
Bone Disease in HIV: Need for Early Diagnosis and Prevention

 ,
, 
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Understanding Bone Disease in PLWHIV and Establishing the Framework for Interventions
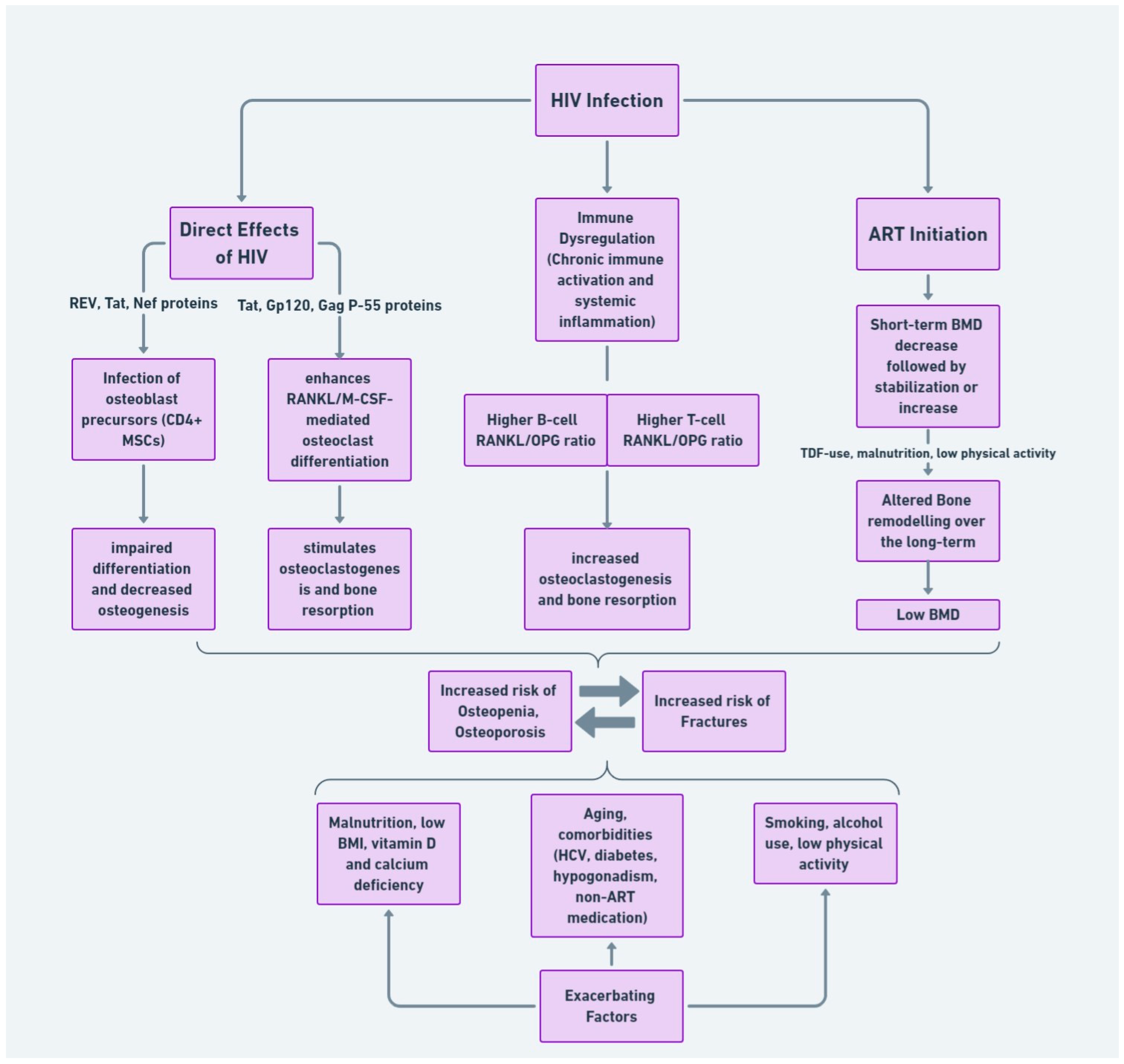
2.1. HIV and Bone Loss Pathophysiology
2.2. Impact of ART on Bone Health
2.2.1. Short-Term Effects of ART on Bone
2.2.2. Long-Term Effects of ART
2.3. Modifiable Risk Factors Contributing to Bone Disease in HIV
2.3.1. Vitamin D Deficiency and Malnutrition
2.3.2. Smoking and Alcohol Use
2.4. Comorbidities Impacting Bone Health
2.4.1. Metabolic Syndrome Elements
2.4.2. Hypogonadism
2.4.3. Hepatitis C Virus (HCV) Infection
3. Preventative and Therapeutic Strategic Planning
3.1. Diagnostic Assessments for Early Detection of Bone Disease
3.1.1. Bone Mineral Density Screening
3.1.2. Future Directions on Early Diagnosis
3.1.3. Evaluating for Secondary Causes
3.2. Prevention and Management of Bone Disease
3.2.1. Vitamin D Supplementation
3.2.2. Pharmacological Treatment
3.2.3. Physical Activity and Exercise
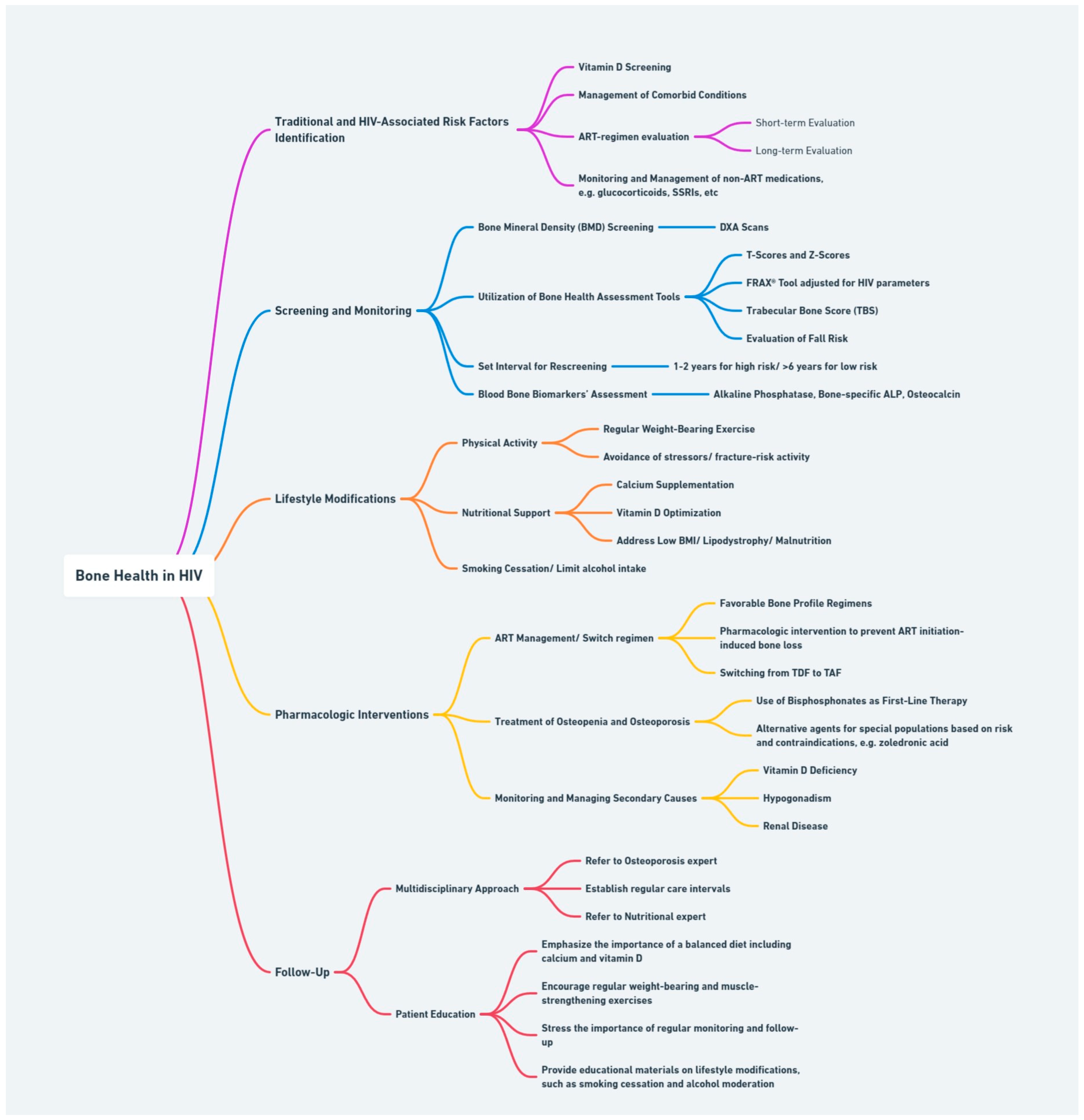
3.3. Comprehensive Bone Health Management Plan
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- McComsey, G.A.; Tebas, P.; Shane, E.; Yin, M.T.; Overton, E.T.; Huang, J.S.; Aldrovandi, G.M.; Cardoso, S.W.; Santana, J.L.; Brown, T.T. Bone disease in HIV infection: A practical review and recommendations for HIV care providers. Clin. Infect. Dis. 2010, 51, 937–946. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, H.M.; Maan, E.J.; Berger, C.; Dunn, R.A.; Côté, H.C.F.; Murray, M.C.M.; Pick, N.; Prior, J.C. Deficits in bone strength, density and microarchitecture in women living with HIV: A cross-sectional HR-pQCT study. Bone 2020, 138, 115509. [Google Scholar] [CrossRef]
- McGinty, T.; Cotter, A.G.; Sabin, C.A.; Macken, A.; Kavanagh, E.; Compston, J.; Sheehan, G.; Lambert, J.; Mallon, P.W.G. Assessment of trabecular bone score, an index of bone microarchitecture, in HIV positive and HIV negative persons within the HIV UPBEAT cohort. PLoS ONE 2019, 14, e0213440. [Google Scholar] [CrossRef]
- Olali, A.Z.; Carpenter, K.A.; Myers, M.; Sharma, A.; Yin, M.T.; Al-Harthi, L.; Ross, R.D. Bone Quality in Relation to HIV and Antiretroviral Drugs. Curr. HIV/AIDS Rep. 2022, 19, 312–327. [Google Scholar] [CrossRef]
- Brown, T.T.; Qaqish, R.B. Antiretroviral therapy and the prevalence of osteopenia and osteoporosis: A meta-analytic review. AIDS 2006, 20, 2165–2174. [Google Scholar] [CrossRef]
- Goh, S.S.L.; Lai, P.S.M.; Tan, A.T.B.; Ponnampalavanar, S. Reduced bone mineral density in human immunodeficiency virus-infected individuals: A meta-analysis of its prevalence and risk factors. Osteoporos. Int. 2018, 29, 595–613. [Google Scholar] [CrossRef] [PubMed]
- Meng, W.; Chen, M.; Song, Y.; Zhang, H.; Xie, R.; Zhang, F. Prevalence and Risk Factors of Low Bone Mineral Density in HIV/AIDS Patients: A Chinese Cross-Sectional Study. J. Acquir. Immune Defic. Syndr. 2022, 90, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Borderi, M.; Gibellini, D.; Vescini, F.; De Crignis, E.; Cimatti, L.; Biagetti, C.; Tampellini, L.; Re, M.C. Metabolic bone disease in HIV infection. AIDS 2009, 23, 1297–1310. [Google Scholar] [CrossRef]
- Pramukti, I.; Lindayani, L.; Chen, Y.-C.; Yeh, C.-Y.; Tai, T.-W.; Fetzer, S.; Ko, N.-Y. Bone fracture among people living with HIV: A systematic review and meta-regression of prevalence, incidence, and risk factors. PLoS ONE 2020, 15, e0233501. [Google Scholar] [CrossRef]
- Battalora, L.; Armon, C.; Palella, F.; Li, J.; Overton, E.T.; Hammer, J.; Fuhrer, J.; Novak, R.M.; Carlson, K.; Spear, J.R.; et al. Incident bone fracture and mortality in a large HIV cohort outpatient study, 2000–2017, USA. Arch. Osteoporos. 2021, 16, 117. [Google Scholar] [CrossRef]
- Cotter, E.J.; Ip, H.S.M.; Powderly, W.G.; Doran, P.P. Mechanism of HIV protein induced modulation of mesenchymal stem cell osteogenic differentiation. BMC Musculoskelet. Disord. 2008, 9, 33. [Google Scholar] [CrossRef] [PubMed]
- Beaupere, C.; Garcia, M.; Larghero, J.; Fève, B.; Capeau, J.; Lagathu, C. The HIV proteins Tat and Nef promote human bone marrow mesenchymal stem cell senescence and alter osteoblastic differentiation. Aging Cell 2015, 14, 534–546. [Google Scholar] [CrossRef] [PubMed]
- Cotter, E.J.; Malizia, A.P.; Chew, N.; Powderly, W.G.; Doran, P.P. HIV proteins regulate bone marker secretion and transcription factor activity in cultured human osteoblasts with consequent potential implications for osteoblast function and development. AIDS Res. Hum. Retrovir. 2007, 23, 1521–1530. [Google Scholar] [CrossRef] [PubMed]
