AK-DL: A Shallow Neural Network Model for Diagnosing Actinic Keratosis with Better Performance than Deep Neural Networks

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Acquisition
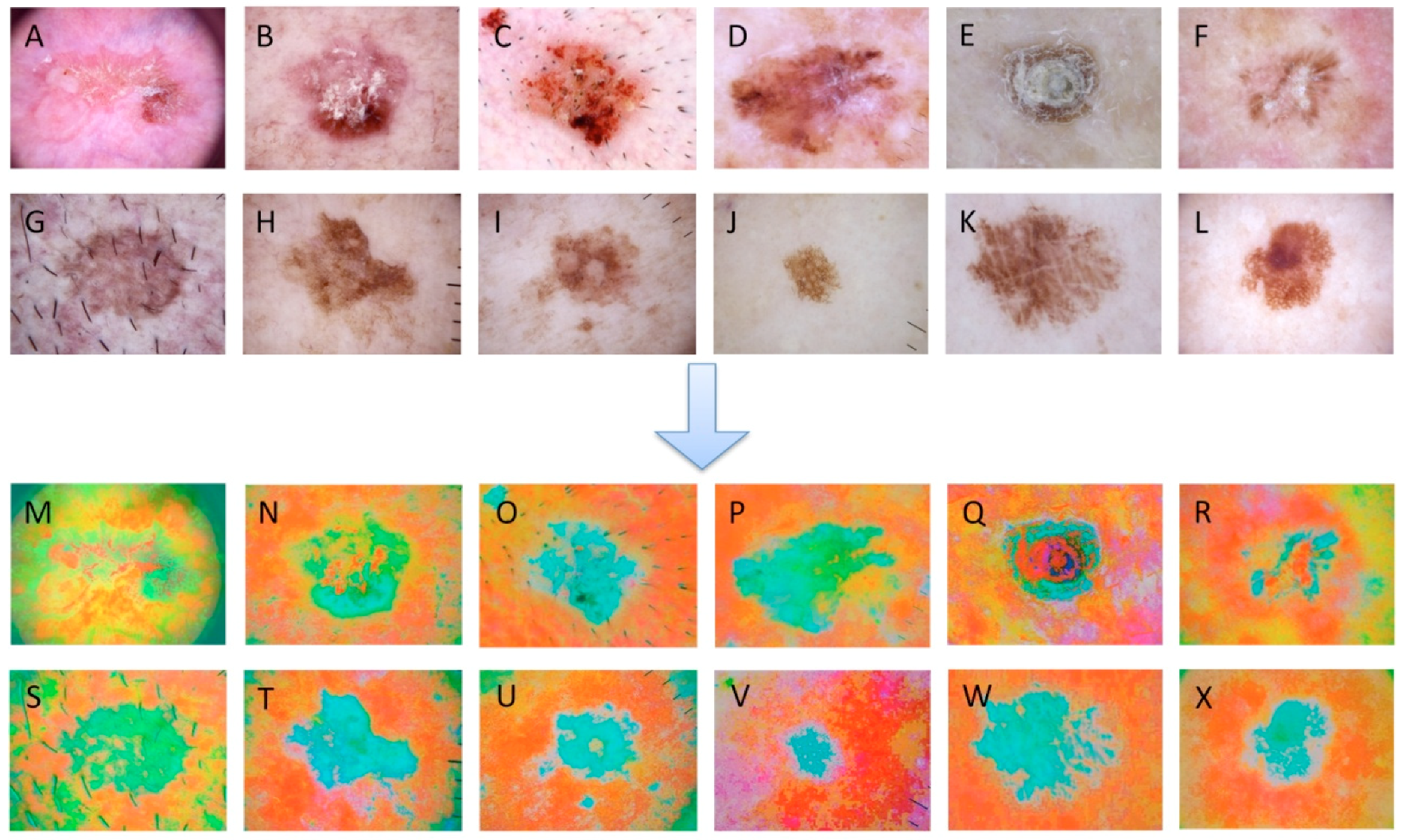
2.2. Data Preprocessing
2.3. Models Building
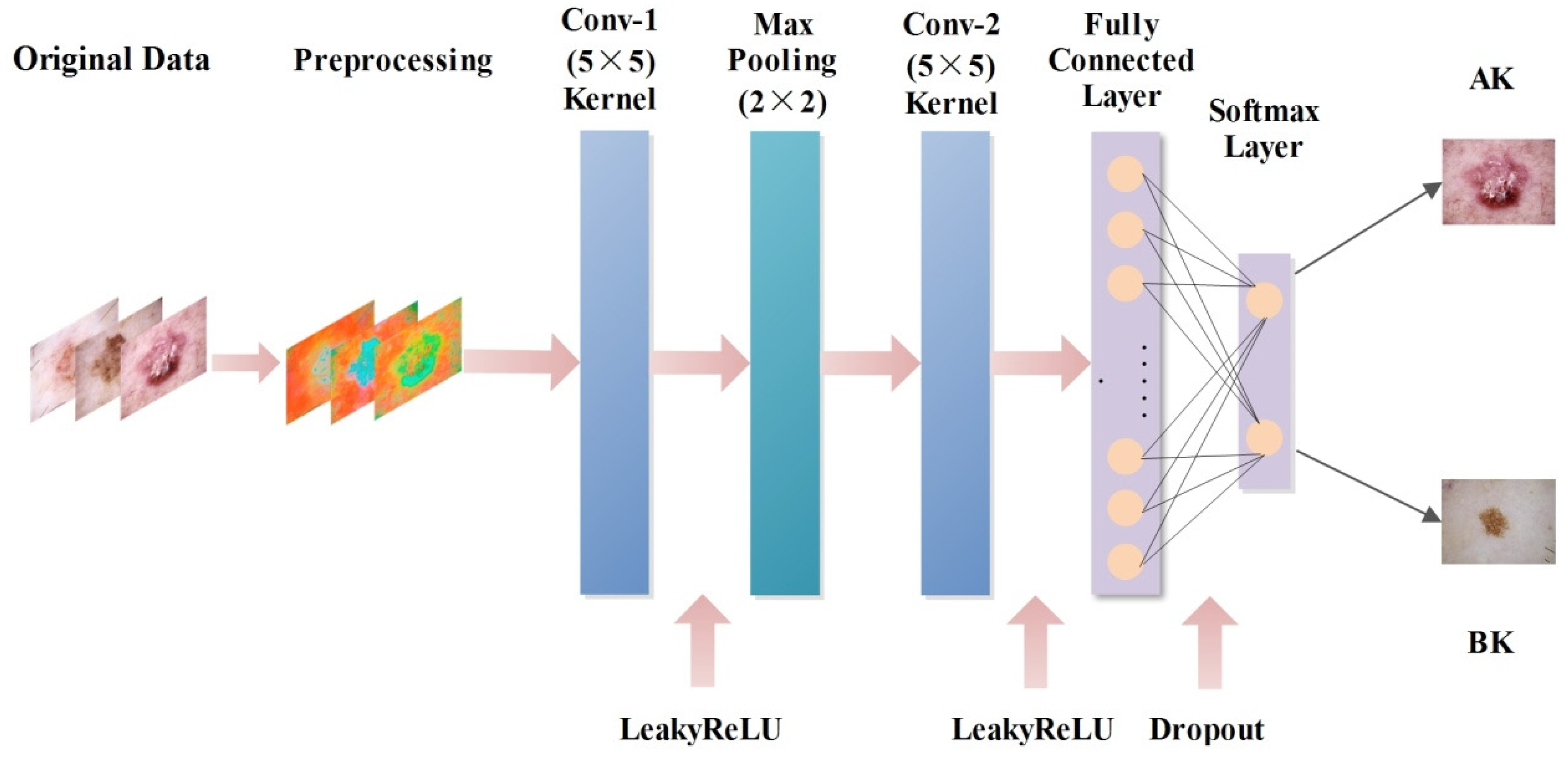
2.3.1. AK-DL Model
2.3.2. AlexNet Transfer Learning
2.3.3. GoogLeNet Transfer Learning
2.3.4. ResNet Transfer Learning
2.4. Traditional Machine Learning
2.5. Parameter Optimization
2.6. Evaluation Indexes
3. Results
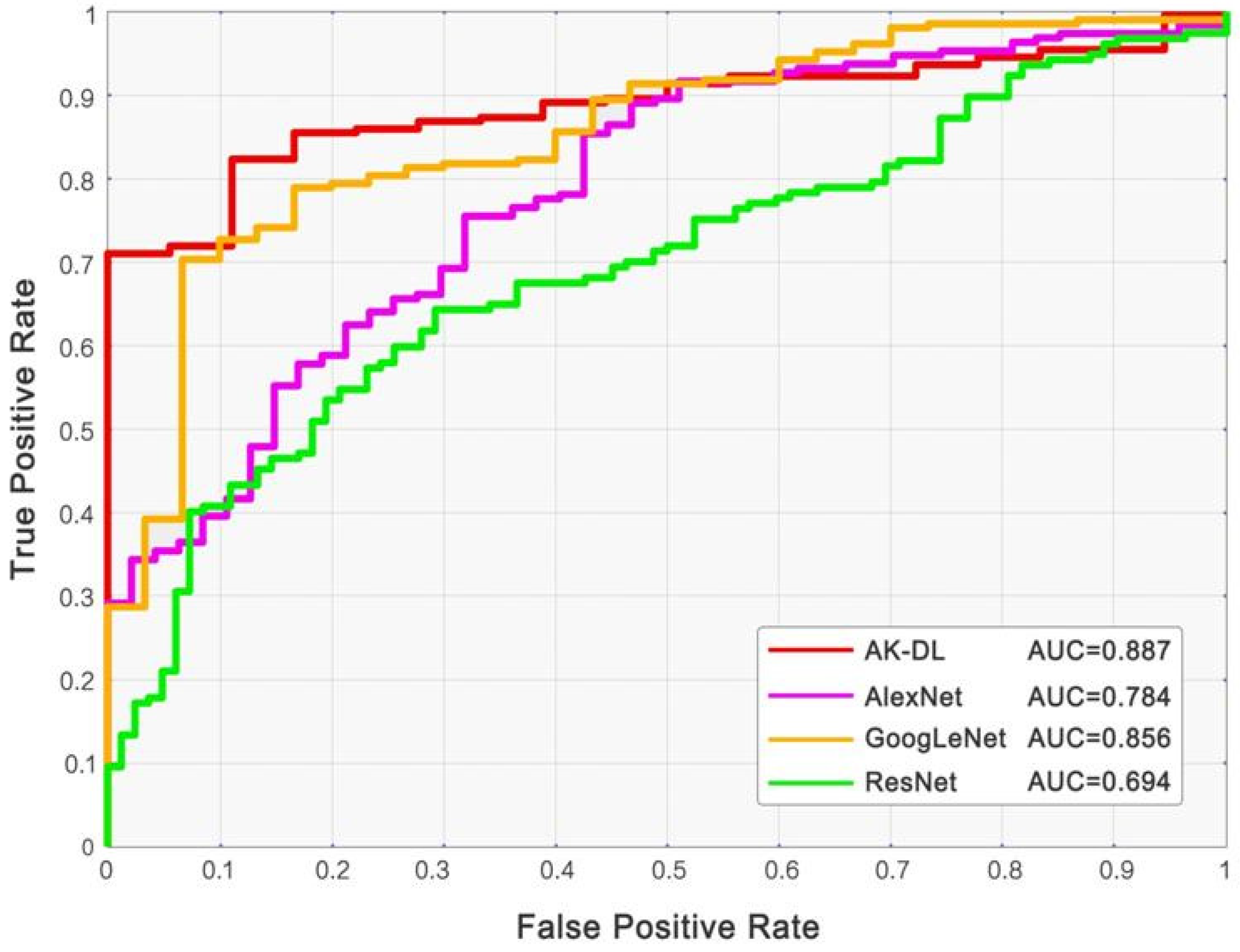
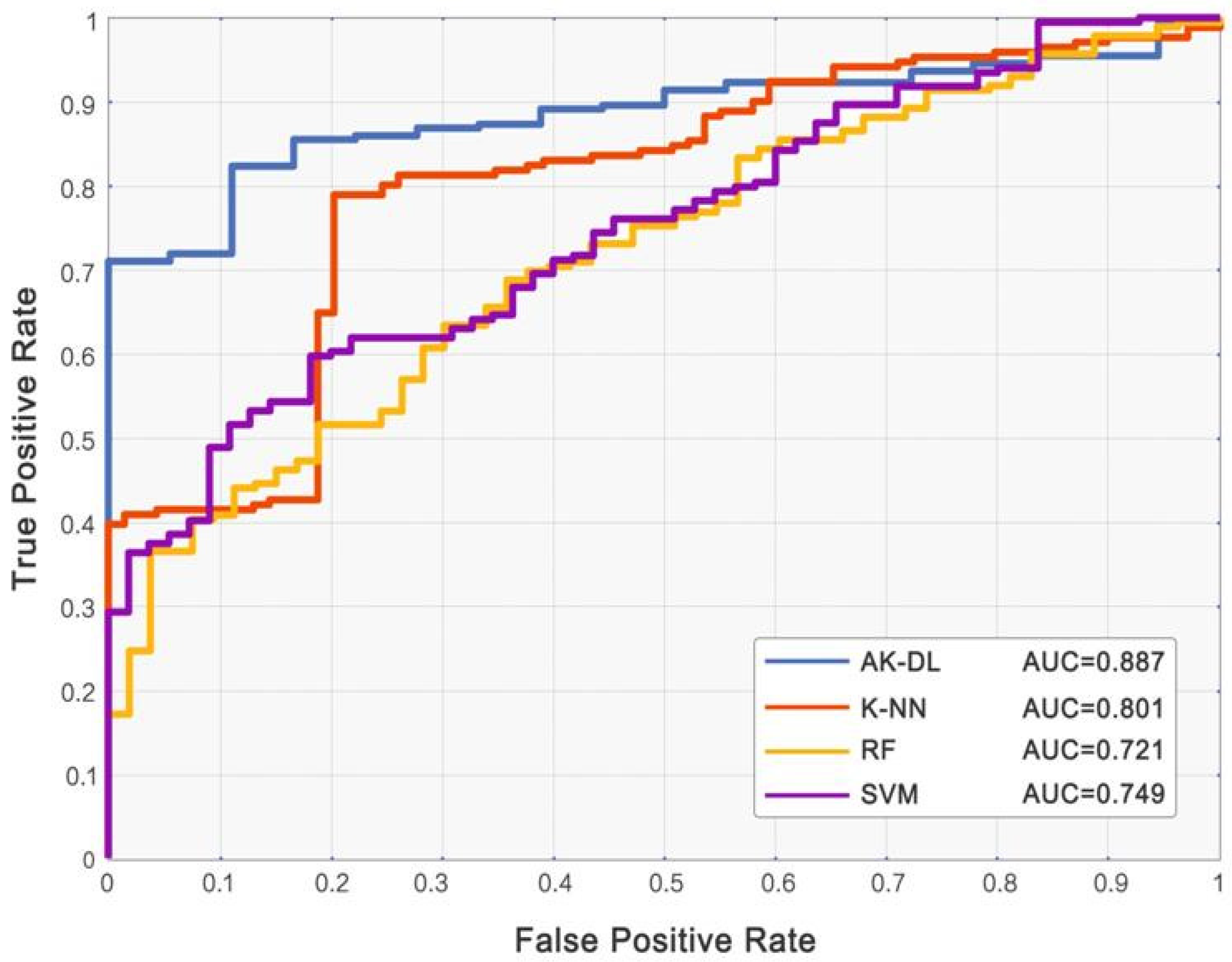
3.1. Comparison of AK-DL with Machine Learning Models
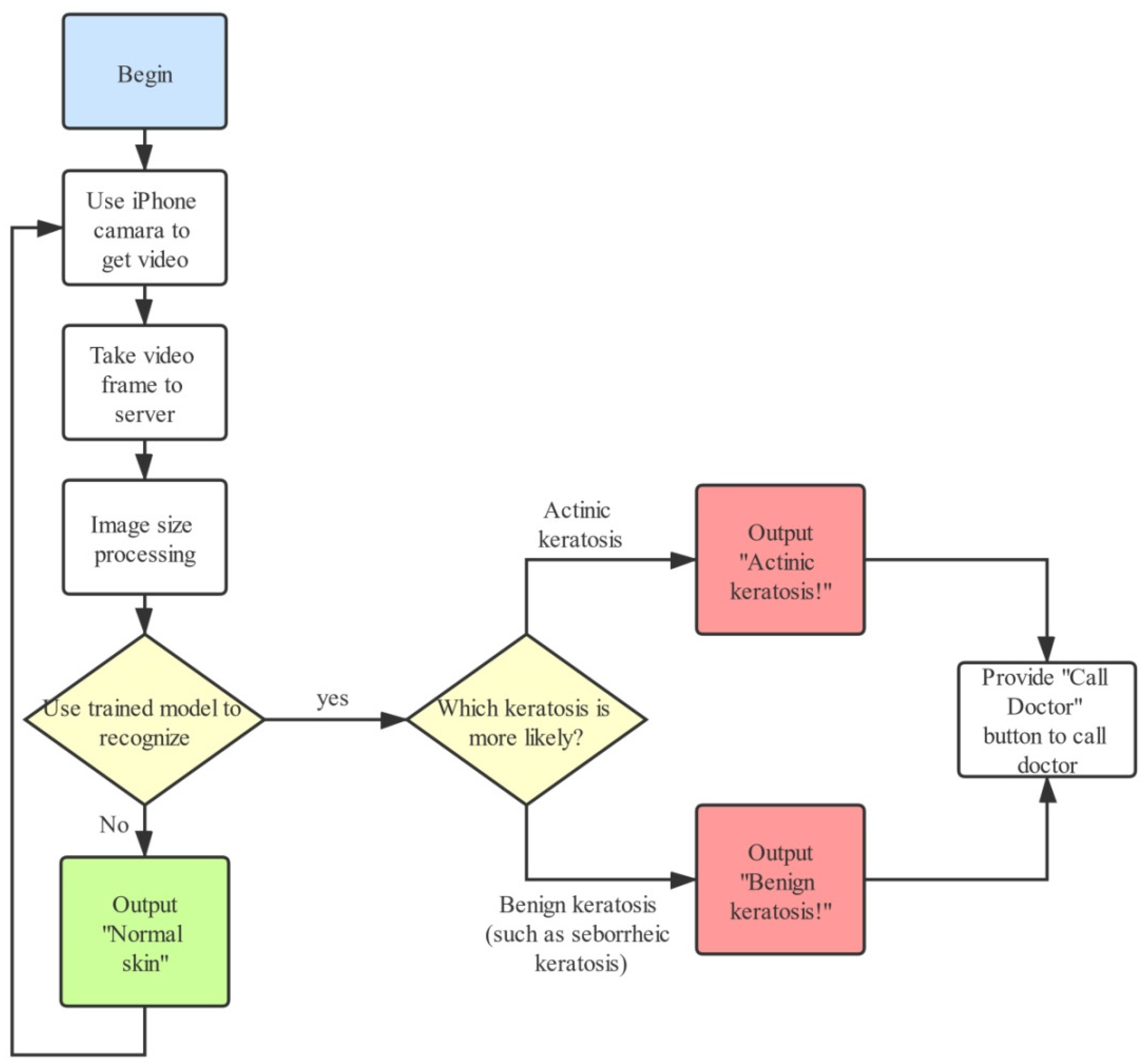
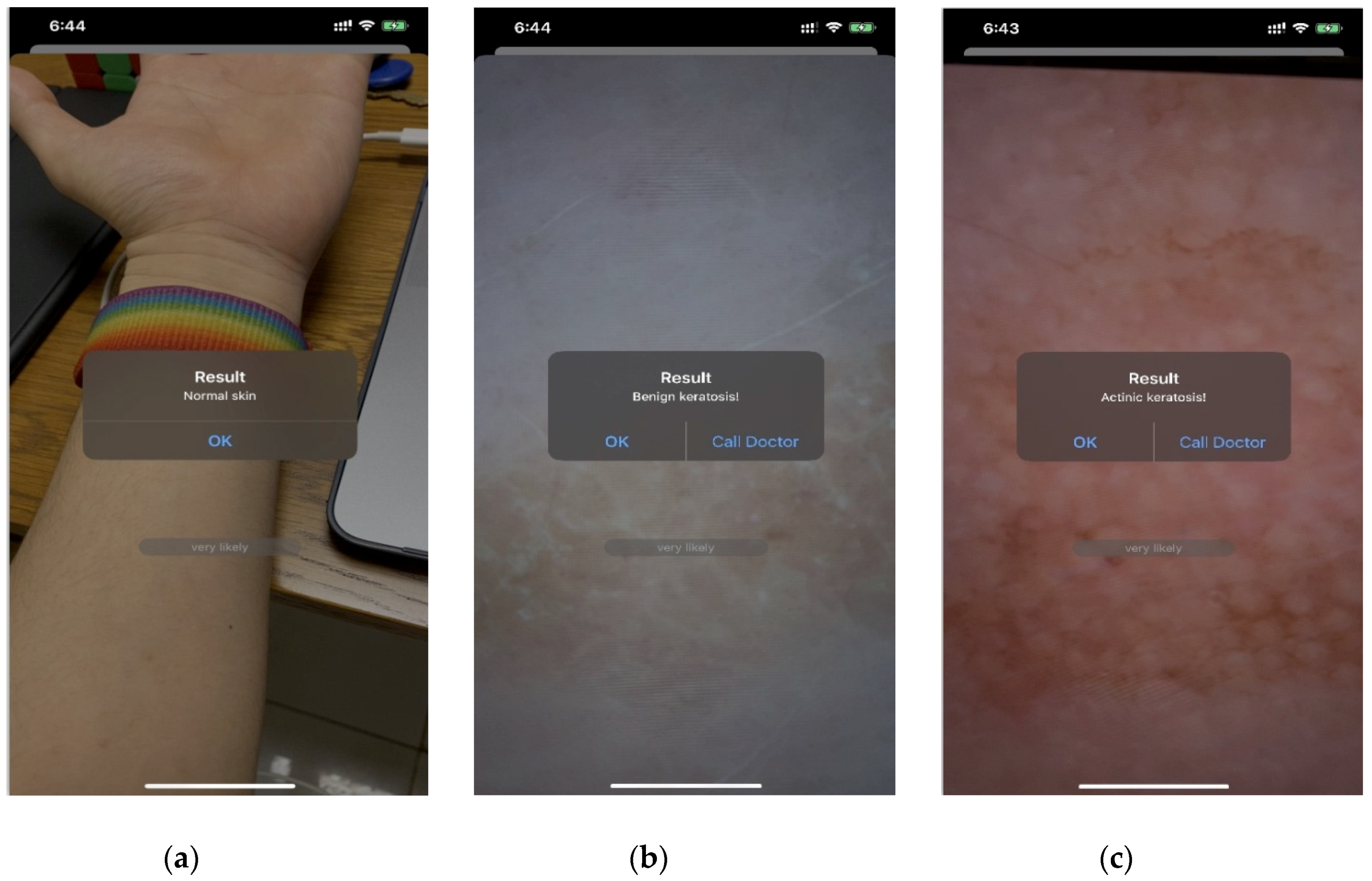
3.2. Intelligent Diagnostic System
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Lebwohl, M. Actinic keratosis: Epidemiology and progression to squamous cell carcinoma. Br. J. Dermatol. 2003, 149, 31–33. [Google Scholar] [CrossRef] [PubMed]
- Cantisani, C.; Paolino, G.; Melis, M.; Faina, V.; Romaniello, F.; Didona, D.; Cardone, M.; Calvieri, S. Actinic Keratosis Pathogenesis Update and New Patents. Recent Pat. Inflamm. Allergy Drug Discov. 2016, 10, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Jetter, N.; Chandan, N.; Wang, S.; Tsoukas, M. Field Cancerization Therapies for Management of Actinic Keratosis: A Narrative Review. Am. J. Clin. Dermatol. 2018, 19, 543–557. [Google Scholar] [CrossRef] [PubMed]
- Lanoue, J.; Chen, C.; Goldenberg, G. Actinic keratosis as a marker of field cancerization in excision specimens of cutaneous malignancies. Cutis 2016, 97, 415–420. [Google Scholar] [PubMed]
