TTF-1/p63-Positive Poorly Differentiated NSCLC: A Histogenetic Hypothesis from the Basal Reserve Cell of the Terminal Respiratory Unit

 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Clinical Data
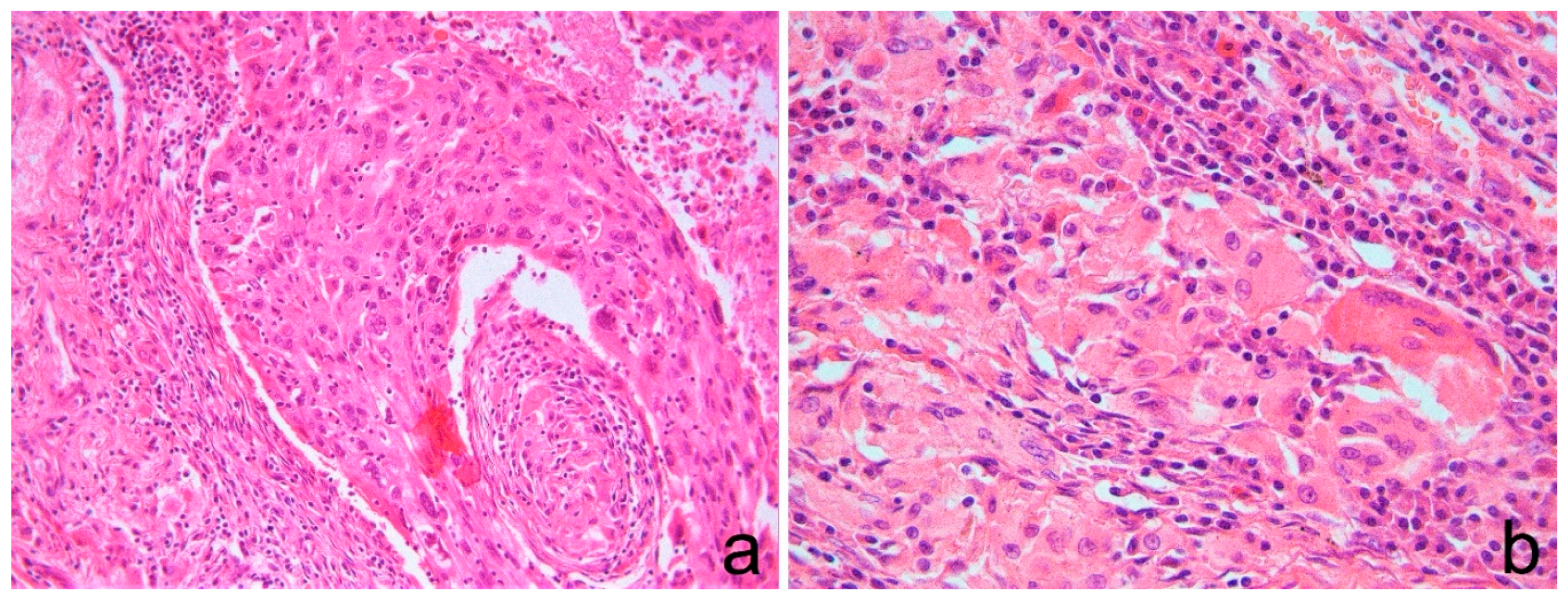
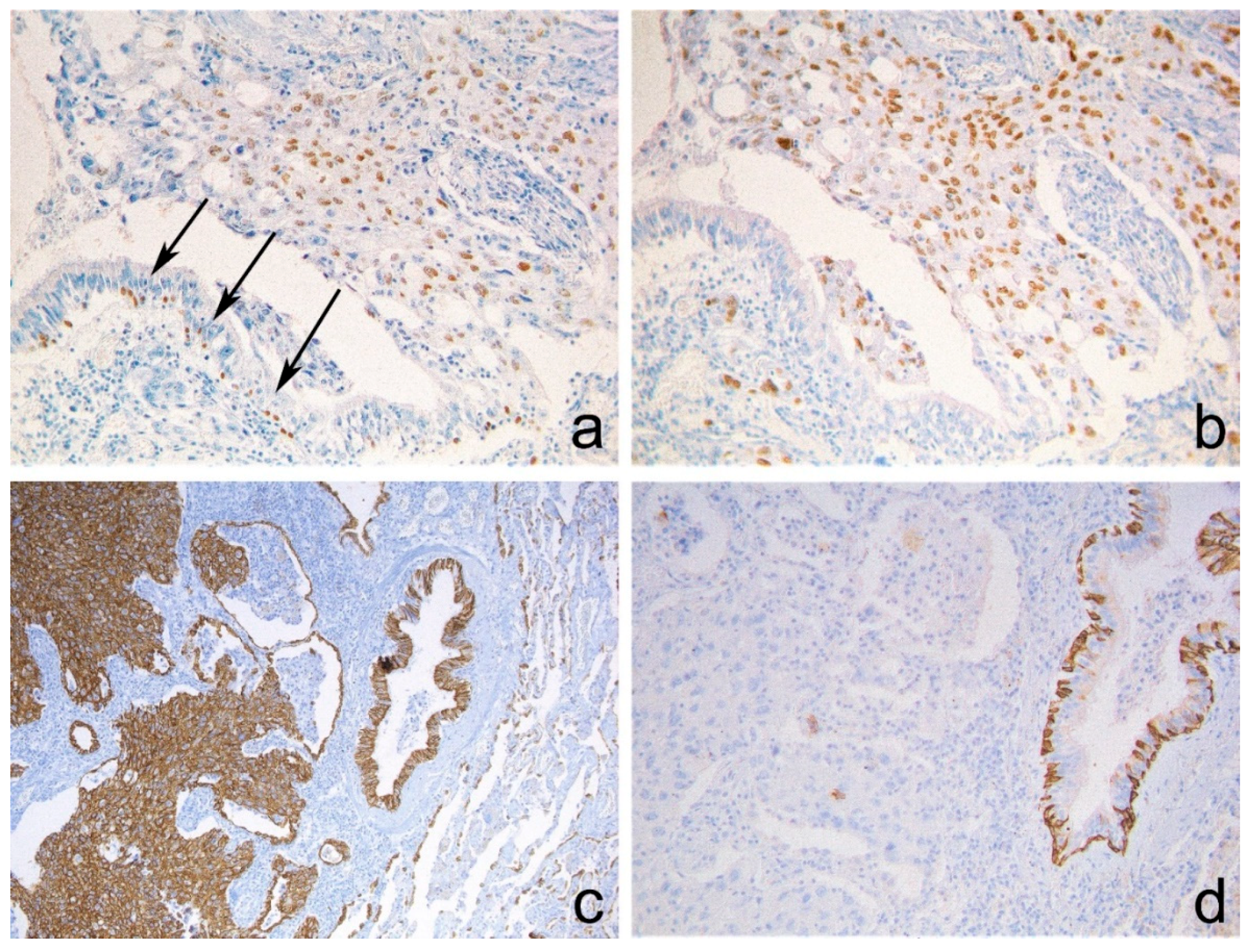
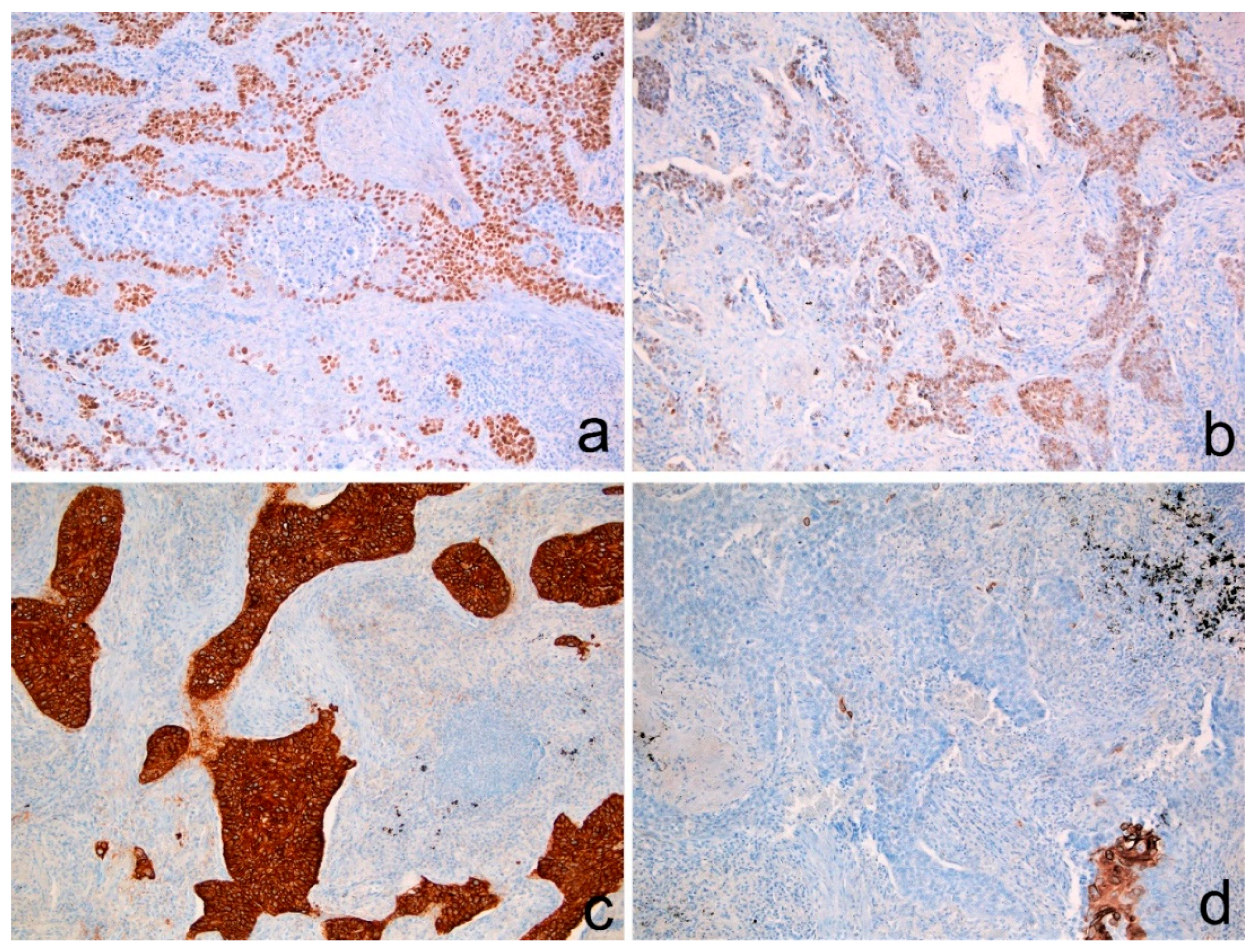
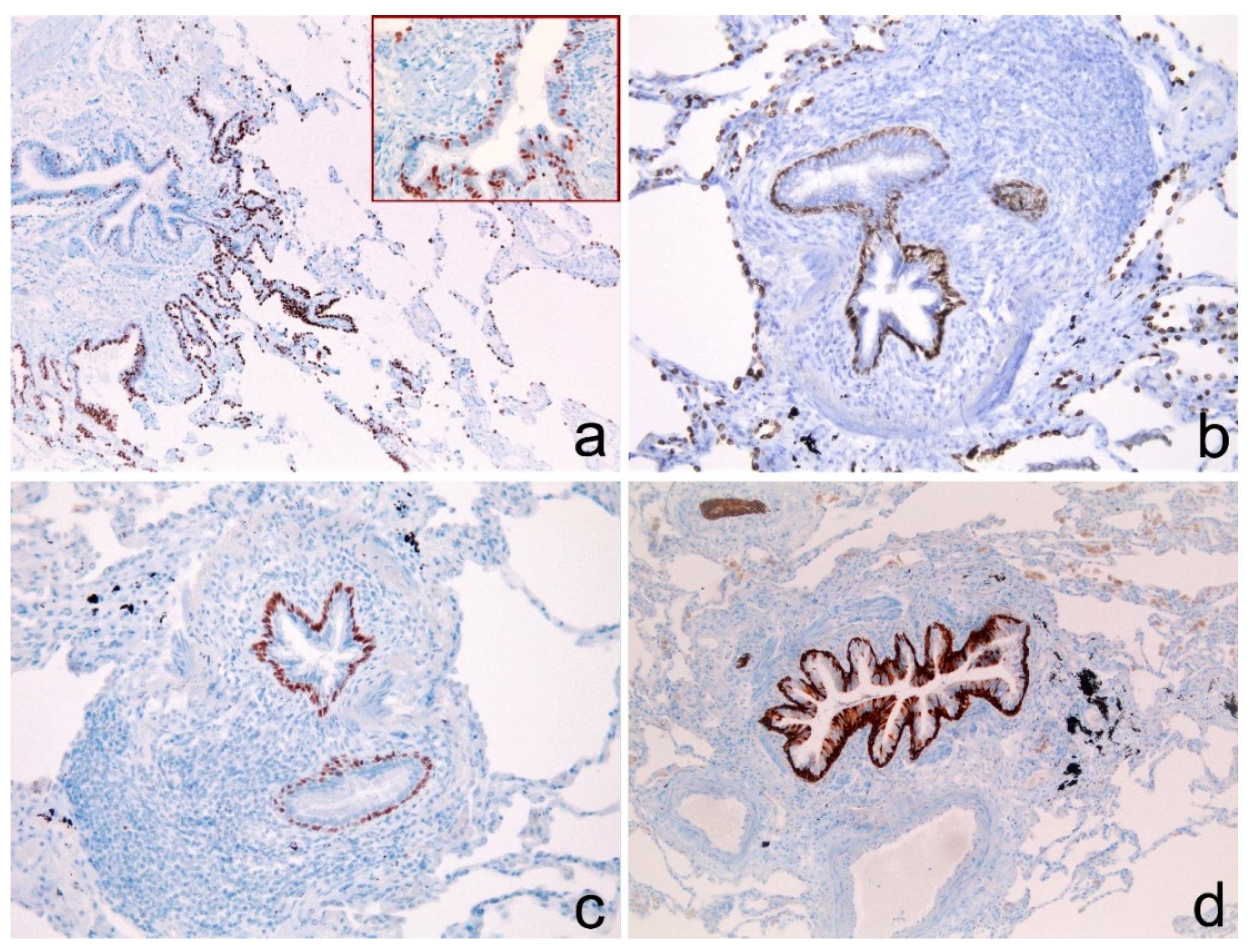
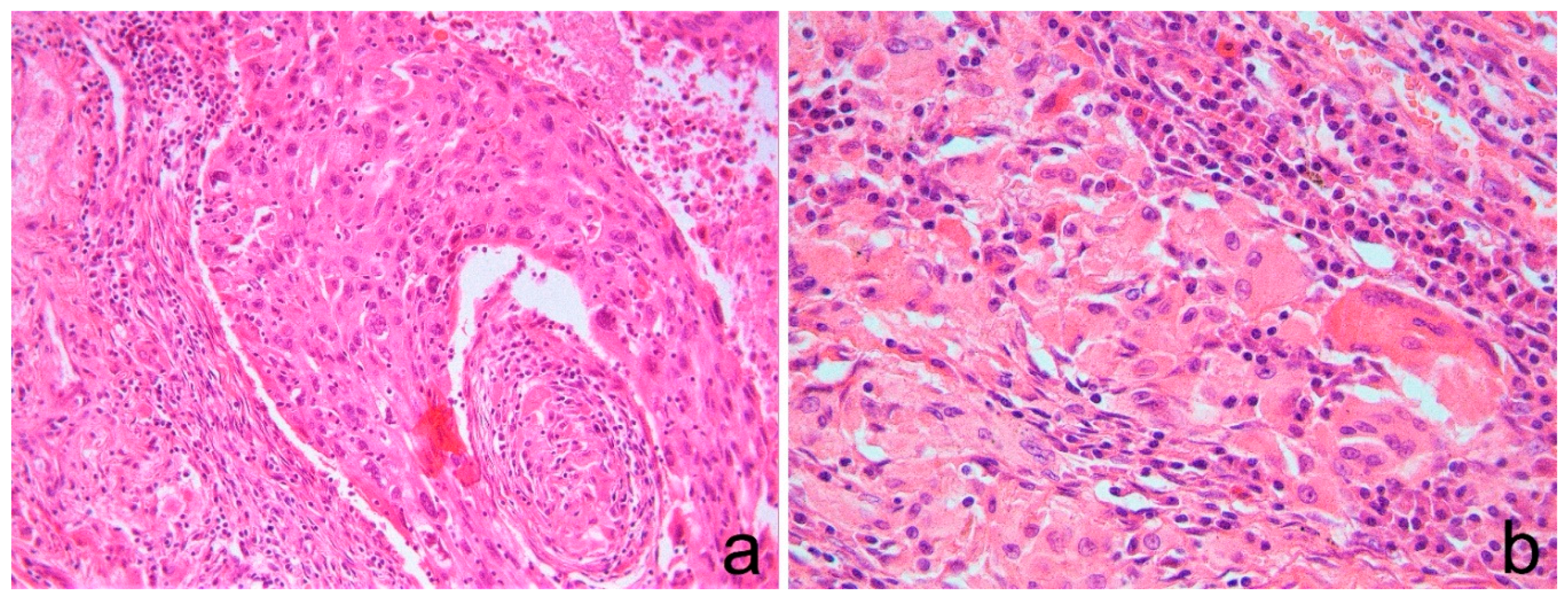
3.2. Histological Data
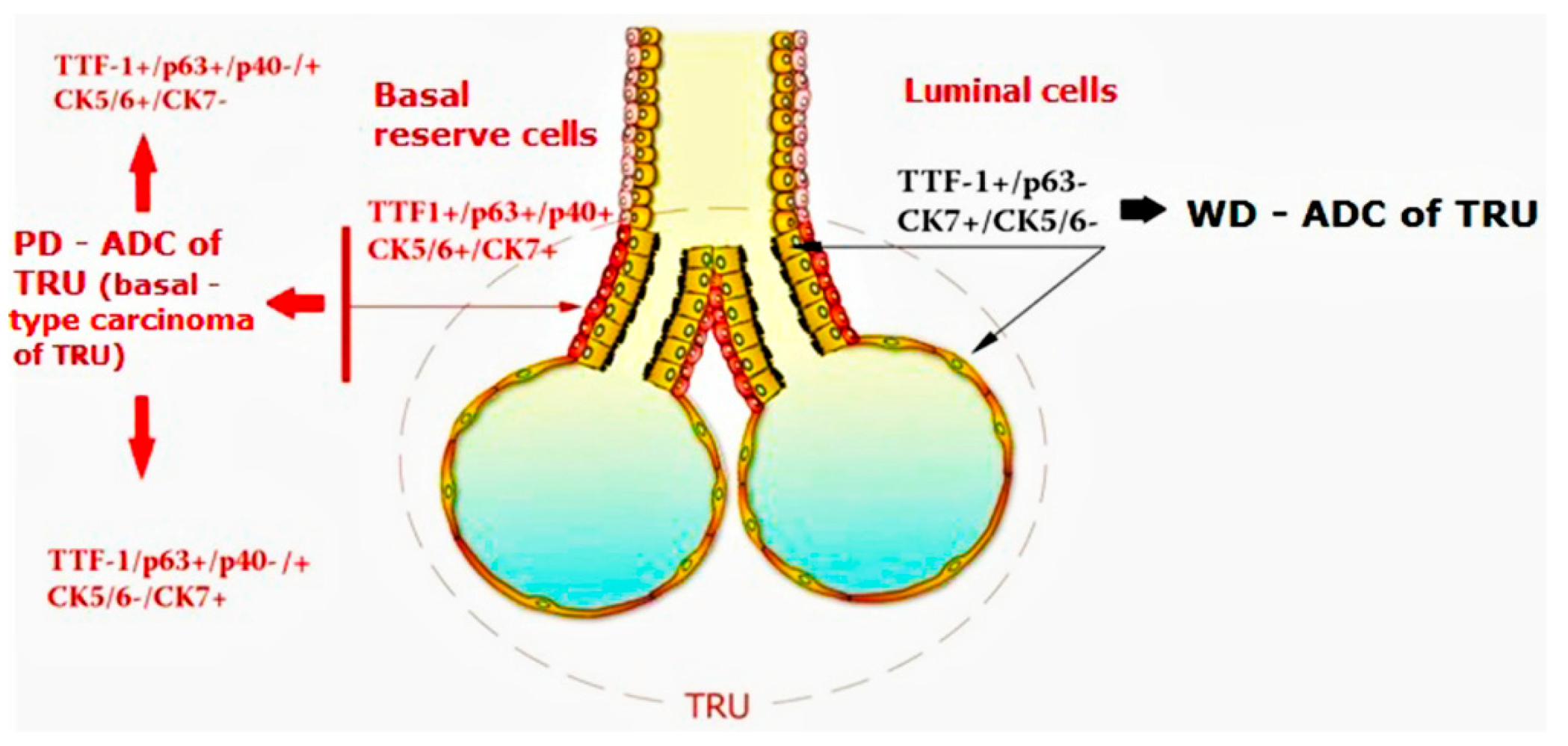
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rossi, G.; Pelosi, G.; Graziano, P.; Barbareschi, M.; Papotti, M.; Rossi, A. A reevaluation of the clinical significance of histological subtyping of non–small-cell lung carcinoma: Diagnostic algorithms in the era of personalized treatments. Int. J. Surg. Pathol. 2009, 17, 206–218. [Google Scholar] [CrossRef]
- Sterlacci, W.; Savic, S.; Schmid, T.; Oberaigner, W.; Auberger, J.; Fiegl, M.; Tzankov, A. Tissue-Sparing Application of the Newly Proposed IASLC/ATS/ERS Classification of Adenocarcinoma of the Lung Shows Practical Diagnostic and Prognostic Impact. Am. J. Clin. Pathol. 2012, 137, 946–956. [Google Scholar] [CrossRef] [Green Version]
