
Impact of Plasminogen Activator Inhibitor-1 Serum Levels and the -675 4G/5G Variant in the SERPINE1 Gene on Systemic Sclerosis in a Mexican Population

 ,
,  , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. DNA Extraction and Genotyping
2.3. Levels of Soluble PAI-1 and Soluble TGF-β (sTGF-β) Isoforms
2.4. Autoantibodies
2.5. Statistical Analyses
3. Results
3.1. Clinical and Demographic Characteristics
3.2. Variant Distribution in SSc Patients and CSs
3.3. Soluble Levels of PAI-1 in SSc Patients and CS
3.4. SERPINE1 Genetic Variant and Clinical Parameters of SSc Patients
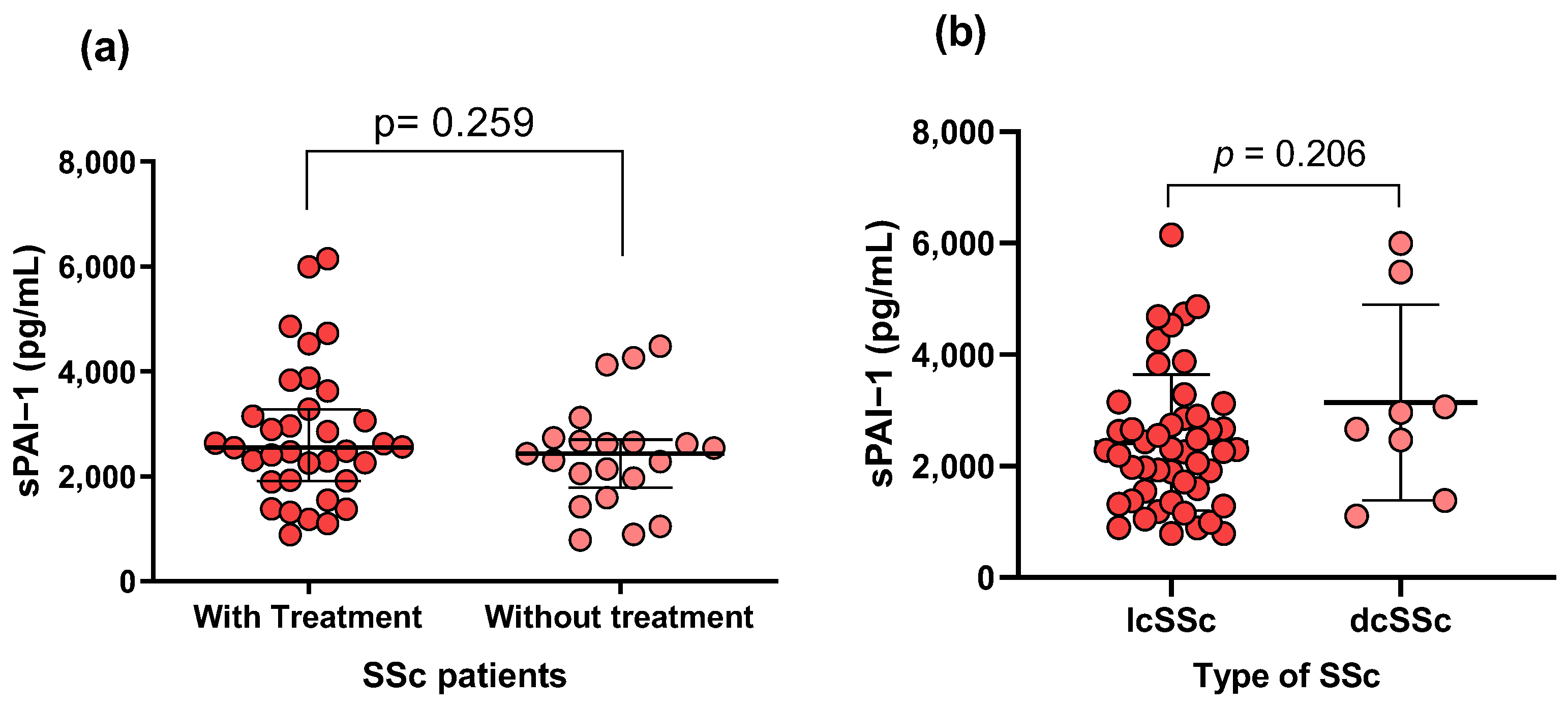
3.5. Association of sPAI-1 Levels with Clinical and Laboratory Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Campochiaro, C.; Allanore, Y. An Update on Targeted Therapies in Systemic Sclerosis Based on a Systematic Review from the Last 3 Years. Arthritis Res. Ther. 2021, 23, 155. [Google Scholar] [CrossRef]
- AlMehmadi, B.A.; To, F.Z.; Anderson, M.A.; Johnson, S.R. Epidemiology and Treatment of Peripheral Neuropathy in Systemic Sclerosis. J. Rheumatol. 2021, 48, 1839–1849. [Google Scholar] [CrossRef]
- Qiu, M.; Nian, X.; Pang, L.; Yu, P.; Zou, S. Prevalence and Risk Factors of Systemic Sclerosis-associated Interstitial Lung Disease in East Asia: A Systematic Review and Meta-analysis. Int. J. Rheum. Dis. 2021, 24, 1449–1459. [Google Scholar] [CrossRef]
- Fischer, A.; Zimovetz, E.; Ling, C.; Esser, D.; Schoof, N. Humanistic and Cost Burden of Systemic Sclerosis: A Review of the Literature. Autoimmun. Rev. 2017, 16, 1147–1154. [Google Scholar] [CrossRef]
- Schmid, M.; Berset, D.G.; Krief, P.; Cherix, A.Z.; Danuser, B.; Rinaldo, M. Should Systemic Sclerosis Be Recognised as an Occupational Disease in Switzerland? Swiss Med. Wkly. 2020, 150, w20193. [Google Scholar] [CrossRef]
- Zuo, X.; Zhang, L.; Luo, H.; Li, Y.; Zhu, H. Systematic Approach to Understanding the Pathogenesis of Systemic Sclerosis. Clin. Genet. 2017, 92, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Kanno, Y.; Shu, E. A2-Antiplasmin as a Potential Therapeutic Target for Systemic Sclerosis. Life 2022, 12, 396. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Jin, Y.; Li, X.; Peng, X.; Peng, N.; Song, J.; Xu, M. Plasminogen Activator Inhibitor-1 (PAI-1) 4G/5G Promoter Polymorphisms and Risk of Venous Thromboembolism—A Meta-Analysis and Systematic Review. Vasa 2020, 49, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Kato, S.; Inui, N.; Hakamata, A.; Suzuki, Y.; Enomoto, N.; Fujisawa, T.; Nakamura, Y.; Watanabe, H.; Suda, T. Changes in Pulmonary Endothelial Cell Properties during Bleomycin-Induced Pulmonary Fibrosis. Respir. Res. 2018, 19, 127. [Google Scholar] [CrossRef]