- Didona, D.; Paolino, G.; Bottoni, U.; Cantisani, C. Non Melanoma Skin Cancer Pathogenesis Overview. Biomedicines 2018, 6, 6. [Google Scholar] [CrossRef] [Green Version]
- Braun, R.P.; Ludwig, S.; Marghoob, A.A. Differential Diagnosis of Seborrheic Keratosis: Clinical and Dermoscopic Features. J. Drugs Dermatol. JDD 2017, 16, 835–842. [Google Scholar]
- Quaedvlieg, P.; Tirsi, E.; Thissen, M.; Krekels, G. Actinic keratosis: How to differentiate the good from the bad ones? Eur. J. Dermatol. 2006, 16, 335–339. [Google Scholar]
- Ortonne, J.P. From actinic keratosis to squamous cell carcinoma. Br. J. Dermatol. 2002, 146, 20–23. [Google Scholar] [CrossRef]
- Lebwohl, M.; Swanson, N.; Anderson, L.L.; Melgaard, A.; Xu, Z.; Berman, B. Ingenol mebutate gel for actinic keratosis. N. Engl. J. Med. 2012, 366, 1010–1019. [Google Scholar] [CrossRef] [Green Version]
- Sirinukunwattana, K.; Raza, S.E.A.; Tsang, Y.-W.; Snead, D.R.; Cree, I.A.; Rajpoot, N.M. Locality sensitive deep learning for detection and classification of nuclei in routine colon cancer histology images. IEEE Trans. Med. Imaging 2016, 35, 1196–1206. [Google Scholar] [CrossRef] [Green Version]
- Albarqouni, S.; Baur, C.; Achilles, F.; Belagiannis, V.; Demirci, S.; Navab, N. Aggnet: Deep learning from crowds for mitosis detection in breast cancer histology images. IEEE Trans. Med. Imaging 2016, 35, 1313–1321. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Li, J.; Sarma, K.V.; Ho, K.C.; Shen, S.; Knudsen, B.S.; Gertych, A.; Arnold, C.W. Path R-CNN for prostate cancer diagnosis and gleason grading of histological images. IEEE Trans. Med. Imaging 2018, 38, 945–954. [Google Scholar] [CrossRef] [PubMed]