- Vikulina, T.; Fan, X.; Yamaguchi, M.; Roser-Page, S.; Zayzafoon, M.; Guidot, D.M.; Ofotokun, I.; Weitzmann, M.N. Alterations in the immuno-skeletal interface drive bone destruction in HIV-1 transgenic rats. Proc. Natl. Acad. Sci. USA 2010, 107, 13848–13853. [Google Scholar] [CrossRef] [PubMed]
- Titanji, K.; Vunnava, A.; Sheth, A.N.; Delille, C.; Lennox, J.L.; Sanford, S.E.; Foster, A.; Knezevic, A.; Easley, K.A.; Weitzmann, M.N.; et al. Dysregulated B cell expression of RANKL and OPG correlates with loss of bone mineral density in HIV infection. PLoS Pathog. 2014, 10, e1004497. [Google Scholar] [CrossRef] [PubMed]
- Chew, N.; Tan, E.; Li, L.; Lim, R. HIV-1 tat and rev upregulates osteoclast bone resorption. J. Int. AIDS Soc. 2014, 17, 19724. [Google Scholar] [CrossRef]
- McGinty, T.; Mirmonsef, P.; Mallon, P.W.; Landay, A.L. Does systemic inflammation and immune activation contribute to fracture risk in HIV? Curr. Opin. HIV AIDS 2016, 11, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Hileman, C.O.; Labbato, D.E.; Storer, N.J.; Tangpricha, V.; McComsey, G.A. Is bone loss linked to chronic inflammation in antiretroviral-naive HIV-infected adults? A 48-week matched cohort study. AIDS 2014, 28, 1759–1767. [Google Scholar] [CrossRef] [PubMed]
- Titanji, K.; Vunnava, A.; Foster, A.; Sheth, A.N.; Lennox, J.L.; Knezevic, A.; Shenvi, N.; Easley, K.A.; Ofotokun, I.; Weitzmann, M.N. T-cell receptor activator of nuclear factor-κB ligand/osteoprotegerin imbalance is associated with HIV-induced bone loss in patients with higher CD4+ T-cell counts. AIDS 2018, 32, 885–894. [Google Scholar] [CrossRef]
- Ahmed, M.; Mital, D.; Abubaker, N.E.; Panourgia, M.; Owles, H.; Papadaki, I.; Ahmed, M.H. Bone Health in People Living with HIV/AIDS: An Update of Where We Are and Potential Future Strategies. Microorganisms 2023, 11, 789. [Google Scholar] [CrossRef]
- Storm-Larsen, C.; Stiksrud, B.; Eriksen, C.; Nowak, P.; Holm, K.; Thalme, A.; Dyrhol-Riise, A.M.; Brix, S.; Hov, J.R.; Trøseid, M. Microbial translocation revisited: Targeting the endotoxic potential of gut microbes in HIV-infected individuals. AIDS 2019, 33, 645–653. [Google Scholar] [CrossRef] [PubMed]
- Gootenberg, D.B.; Paer, J.M.; Luevano, J.-M.; Kwon, D.S. HIV-associated changes in the enteric microbial community: Potential role in loss of homeostasis and development of systemic inflammation. Curr. Opin. Infect. Dis. 2017, 30, 31–43. [Google Scholar] [CrossRef] [PubMed]
- Delpino, M.V.; Quarleri, J. Influence of HIV Infection and Antiretroviral Therapy on Bone Homeostasis. Front. Endocrinol. 2020, 11, 502. [Google Scholar] [CrossRef] [PubMed]
- Mei, Z.; Yin, M.T.; Sharma, A.; Wang, Z.; Peters, B.A.; Chandran, A.; Weber, K.M.; Ross, R.D.; Gustafson, D.; Zheng, Y.; et al. Gut microbiota and plasma metabolites associated with bone mineral density in women with or at risk of HIV infection. AIDS 2023, 37, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Biver, E. Osteoporosis and HIV Infection. Calcif. Tissue Int. 2022, 110, 624–640. [Google Scholar] [CrossRef] [PubMed]
- Vlot, M.C.; Grijsen, M.L.; Prins, J.M.; de Jongh, R.T.; de Jonge, R.; den Heijer, M.; Heijboer, A.C. Effect of antiretroviral therapy on bone turnover and bone mineral density in men with primary HIV-1 infection. PLoS ONE 2018, 13, e0193679. [Google Scholar] [CrossRef] [PubMed]
- McComsey, G.A.; Kitch, D.; Daar, E.S.; Tierney, C.; Jahed, N.C.; Tebas, P.; Myers, L.; Melbourne, K.; Ha, B.; Sax, P.E. Bone mineral density and fractures in antiretroviral-naive persons randomized to receive abacavir-lamivudine or tenofovir disoproxil fumarate-emtricitabine along with efavirenz or atazanavir-ritonavir: Aids Clinical Trials Group A5224s, a substudy of ACTG A5202. J. Infect. Dis. 2011, 203, 1791–1801. [Google Scholar] [CrossRef] [PubMed]
- Stellbrink, H.J.; Orkin, C.; Arribas, J.R.; Compston, J.; Gerstoft, J.; Van Wijngaerden, E.; Lazzarin, A.; Rizzardini, G.; Sprenger, H.G.; Lambert, J.; et al. Comparison of changes in bone density and turnover with abacavir-lamivudine versus tenofovir-emtricitabine in HIV-infected adults: 48-week results from the ASSERT study. Clin. Infect. Dis. 2010, 51, 963–972. [Google Scholar] [CrossRef]
- Han, W.M.; Wattanachanya, L.; Apornpong, T.; Jantrapakde, J.; Avihingsanon, A.; Kerr, S.J.; Teeratakulpisarn, N.; Jadwattanakul, T.; Chaiwatanarat, T.; Buranasupkajorn, P.; et al. Bone mineral density changes among people living with HIV who have started with TDF-containing regimen: A five-year prospective study. PLoS ONE 2020, 15, e0230368. [Google Scholar] [CrossRef]
