Mammographic Breast Density and Urbanization: Interactions with BMI, Environmental, Lifestyle, and Other Patient Factors

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample
2.2. Questionnaire
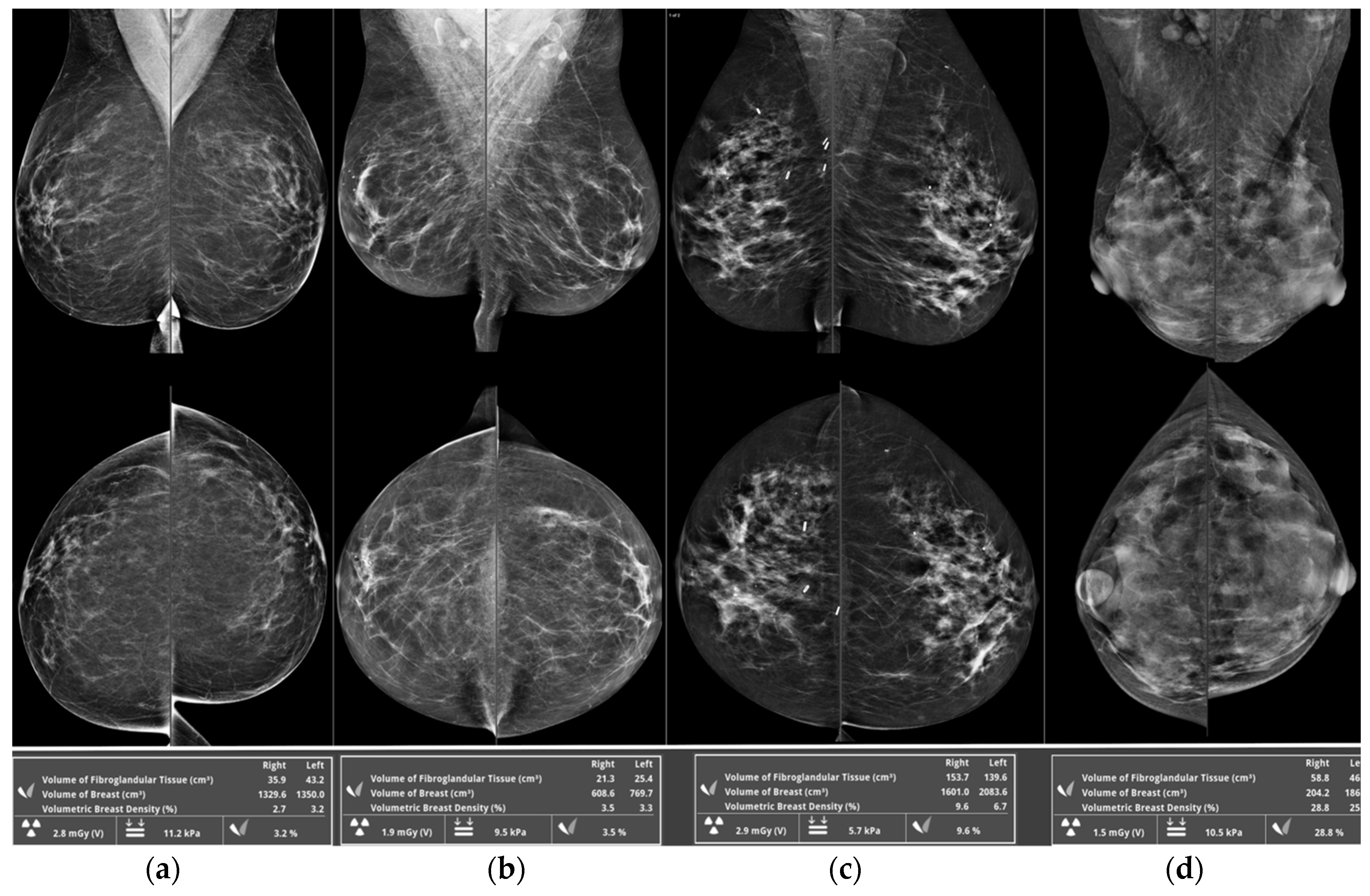
2.3. Breast Density Assessment
2.4. Statistical Analysis
3. Results
3.1. Study Population Characteristics
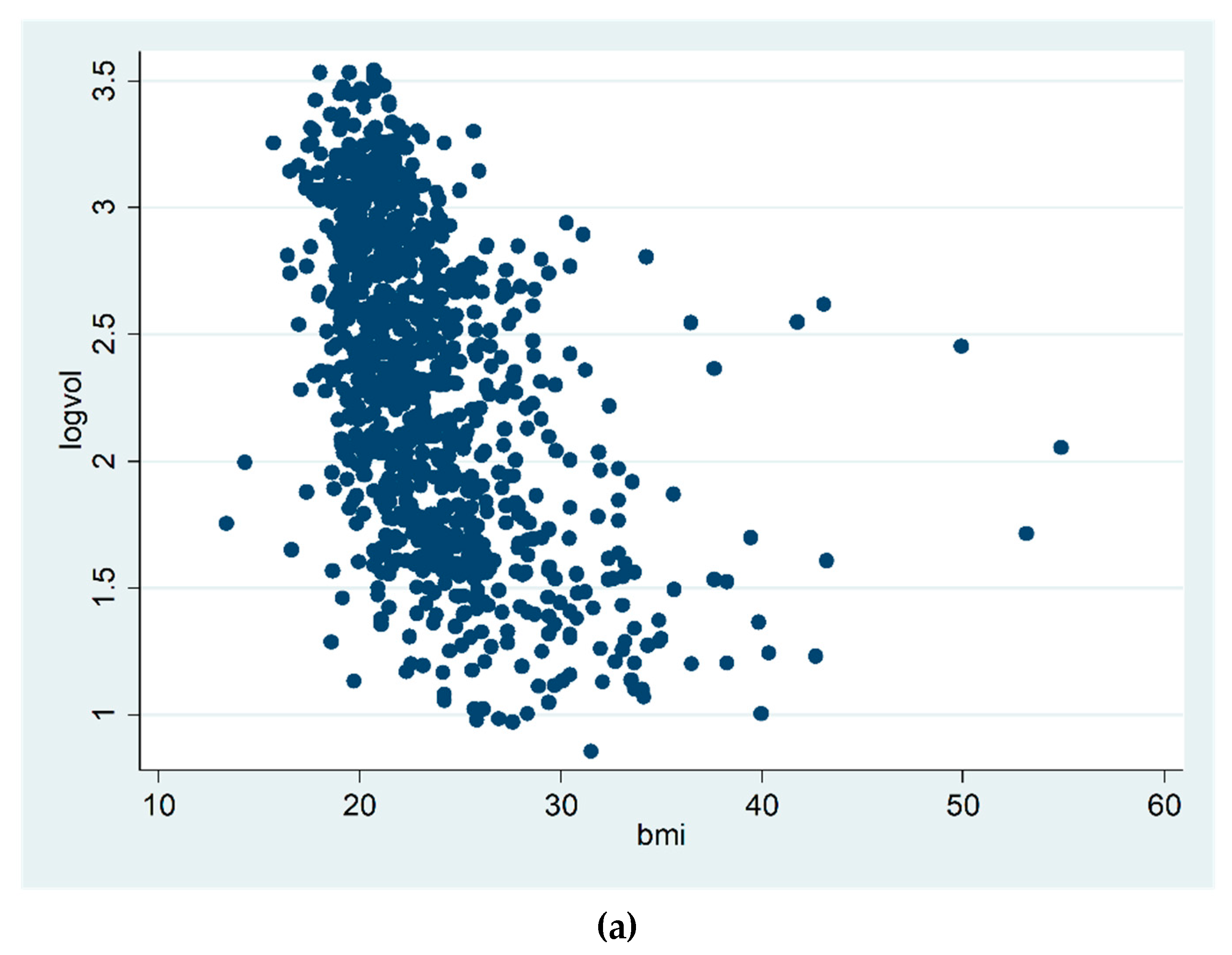
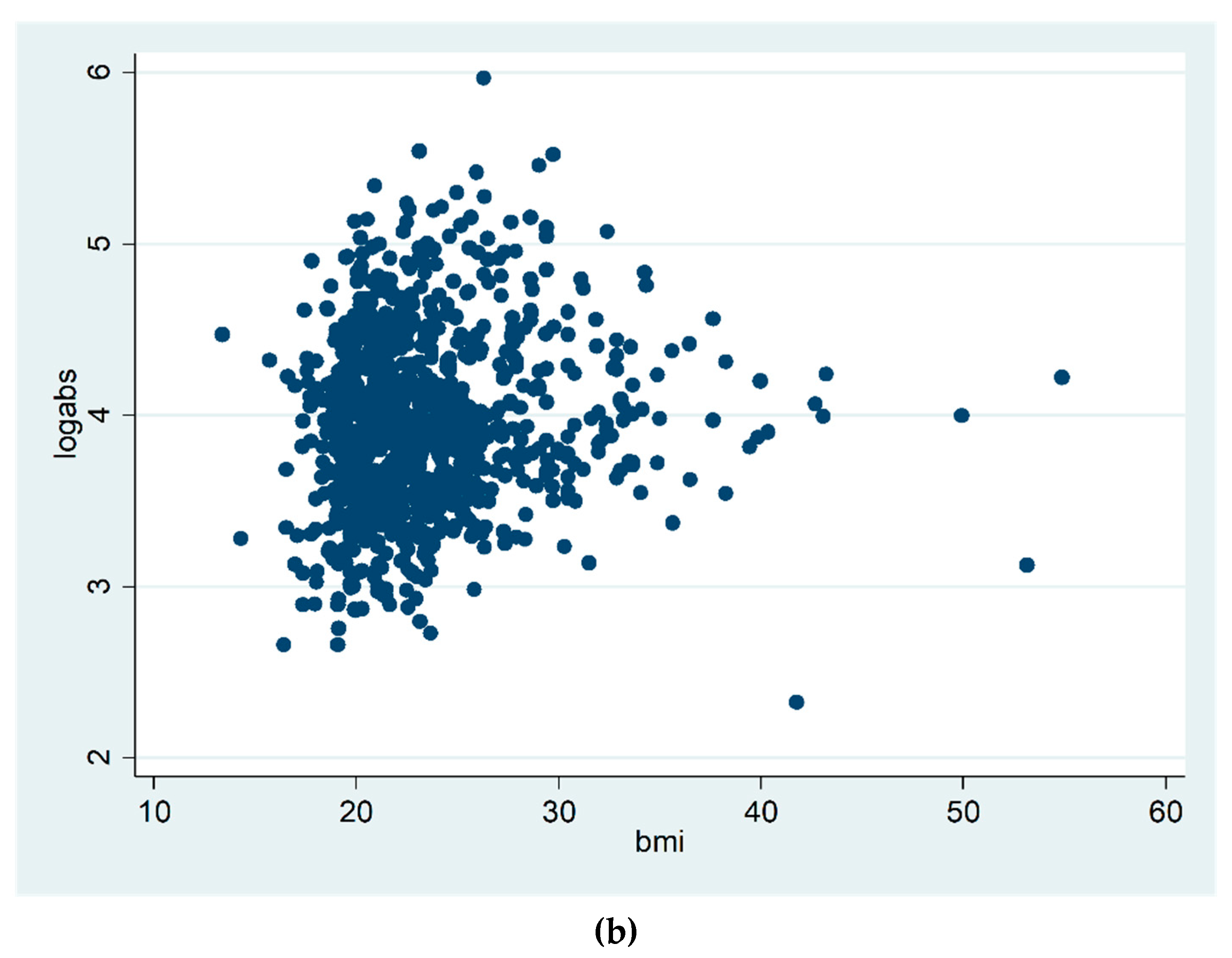
3.2. Age and BMI and Breast Density
3.3. Urban Residence/Working in the Urban Setting and BMI
3.4. Urban Residence and Breast Density
3.5. Working in the Urban Setting and Breast Density
3.6. Urban Residence and Working in the Urban Setting and Breast Density
3.7. Automated Quantitative vs. Qualitative Breast Density Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- McCormack, V.A.; Silva, I.D.S. Breast density and parenchymal patterns as markers of breast cancer risk: A meta-analysis. Cancer Epidemiol. Biomark. Prev. 2006, 15, 1159–1169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyd, N.F.; Martin, L.J.; Sun, L.; Guo, H.; Chiarelli, A.; Hislop, G.; Minkin, S. Body size, mammographic density, and breast cancer risk. Cancer Epidemiol. Biomark. Prev. 2006, 15, 2086–2092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciatto, S.; Houssami, N.; Apruzzese, A.; Bassetti, E.; Brancato, B.; Carozzi, F.; Pesce, B. Categorizing breast mammographic density: Intra- and interobserver reproducibility of BI-RADS density categories. Breast 2005, 14, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Chan, H.P.; Petrick, N.; Helvie, M.A.; Goodsitt, M.M.; Sahiner, B.; Hadjiiski, L.M. Computerized image analysis: Estimation of breast density on mammograms. Med. Phys. 2001, 28, 1056–1069. [Google Scholar] [CrossRef] [PubMed]