- Jalal Deen, K.; Ganesan, R.; Merline, A. Fuzzy-C-means clustering based segmentation and CNN-classification for accurate segmentation of lung nodules. Asian Pac. J. Cancer Prev. APJCP 2017, 18, 1869. [Google Scholar]
- Gao, F.; Wu, T.; Li, J.; Zheng, B.; Ruan, L.; Shang, D.; Patel, B. SD-CNN: A shallow-deep CNN for improved breast cancer diagnosis. Comput. Med. Imaging Graph. 2018, 70, 53–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Hu, H.; Chen, S.; Huang, Y.; Guan, Q. Cancer cells detection in phase-contrast microscopy images based on Faster R-CNN. In Proceedings of the 2016 9th International Symposium on Computational Intelligence and Design (ISCID), Hangzhou, China, 10–11 December 2016; pp. 363–367. [Google Scholar]
- Kawahara, J.; Hamarneh, G. Multi-resolution-tract CNN with hybrid pretrained and skin-lesion trained layers. In Proceedings of the International Workshop on Machine Learning in Medical Imaging, Athens, Greece, 17 October 2016; pp. 164–171. [Google Scholar]
- Kaur, P.; Dana, K.J.; Cula, G.O.; Mack, M.C. Hybrid deep learning for reflectance confocal microscopy skin images. In Proceedings of the 2016 23rd International Conference on Pattern Recognition (ICPR), Cancún, Mexico, 4–8 December 2016; pp. 1466–1471. [Google Scholar]
- Lopez, A.R.; Giro-i-Nieto, X.; Burdick, J.; Marques, O. Skin lesion classification from dermoscopic images using deep learning techniques. In Proceedings of the 2017 13th IASTED International Conference on Biomedical Engineering (BioMed), Innsbruck, Austria, 20–21 February 2017; pp. 49–54. [Google Scholar]