- Baranek, B.; Wang, S.; Cheung, A.M.; Mishra, S.; Tan, D.H. The effect of tenofovir disoproxil fumarate on bone mineral density: A systematic review and meta-analysis. Antivir. Ther. 2020, 25, 21–32. [Google Scholar] [CrossRef]
- Mathew, G.; Knaus, S.J. Acquired Fanconi’s syndrome associated with tenofovir therapy. J. Gen. Intern. Med. 2006, 21, C3–C5. [Google Scholar] [CrossRef] [PubMed]
- Casado, J.L.; Santiuste, C.; Vazquez, M.; Bañón, S.; Rosillo, M.; Gomez, A.; Perez-Elías, M.J.; Caballero, C.; Rey, J.M.; Moreno, S. Bone mineral density decline according to renal tubular dysfunction and phosphaturia in tenofovir-exposed HIV-infected patients. AIDS 2016, 30, 1423–1431. [Google Scholar] [CrossRef] [PubMed]
- Mothobi, N.Z.; Masters, J.; Marriott, D.J. Fanconi syndrome due to tenofovir disoproxil fumarate reversed by switching to tenofovir alafenamide fumarate in an HIV-infected patient. Ther. Adv. Infect. Dis. 2018, 5, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Pozniak, A.; Arribas, J.R.; Gathe, J.; Gupta, S.K.; Post, F.A.; Bloch, M.; Avihingsanon, A.; Crofoot, G.; Benson, P.; Lichtenstein, K.; et al. Switching to Tenofovir Alafenamide, Coformulated with Elvitegravir, Cobicistat, and Emtricitabine, in HIV-Infected Patients with Renal Impairment: 48-Week Results from a Single-Arm, Multicenter, Open-Label Phase 3 Study. J. Acquir. Immune Defic. Syndr. 2016, 71, 530–537. [Google Scholar] [CrossRef] [PubMed]
- Mills, A.; Arribas, J.R.; Andrade-Villanueva, J.; DiPerri, G.; Van Lunzen, J.; Koenig, E.; Elion, R.; Cavassini, M.; Madruga, J.V.; Brunetta, J.; et al. Switching from tenofovir disoproxil fumarate to tenofovir alafenamide in antiretroviral regimens for virologically suppressed adults with HIV-1 infection: A randomised, active-controlled, multicentre, open-label, phase 3, non-inferiority study. Lancet Infect. Dis. 2016, 16, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Bonjoch, A.; Figueras, M.; Estany, C.; Perez-Alvarez, N.; Rosales, J.; del Rio, L.; di Gregorio, S.; Puig, J.; Gómez, G.; Clotet, B.; et al. High prevalence of and progression to low bone mineral density in HIV-infected patients: A longitudinal cohort study. AIDS 2010, 24, 2827–2833. [Google Scholar] [CrossRef] [PubMed]
- Modarresi, R.; Xiang, Z.; Yin, M.; Laurence, J. WNT/β-catenin signaling is involved in regulation of osteoclast differentiation by human immunodeficiency virus protease inhibitor ritonavir: Relationship to human immunodeficiency virus-linked bone mineral loss. Am. J. Pathol. 2009, 174, 123–135. [Google Scholar] [CrossRef] [PubMed]
- Santiago, F.; Oguma, J.; Brown, A.M.; Laurence, J. Noncanonical Wnt signaling promotes osteoclast differentiation and is facilitated by the human immunodeficiency virus protease inhibitor ritonavir. Biochem. Biophys. Res. Commun. 2012, 417, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Moran, C.A.; Weitzmann, M.N.; Ofotokun, I. The protease inhibitors and HIV-associated bone loss. Curr. Opin. HIV AIDS 2016, 11, 333–342. [Google Scholar] [CrossRef]
- Bonfanti, P.; De Vito, A.; Ricci, E.; Menzaghi, B.; Orofino, G.; Squillace, N.; Molteni, C.; De Socio, G.V.; Salomoni, E.; Celesia, B.M.; et al. Bone Safety of Dolutegravir-Containing Regimens in People Living with HIV: Results from a Real-World Cohort. Infect. Drug Resist. 2020, 13, 2291–2300. [Google Scholar] [CrossRef]
- Hoy, J.F.; Grund, B.; Roediger, M.; Schwartz, A.V.; Shepherd, J.; Avihingsanon, A.; Badal-Faesen, S.; de Wit, S.; Jacoby, S.; La Rosa, A.; et al. Immediate Initiation of Antiretroviral Therapy for HIV Infection Accelerates Bone Loss Relative to Deferring Therapy: Findings from the START Bone Mineral Density Substudy, a Randomized Trial. J. Bone Miner. Res. 2017, 32, 1945–1955. [Google Scholar] [CrossRef] [PubMed]
- Yin, M.T.; Kendall, M.A.; Wu, X.; Tassiopoulos, K.; Hochberg, M.; Huang, J.S.; Glesby, M.J.; Bolivar, H.; McComsey, G.A. Fractures after antiretroviral initiation. AIDS 2012, 26, 2175–2184. [Google Scholar] [CrossRef] [PubMed]
- Ofotokun, I.; Titanji, K.; Vikulina, T.; Roser-Page, S.; Yamaguchi, M.; Zayzafoon, M.; Williams, I.R.; Weitzmann, M.N. Role of T-cell reconstitution in HIV-1 antiretroviral therapy-induced bone loss. Nat. Commun. 2015, 6, 8282. [Google Scholar] [CrossRef] [PubMed]
- Ofotokun, I.; Titanji, K.; Vunnava, A.; Roser-Page, S.; Vikulina, T.; Villinger, F.; Rogers, K.; Sheth, A.N.; Lahiri, C.D.; Lennox, J.L.; et al. Antiretroviral therapy induces a rapid increase in bone resorption that is positively associated with the magnitude of immune reconstitution in HIV infection. AIDS 2016, 30, 405–414. [Google Scholar] [CrossRef] [PubMed]
