef]
- Lippi, G.; Plebani, M. Red blood cell distribution width (RDW) and human pathology. One size fits all. Clin. Chem. Lab. Med. 2014, 52, 1247–1249. [Google Scholar] [CrossRef]
- Lucijanic, M.; Pejsa, V.; Jaksic, O.; Mitrovic, Z.; Tomasovic-Loncaric, C.; Stoos-Veic, T.; Prka, Z.; Pirsic, M.; Haris, V.; Vasilj, T.; et al. The Degree of Anisocytosis Predicts Survival in Patients with Primary Myelofibrosis. Acta Haematol. 2016, 136, 98–100. [Google Scholar] [CrossRef] [PubMed]
- Krečak, I.; Krečak, F.; Gverić-Krečak, V. High red blood cell distribution width might predict thrombosis in essential thrombocythemia and polycythemia vera. Blood Cells Mol. Dis. 2020, 80, 102368. [Google Scholar] [CrossRef] [PubMed]
- Lucijanic, M.; Krecak, I.; Verstovsek, S.; Soric, E.; Galusic, D.; Holik, H.; Perisa, V.; Peric, M.M.; Zekanovic, I.; Kusec, R. Higher red blood cell distribution width predicts thrombosis risk in primary and secondary myelofibrosis. Ann. Hematol. 2022, 101, 1355–1357. [Google Scholar] [CrossRef] [PubMed]
- Verstovsek, S.; Krečak, I.; Heidel, F.H.; De Stefano, V.; Bryan, K.; Zuurman, M.W.; Zaiac, M.; Morelli, M.; Smyth, A.; Redondo, S.; et al. Identifying Patients with Polycythemia Vera at Risk of Thrombosis after Hydroxyurea Initiation: The Polycythemia Vera-Advanced Integrated Models (PV-AIM) Project. Biomedicines 2023, 11, 1925. [Google Scholar] [CrossRef]
- Liu, D.; Li, B.; Xu, Z.; Zhang, P.; Qin, T.; Qu, S.; Pan, L.; Sun, X.; Shi, Z.; Huang, H.; et al. RBC distribution width predicts thrombosis risk in polycythemia vera. Leukemia 2022, 36, 566–568. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lucijanic, M.; Krecak, I.; Soric, E.; Sabljic, A.; Galusic, D.; Holik, H.; Perisa, V.; Moric Peric, M.; Zekanovic, I.; Budimir, J.; et al. Evaluation of Absolute Neutrophil, Lymphocyte and Platelet Count and Their Ratios as Predictors of Thrombotic Risk in Patients with Prefibrotic and Overt Myelofibrosis. Life 2024, 14, 523. https://doi.org/10.3390/life14040523
Lucijanic M, Krecak I, Soric E, Sabljic A, Galusic D, Holik H, Perisa V, Moric Peric M, Zekanovic I, Budimir J, et al. Evaluation of Absolute Neutrophil, Lymphocyte and Platelet Count and Their Ratios as Predictors of Thrombotic Risk in Patients with Prefibrotic and Overt Myelofibrosis. Life. 2024; 14(4):523. https://doi.org/10.3390/life14040523
Chicago/Turabian StyleLucijanic, Marko, Ivan Krecak, Ena Soric, Anica Sabljic, Davor Galusic, Hrvoje Holik, Vlatka Perisa, Martina Moric Peric, Ivan Zekanovic, Josipa Budimir, and et al. 2024. "Evaluation of Absolute Neutrophil, Lymphocyte and Platelet Count and Their Ratios as Predictors of Thrombotic Risk in Patients with Prefibrotic and Overt Myelofibrosis" Life 14, no. 4: 523. https://doi.org/10.3390/life14040523
APA StyleLucijanic, M., Krecak, I., Soric, E., Sabljic, A., Galusic, D., Holik, H., Perisa, V., Moric Peric, M., Zekanovic, I., Budimir, J., & Kusec, R. (2024). Evaluation of Absolute Neutrophil, Lymphocyte and Platelet Count and Their Ratios as Predictors of Thrombotic Risk in Patients with Prefibrotic and Overt Myelofibrosis. Life, 14(4), 523. https://doi.org/10.3390/life14040523