The Effects of Thermal Water Physical Exercise in Patients with Lower Limb Chronic Venous Insufficiency Monitored by Bioimpedance Analysis

 ,
,  ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Population
- -
- Age from 18 to 80 years old;
- -
- BMI < 35;
- -
- CVD with visible varicose veins and edema.
- -
- Cardiac comorbidity (e.g., congestive heart failure, cardiomyopathy, coronary artery disease);
- -
- lower limb arterial disease;
- -
- severe biochemical alterations (e.g., diabetes mellitus, hypothyroidism);
- -
- chronic kidney disease;
- -
- fear of water;
- -
- venous active drugs and/or graduated compression use;
- -
- use of drugs potentially leading to edema.
2.2. Exercise Program
- -
- Warming up by a cycling-like activity, in a supine position while holding the handrail;
- -
- tip–toe exercise (four series of ten repetitions each);
- -
- hip flexion–extension on the non-weight bearing limb (four series of ten repetitions each);
- -
- tip–toe exercise on a step (four series of ten repetitions each);
- -
- knee flexion–extension (four series of ten repetitions each);
- -
- forward and backward walking for 5 min;
- -
- lateral walking on both sides for 5 min;
- -
- cycling-like single push while standing up on the contralateral limb (four series of ten repetitions each);
- -
- ankle flexion–extension while keeping the knee bent at 90° (four series of 10 repetitions each);
- -
- cool-down by a cycling-like activity, in a supine position while holding the handrail.
2.3. Bioimpedance Analysis (BIA)
- -
- ECW % calculated according to the following formula: (extracellular water/extracellular + intracellular water) × 100 [29].
- -
- R as the expression of extracellular fluids amount. This latter is inversely proportional to the extracellular fluids components [13].
- -
- Xc depends on the interaction between cell membranes and BIA current, and it is directly proportional to cell density [13].
- -
- PA is obtained through the relationship between direct measures of resistance (R) and reactance (Xc). In young healthy subjects, the value ranged from 6° and 7°. In general, values < 5° indicate a rupture of cell membranes or an accumulation of extracellular fluids, and values around 10° indicate severe dehydration [14,15].
2.4. Lower Limb Volumetry
- -
- The water level was above the pretibial region;
- -
- the water temperature ranged from 28 °C to 32 °C;
- -
- the subjects were measured in sitting and resting position
- -
- the volume assessment was performed right before and right after the 5 exercise sessions
- -
- the time of the measurements was between 9 and 12 a.m.
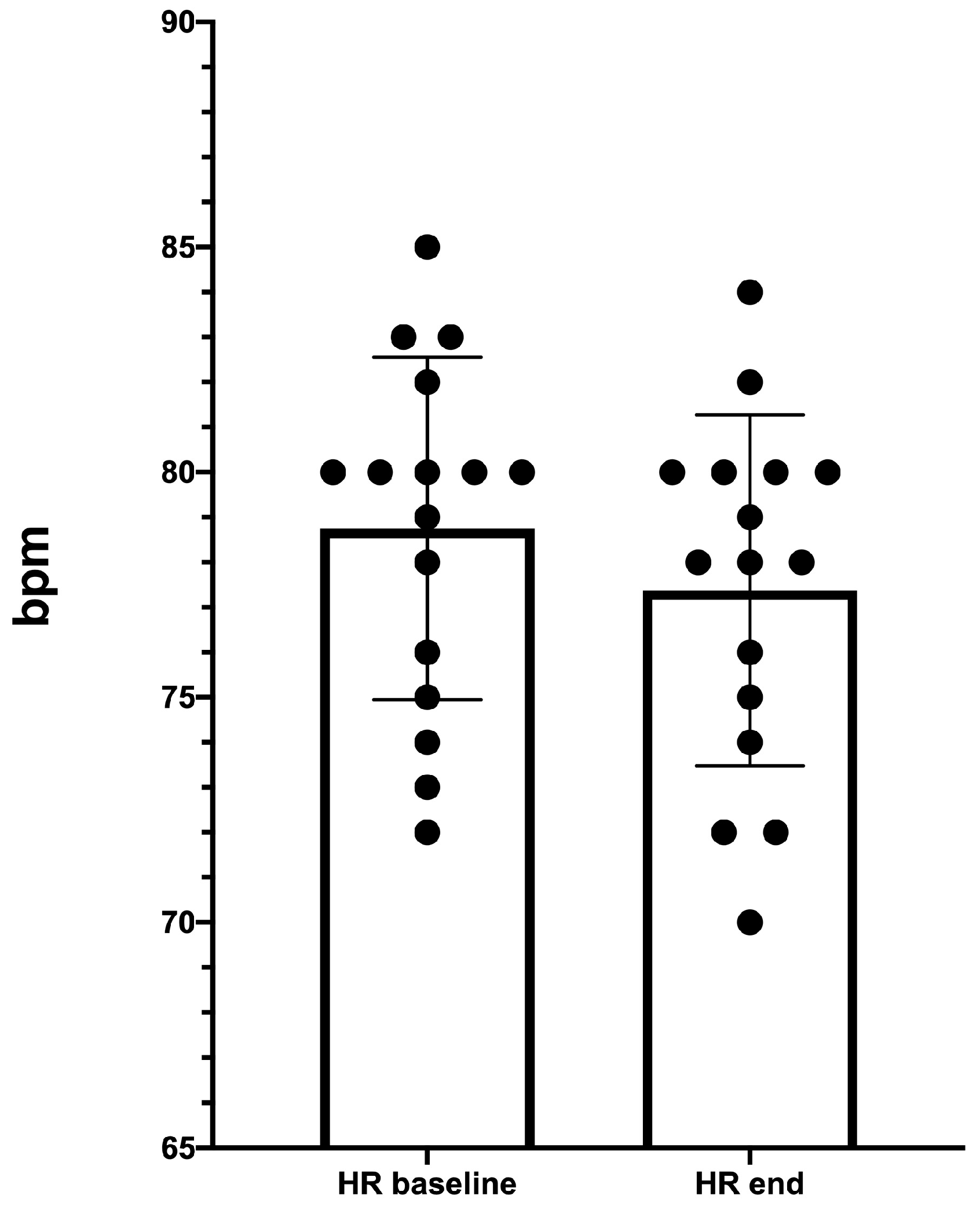
2.5. Heart Rate at Rest
2.6. Statistical Analysis
3. Results
3.1. BIA
3.2. Lower Limb Volume

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Session | Leg Volume Pre-Exercise (mL) | Leg Volume Post-Exercise (mL) | Variation (%) | p |