- Grant, P.M.; Kitch, D.; McComsey, G.A.; Dube, M.P.; Haubrich, R.; Huang, J.; Riddler, S.; Tebas, P.; Zolopa, A.R.; Collier, A.C.; et al. Low baseline CD4+ count is associated with greater bone mineral density loss after antiretroviral therapy initiation. Clin. Infect. Dis. 2013, 57, 1483–1488. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.; Grund, B.; Schwartz, A.V.; Avihingsanon, A.; Badal-Faesen, S.; Bernadino, J.I.; Estrada, V.; La Rosa, A.; Mallon, P.W.G.; Pujari, S.; et al. The rate of bone loss slows after 1–2 years of initial antiretroviral therapy: Final results of the Strategic Timing of Antiretroviral Therapy (START) bone mineral density substudy. HIV Med. 2020, 21, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Biver, E.; Calmy, A.; Delhumeau, C.; Durosier, C.; Zawadynski, S.; Rizzoli, R. Microstructural alterations of trabecular and cortical bone in long-term HIV-infected elderly men on successful antiretroviral therapy. AIDS 2014, 28, 2417–2427. [Google Scholar] [CrossRef] [PubMed]
- Foreman, S.C.; Wu, P.H.; Kuang, R.; John, M.D.; Tien, P.C.; Link, T.M.; Krug, R.; Kazakia, G.J. Factors associated with bone microstructural alterations assessed by HR-pQCT in long-term HIV-infected individuals. Bone 2020, 133, 115210. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, D.L.; Spiegelman, D.; Knox, T.K.; Wilson, I.B. Evolution and predictors of change in total bone mineral density over time in HIV-infected men and women in the nutrition for healthy living study. J. Acquir. Immune Defic. Syndr. 2008, 49, 298–308. [Google Scholar] [CrossRef]
- Young, B.; Dao, C.N.; Buchacz, K.; Baker, R.; Brooks, J.T. Increased rates of bone fracture among HIV-infected persons in the HIV Outpatient Study (HOPS) compared with the US general population, 2000–2006. Clin. Infect. Dis. 2011, 52, 1061–1068. [Google Scholar] [CrossRef]
- Grund, B.; Peng, G.; Gibert, C.L.; Hoy, J.F.; Isaksson, R.L.; Shlay, J.C.; Martinez, E.; Reiss, P.; Visnegarwala, F.; Carr, A.D. Continuous antiretroviral therapy decreases bone mineral density. AIDS 2009, 23, 1519–1529. [Google Scholar] [CrossRef] [PubMed]
- Mueller, N.J.; Fux, C.A.; Ledergerber, B.; Elzi, L.; Schmid, P.; Dang, T.; Magenta, L.; Calmy, A.; Vergopoulos, A.; Bischoff-Ferrari, H.A. High prevalence of severe vitamin D deficiency in combined antiretroviral therapy-naive and successfully treated Swiss HIV patients. AIDS 2010, 24, 1127–1134. [Google Scholar] [CrossRef] [PubMed]
- Dao, C.N.; Patel, P.; Overton, E.T.; Rhame, F.; Pals, S.L.; Johnson, C.; Bush, T.; Brooks, J.T.; The Study to Understand the Natural History of HIV and AIDS in the Era of Effective Therapy (SUN) Investigators. Low vitamin D among HIV-infected adults: Prevalence of and risk factors for low vitamin D Levels in a cohort of HIV-infected adults and comparison to prevalence among adults in the US general population. Clin. Infect. Dis. 2011, 52, 396–405. [Google Scholar] [CrossRef] [PubMed]
- Sherwood, J.E.; Mesner, O.C.; Weintrob, A.C.; Hadigan, C.M.; Wilkins, K.J.; Crum-Cianflone, N.F.; Aronson, N.E. Vitamin D deficiency and its association with low bone mineral density, HIV-related factors, hospitalization, and death in a predominantly black HIV-infected cohort. Clin. Infect. Dis. 2012, 55, 1727–1736. [Google Scholar] [CrossRef] [PubMed]
- Kuehn, E.W.; Anders, H.J.; Bogner, J.R.; Obermaier, J.; Goebel, F.D.; Schlöndorff, D. Hypocalcaemia in HIV infection and AIDS. J. Intern. Med. 1999, 245, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Yoon, V.; Maalouf, N.M.; Sakhaee, K. The effects of smoking on bone metabolism. Osteoporos. Int. 2012, 23, 2081–2092. [Google Scholar] [CrossRef] [PubMed]
- Godos, J.; Giampieri, F.; Chisari, E.; Micek, A.; Paladino, N.; Forbes-Hernández, T.Y.; Quiles, J.L.; Battino, M.; La Vignera, S.; Musumeci, G.; et al. Alcohol Consumption, Bone Mineral Density, and Risk of Osteoporotic Fractures: A Dose-Response Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 1515. [Google Scholar] [CrossRef] [PubMed]
- Kooij, K.W.; Wit, F.W.; Bisschop, P.H.; Schouten, J.; Stolte, I.G.; Prins, M.; van der Valk, M.; Prins, J.M.; van Eck-Smit, B.L.; Lips, P.; et al. Low bone mineral density in patients with well-suppressed HIV infection: Association with body weight, smoking, and prior advanced HIV disease. J. Infect. Dis. 2014, 211, 539–548. [Google Scholar] [CrossRef]