- Assi, V.; Warwick, J.; Cuzick, J.; Duffy, S.W. Clinical and epidemiological issues in mammographic density. Nat. Rev. Clin. Oncol. 2011, 9, 33–40. [Google Scholar] [CrossRef]
- Aitken, Z.; Walker, K.; Stegeman, B.H.; Wark, P.A.; Moss, S.M.; McCormack, V.A.; dos Santos Silva, I. Mammographic density and markers of socioeconomic status: A cross-sectional study. BMC Cancer 2010, 10, 35. [Google Scholar] [CrossRef] [Green Version]
- Hopper, J.L. Odds per adjusted standard deviation: Comparing strengths of associations for risk factors measured on different scales and across diseases and populations. Am. J. Epidemiol. 2015, 182, 863–867. [Google Scholar] [CrossRef] [Green Version]
- Cabanes, A.; Pastor-Barriuso, R.; García-López, M.; Pedraz-Pingarrón, C.; Sánchez-Contador, C.; Carrete, J.A.V.; Peris, M. Alcohol, tobacco, and mammographic density: A population-based study. Breast Cancer Res. Treat. 2011, 129, 135–147. [Google Scholar] [CrossRef] [Green Version]
- Butler, L.M.; Gold, E.B.; Greendale, G.A.; Crandall, C.J.; Modugno, F.; Oestreicher, N.; Habel, L.A. Menstrual and reproductive factors in relation to mammographic density: The study of women’s health across the nation (SWAN). Breast Cancer Res. Treat. 2008, 112, 165–174. [Google Scholar] [CrossRef] [Green Version]
- Viel, J.F.; Rymzhanova, R. Mammographic density and urbanization: A population-based screening study. J. Med. Screen 2012, 19, 20–25. [Google Scholar] [CrossRef]
- Emaus, M.J.; Bakker, M.F.; Beelen, R.M.; Veldhuis, W.B.; Peeters, P.H.; van Gils, C.H. Degree of urbanization and mammographic density in Dutch breast cancer screening participants: Results from the EPIC-NL cohort. Breast Cancer Res. Treat. 