- Harangi, B. Skin lesion detection based on an ensemble of deep convolutional neural network. arXiv 2017, arXiv:1705.03360. [Google Scholar]
- Tajbakhsh, N.; Suzuki, K. Comparing two classes of end-to-end machine-learning models in lung nodule detection and classification: MTANNs vs. CNNs. Pattern Recognit. 2017, 63, 476–486. [Google Scholar] [CrossRef]
- Zhao, X.; Liu, L.; Qi, S.; Teng, Y.; Li, J.; Qian, W. Agile convolutional neural network for pulmonary nodule classification using CT images. Int. J. Comput. Assist. Radiol. Surg. 2018, 13, 585–595. [Google Scholar] [CrossRef]
- Tschandl, P.; Rosendahl, C.; Kittler, H. The HAM10000 dataset, a large collection of multi-source dermatoscopic images of common pigmented skin lesions. Sci. Data 2018, 5, 180161. [Google Scholar] [CrossRef]
- LeCun, Y.; Bottou, L.; Bengio, Y.; Haffner, P. Gradient-based learning applied to document recognition. Proc. IEEE 1998, 86, 2278–2324. [Google Scholar] [CrossRef] [Green Version]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. In Proceedings of the Advances in Neural Information Processing Systems, Lake Tahoe, NV, USA, 3–6 December 2012; pp. 1097–1105. [Google Scholar]
- Han, S.S.; Lim, W.; Kim, M.S.; Park, I.; Park, G.H.; Chang, S.E. Interpretation of the Outputs of a Deep Learning Model Trained with a Skin Cancer Dataset. J. Investig. Dermatol. 2018, 138, 2275. [Google Scholar] [CrossRef] [Green Version]