- Thomsen, M.T.; Wiegandt, Y.L.; Gelpi, M.; Knudsen, A.D.; Fuchs, A.; Sigvardsen, P.E.; Kühl, J.T.; Nordestgaard, B.; Køber, L.; Lundgren, J.; et al. Prevalence of and Risk Factors for Low Bone Mineral Density Assessed by Quantitative Computed Tomography in People Living with HIV and Uninfected Controls. J. Acquir. Immune Defic. Syndr. 2020, 83, 165–172. [Google Scholar] [CrossRef]
- Helleberg, M.; Afzal, S.; Kronborg, G.; Larsen, C.S.; Pedersen, G.; Pedersen, C.; Gerstoft, J.; Nordestgaard, B.G.; Obel, N. Mortality Attributable to Smoking Among HIV-1–Infected Individuals: A Nationwide, Population-Based Cohort Study. Clin. Infect. Dis. 2013, 56, 727–734. [Google Scholar] [CrossRef]
- Helleberg, M.; May, M.T.; Ingle, S.M.; Dabis, F.; Reiss, P.; Fätkenheuer, G.; Costagliola, D.; d’Arminio, A.; Cavassini, M.; Smith, C.; et al. Smoking and life expectancy among HIV-infected individuals on antiretroviral therapy in Europe and North America. AIDS 2015, 29, 221–229. [Google Scholar] [CrossRef] [PubMed]
- NIH National Cancer Institute. Available online: https://cancercontrol.cancer.gov/brp/tcrb/tobacco-hiv (accessed on 1 April 2024).
- Oncken, C.; Prestwood, K.; Kleppinger, A.; Wang, Y.; Cooney, J.; Raisz, L. Impact of smoking cessation on bone mineral density in postmenopausal women. J. Women’s Health 2006, 15, 1141–1150. [Google Scholar] [CrossRef] [PubMed]
- Kiyota, Y.; Muramatsu, H.; Sato, Y.; Kobayashi, T.; Miyamoto, K.; Iwamoto, T.; Matsumoto, M.; Nakamura, M.; Tateno, H.; Sato, K.; et al. Smoking cessation increases levels of osteocalcin and uncarboxylated osteocalcin in human sera. Sci. Rep. 2020, 10, 16845. [Google Scholar] [CrossRef] [PubMed]
- Rahmanian, S.; Wewers, M.E.; Koletar, S.; Reynolds, N.; Ferketich, A.; Diaz, P. Cigarette smoking in the HIV-infected population. Proc. Am. Thorac. Soc. 2011, 8, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Samet, J.H.; Cheng, D.M.; Libman, H.; Nunes, D.P.; Alperen, J.K.; Saitz, R. Alcohol consumption and HIV disease progression. J. Acquir. Immune Defic. Syndr. 2007, 46, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Womack, J.A.; Goulet, J.L.; Gibert, C.; Brandt, C.; Chang, C.C.; Gulanski, B.; Fraenkel, L.; Mattocks, K.; Rimland, D.; Rodriguez-Barradas, M.C.; et al. Increased risk of fragility fractures among HIV infected compared to uninfected male veterans. PLoS ONE 2011, 6, e17217. [Google Scholar] [CrossRef] [PubMed]
- Saitz, R.; Mesic, A.; Ventura, A.S.; Winter, M.R.; Heeren, T.C.; Sullivan, M.M.; Walley, A.Y.; Patts, G.J.; Meli, S.M.; Holick, M.F.; et al. Alcohol Consumption and Bone Mineral Density in People with HIV and Substance Use Disorder: A Prospective Cohort Study. Alcohol. Clin. Exp. Res. 2018, 42, 1518–1529. [Google Scholar] [CrossRef]
- Watt, J.; Schuon, J.; Davis, J.; Ferguson, T.F.; Welsh, D.A.; Molina, P.E.; Ronis, M.J.J. Reduced Serum Osteocalcin in High-Risk Alcohol Using People Living with HIV Does Not Correlate with Systemic Oxidative Stress or Inflammation: Data from the New Orleans Alcohol Use in HIV Study. Alcohol. Clin. Exp. Res. 2019, 43, 2374–2383. [Google Scholar] [CrossRef]
- Kim, T.W.; Ventura, A.S.; Winter, M.R.; Heeren, T.C.; Holick, M.F.; Walley, A.Y.; Bryant, K.J.; Saitz, R. Alcohol and Bone Turnover Markers among People Living with HIV and Substance Use Disorder. Alcohol. Clin. Exp. Res. 2020, 44, 992–1000. [Google Scholar] [CrossRef] [PubMed]
- Denys, A.; Norman, A.; Perrien, D.S.; Suva, L.J.; Simon, L.; McDaniel, L.S.; Ferguson, T.; Pedersen, K.; Welsh, D.; Molina, P.E.; et al. Impact of Alcohol on Bone Health in People Living with HIV: Integrating Clinical Data from Serum Bone Markers with Morphometric Analysis in a Non-Human Primate Model. JBMR Plus 2023, 7, e10703. [Google Scholar] [CrossRef]
- Chander, G. Addressing alcohol use in HIV-infected persons. Top. Antivir. Med. 2011, 19, 143–147. [Google Scholar] [PubMed]
- Husain, N.E.; Noor, S.K.; Elmadhoun, W.M.; Almobarak, A.O.; Awadalla, H.; Woodward, C.L.; Mital, D.; Ahmed, M.H. Diabetes, metabolic syndrome and dyslipidemia in people living with HIV in Africa: Re-emerging challenges not to be forgotten. HIV/AIDS Res. Palliat. Care 2017, 9, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Grinspoon, S.; Carr, A. Cardiovascular Risk and Body-Fat Abnormalities in HIV-Infected Adults. N. Engl. J. Med. 2005, 352, 48–62. [Google Scholar] [CrossRef] [PubMed]
- Napoli, N.; Incalzi, R.A.; De Gennaro, G.; Marcocci, C.; Marfella, R.; Papalia, R.; Purrello, F.; Ruggiero, C.; Tarantino, U.; Tramontana, F.; et al. Bone fragility in patients with diabetes mellitus: A consensus statement from the working group of the Italian Diabetes Society (SID), Italian Society of Endocrinology (SIE), Italian Society of Gerontology and Geriatrics (SIGG), Italian Society of Orthopaedics and Traumatology (SIOT). Nutr. Metab. Cardiovasc. Dis. 2021, 31, 1375–1390. [Google Scholar] [CrossRef] [PubMed]