- Sillen, M.; Declerck, P.J. A Narrative Review on Plasminogen Activator Inhibitor-1 and Its (Patho)Physiological Role: To Target or Not to Target? Int. J. Mol. Sci. 2021, 22, 2721. [Google Scholar] [CrossRef]
- Postiglione, L.; Montuori, N.; Riccio, A.; Di Spigna, G.; Salzano, S.; Rossi, G.; Ragno, P. The Plasminogen Activator System in Fibroblasts from Systemic Sclerosis. Int. J. Immunopathol. Pharmacol. 2010, 23, 891–900. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Valle, J.F.; Ruiz-Quezada, S.L.; Oregón-Romero, E.; Navarro-Hernández, R.E.; Castañeda-Saucedo, E.; De la Cruz-Mosso, U.; Illades-Aguiar, B.; Leyva-Vázquez, M.A.; Castro-Alarcón, N.; Parra-Rojas, I. PAI-1 mRNA Expression and Plasma Level in Rheumatoid Arthritis: Relationship with 4G/5G PAI-1 Polymorphism. Rheumatol. Int. 2012, 32, 3951–3956. [Google Scholar] [CrossRef] [PubMed]
- Kanno, Y. The Role of Fibrinolytic Regulators in Vascular Dysfunction of Systemic Sclerosis. Int. J. Mol. Sci. 2019, 20, 619. [Google Scholar] [CrossRef]
- Bandinelli, F.; Bartoli, F.; Perfetto, E.; Del Rosso, A.; Moggi-Pignone, A.; Guiducci, S.; Cinelli, M.; Fatini, C.; Generini, S.; Gabrielli, A.; et al. The Fibrinolytic System Components Are Increased in Systemic Sclerosis and Modulated by Alprostadil (Alpha1 Ciclodestryn). Clin. Exp. Rheumatol. 2005, 23, 671–677. [Google Scholar]
- Yousef, A.A.; Mohamed, F.Y.; Boraey, N.F.; Akeel, N.E.; Soliman, A.A.; Waked, N.M.; Hashem, M.I.A.; Shehata, H.; Fahmy, D.S.; Ismael, A.; et al. Association of Plasminogen Activator Inhibitor 1 (PAI-1) 4G/5G Polymorphism and Susceptibility to SLE in Egyptian Children and Adolescents: A Multicenter Study. J. Inflamm. Res. 2020, 13, 1103–1111. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Zhou, M.; Lin, M.; Liang, S.; Yan, Y.; Wang, S.; Fang, C.; Li, D.; Ruan, Y. Research Progress on the SERPINE1 Protein and Chronic Inflammatory Diseases of the Upper Respiratory Tract: A Literature Review. Int. Arch. Allergy Immunol. 2021, 182, 1097–1102. [Google Scholar] [CrossRef] [PubMed]
- Sotos-Prieto, M.; Guillén, M.; Portolés, O.; Sorlí, J.V.; González, J.I.; Asensio, E.M.; Corella, D. Association between the Rs6950982 Polymorphism near the SERPINE1 Gene and Blood Pressure and Lipid Parameters in a High-Cardiovascular-Risk Population: Interaction with Mediterranean Diet. Genes Nutr. 2013, 8, 401–409. [Google Scholar] [CrossRef]