2014, 148, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Perry, N.M.; Allgood, P.C.; Milner, S.E.; Mokbel, K.; Duffy, S.W. Mammographic breast density by area of residence: Possible evidence of higher density in urban areas. Curr. Med. Res. Opin. 2008, 24, 365–368. [Google Scholar] [CrossRef] [PubMed]
- Perry, N.M.; Allgood, P.C.; Duffy, S.W.; Mokbel, K. Exposure to traffic emissions throughout life and risk of breast cancer. Cancer Causes Control 2008, 19, 435. [Google Scholar] [CrossRef] [PubMed]
- Hall, S.A.; Kaufman, J.S.; Millikan, R.C.; Ricketts, T.C.; Herman, D.; Savitz, D.A. Urbanization and breast cancer incidence in North Carolina, 1995-1999. Ann. Epidemiol. 2005, 15, 796–803. [Google Scholar] [CrossRef]
- Wang, J.; Xie, P.; Xu, Y.; Kettrup, A.; Schramm, K.-W. Differing estrogen activities in the organic phase of air particulate matter collected during sunny and foggy weather in a Chinese city detected by a recombinant yeast bioassay. Atmos. Env. 2004, 38, 6157–6166. [Google Scholar] [CrossRef]
- Nie, J.; Beyea, J.; Bonner, M.R.; Han, D.; Vena, J.E.; Rogerson, P.; Freudenheim, J.L. Exposure to traffic emissions throughout life and risk of breast cancer: The Western New York Exposures and Breast Cancer (WEB) study. Cancer Causes Control 2007, 18, 947–955. [Google Scholar] [CrossRef] [Green Version]
- Sickles, E.; D’Orsi, C.J.; Bassett, L.W. (Eds.) ACR BI-RADS® Mammography. In ACR BI-RADS® Atlas, Breast Imaging Reporting and Data System, 5th ed.; American College of Radiology: Reston, VA, USA, 2003. [Google Scholar]
- Huo, C.W.; Chew, G.L.; Britt, K.; Ingman, W.V.; Henderson, M.A.; Hopper, J.L.; Thompson, E.W. Mammographic density-a review on the current understanding of its association with breast cancer. Breast Cancer Res. Treat. 2014, 144, 479–502. [Google Scholar] [CrossRef]