- Shieh, A.; Greendale, G.A.; Cauley, J.A.; Srikanthan, P.; Karlamangla, A.S. Longitudinal associations of insulin resistance with change in bone mineral density in midlife women. JCI Insight 2022, 7, e162085. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Chen, F.; Liu, L.; Zhang, Q. Prevalence of osteoporosis in patients with diabetes mellitus: A systematic review and meta-analysis of observational studies. BMC Endocr. Disord. 2023, 23, 1. [Google Scholar] [CrossRef]
- Kruger, M.J.; Nell, T.A. Bone mineral density in people living with HIV: A narrative review of the literature. AIDS Res. Ther. 2017, 14, 35. [Google Scholar] [CrossRef] [PubMed]
- Caeran, G.; de Almeida, L.L.; Ilha, T.A.S.H.; de Carvalho, J.A.M.; Stein, C.; Moresco, R.N.; Haygert, C.J.P.; Comim, F.V.; Premaor, M.O. Insulin Resistance and Its Association with Osteoporosis in People Living with HIV. J. Endocr. Soc. 2022, 6, bvac148. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; He, P.; Xian, J.; Lu, W.; Shu, J.; Luo, W.; Gan, C.; Ke, R.; Xia, J.; Han, Z.; et al. Association between Nonalcoholic Fatty Liver Disease and Bone Mineral Density in HIV-Infected Patients Receiving Long-term TDF-Based Antiretroviral Therapy. Curr. HIV Res. 2021, 19, 40–46. [Google Scholar] [CrossRef]
- Maffezzoni, F.; Porcelli, T.; Delbarba, A.; Pezzaioli, L.C.; Properzi, M.; Cappelli, C.; Castelli, F.; Quiros-Roldan, M.E.; Ferlin, A. Hypogonadism and bone health in men with HIV. Lancet HIV 2020, 7, e782–e790. [Google Scholar] [CrossRef]
- Pezzaioli, L.C.; Porcelli, T.; Delbarba, A.; Maffezzoni, F.; Focà, E.; Castelli, F.; Cappelli, C.; Ferlin, A.; Quiros-Roldan, M.E. Impact of hypogonadism on bone mineral density and vertebral fractures in HIV-infected men. J. Endocrinol. Investig. 2022, 45, 433–443. [Google Scholar] [CrossRef] [PubMed]
- Teichmann, J.; Lange, U.; Discher, T.; Lohmeyer, J.; Stracke, H.; Bretzel, R.G. Bone mineral density in human immunodeficiency virus-1 infected men with hypogonadism prior to highly-active-antiretroviral-therapy (HAART). Eur. J. Med. Res. 2009, 14, 59. [Google Scholar] [CrossRef] [PubMed]
- Hansen, A.-B.E.; Omland, L.H.; Krarup, H.; Obel, N. Fracture risk in hepatitis C virus infected persons: Results from the DANVIR cohort study. J. Hepatol. 2014, 61, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Wijarnpreecha, K.; Thongprayoon, C.; Panjawatanan, P.; Phatharacharukul, P.; Ungprasert, P. Hepatitis C virus infection and risk of osteoporosis: A meta-analysis. Saudi J. Gastroenterol. 2017, 23, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Lo Re, V., 3rd; Volk, J.; Newcomb, C.W.; Yang, Y.-X.; Freeman, C.P.; Hennessy, S.; Kostman, J.R.; Tebas, P.; Leonard, M.B.; Localio, A.R. Risk of hip fracture associated with hepatitis C virus infection and hepatitis C/human immunodeficiency virus coinfection. Hepatology 2012, 56, 1688–1698. [Google Scholar] [CrossRef] [PubMed]
- Carrero, A.; Berenguer, J.; Hontañón, V.; Guardiola, J.M.; Navarro, J.; von Wichmann, M.A.; Téllez, M.J.; Quereda, C.; Santos, I.; Sanz, J.; et al. Effects of Hepatitis C Virus (HCV) Eradication on Bone Mineral Density in Human Immunodeficiency Virus/HCV-Coinfected Patients. Clin. Infect. Dis. 2021, 73, e2026–e2033. [Google Scholar] [CrossRef] [PubMed]
- Aberg, J.A.; Gallant, J.E.; Ghanem, K.G.; Emmanuel, P.; Zingman, B.S.; Horberg, M.A. Primary care guidelines for the management of persons infected with HIV: 2013 update by the HIV Medicine Association of the Infectious Diseases Society of America. Clin. Infect. Dis. 2014, 58, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Blake, G.M.; Fogelman, I. The clinical role of dual energy X-ray absorptiometry. Eur. J. Radiol. 2009, 71, 406–414. [Google Scholar] [CrossRef] [PubMed]
- Kanis, J.A.; McCloskey, E.; Johansson, H.; Oden, A.; Leslie, W.D. FRAX® with and without bone mineral density. Calcif. Tissue Int. 2012, 90, 1–13. [Google Scholar] [CrossRef]
- Mazzitelli, M.; Branca Isabel, P.; Muramatsu, T.; Chirwa, M.; Mandalia, S.; Moyle, G.; Marta, B.; Milinkovic, A. FRAX assessment in people ageing with HIV. HIV Med. 2022, 23, 103–108. [Google Scholar] [CrossRef]
- European Aids Clinical Society Guidelines Version 12.0. Available online: https://eacs.sanfordguide.com/prevention-non-infectious-co-morbidities/bone-disease-screening-dx (accessed on 1 April 2024).