- Anaya-Macias, B.U.; De la Cruz-Mosso, U.; Palafox-Sánchez, C.A.; Parra-Rojas, I.; Martínez-Bonilla, G.; González-López, L.; Gámez-Nava, J.I.; Pérez-Guerrero, E.E.; Barrientos-Avalos, S.L.; Muñoz-Valle, J.F. The -675 4G/5G PAI-1 Polymorphism Confers Genetic Susceptibility to Systemic Lupus Erythematosus, Its Clinical Manifestations, and Comorbidities in Mexican-Mestizo Population. Autoimmunity 2020, 53, 71–77. [Google Scholar] [CrossRef]
- Eriksson, P.; Kallin, B.; van’t Hooft, F.M.; Båvenholm, P.; Hamsten, A. Allele-Specific Increase in Basal Transcription of the Plasminogen-Activator Inhibitor 1 Gene Is Associated with Myocardial Infarction. Proc. Natl. Acad. Sci. USA 1995, 92, 1851–1855. [Google Scholar] [CrossRef]
- Choi, G.H.; Cho, S.H.; An, H.J.; Park, H.S.; Lee, J.Y.; Ko, E.J.; Oh, S.H.; Kim, O.J.; Kim, N.K. Association between PAI-1 Polymorphisms and Ischemic Stroke in a South Korean Case-Control Cohort. Int. J. Mol. Sci. 2023, 24, 8041. [Google Scholar] [CrossRef]
- van den Hoogen, F.; Khanna, D.; Fransen, J.; Johnson, S.R.; Baron, M.; Tyndall, A.; Matucci-Cerinic, M.; Naden, R.P.; Medsger, T.A.; Carreira, P.E.; et al. 2013 Classification Criteria for Systemic Sclerosis: An American College of Rheumatology/European League against Rheumatism Collaborative Initiative. Ann. Rheum. Dis. 2013, 72, 1747–1755. [Google Scholar] [CrossRef] [PubMed]
- Miller, S.A.; Dykes, D.D.; Polesky, H.F. A Simple Salting out Procedure for Extracting DNA from Human Nucleated Cells. Nucleic Acids Res. 1988, 16, 1215. [Google Scholar] [CrossRef] [PubMed]
- Lomelí-Nieto, J.A.; Muñoz-Valle, J.F.; Baños-Hernández, C.J.; Navarro-Zarza, J.E.; Godínez-Rubí, J.M.; García-Arellano, S.; Ramírez-Dueñas, M.G.; Parra-Rojas, I.; Villanueva-Pérez, A.; Hernández-Bello, J. Transforming Growth Factor Beta Isoforms and TGF-βR1 and TGF-βR2 Expression in Systemic Sclerosis Patients. Clin. Exp. Med. 2023, 23, 471–481. [Google Scholar] [CrossRef] [PubMed]
- Schumacher, H.R. Joint Involvement in Progressive Systemic Sclerosis (Scleroderma): A Light and Electron Microscopic Study of Synovial Membrane and Fluid. Am. J. Clin. Pathol. 1973, 60, 593–600. [Google Scholar] [CrossRef]
- Wållberg-Jonsson, S.; Rantapää-Dahlqvist, S.; Nordmark, L.; Rånby, M. Mobilization of Fibrinolytic Enzymes in Synovial Fluid and Plasma of Rheumatoid Arthritis and Spondyloarthropathy and Their Relation to Radiological Destruction. J. Rheumatol. 1996, 23, 1704–1709. [Google Scholar]
- Dimitroulas, T.; Douglas, K.M.J.; Panoulas, V.F.; Toms, T.; Smith, J.P.; Treharne, G.J.; Nightingale, P.; Hodson, J.; Kitas, G.D. Derangement of Hemostasis in Rheumatoid Arthritis: Association with Demographic, Inflammatory and Metabolic Factors. Clin. Rheumatol. 2013, 32, 1357–1364. [Google Scholar] [CrossRef]