|---|---|---|---|---|
| S1 | 2288 ± 348 | 2079 ± 385 | −9.1% | 0.0001 |
| S2 | 2244 ± 310 | 2032 ± 338 | −9.4% | 0.0001 |
| S3 | 2237 ± 327 | 2024 ± 356 | −9.5% | 0.0001 |
| S4 | 2216 ± 335 | 2012 ± 367 | −9.2% | 0.0001 |
| S5 | 2172 ± 310 | 1928 ± 321 | −11.2% | 0.0001 |
3.3. Resting-HR Measurement
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lurie, F.; Passman, M.; Meisner, M.; Dalsing, M.; Masuda, E.; Welch, H.; Bush, R.L.; Blebea, J.; Carpentier, P.H.; De Maeseneer, M.; et al. The 2020 update of the CEAP classification system and reporting standards. J. Vasc. Surg. Venous Lymphat. Disord. 2020, 8, 342–352. [Google Scholar] [CrossRef] [PubMed]
- Leu, A.J.; Leu, H.J.; Franzeck, U.K.; Bollinger, A. Microvascular changes in chronic venous insufficiency-a review. Cardiovasc Surg. 1995, 3, 237–245. [Google Scholar] [CrossRef]
- Bunke, N.; Brown, K.; Bergan, J. Phlebolymphedema: Usually unrecognized, often poorly treated. Perspect Vasc. Surg. Endovasc. Ther. 2009, 21, 65–68. [Google Scholar] [CrossRef] [PubMed]
- Khalil, S.F.; Mohktar, M.S.; Ibrahim, F. The theory and fundamentals of bioimpedance analysis in clinical status monitoring and diagnosis of diseases. Sensors (Basel) 2014, 14, 10895–10928. [Google Scholar] [CrossRef] [PubMed]
- Martinsen, O.G.; Grimnes, S. Bioimpedance and Bioelectricity Basics; Academic Press: Waltham, MA, USA, 2011. [Google Scholar]
- Mulasi, U.; Kuchnia, A.J.; Cole, A.J.; Earthman, C.P. Bioimpedance at the bedside: Current applications, limitations, and opportunities [published correction appears in Nutr Clin Pract. 2015, 30:589]. Nutr. Clin. Pract. 2015, 30, 180–193. [Google Scholar] [CrossRef] [Green Version]
- Sergi, G.; Bussolotto, M.; Perini, P.; Calliari, I.; Giantin, V.; Ceccon, A.; Scanferla, F.; Bressan, M.; Moschini, G.; Enzi, G. Accuracy of bioelectrical impedance analysis in estimation of extracellular space in healthy subjects and in fluid retention states. Ann. Nutr. Metab. 1994, 38, 158–165. [Google Scholar] [CrossRef]
- Sargent, J.A.; Gotch, F.A. Principles and biophysics of dialysis. In Replacement of Renal Function by Dialysis; Springer: Dordrecht, The Netherlands, 1989; pp. 87–143. [Google Scholar]
- Maffrin, M.Y.; Morel, H. Body fluid volumes measurements by impedance: A review of bioimpedance spectroscopy (BIS) and bioimpedance analysis (BIA) methods. Med. Eng. Phys. 2008, 30, 1257–1269. [Google Scholar] [CrossRef]
- Earthman, C.; Traughber, D.; Dobratz, J.; Howell, W. Bioimpedance spectroscopy for clinical assessment of fluid distribution and body cell mass. Nutr. Clin. Pract. 2007, 22, 389–405. [Google Scholar] [CrossRef]