- Vizcarra, P.; Gallego, J.; Vivancos, M.J.; Sifuentes, W.A.; Llop, M.; Casado, J.L. Evaluation of the fracture risk assessment tool for determining bone disease and the impact of secondary causes of osteoporosis in people living with HIV. HIV Res. Clin. Pract. 2020, 21, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Gourlay, M.L.; Fine, J.P.; Preisser, J.S.; May, R.C.; Li, C.; Lui, L.Y.; Ransohoff, D.F.; Cauley, J.A.; Ensrud, K.E. Bone-density testing interval and transition to osteoporosis in older women. N. Engl. J. Med. 2012, 366, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Negredo, E.; Bonjoch, A.; Gómez-Mateu, M.; Estany, C.; Puig, J.; Perez-Alvarez, N.; Rosales, J.; di Gregorio, S.; del Rio, L.; Gómez, G.; et al. Time of progression to osteopenia/osteoporosis in chronically HIV-infected patients: Screening DXA scan. PLoS ONE 2012, 7, e46031. [Google Scholar] [CrossRef] [PubMed]
- Adami, S.; Maggi, P.; Montinaro, V.; Povero, M.; Pradelli, L.; Bellagamba, R.; Bonfanti, P.; Di Biagio, A.; Rusconi, S.; Di Campli, F.M.; et al. Simulating the development and progression of Chronic Kidney Disease and osteoporosis in people living with HIV. Farmeconomia. Health Econ. Ther. Pathw. 2016, 17, 3–23. [Google Scholar] [CrossRef]
- Adams, J.E. Advances in bone imaging for osteoporosis. Nat. Rev. Endocrinol. 2013, 9, 28–42. [Google Scholar] [CrossRef] [PubMed]
- Lenchik, L.; Rogers, L.F.; Delmas, P.D.; Genant, H.K. Diagnosis of Osteoporotic Vertebral Fractures: Importance of Recognition and Description by Radiologists. Am. J. Roentgenol. 2004, 183, 949–958. [Google Scholar] [CrossRef] [PubMed]
- Khaw, K.-T.; Reeve, J.; Luben, R.; Bingham, S.; Welch, A.; Wareham, N.; Oakes, S.; Day, N. Prediction of total and hip fracture risk in men and women by quantitative ultrasound of the calcaneus: EPIC-Norfolk prospective population study. Lancet 2004, 363, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Glüer, C.C.; Wu, C.Y.; Jergas, M.; Goldstein, S.A.; Genant, H.K. Three quantitative ultrasound parameters reflect bone structure. Calcif. Tissue Int. 1994, 55, 46–52. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Cournil, A.; Eymard-Duvernay, S.; Diouf, A.; Moquet, C.; Coutherut, J.; Gueye, N.F.N.; Cames, C.; Taverne, B.; Bork, K.; Sow, P.S.; et al. Reduced Quantitative Ultrasound Bone Mineral Density in HIV-Infected Patients on Antiretroviral Therapy in Senegal. PLoS ONE 2012, 7, e31726. [Google Scholar] [CrossRef]
- Marocco, R.; Martini, H.; Belvisi, V.; Tieghi, T.; Cesareo, R.; Del Borgo, C.; Lichtner, M.; Mastroianni, C.M. Quantitative ultrasound (QUS) in HIV-infected patients: A reliable and low-cost technique for bone health assessment. J. Int. AIDS Soc. 2010, 13, P98. [Google Scholar] [CrossRef]
- Wyatt, C.M.; Winston, J.A.; Malvestutto, C.D.; Fishbein, D.A.; Barash, I.; Cohen, A.J.; Klotman, M.E.; Klotman, P.E. Chronic kidney disease in HIV infection: An urban epidemic. AIDS 2007, 21, 2101–2103. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, E.; Campbell, L.; Tinago, W.; Garcia-Leon, A.; Walsh, I.; Brady, J.J.; Burling, K.; Noe, S.; Neuville, M.F.; Jouret, F.; et al. The renal-bone axis in older people living with HIV on stable antiretroviral therapy: A sub-analysis of the GS-US-104-0423 study. Antivir. Ther. 2022, 27, 13596535221094898. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.J.; Gwetu, T.; Labadarios, D.; Muller, E.; Veldman, F.J.; Ellis, C.; Kassier, S.M. Prevalence of osteoporosis and factors associated with bone density in HIV-positive kidney transplant candidates and recipients from an HIV-positive donor. S. Afr. J. Clin. Nutr. 2023. [Google Scholar] [CrossRef]
- Grant, P.M.; Cotter, A.G. Tenofovir and bone health. Curr. Opin. HIV AIDS 2016, 11, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.T.; McComsey, G.A. Osteopenia and osteoporosis in patients with HIV: A review of current concepts. Curr. Infect. Dis. Rep. 2006, 8, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Overton, E.T.; Chan, E.S.; Brown, T.T.; Tebas, P.; McComsey, G.A.; Melbourne, K.M.; Napoli, A.; Hardin, W.R.; Ribaudo, H.J.; Yin, M.T. Vitamin D and Calcium Attenuate Bone Loss with Antiretroviral Therapy Initiation: A Randomized Trial. Ann. Intern. Med. 2015, 162, 815–824. [Google Scholar] [CrossRef]
- Havens, P.L.; Stephensen, C.B.; Van Loan, M.D.; Schuster, G.U.; Woodhouse, L.R.; Flynn, P.M.; Gordon, C.M.; Pan, C.G.; Rutledge, B.; Harris, D.R.; et al. Vitamin D3 Supplementation Increases Spine Bone Mineral Density in Adolescents and Young Adults with Human Immunodeficiency Virus Infection Being Treated with Tenofovir Disoproxil Fumarate: A Randomized, Placebo-Controlled Trial. Clin. Infect. Dis. 2018, 66, 220–228. [Google Scholar] [CrossRef]
- Singhato, A.; Khongkhon, S.; Rueangsri, N.; Booranasuksakul, U. Effectiveness of Medical Nutrition Therapy to Improve Dietary Habits for Promoting Bone Health in People Living with Chronic HIV. Ann. Nutr. Metab. 2020, 76, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Li Vecchi, V.; Soresi, M.; Giannitrapani, L.; Mazzola, G.; La Sala, S.; Tramuto, F.; Caruso, G.; Colomba, C.; Mansueto, P.; Madonia, S.; et al. Dairy calcium intake and lifestyle risk factors for bone loss in HIV-infected and uninfected Mediterranean subjects. BMC Infect. Dis. 2012, 12, 192. [Google Scholar] [CrossRef]
- Pinzone, M.R.; Moreno, S.; Cacopardo, B.; Nunnari, G. Is there enough evidence to use bisphosphonates in HIV-infected patients? A systematic review and meta-analysis. AIDS Rev. 2014, 16, 213–222. [Google Scholar]
- Rocha, V.M.D.; Faria, M.B.B.; Júnior, F.; Lima, C.; Fiorelli, R.K.A.; Cassiano, K.M. Use of Bisphosphonates, Calcium and Vitamin D for Bone Demineralization in Patients with Human Immunodeficiency Virus/Acquired Immune Deficiency Syndrome: A Systematic Review and Meta-Analysis of Clinical Trials. J. Bone Metab. 2020, 27, 175–186. [Google Scholar] [CrossRef]
- Mondy, K.; Powderly, W.G.; Claxton, S.A.; Yarasheski, K.H.; Royal, M.; Stoneman, J.S.; Hoffmann, M.E.; Tebas, P. Alendronate, vitamin D, and calcium for the treatment of osteopenia/osteoporosis associated with HIV infection. J. Acquir. Immune Defic. Syndr. 2005, 38, 426–431. [Google Scholar] [CrossRef]