- de Sá, M.C.; Simão, A.N.C.; de Medeiros, F.A.; Iriyoda, T.M.V.; Costa, N.T.; Alfieri, D.F.; Flauzino, T.; Sekiguchi, B.A.; Lozovoy, M.A.B.; Reiche, E.M.V.; et al. Cell Adhesion Molecules and Plasminogen Activator Inhibitor Type-1 (PAI-1) in Patients with Rheumatoid Arthritis: Influence of Metabolic Syndrome. Clin. Exp. Med. 2018, 18, 495–504. [Google Scholar] [CrossRef]
- Bicakcigil, M.; Tasan, D.; Tasdelen, N.; Mutlu, N.; Yavuz, S. Role of Fibrinolytic Parameters and Plasminogen Activator Inhibitor 1 (PAI-1) Promoter Polymorphism on Premature Atherosclerosis in SLE Patients. Lupus 2011, 20, 1063–1071. [Google Scholar] [CrossRef]
- Bae, S.-C.; Lee, Y.H. Association between Plasminogen Activator Inhibitor-1 (PAI-1) 4G/5G Polymorphism and Circulating PAI-1 Level in Systemic Lupus Erythematosus and Rheumatoid Arthritis: A Meta-Analysis. Z. Rheumatol. 2020, 79, 312–318. [Google Scholar] [CrossRef]
- Lemaire, R.; Burwell, T.; Sun, H.; Delaney, T.; Bakken, J.; Cheng, L.; Rebelatto, M.C.; Czapiga, M.; de-Mendez, I.; Coyle, A.J.; et al. Resolution of Skin Fibrosis by Neutralization of the Antifibrinolytic Function of Plasminogen Activator Inhibitor 1. Arthritis Rheumatol. 2016, 68, 473–483. [Google Scholar] [CrossRef]
- Matsushita, M.; Yamamoto, T.; Nishioka, K. Plasminogen Activator Inhibitor-1 Is Elevated, but Not Essential, in the Development of Bleomycin-Induced Murine Scleroderma. Clin. Exp. Immunol. 2005, 139, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, A.K.; Vaughan, D.E. PAI-1 in Tissue Fibrosis. J. Cell Physiol. 2012, 227, 493–507. [Google Scholar] [CrossRef]
- Ames, P.R.; Lupoli, S.; Alves, J.; Atsumi, T.; Edwards, C.; Iannaccone, L.; Khamashta, M.A.; Hughes, G.R.; Brancaccio, V. The Coagulation/Fibrinolysis Balance in Systemic Sclerosis: Evidence for a Haematological Stress Syndrome. Br. J. Rheumatol. 1997, 36, 1045–1050. [Google Scholar] [CrossRef]
- Rabieian, R.; Boshtam, M.; Zareei, M.; Kouhpayeh, S.; Masoudifar, A.; Mirzaei, H. Plasminogen Activator Inhibitor Type-1 as a Regulator of Fibrosis. J. Cell Biochem. 2018, 119, 17–27. [Google Scholar] [CrossRef]
- Samarakoon, R.; Higgins, C.E.; Higgins, S.P.; Higgins, P.J. TGF-Β1-Induced Expression of the Poor Prognosis SERPINE1/PAI-1 Gene Requires EGFR Signaling: A New Target for Anti-EGFR Therapy. J. Oncol. 2009, 2009, 342391. [Google Scholar] [CrossRef]
- Samarakoon, R.; Higgins, S.P.; Higgins, C.E.; Higgins, P.J. TGF-Β1-Induced Plasminogen Activator Inhibitor-1 Expression in Vascular Smooth Muscle Cells Requires Pp60c-Src/EGFRY845 and Rho/ROCK Signaling. J. Mol. Cell Cardiol. 2008, 44, 527–538. [Google Scholar] [CrossRef]