- Pelosi, G.; Rossi, G.; Cavazza, A.; Righi, L.; Maisonneuve, P.; Barbareschi, M.; Graziano, P.; Pastorino, U.; Garassino, M.; de Braud, F.; et al. ΔNp63 (p40) distribution inside lung cancer: A driver biomarker approach to tumor characterization. Int. J. Surg. Pathol. 2013, 21, 229–239. [Google Scholar] [CrossRef]
- Dubinski, W.; Leighl, N.B.; Tsao, M.-S.; Hwang, D.M. Ancillary Testing in Lung Cancer Diagnosis. Pulm. Med. 2012, 2012, 249082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ocque, R.; Tochigi, N.; Ohori, N.P.; Dacic, S. Usefulness of Immunohistochemical and Histochemical Studies in the Classification of Lung Adenocarcinoma and Squamous Cell Carcinoma in Cytologic Specimens. Am. J. Clin. Pathol. 2011, 136, 81–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rekhtman, N.; Ang, D.C.; Sima, C.S.; Travis, W.D.; Moreira, A.L. Immunohistochemical algorithm for differentiation of lung adenocarcinoma and squamous cell carcinoma based on large series of whole-tissue sections with validation in small specimens. Mod. Pathol. 2011, 24, 1348–1359. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, A.G.; Gonzalez, D.; Shah, P.; Pynegar, M.J.; Deshmukh, M.; Rice, A.; Popat, S. Refining the diagnosis and EGFR status of non–small cell lung carcinoma in biopsy and cytologic material, using a panel of mucin staining, TTF-1, cytokeratin 5/6, and P63, and EGFR mutation analysis. J. Thorac. Oncol. 