- Boyd, N.F.; Lockwood, G.A.; Byng, J.W.; Little, L.E.; Yaffe, M.J.; Tritchler, D.L. The relationship of anthropometric measures to radiological features of the breast in premenopausal women. Br. J. Cancer. 1998, 78, 1233–1238. [Google Scholar] [CrossRef] [Green Version]
- Schetter, S.E.; Hartman, T.J.; Liao, J.; Richie, J.P.; Prokopczyk, B.; DuBrock, C.; Manni, A. Differential impact of body mass index on absolute and percent breast density: Implications regarding their use as breast cancer risk biomarkers. Breast Cancer Res. Treat. 2014, 146, 355–363. [Google Scholar] [CrossRef]
- Reeves, K.W.; Stone, R.A.; Modugno, F.; Ness, R.B.; Vogel, V.G.; Weissfeld, J.L.; Cauley, J.A. Longitudinal association of anthropometry with mammographic breast density in the Study of Women’s Health Across the Nation. Int. J. Cancer 2009, 124, 1169–1177. [Google Scholar] [CrossRef] [Green Version]
- Haars, G.; van Noord, P.A.; van Gils, C.H.; Grobbee, D.E.; Peeters, P.H. Measurements of breast density: No ratio for a ratio. Cancer Epidemiol. Biomark. Pre. 2005, 14, 2634–2640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Assi, V.; Massat, N.J.; Thomas, S.; MacKay, J.; Warwick, J.; Kataoka, M.; Duffy, S.W. A case-control study to assess the impact of mammographic density on breast cancer risk in women aged 40-49 at intermediate familial risk. Int. J. Cancer 2015, 136, 2378–2387. [Google Scholar] [CrossRef] [PubMed]
- Van der Waal, D.; en Heeten, G.J.; Pijnappel, R.M.; Schuur, K.H.; Timmers, J.M.; Verbeek, A.L.; Broeders, M.J. Comparing visually assessed BI-RADS breast density and automated volumetric breast density software: A cross-sectional study in a Breast cancer screening