- Matthie, J.R.; Withers, P.O. Bioimpedance: 50 kHz parallel reactance and the prediction of body cell mass. Am. J. Clin. Nutr. 1998, 68, 403–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaw, R.; Box, R.; Cornish, B. Bioimpedance in the assessment of unilateral lymphedema of a limb: The optimal frequency. Lymphat. Res. Biol. 2011, 9, 93–99. [Google Scholar] [CrossRef] [Green Version]
- Cavezzi, A.; Urso, S.U.; Paccasassi, S.; Mosti, G.; Campana, F.; Colucci, R. Bioimpedance spectroscopy and volumetry in the immediate/short-term monitoring of intensive complex decongestive treatment of lymphedema. Phlebology 2020, 35, 715–723. [Google Scholar] [CrossRef]
- Mattiello, R.; Amaral, M.A.; Mundstock, E.; Ziegelmann, P.K. Reference values for the phase angle of the electrical bioimpedance: Systematic review and meta-analysis involving more than 250,000 subjects. Clin. Nutr. 2020, 39, 1411–1417. [Google Scholar] [CrossRef]
- Kumar, S.; Dutt, A.; Hemraj, S.; Bhat, S.; Manipadybhima, B. Phase Angle Measurement in Healthy Human Subjects through Bio-Impedance Analysis. Iran J. Basic Med. Sci. 2012, 15, 1180–1184. [Google Scholar] [PubMed]
- Ward, L.C.; Bunce, I.H.; Cornish, B.H.; Mirolo, B.R.; Thomas, B.J.; Jones, L.C. Multi-frequency bioelectrical impedance augments the diagnosis and management of lymphoedema in post-mastectomy patients. Eur. J. Clin. Investig. 1992, 22, 751–754. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.H.; Seo, K.S. Correlation among bioimpedance analysis, sonographic and circumferential measurement in assessment of breast cancer-related arm lymphedema. Lymphology 2014, 47, 123–133. [Google Scholar] [PubMed]
- Coroneos, C.J.; Wong, F.C.; DeSnyder, S.M.; Shaitelman, S.F.; Schaverien, M.V. Correlation of L-Dex Bioimpedance Spectroscopy with Limb Volume and Lymphatic Function in Lymphedema. Lymphat. Res. Biol. 2019, 17, 301–307. [Google Scholar] [CrossRef]
- Bundred, N.J.; Stockton, C.; Keeley, V.; Riches, K.; Ashcroft, L.; Evans, A.; Skene, A.; Purushotham, A.; Bramley, M.; Hodgkiss, T. Investigators of BEA/PLACE studies. Comparison of multi-frequency bioimpedance with perometry for the early detection and intervention of lymphoedema after axillary node clearance for breast cancer. Breast Cancer Res Treat. 2015, 151, 121–129. [Google Scholar] [CrossRef]
- Cornish, B.H.; Chapman, M.; Hirst, C.; Mirolo, B.; Bunce, I.H.; Ward, L.C.; Thomas, B.J. Early diagnosis of lymphedema using multiple frequency bioimpedance. Lymphology 2001, 34, 2–11. [Google Scholar]
- Cho, K.H.; Han, E.Y.; Lee, S.A.; Park, H.; Lee, C.; Im, S.H. Feasibility of Bioimpedance Analysis to Assess the Outcome of Complex Decongestive Therapy in Cancer Treatment-Related Lymphedema. Front Oncol. 2020, 10, 111. [Google Scholar] [CrossRef]
- Dionne, A.; Goulet, S.; Leone, M.; Comtois, A.S. Aquatic Exercise Training Outcomes on Functional Capacity, Quality of Life, and Lower Limb Lymphedema: Pilot Study. J. Altern. Complement. Med. 2018, 24, 1007–1009. [Google Scholar] [CrossRef]