- Wu, E.; Wu, K.; Cox, D.; Lotter, W. Conditional infilling GANs for data augmentation in mammogram classification. In Image Analysis for Moving Organ, Breast, and Thoracic Images; Springer: Berlin/Heidelberg, Germany, 2018; pp. 98–106. [Google Scholar]
- Mendes, D.B.; da Silva, N.C. Skin lesions classification using convolutional neural networks in clinical images. arXiv 2018, arXiv:1812.02316. [Google Scholar]
- Li, Y.; Shen, L. Skin lesion analysis towards melanoma detection using deep learning network. Sensors 2018, 18, 556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Codella, N.; Cai, J.; Abedini, M.; Garnavi, R.; Halpern, A.; Smith, J.R. Deep learning, sparse coding, and SVM for melanoma recognition in dermoscopy images. In Proceedings of the International workshop on machine learning in medical imaging, Nice, France, 1 October 2012; pp. 118–126. [Google Scholar]
- Mirunalini, P.; Chandrabose, A.; Gokul, V.; Jaisakthi, S. Deep learning for skin lesion classification. arXiv 2017, arXiv:1703.04364. [Google Scholar]
- Vasconcelos, M.J.M.; Rosado, L.; Ferreira, M. A new color assessment methodology using cluster-based features for skin lesion analysis. In Proceedings of the 2015 38th International Convention on Information and Communication Technology, Electronics and Microelectronics (MIPRO), Opatija, Croatia, 25–29 May 2015; pp. 373–378. [Google Scholar]
- Ohki, K.; Celebi, M.E.; Schaefer, G.; Iyatomi, H. Building of readable decision trees for automated melanoma discrimination. In Proceedings of the International Symposium on Visual Computing, Las Vegas, NV, USA, 14–16 December 2015; pp. 712–721. [Google Scholar]
- Lober, B.A.; Lober, C.W. Actinic keratosis is squamous cell carcinoma. South. Med. J. 2000, 93, 650–655. [Google Scholar] [CrossRef] [PubMed]