setting. PLoS ONE 2015, 10, e0136667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yaghjyan, L.; Arao, R.; Brokamp, C.; O’Meara, E.S.; Sprague, B.L.; Ghita, G.; Ryan, P. Association between air pollution and mammographic breast density in the Breast Cancer Surveilance Consortium. Breast Cancer Res. 2017, 19, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | n (%) | Percent Density Mean (SD) | Absolute Density Mean (SD) |
|---|---|---|---|
| Entire population sample | 967 (100) | 11.9 (6.9) | 60.3 (35.6) |
| Ethnicity | |||
| White | 912 (94.3) | 11.9 (6.9) | 60.0 (35.6) |
| Mixed | 11 (1.1) | 12.1 (3.3) | 58.2 (36.2) |
| Asian | 21 (2.2) | 14.2 (8.3) | 62.7 (39.5) |
| Black | 3 (0.3) | 12.7 (11.4) | 99.4 (76.2) |
| Other | 16 (1.6) | 12.4 (6.6) | 68.5 (27.0) |
| Missing | 4 (0.4) | 8.3 (5.9) | 58.5 (20.8) |
| Education level 1 | |||
| None | 29 (3.0) | 9.4 (4.9) | 56.1 (26.9) |
| GCSE | 141 (14.6) | 11.2 (7.2) | 61.2 (34.8) |
| A level | 190 (19.6) | 11.2 (6.9) | 61.9 (36.3) |
| University | 351 (36.3) | 12.4 (7.1) | 58.7 (33.2) |
| Postgrad | 248 (25.6) | 12.9 (6.8) | 61.6 (40.1) |
| Missing | 8 (0.8) | 7.3 2.2) | 51.8 (11.2) |
| Urban Resident | |||
| No | 365 (37.7) | 11.3 (6.7) | 60.9 (37.8) |
| Yes | 602 (62.2) | 12.4 (7.1) | 60.0 (34.3) |
| Urban Workplace 1A | |||
| No | 149 (15.4) | 11.6 (6.7) | 60.8 (36.3) |
| Yes | 282 (29.2) | 13.0 (7.1) | 65.0 (39.5) |
| Missing | 536 (55.4) | 11.5 (6.1) | 57.7 (33.1) |
| Smoker | |||
| Current | 47 (4.9) | 11.8 (7.5) | 56.1 (32.2) |
| Ex-smoker | 364 (37.6) | 12.2 (6.9) | 61.2 (35.9) |
| Never | 552 (37.1) | 11.8 (7.0) | 60.0 (35.8) |
| Missing | 4 (0.4) | 15.5 (3.9) | 66.2 (30.1) |
| Drinks per week | |||
| 0 | 137 (14.2) | 12.0 (7.9) | 66.6 (44.6) |