- Ergin, G.; Karadibak, D.; Sener, H.O.; Gurpinar, B. Effects of Aqua-Lymphatic Therapy on Lower Extremity Lymphedema: A Randomized Controlled Study. Lymphat. Res. Biol. 2017, 15, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Yeung, W.; Semciw, A.I. Aquatic Therapy for People with Lymphedema: A Systematic Review and Meta-analysis. Lymphat. Res. Biol. 2018, 16, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Iyer, N.S.; Cartmel, B.; Friedman, L.; Li, F.; Zhou, Y.; Ercolano, E.; Harrigan, M.; Gottlieb, L.; McCorkle, R.; Schwartz, P.E.; et al. Lymphedema in ovarian cancer survivors: Assessing diagnostic methods and the effects of physical activity. Cancer 2018, 124, 1929–1937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukushima, T.; Tsuji, T.; Sano, Y.; Miyata, C.; Kamisako, M.; Hohri, H.; Yoshimura, C.; Asakura, M.; Okitsu, T.; Muraoka, K.; et al. Immediate effects of active exercise with compression therapy on lower-limb lymphedema. Support Care Cancer 2017, 25, 2603–2610. [Google Scholar] [CrossRef] [Green Version]
- Gianesini, S.; Tessari, M.; Bacciglieri, P.; Malagoni, A.M.; Menegatti, E.; Occhionorelli, S.; Basaglia, N.; Zamboni, P. A specifically designed aquatic exercise protocol to reduce chronic lower limb edema. Phlebology 2017, 32, 594–600. [Google Scholar] [CrossRef]
- Musumeci, A.; Pranovi, G.; Masiero, S. Patient education and rehabilitation after hip arthroplasty in an Italian spa center: A pilot study on its feasibility. Int. J. Biometeorol. 2018, 62, 1489–1496. [Google Scholar] [CrossRef]
- Gianesini, S.; Raffetto, J.D.; Mosti, G.; Maietti, E.; Sibilla, M.G.; Zamboni, P.; Menegatti, E. Volume control of the lower limb with graduated compression during different muscle pump activation conditions and the relation to limb circumference variation. J. Vasc. Surg. Venous Lymphat. Disord. 2020, 8, 814–820. [Google Scholar] [CrossRef]
- Rabe, E.; Stucker, M.; Ottillinger, B. Water displacement leg volumetry in clinical studies–A discussion of error sources. BMC Med. Res. Methodol. 2010, 10, 5. [Google Scholar] [CrossRef]
- Perrin, M.; Guex, J.J. Edema and leg volume: Methods of assessment. Angiology 2000, 51, 9–12. [Google Scholar]
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation Coefficients: Appropriate Use and Interpretation. Anesth Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef]
- Caggiati, A.; Lattimer, C.; Kalodiki, E.; Oberto, S.; Bergamo, G.; Kontothanassis, D. Underwater Sonography of Leg Veins. EJVES Short Rep. 2018, 41, 13–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masiero, S.; Vittadini, F.; Ferroni, C.; Bosco, A.; Serra, R.; Frigo, A.C.; Frizziero, A. The role of thermal balneotherapy in the treatment of obese patient with knee osteoarthritis. Int. J. Biometeorol. 2018, 62, 243–252. [Google Scholar] [CrossRef]