- Imai, J.; Yahata, T.; Ichikawa, H.; Ibrahim, A.A.; Yazawa, M.; Sumiyoshi, H.; Inagaki, Y.; Matsushima, M.; Suzuki, T.; Mine, T.; et al. Inhibition of Plasminogen Activator Inhibitor-1 Attenuates against Intestinal Fibrosis in Mice. Intest. Res. 2020, 18, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.Q.; Sloan-Lancaster, J.; Berg, D.T.; Richardson, M.A.; Grinnell, B.; Tseng-Crank, J. Differential Mechanisms of Plasminogen Activator Inhibitor-1 Gene Activation by Transforming Growth Factor-Beta and Tumor Necrosis Factor-Alpha in Endothelial Cells. Thromb. Haemost. 2001, 86, 1563–1572. [Google Scholar] [CrossRef] [PubMed]
- Peoples, C.; Medsger, T.A.; Lucas, M.; Rosario, B.L.; Feghali-Bostwick, C.A. Gender Differences in Systemic Sclerosis: Relationship to Clinical Features, Serologic Status and Outcomes. J. Scleroderma Relat. Disord. 2016, 1, 177–240. [Google Scholar] [CrossRef]
- Cesari, M.; Pahor, M.; Incalzi, R.A. Plasminogen Activator Inhibitor-1 (PAI-1): A Key Factor Linking Fibrinolysis and Age-Related Subclinical and Clinical Conditions. Cardiovasc. Ther. 2010, 28, e72–e91. [Google Scholar] [CrossRef]
- Yamamoto, K.; Takeshita, K.; Kojima, T.; Takamatsu, J.; Saito, H. Aging and Plasminogen Activator Inhibitor-1 (PAI-1) Regulation: Implication in the Pathogenesis of Thrombotic Disorders in the Elderly. Cardiovasc. Res. 2005, 66, 276–285. [Google Scholar] [CrossRef]
- Heiman, M.; Gupta, S.; Lewandowska, M.; Shapiro, A.D. Complete Plasminogen Activator Inhibitor 1 Deficiency. In GeneReviews®; Adam, M.P., Feldman, J., Mirzaa, G.M., Pagon, R.A., Wallace, S.E., Bean, L.J., Gripp, K.W., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 1993. [Google Scholar]
- Brogren, H.; Karlsson, L.; Andersson, M.; Wang, L.; Erlinge, D.; Jern, S. Platelets Synthesize Large Amounts of Active Plasminogen Activator Inhibitor 1. Blood 2004, 104, 3943–3948. [Google Scholar] [CrossRef]
- Brogren, H.; Wallmark, K.; Deinum, J.; Karlsson, L.; Jern, S. Platelets Retain High Levels of Active Plasminogen Activator Inhibitor 1. PLoS ONE 2011, 6, e26762. [Google Scholar] [CrossRef] [PubMed]
- Pandolfi, A.; Cetrullo, D.; Polishuck, R.; Alberta, M.M.; Calafiore, A.; Pellegrini, G.; Vitacolonna, E.; Capani, F.; Consoli, A. Plasminogen Activator Inhibitor Type 1 Is Increased in the Arterial Wall of Type II Diabetic Subjects. Arterioscler. Thromb. Vasc. Biol. 2001, 21, 1378–1382. [Google Scholar] [CrossRef] [PubMed]
- Booth, N.A.; Simpson, A.J.; Croll, A.; Bennett, B.; MacGregor, I.R. Plasminogen Activator Inhibitor (PAI-1) in Plasma and Platelets. Br. J. Haematol. 1988, 70, 327–333. [Google Scholar] [CrossRef]