| < 5 | 411 (42.5) | 11.8 (6.8) | 57.4 (33.5) |
| 5–14 | 315 (32.6) | 12.4 (7.0) | 61.7 (34.4) |
| > 14 | 58 (6.0) | 11.2 (6.2) | 59.5 (36.0) |
| Missing | 46 (4.8) | 11.8 (5.9) | 58.7 (30.4) |
| HRT use: current | |||
| No | 788 (81.5) | 12.0 (7.0) | 60.5 (36.6) |
| Yes | 169 (17.5) | 12.1 (6.9) | 59.9 (31.5) |
| Missing | 10 (1.0) | 8.9 (5.3) | 54.0 (22.8) |
| HRT use: ever | |||
| No | 645 (66.7) | 12.6 (7.1) | 62.0 (38.4) |
| Yes | 319 (33) | 10.7 (6.5) | 56.9 (9.2) |
| Missing | 3 (0.3) | 12.6 (8.5) | 61.2 (17.1) |
| Calcium supplement | |||
| No | 748 (77.3) | 12.2 (7.1) | 62.2 (37.0) |
| Yes | 194 (20.1) | 11.2 (5.9) | 53.9 (29.0) |
| Missing | 25 (2.6) | 12.0 (9.2) | 52.3 (35.1) |
| Vitamin D supplement | |||
| No | 635 (65.7) | 12.0 (7.0) | 62.3 (36.0) |
| Yes | 239 (24.7) | 11.7 (6.8) | 55.6 (29.2) |
| Missing | 93 (9.6) | 12.3 (7.3) | 58.6 (45.8) |
| Physical activity per week | |||
| < 30 mins | 75 (7.8) | 10.8 (7.7) | 65.5 (39.6) |
| 30–60 | 148 (15.3) | 10.4 (6.6) | 61.7 (32.8) |
| > 60 | 716 (74.0) | 12.4 (6.9) | 59.8 (35.8) |
| Missing | 28 (2.9) | 12.2 (7.1) | 52.0 (33.9) |
| OCs (current use) | |||
| No | 914 (94.6) | 12.0 (7.0) | 60.9 (3.0) |
| Yes | 34 (3.6) | 11.3 (5.3) | 50.1 (28.2) |
| Missing | 19 (2.0) | 10.6 (6.0) | 51.7 (28.3) |
| OCs (ever use) | |||
| No | 233 (24.1) | 11.3 (6.9) | 60.6 (36.8) |
| Yes | 721 (74.9) | 12.2 (7.0) | 60.5 (35.4) |
| Missing | 10 (1.0) | 10.3 (5.2) | 39.8 (10.4) |
| Nulliparous | |||
| No | 827 (85.5) | 12.1 (6.9) | 59.8 (35.4) |
| Yes | 137 (14.2) | 11.4 (7.1) | 63.9 (37.0) |
| Missing | 3 (0.3) | 9.5 (4.2) | 44.1 (10.2) |
| Menopausal status | |||
| Pre-menopausal | 305 (31.5) | 14.8 (7.3) | 69.2 (43.8) |
| Peri-menopausal | 100 (10.3) | 13.6 (6.5) | 64.1 (37.0) |