- Cozzi, F.; Carrara, M.; Sfriso, P.; Todesco, S.; Cima, L. Anti-inflammatory effect of mud-bath applications on adjuvant arthritis in rats. Clin. Exp. Rheumatol. 2004, 22, 763–766. [Google Scholar] [PubMed]
- Bellometti, S.; Galzigna, L. Serum levels of a prostaglandin and a leukotriene after thermal mud pack therapy. J. Investig. Med. 1998, 46, 140–145. [Google Scholar]
- Bellometti, S.; Galzigna, L.; Richelmi, P.; Gregotti, C.; Bertè, F. Both serum receptors of tumor necrosis factor are influenced by mud pack treatment in osteoarthrotic patients. Int. J. Tissue React. 2002, 24, 57–64. [Google Scholar]
- Bacolla, A.; Giraudi, G.; Lorenzini, P.; Varacca, G.; Costa, A. Observations in iodine exchange in thermal therapy with salsobromoiodic water. Panminerva Med. 1983, 25, 241–247. [Google Scholar] [PubMed]
- Ippolito, E.; De Luca, S.; Sommaruga, S.; Grassellino, V.; Nappi, G. Experimental-clinical study on the effects of hydromassage with Thermae Oasis’s salsobromoiodine water in chronic venous stasis disease of the lower extremities. Minerva Cardioangiol. 2008, 56, 401–408. [Google Scholar]
- Kimura, G. Pathogenesis of edema and its classification. Nihon Rinsho. Jpn. J. Clin. Med. 2005, 63, 11–16. [Google Scholar]
- Cavezzi, A.; Mosti, G.; Colucci, R.; Quinzi, V.; Bastiani, L.; Urso, S.U. Compression with 23 mmHg or 35 mmHg stockings after saphenous catheter foam sclerotherapy and phlebectomy of varicose veins: A randomized controlled study. Phlebology 2019, 34, 98–106. [Google Scholar] [CrossRef]
- Genton, L.; Norman, K.; Spoerri, A.; Pichard, C.; Karsegard, V.L.; Herrmann, F.R.; Graf, C.E. Bioimpedance-Derived Phase Angle and Mortality Among Older People. Rejuvenation Res. 2017, 20, 118–124. [Google Scholar] [CrossRef]
- Aukland, K. Distribution of body fluids: Local mechanisms guarding interstitial fluid volume. J. Physiol. (Paris) 1984, 79, 395–400. [Google Scholar]
- Lurie, F. Physiology and Pathophysiology of the Venous System. PanVascular Med. 2014. [Google Scholar] [CrossRef]
- Raju, S.; Varney, E.; Flowers, W.; Cruse, G. Effect of External Positive and Negative Pressure on Venous Flow in an Experimental Model. Eur. J. Vasc. Endovasc. Surg. 2016, 51, 275–284. [Google Scholar] [CrossRef] [Green Version]
- Sarin, S.; Scurr, J.H.; Coleridge Smith, P.D. Mechanism of action of external compression on venous function. Br. J. Surg. 1992, 79, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Tisato, V.; Zauli, G.; Voltan, R.; Gianesini, S.; di Iasio, M.G.; Volpi, I.; Fiorentini, G.; Zamboni, P.; Secchiero, P. Endothelial cells obtained from patients affected by chronic venous disease exhibit a pro-inflammatory phenotype. PLoS ONE 2012, 7, e39543. [Google Scholar] [CrossRef] [Green Version]