2010, 5, 436–441. [Google Scholar] [CrossRef] [Green Version]
- Loo, P.S.; Thomas, S.C.; Nicolson, M.C.; Fyfe, M.N.; Kerr, K.M. Subtyping of undifferentiated non–small cell carcinomas in bronchial biopsy specimens. J. Thorac. Oncol. 2010, 5, 442–447. [Google Scholar] [CrossRef] [Green Version]
- Walia, R.; Jain, D.; Madan, K.; Sharma, M.C.; Mathur, S.R.; Mohan, A.; Iyer, V.K.; Kumar, L. p40 e thyroid transcription factor-1 immunohistochemistry: A useful panel to characterize non-small cell lung carcinoma-not otherwise specified (NSCLC-NOS) category. Indian J. Med. Res. 2017, 146, 42–48. [Google Scholar]
- Warth, A.; Muley, T.; Herpel, E.; Meister, M.; Herth, F.J.F.; Schirmacher, P.; Weichert, W.; Hoffmann, H.; Schnabel, P.A. Large-scale comparative analyses of immunomarkers for diagnostic subtyping of non-small-cell lung cancer biopsies. Histopathology 2012, 61, 1017–1025. [Google Scholar] [CrossRef]
- Sheikh, H.A.; Fuhrer, K.; Cieply, K.; Yousem, S. P63 expression in assessment of bronchioloalveolar proliferation of the lung. Mod. Pathol. 2004, 17, 1134–1140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, M.; Orta, L.; Gil, J.; Li, G.; Hu, A.; Burstein, D.E. Immunohistochemical detection of XIAP and p63 in adenomatous hyperplasia, atypical adenomatous hyperplasia, bronchioloalveolar carcinoma and well-differentiated adenocarcinoma. Mod. Pathol. 2008, 21, 553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, B.Y.; Gil, J.; Kaufman, D.; Gan, L.; Kohtz, D.S.; Burstein, D.E. p63 in pulmonary epithelium, pulmonary squamous neoplasms, and other pulmonary tumors. Hum. Pathol. 2002, 33, 921–926. [Google Scholar] [CrossRef] [PubMed]
- Ang, D.; Ghaffar, H.; Zakowski, M.; Teruya-Feldstein, J.; Moreira, A.; Rekhtman, N. Expression of squamous markers in lung adenocarcinoma: Clinicopathologic and molecular correlates, and implications for differentiation from squamous cell carcinoma. Mod. Pathol. 2010, 90, 397A. [Google Scholar]
- Pelosi, G.; Pasini, F.; Stenholm, C.O.; Pastorino, U.; Maisonneuve, P.; Sonzogni, A.M.; Maffini, F.; Pruneri, G.; Fraggetta, F.; Cavallon, A.; et al. p63 immunoreactivity in lung cancer: Yet another player in the development of squamous cell carcinomas? J. Pathol. 2002, 198, 100–109. [Google Scholar] [CrossRef]