| Post-menopausal | 536 (55.4) | 10.0 (6.1) | 53.5 (27.8) |
| Missing | 26 (2.7) | 14.1 (6.7) | 80.4 (36.1) |
| Ever breast fed | |||
| No | 308 (31.8) | 10.8 (6.8) | 63.3 (37.6) |
| Yes | 600 (62.0) | 12.5 (6.9) | 58.6 (34.7) |
| Missing | 59 (6.1) | 13.2 (7.7) | 61.8 (34.1) |
| Hysterectomy | |||
| No | 785 (81.2) | 12.3 (7.0) | 60.4 (36.4) |
| Yes | 156 (16.1) | 9.9 (6.5) | 58.3 (29.5) |
| Missing | 26 (2.7) | 13.5 (6.2) | 68.7 (45.4) |
| Family history breast cancer | |||
| No | 541 (55.9) | 12.0 (7.1) | 59.3 (33.2) |
| Yes | 381 (39.4) | 12.0 (6.8) | 62.2 (38.7) |
| Missing | 45 (4.6) | 10.6 (6.2) | 55.9 (36.0) |
| Age (years) | |||
| < 45 | 151 (15.6) | 153 (7.3) | 67.4 (37.1) |
| 45–54 | 381 (39.4) | 13.6 (6.8) | 67.2 (41.8) |
| 55–64 | 254 (26.3) | 9.8 (6.2) | 53.5 (29.7) |
| 65+ | 181 (18.7) | 8.7 (5.6) | 49.4 (20.5) |
| BMI | |||
| < 20.6 | 246 (25.4) | 16.3 (6.7) | 55.3 (29.5) |
| 20.6 to < 22.4 | 239 (24.7) | 14.2 (7.3) | 59.3 (29.0) |
| 22.4 to < 25.0 | 249 (25.7) | 10.1 (5.2) | 59.3 (36.7) |
| ≥ 25.0 | 233 (24.1) | 7.2 (4.3) | 67.7 (44.6) |
| Smoking (pack-years in ever smokers) | |||
| <1 | 39 (11.4) | 12.8 (7.3) | 55.2 (32.0) |
| 1-4 | 113 (32.9) | 12.6 (6.4) | 59.0 (32.7) |
| 5–11 | 98 (28.6) | 11.0 (6.5) | 60.6 (34.7) |
| 12+ | 93 (27.1) | 11.4 (6.9) | 61.9 (33.9) |
| Age at menarche (years) | |||
| < 12 | 130 (13.4) | 9.8 (6.1) | 55.8 (29.8) |
| 12 | 213 (22.0) | 11.2 (6.9) | 60.0 (34.0) |
| 13–14 | 466 (48.2) | 12.5 (7.1) | 60.9 (39.0) |
| 15+ | 143 (14.8) | 13.2 (6.9) | 62.3 (30.8) |
| Age at first birth (years) | |||
| < 25 | 134 (13.9) | 9.7 (6.4) | 57.4 (36.5) |
| 25–29 | 255 (26.4) | 12.4 (7.1) | 59.9 (38.7) |
| 30–34 | 228 (23.6) | 12.6 (6.6) | 59.1 (34.1) |
| 35+ | 122 (12.6) | 12.9 (7.0) | 63.1 (31.2) |