- Forood, A.; Malekpour-Afshar, R.; Mahdavi, A. Serum Level of Plasminogen Activator Inhibitor Type-1 in Addicted Patients with Coronary Artery Disease. Addict. Health 2014, 6, 119–126. [Google Scholar]
- Morrow, G.B.; Whyte, C.S.; Mutch, N.J. A Serpin with a Finger in Many PAIs: PAI-1’s Central Function in Thromboinflammation and Cardiovascular Disease. Front. Cardiovasc. Med. 2021, 8, 653655. [Google Scholar] [CrossRef]
- Berberoğlu, M.; Evliyaoğlu, O.; Adiyaman, P.; Ocal, G.; Ulukol, B.; Simşek, F.; Siklar, Z.; Törel, A.; Ozel, D.; Akar, N. Plasminogen Activator Inhibitor-1 (PAI-1) Gene Polymorphism (-675 4G/5G) Associated with Obesity and Vascular Risk in Children. J. Pediatr. Endocrinol. Metab. 2006, 19, 741–748. [Google Scholar] [CrossRef] [PubMed]
- Juhan-Vague, I.; Morange, P.E.; Frere, C.; Aillaud, M.F.; Alessi, M.C.; Hawe, E.; Boquist, S.; Tornvall, P.; Yudkin, J.S.; Tremoli, E.; et al. The Plasminogen Activator Inhibitor-1 -675 4G/5G Genotype Influences the Risk of Myocardial Infarction Associated with Elevated Plasma Proinsulin and Insulin Concentrations in Men from Europe: The HIFMECH Study. J. Thromb. Haemost. 2003, 1, 2322–2329. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| SSc, n = 56 | CSs, n = 114 | p-Value | ||
|---|---|---|---|---|
| Demographic Data | ||||
| Age (years) a | 50 (38–57) | 47 (35–56) | 0.242 | |
| Male b Female b | 7 (12) 49 (88) | 10 (9) 104 (91) | 0.413 | |
| Type of SSc and Clinical Record | ||||
| lcSSc b | 48 (86) | - | ||
| dcSSc b | 8 (14) | - | ||
| Age of disease onset (years) c | 41 ± 16 | - | ||
| Disease evolution (years) a | 7.9 (0.71–20.9) | - | ||
| Signs and symptoms (n (%)) | ||||
| Active Raynaud’s phenomenon b | 41 (73) | - | ||
| Calcinosis b | 4 (7) | |||
| Esophageal dysfunction b | 9 (16) | |||
| Sclerodactyly b | 52 (93) | - | ||
| Telangiectasia b | 33 (59) | - | ||
| Digital ulcers b | 24 (43) | - | ||
| Puffy fingers b | 39 (70) | - | ||
| PAH b | 5 (9) | |||
| PID b | 4 (7) | |||
| Arthritis b | 49 (88) | - | ||
| Clinical evaluation | ||||
| Mouth opening (cm) a | 5.4 (3.08–7.00) | - | ||
| MRSS score a | 6.4 (0.00–27.7) | - | ||
| HAQ-DI, 0–3 score a | 0.40 (0.0–1.3) | - | ||
| VAS score a | 29.8 (0.0–78.5) | |||
| ANAs b | 43 (77) | 0 (0) | ||
| ACAs b | 14 (25) | 0 (0) | ||
| Anti-Scl70 b | 4 (7) | 0 (0) | ||
| Anti-RNA pol III b | 1 (2) | 0 (0) | ||
| Anti-fibrillarin b | 7 (13) | 0 (0) | ||
| TGF-β1 a | 7307 (3905–9448) | 24,386 (14,683–24,386) | p < 0.0001 | |
| TGF-β2 a | 275.2 (243.7–304.6) | 386.3 (359.1–437.3) | p < 0.0001 | |
| TGF-β3 a | 27.25 (18.42–34.27) | 49.86 (42.44–55.37) | p < 0.0001 | |