- Tisato, V.; Zauli, G.; Gianesini, S.; Menegatti, E.; Brunelli, L.; Manfredini, R.; Zamboni, P.; Secchiero, P. Modulation of circulating cytokine-chemokine profile in patients affected by chronic venous insufficiency undergoing surgical hemodynamic correction. J. Immunol. Res. 2014, 2014, 473765. [Google Scholar] [CrossRef] [PubMed]
- Tessari, M.; Tisato, V.; Rimondi, E.; Zamboni, P.; Malagoni, A.M. Effects of intermittent pneumatic compression treatment on clinical outcomes and biochemical markers in patients at low mobility with lower limb edema. J. Vasc. Surg. Venous Lymphat. Disord. 2018, 6, 500–510. [Google Scholar] [CrossRef]
- Becker, B.E. Aquatic therapy: Scientific foundations and clinical rehabilitation applications. PM R 2009, 1, 859–872. [Google Scholar] [CrossRef]
- Michalsen, A.; Lüdtke, R.; Bühring, M.; Spahn, G.; Langhorst, J.; Dobos, G.J. Thermal hydrotherapy improves quality of life and hemodynamic function in patients with chronic heart failure. Am. Heart J. 2003, 146, 728–733. [Google Scholar] [CrossRef]




| Properties | Value |
|---|---|
| Temperature before arriving at the surface | 80/90 °C |
| pH | 7.1 |
| Conductivity | 7042 μS/cm |
| Fixed residue at 180° | 5050 mg/L |
| Sodium (Na+) | 1239 mg/L |
| Potassium (K+) | 88 mg/L |
| Calcium (Ca2+) | 3667 mg/L |
| Magnesium (Mg2+) | 80 mg/L |
| Silica (SiO2) | 51 mg/L |
| Ammonium (NH4+) | 2.7 mg/L |
| Total iron | <0.05 mg/L |
| Sulfate (SO42−) | 980 mg/L |
| Chlorides (Cl−) | 2176 mg/L |
| Bicarbonate (HCO3−) | 169 mg/L |
| Bromide (Br−) | 13.6 mg/L |
| Iodide (I−) | 0.82 mg/L |
| Hydrogen Sulfide (H2S) | 1.67 mg/L |
| Baseline (T0) | 7 Days (T7) | 14 Day (T14) | p Value (T0-T7) | p Value (T7-T14) | p Value (T0-T14) | |
|---|---|---|---|---|---|---|
| % ECW | 42.1 ± 5.8 | 41.8 ± 5.5 | 41.2 ± 5.5 | 0.001 | 0.03 | 0.001 |
| R (Ohm) | 455.4 ± 78.2 | 471. 0 ± 81.1 | 488.1 ± 83.6 | 0.001 | 0.05 | 0.0009 |
| Xc (Ohm) | 53.1 ± 11.9 | 54.2 ± 11.7 | 57.6 ± 14.7 | 0.2602 | 0.04 | 0.009 |
| PA ° | 6.6 ±0.7 | 6.5 ± 0.8 | 6.6 ± 0.9 | 0.3761 | 0.2305 | 0.5610 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Menegatti, E.; Pagani, A.; Avruscio, G.; Mucignat, M.; Gianesini, S. The Effects of Thermal Water Physical Exercise in Patients with Lower Limb Chronic Venous Insufficiency Monitored by Bioimpedance Analysis. Diagnostics 2020, 10, 889. https://doi.org/10.3390/diagnostics10110889
Menegatti E, Pagani A, Avruscio G, Mucignat M, Gianesini S. The Effects of Thermal Water Physical Exercise in Patients with Lower Limb Chronic Venous Insufficiency Monitored by Bioimpedance Analysis. Diagnostics. 2020; 10(11):889. https://doi.org/10.3390/diagnostics10110889
Chicago/Turabian StyleMenegatti, Erica, Anselmo Pagani, Giampiero Avruscio, Marianna Mucignat, and Sergio Gianesini. 2020. "The Effects of Thermal Water Physical Exercise in Patients with Lower Limb Chronic Venous Insufficiency Monitored by Bioimpedance Analysis" Diagnostics 10, no. 11: 889. https://doi.org/10.3390/diagnostics10110889