- De Molengraft, F.; Niekerk, C.; Jap, P.; Poels, L. OV-TL 12/30 (keratin 7 antibody) is a marker of glandular differentiation in lung cancer. Histopathology 1993, 22, 35–38. [Google Scholar] [CrossRef]
- Nakamura, N.; Miyagi, E.; Murata, S.-I.; Kawaoi, A.; Katoh, R. Expression of thyroid transcription factor-1 in normal and neoplastic lung tissues. Mod. Pathol. 2002, 15, 1058–1067. [Google Scholar] [CrossRef]
- Yatabe, Y.; Mitsudomi, T. Epidermal growth factor receptor mutations in lung cancers. Pathol. Int. 2007, 57, 233–244. [Google Scholar] [CrossRef]
- Yatabe, Y.; Mitsudomi, T.; Takahashi, T. TTF-1 expression in pulmonary adenocarcinomas. Am. J. Surg. Pathol. 2002, 26, 767–773. [Google Scholar] [CrossRef]
- Maeshima, A.M.; Omatsu, M.; Tsuta, K.; Asamura, H.; Matsuno, Y. Immunohistochemical expression of TTF-1 in various cytological subtypes of primary lung adenocarcinoma, with special reference to intratumoral heterogeneity. Pathol. Int. 2008, 58, 31–37. [Google Scholar] [CrossRef]
- Pelosi, G.; Fabbri, A.; Tamborini, E.; Perrone, F.; Testi, A.M.; Settanni, G.; Busico, A.; Centonze, G.; Braidotti, P.; Bulfamante, G.; et al. Challenging Lung Carcinoma with Coexistent ΔNp63/p40 and Thyroid Transcription Factor-1 Labeling Within the Same Individual Tumor Cells. J. Thorac. Oncol. 