- Dinehart, S.M.; Nelson-Adesokan, P.; Cockerell, C.; Russell, S.; Brown, R. Metastatic cutaneous squamous cell carcinoma derived from actinic keratosis. Cancer 1997, 79, 920–923. [Google Scholar] [CrossRef]
- Zhao, Y.; Li, C.; Wen, C.; Wei, Y.; Li, R.; Wang, G.; Tu, P. The prevalence of actinic keratosis in patients visiting dermatologists in two hospitals in China. Br. J. Dermatol. 2016, 174, 1005–1010. [Google Scholar] [CrossRef]
- Gagniuc, P.A.; Ionescu-Tirgoviste, C.; Gagniuc, E.; Militaru, M.; Nwabudike, L.C.; Pavaloiu, B.I.; Vasilăţeanu, A.; Goga, N.; Drăgoi, G.; Popescu, I. Spectral forecast: A general purpose prediction model as an alternative to classical neural networks. Chaos Interdiscip. J. Nonlinear Sci. 2020, 30, 033119. [Google Scholar] [CrossRef]
- Lanzanò, L.; Scordino, A.; Privitera, S.; Tudisco, S.; Musumeci, F. Spectral analysis of Delayed Luminescence from human skin as a possible non-invasive diagnostic tool. Eur. Biophys. J. 2007, 36, 823–829. [Google Scholar] [CrossRef]
- Gagniuc, P.A. Markov Chains: From Theory to Implementation and Experimentation; John Wiley & Sons: Hoboken, NJ, USA, 2017. [Google Scholar]
- Cantisani, C.; Paolino, G.; Pellacani, G.; Didona, D.; Scarno, M.; Faina, V.; Gobello, T.; Calvieri, S. MAL daylight photodynamic therapy for actinic keratosis: Clinical and imaging evaluation by 3D camera. Int. J. Mol. Sci. 2016, 17, 1108. [Google Scholar] [CrossRef] [Green Version]