| Treatment (n (%)) | ||||
| NSAIDs b | 8 (14) | - | ||
| Prednisone b | 20 (36) | - | ||
| Methotrexate b | 28 (50) | - | ||
| Chloroquine b | 7 (13) | - | ||
| No treatment b | 21 (38) | - | ||
| Variant | Allele/Genotype | SSc, n = 56: n (%) | CSs, n = 114: n (%) | OR (CI 95%); p |
|---|---|---|---|---|
| -675 4G/5G | ||||
| Alleles | 4G 5G | 22 (20) 90 (80) | 55 (24) 173 (76) | 1.0 1.3 (0.7–2.2); 0.3 |
| Assessed association model | ||||
| Codominant | 4G/4G 4G/5G 5G/5G | 2 (4) 18 (32) 36 (64) | 7 (6) 41 (36) 66 (58) | 1.0 1.5 (0.2–8.1); 0.6 0.8 (0.4–1.6); 0.5 |
| Dominant | 4G/4G 4G/5G + 5G/5G | 2 (4) 54 (96) | 7 (6) 107 (94) | 1.0 1.9 (0.3–9.6); 0.4 |
| Recessive | 4G/4G + 4G/5G 5G/5G | 20 (36) 36 (64) | 48 (42) 66 (58) | 1.0 1.7 (0.3–8.7); 0.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lomelí-Nieto, J.A.; Muñoz-Valle, J.F.; Navarro-Zarza, J.E.; Baños-Hernández, C.J.; Gutierrez-Brito, J.A.; Renteria-Cabrera, V.; Horta-Chávez, E.A.; Morales-Núñez, J.J.; García-Arellano, S.; Parra-Rojas, I.; et al. Impact of Plasminogen Activator Inhibitor-1 Serum Levels and the -675 4G/5G Variant in the SERPINE1 Gene on Systemic Sclerosis in a Mexican Population. Life 2024, 14, 1056. https://doi.org/10.3390/life14091056
Lomelí-Nieto JA, Muñoz-Valle JF, Navarro-Zarza JE, Baños-Hernández CJ, Gutierrez-Brito JA, Renteria-Cabrera V, Horta-Chávez EA, Morales-Núñez JJ, García-Arellano S, Parra-Rojas I, et al. Impact of Plasminogen Activator Inhibitor-1 Serum Levels and the -675 4G/5G Variant in the SERPINE1 Gene on Systemic Sclerosis in a Mexican Population. Life. 2024; 14(9):1056. https://doi.org/10.3390/life14091056
Chicago/Turabian StyleLomelí-Nieto, José Alvaro, José Francisco Muñoz-Valle, José Eduardo Navarro-Zarza, Christian Johana Baños-Hernández, Jesús Alberto Gutierrez-Brito, Valeria Renteria-Cabrera, Eduardo Arturo Horta-Chávez, José Javier Morales-Núñez, Samuel García-Arellano, Isela Parra-Rojas, and et al. 2024. "Impact of Plasminogen Activator Inhibitor-1 Serum Levels and the -675 4G/5G Variant in the SERPINE1 Gene on Systemic Sclerosis in a Mexican Population" Life 14, no. 9: 1056. https://doi.org/10.3390/life14091056
APA StyleLomelí-Nieto, J. A., Muñoz-Valle, J. F., Navarro-Zarza, J. E., Baños-Hernández, C. J., Gutierrez-Brito, J. A., Renteria-Cabrera, V., Horta-Chávez, E. A., Morales-Núñez, J. J., García-Arellano, S., Parra-Rojas, I., & Hernández-Bello, J. (2024). Impact of Plasminogen Activator Inhibitor-1 Serum Levels and the -675 4G/5G Variant in the SERPINE1 Gene on Systemic Sclerosis in a Mexican Population. Life, 14(9), 1056. https://doi.org/10.3390/life14091056