2015, 10, 1500–1502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayashi, T.; Takamochi, K.; Yanai, Y.; Mitani, M.; Tomita, H.; Mogushi, K.; Suehara, Y.; Takahashi, F.; Suzuki, K.; Saito, T.; et al. Non small cell lung carcinoma with diffuse co-expression of thyroid transcription factor-1 and ΔNp63/p40. Hum. Pathol. 2018, 78, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, T.; Tomida, S.; Yatabe, Y.; Kosaka, T.; Osada, H.; Yanagisawa, K.; Mitsudomi, T.; Takahashi, T. Expression profile-defined classification of lung adenocarcinoma shows close relationship with underlying major genetic changes and clinicopathologic behaviors. J. Clin. Oncol. 2006, 24, 1679–1688. [Google Scholar] [CrossRef]
- Perou, C.M.; Sørlie, T.; Eisen, M.B.; Van De Rijn, M.; Jeffrey, S.S.; Rees, C.A.; Pollack, J.R.; Ross, U.T.; Johnsen, H.; Akslen, L.A.; et al. Molecular portraits of human breast tumours. Nature 2000, 406, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Sørlie, T.; Perou, C.M.; Tibshirani, R.; Aas, T.; Geisler, S.; Johnsen, H.; Hastie, T.; Eisen, M.B.; van de Rijn, M.; Jeffrey, S.S.; et al. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc. Natl. Acad. Sci. USA 2001, 98, 10869–10874. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, T.O.; Hsu, F.D.; Cheang, M.C.U.; Karaca, G.; Hu, Z.; Livasy, C.; Dressler, L.; Ragaz, J.; Gown, A.M.; Van De Rijn, M.; et al. Immunohistochemical and clinical characterization of the basal-like subtype of invasive breast carcinoma. Clin. Cancer Res. 2004, 10, 5367–5374. [Google Scholar] [CrossRef] [Green Version]
- Banerjee, S.; Reis-Filho, J.S.; Ashley, S.; Steele, D.; Ashworth, A.; Lakhani, S.R.; Smith, I.E. Basal-like breast carcinomas: Clinical outcome and response to chemotherapy. J. Clin. Pathol. 2006, 59, 729–735. [Google Scholar] [CrossRef]
- Rody, A.; Karn, T.; Liedtke, C.; Pusztai, L.; Ruckhaeberle, E.; Hanker, L.; Gaetje, R.; Solbach, C.; Ahr, A.; Metzler, D.; et al. A clinically relevant gene signature in triple negative and basal-like breast cancer. Breast Cancer Res. 2011, 13, R97. [Google Scholar] [CrossRef] [Green Version]



© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cabibi, D.; Bellavia, S.; Giannone, A.G.; Barraco, N.; Cipolla, C.; Martorana, A.; Rodolico, V.; Cajozzo, M.; Florena, A.M. TTF-1/p63-Positive Poorly Differentiated NSCLC: A Histogenetic Hypothesis from the Basal Reserve Cell of the Terminal Respiratory Unit. Diagnostics 2020, 10, 25. https://doi.org/10.3390/diagnostics10010025