- Cantisani, C.; Paolino, G.; Corsetti, P.; Bottoni, U.; Didona, D.; Calvieri, S. Evaluation of Ingenol mebutate efficacy for the treatment of actinic keratosis with Antera 3D camera. Eur. Rev. Med. Pharm. Sci. 2015, 19, 92–97. [Google Scholar]
- Mazzella, C.; Greco, V.; Costa, C.; Scalvenzi, M.; Russo, D.; Savastano, R.; Staibano, S.; Fabbrocini, G. Management of clinical and subclinical actinic keratoses with histological and immunohistochemical assessments by confocal microscopy. Dermatol. Ther. 2018, 31, e12672. [Google Scholar] [CrossRef] [PubMed]
- Mercuri, S.R.; Rizzo, N.; Bellinzona, F.; Pampena, R.; Brianti, P.; Moffa, G.; Colombo, F.L.; Bearzi, P.; Longo, C.; Paolino, G. Digital ex-vivo confocal imaging for fast Mohs surgery in nonmelanoma skin cancers: An emerging technique in dermatologic surgery. Dermatol. Ther. 2019, 32, e13127. [Google Scholar] [CrossRef] [PubMed]
- Carbone, A.; Ferrari, A.; Paolino, G.; Buccini, P.; De Simone, P.; Eibenschutz, L.; Piemonte, P.; Silipo, V.; Sperduti, I.; Catricalà, C. Lentigo maligna of the face: A quantitative simple method to identify individual patient risk probability on dermoscopy. Australas. J. Dermatol. 2017, 58, 286–291. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | AK-DL | AlexNet Transfer | GoogLeNet Transfer | ResNet Transfer |
|---|---|---|---|---|
| Momentum | 0.9 | 0.6 | 0.9 | 0.7 |
| InitialLearnRate | 0.0001 | 0.0001 | 0.0001 | 0.0001 |
| MiniBatchSize | 10 | 20 | 15 | 20 |
| L2Regularization | 0.0005 | 0.0001 | 0.0001 | 0.00001 |
| CNN Models | Acc | Sens | Spec | Prec | MCC | Training Time (s) |
|---|---|---|---|---|---|---|
| AK-DL | 0.925 | 0.938 | 0.909 | 0.924 | 0.848 | 123.0 |
| AlexNet | 0.862 | 0.908 | 0.815 | 0.832 | 0.727 | 2426.0 |