- McComsey, G.A.; Kendall, M.A.; Tebas, P.; Swindells, S.; Hogg, E.; Alston-Smith, B.; Suckow, C.; Gopalakrishnan, G.; Benson, C.; Wohl, D.A. Alendronate with calcium and vitamin D supplementation is safe and effective for the treatment of decreased bone mineral density in HIV. AIDS 2007, 21, 2473–2482. [Google Scholar] [CrossRef]
- Carr, A.; Kerr, S.J.; Richardson, R.; Ebeling, P.; Pocock, N.; Rojas, J.; Martinez, E.; Hoy, J.; ZEST Study Investigators. Prolonged Effect of Zoledronic Acid on Bone Mineral Density and Turnover in HIV-Infected Adults on Tenofovir: A Randomized, Open-Label Study. J. Bone Miner. Res. 2019, 34, 2192–2197. [Google Scholar] [CrossRef]
- Huang, J.; Meixner, L.; Fernandez, S.; McCutchan, J.A. A double-blinded, randomized controlled trial of zoledronate therapy for HIV-associated osteopenia and osteoporosis. AIDS 2009, 23, 51–57. [Google Scholar] [CrossRef]
- Bolland, M.J.; Grey, A.B.; Horne, A.M.; Briggs, S.E.; Thomas, M.G.; Ellis-Pegler, R.B.; Woodhouse, A.F.; Gamble, G.D.; Reid, I.R. Annual zoledronate increases bone density in highly active antiretroviral therapy-treated human immunodeficiency virus-infected men: A randomized controlled trial. J. Clin. Endocrinol. Metab. 2007, 92, 1283–1288. [Google Scholar] [CrossRef]
- Bolland, M.J.; Horne, A.M.; Briggs, S.E.; Thomas, M.G.; Reid, I.; Gamble, G.D.; Grey, A. Effects of Intravenous Zoledronate on Bone Turnover and Bone Density Persist for at Least 11 Years in HIV-Infected Men. J. Bone Miner. Res. 2019, 34, 1248–1253. [Google Scholar] [CrossRef]
- Hoy, J.F.; Richardson, R.; Ebeling, P.R.; Rojas, J.; Pocock, N.; Kerr, S.J.; Martinez, E.; Carr, A. Zoledronic acid is superior to tenofovir disoproxil fumarate-switching for low bone mineral density in adults with HIV. AIDS 2018, 32, 1967–1975. [Google Scholar] [CrossRef]
- Ofotokun, I.; Titanji, K.; Lahiri, C.D.; Vunnava, A.; Foster, A.; Sanford, S.E.; Sheth, A.N.; Lennox, J.L.; Knezevic, A.; Ward, L.; et al. A Single-dose Zoledronic Acid Infusion Prevents Antiretroviral Therapy-induced Bone Loss in Treatment-naive HIV-infected Patients: A Phase IIb Trial. Clin. Infect. Dis. 2016, 63, 663–671. [Google Scholar] [CrossRef]
- Huang, X.-L.; Liu, C.; Shi, X.-M.; Cheng, Y.-T.; Zhou, Q.; Li, J.-P.; Liao, J. Zoledronic acid inhibits osteoclastogenesis and bone resorptive function by suppressing RANKL-mediated NF-κB and JNK and their downstream signalling pathways. Mol. Med. Rep. 2022, 25, 59. [Google Scholar] [CrossRef]
- Lin, W.; Li, X.-F.; Ren, D.-C.; Song, M.; Duan, L.; Liu, J.-Z.; Zhan, Z.-R. Administration of zoledronic acid alleviates osteoporosis in HIV patients by suppressing osteoclastogenesis via regulating RANKL expression. Mol. Med. 2021, 27, 19. [Google Scholar] [CrossRef]
- Makras, P.; Petrikkos, P.; Anastasilakis, A.D.; Kolynou, A.; Katsarou, A.; Tsachouridou, O.; Metallidis, S.; Yavropoulou, M.P. Denosumab versus zoledronate for the treatment of low bone mineral density in male HIV-infected patients. Bone Rep. 2021, 15, 101128. [Google Scholar] [CrossRef]
- Chisati, E.M.; Constantinou, D.; Lampiao, F. Management of Reduced Bone Mineral Density in HIV: Pharmacological Challenges and the Role of Exercise. Front. Physiol. 2018, 9, 1074. [Google Scholar] [CrossRef]
- Perazzo, J.D.; Webel, A.R.; Alam, K.S.M.; Sattar, A.; McComsey, G.A. Relationships Between Physical Activity and Bone Density in People Living with HIV: Results from the SATURN-HIV Study. J. Assoc. Nurses AIDS Care 2018, 29, 528–537. [Google Scholar] [CrossRef]
- Ellis, C.; Kruger, H.S.; Viljoen, M.; Dave, J.A.; Kruger, M.C. Factors Associated with Bone Mineral Density and Bone Resorption Markers in Postmenopausal HIV-Infected Women on Antiretroviral Therapy: A Prospective Cohort Study. Nutrients 2021, 13, 2090. [Google Scholar] [CrossRef]
- Chisati, E.M.; Constantinou, D.; Lampiao, F. Effects of maximal strength training on bone mineral density in people living with HIV and receiving anti-retroviral therapy: A pilot study. BMC Sports Sci. Med. Rehabil. 2020, 12, 67. [Google Scholar] [CrossRef]
- Santos, W.R.; Santos, W.R.; Paes, P.P.; Ferreira-Silva, I.A.; Santos, A.P.; Vercese, N.; Machado, D.R.; de Paula, F.J.; Donadi, E.A.; Navarro, A.M.; et al. Impact of Strength Training on Bone Mineral Density in Patients Infected with HIV Exhibiting Lipodystrophy. J. Strength Cond. Res. 2015, 29, 3466–3471. [Google Scholar] [CrossRef]
- Fairfield, W.P.; Finkelstein, J.S.; Klibanski, A.; Grinspoon, S.K. Osteopenia in eugonadal men with acquired immune deficiency syndrome wasting syndrome. J. Clin. Endocrinol. Metab. 2001, 86, 2020–2026. [Google Scholar] [CrossRef]
- Grant, P.M.; Li, X.; Jacobson, L.P.; Palella, F.J., Jr.; Kingsley, L.A.; Margolick, J.B.; Dobs, A.S.; Lake, J.E.; Althoff, K.N.; Brown, T.T. Effect of Testosterone Use on Bone Mineral Density in HIV-Infected Men. AIDS Res. Hum. Retrovir. 2019, 35, 75–80. [Google Scholar] [CrossRef]
- Erlandson, K.M.; Allshouse, A.A.; Jankowski, C.M.; Duong, S.; MaWhinney, S.; Kohrt, W.M.; Campbell, T.B. Risk factors for falls in HIV-infected persons. J. Acquir. Immune Defic. Syndr. 2012, 61, 484–489. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schinas, G.; Schinas, I.; Ntampanlis, G.; Polyzou, E.; Gogos, C.; Akinosoglou, K. Bone Disease in HIV: Need for Early Diagnosis and Prevention. Life 2024, 14, 522. https://doi.org/10.3390/life14040522
Schinas G, Schinas I, Ntampanlis G, Polyzou E, Gogos C, Akinosoglou K. Bone Disease in HIV: Need for Early Diagnosis and Prevention. Life. 2024; 14(4):522. https://doi.org/10.3390/life14040522
Chicago/Turabian StyleSchinas, Georgios, Ioannis Schinas, Georgios Ntampanlis, Eleni Polyzou, Charalambos Gogos, and Karolina Akinosoglou. 2024. "Bone Disease in HIV: Need for Early Diagnosis and Prevention" Life 14, no. 4: 522. https://doi.org/10.3390/life14040522
APA StyleSchinas, G., Schinas, I., Ntampanlis, G., Polyzou, E., Gogos, C., & Akinosoglou, K. (2024). Bone Disease in HIV: Need for Early Diagnosis and Prevention. Life, 14(4), 522. https://doi.org/10.3390/life14040522