Cabibi D, Bellavia S, Giannone AG, Barraco N, Cipolla C, Martorana A, Rodolico V, Cajozzo M, Florena AM. TTF-1/p63-Positive Poorly Differentiated NSCLC: A Histogenetic Hypothesis from the Basal Reserve Cell of the Terminal Respiratory Unit. Diagnostics. 2020; 10(1):25. https://doi.org/10.3390/diagnostics10010025
Chicago/Turabian StyleCabibi, Daniela, Sandro Bellavia, Antonino Giulio Giannone, Nadia Barraco, Calogero Cipolla, Anna Martorana, Vito Rodolico, Massimo Cajozzo, and Ada Maria Florena. 2020. "TTF-1/p63-Positive Poorly Differentiated NSCLC: A Histogenetic Hypothesis from the Basal Reserve Cell of the Terminal Respiratory Unit" Diagnostics 10, no. 1: 25. https://doi.org/10.3390/diagnostics10010025
APA StyleCabibi, D., Bellavia, S., Giannone, A. G., Barraco, N., Cipolla, C., Martorana, A., Rodolico, V., Cajozzo, M., & Florena, A. M. (2020). TTF-1/p63-Positive Poorly Differentiated NSCLC: A Histogenetic Hypothesis from the Basal Reserve Cell of the Terminal Respiratory Unit. Diagnostics, 10(1), 25. https://doi.org/10.3390/diagnostics10010025