| GoogLeNet | 0.874 | 0.874 | 0.875 | 0.901 | 0.746 | 13,761.0 |
| ResNet | 0.774 | 0.829 | 0.721 | 0.740 | 0.553 | 15,488.0 |
| Models | Acc | Sens | Spec | Prec | MCC | Training Time (s) |
|---|---|---|---|---|---|---|
| AK-DL | 0.925 | 0.938 | 0.909 | 0.924 | 0.848 | 123.0 |
| HOG+K-NN | 0.713 | 0.954 | 0.511 | 0.619 | 0.506 | 12.4 |
| HOG+RF | 0.778 | 0.796 | 0.763 | 0.735 | 0.557 | 20.1 |
| HOG+SVM | 0.791 | 0.780 | 0.800 | 0.766 | 0.579 | 20.2 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, L.; Chen, A.; Zhang, Y.; Wang, X.; Zhang, Y.; Shen, Q.; Xue, Y. AK-DL: A Shallow Neural Network Model for Diagnosing Actinic Keratosis with Better Performance than Deep Neural Networks. Diagnostics 2020, 10, 217. https://doi.org/10.3390/diagnostics10040217
Wang L, Chen A, Zhang Y, Wang X, Zhang Y, Shen Q, Xue Y. AK-DL: A Shallow Neural Network Model for Diagnosing Actinic Keratosis with Better Performance than Deep Neural Networks. Diagnostics. 2020; 10(4):217. https://doi.org/10.3390/diagnostics10040217
Chicago/Turabian StyleWang, Liyang, Angxuan Chen, Yan Zhang, Xiaoya Wang, Yu Zhang, Qun Shen, and Yong Xue. 2020. "AK-DL: A Shallow Neural Network Model for Diagnosing Actinic Keratosis with Better Performance than Deep Neural Networks" Diagnostics 10, no. 4: 217. https://doi.org/10.3390/diagnostics10040217
APA StyleWang, L., Chen, A., Zhang, Y., Wang, X., Zhang, Y., Shen, Q., & Xue, Y. (2020). AK-DL: A Shallow Neural Network Model for Diagnosing Actinic Keratosis with Better Performance than Deep Neural Networks. Diagnostics, 10(4), 217. https://doi.org/10.3390/diagnostics10040217