| Missing | 228 (23.6) | 11.7 (7.2) | 62.2 (35.5) |
| Parity | |||
| 0 | 154 (15.9) | 11.3 (6.9) | 62.5 (35.8) |
| 1 | 107 (11.1) | 12.2 (7.3) | 73.8 (42.0) |
| 2 | 373 (38.6) | 11.9 (7.1) | 57.1 (31.4) |
| 3 | 206 (21.3) | 12.0 (6.3) | 56.4 (36.7) |
| 4+ | 55 (5.7) | 12.7 (7.3) | 61.8 (39.5) |
| Missing | 72 (7.4) | 12.8 (7.8) | 61.8 (35.4) |
| Percent density (n = 917) | Absolute Density (n = 859) | |||
|---|---|---|---|---|
| Coefficient (SE) | p-value | Coefficient (SE) | p-value | |
| Urban resident | ||||
| No | Ref | Ref | ||
| Yes | 0.02 (0.03) | 0.6 | −0.04 (0.04) | 0.3 |
| BMI | −0.06 (0.004) | < 0.001 | 0.009 (0.004) | 0.03 |
| Age | −0.02 (0.003) | < 0.001 | −0.005 (0.003) | 0.1 |
| HRT current use | ||||
| No | Ref | Ref | ||
| Yes | 0.15 (0.04) | 0.01 | 0.14 (0.05) | 0.01 |
| Age at menarche | 0.04 (0.01) | 0.01 | 0.02 (0.01) | 0.1 |
| Menopausal status | ||||
| Premenopausal | Ref | Ref | ||
| Perimenopausal | −0.01 (0.06) | 0.9 | −0.02 (0.07) | 0.8 |
| Postmenopausal | −0.01 (0.05) | < 0.001 | −0.19 (0.06) | 0.002 |
| Breast fed | ||||
| No | Ref | |||
| Yes | −0.10 (0.05) | 0.04 | ||
| OC (ever use) | ||||
| No | Ref | |||
| Yes | −0.06 (0.04) | 0.15 | ||
| Parity | −0.03 (0.02) | 0.1 | ||
| Family history of breast cancer | ||||
| No | Ref | |||
| Yes | 0.05 (0.04) | 0.2 | ||
| Smoker | ||||
| Never | Ref | |||
| Past | 0.05 (0.04) | 0.2 | ||
| Current | −0.11 (0.09) | 0.2 | ||
| Calcium supplement | ||||
| No | Ref | |||
| Yes | −0.08 (0.05) | 0.1 | ||
| Drinks per week | ||||
| 0 | Ref | |||
| < 5 | −0.18 (0.06) | 0.002 | ||
| 5–14 | −0.10 (0.06) | 0.1 | ||
| > 14 | −0.13 (0.09) | 0.2 | ||
| Percent Density (n = 330) | Absolute Density (n = 323) | |||
|---|---|---|---|---|
| Coefficient (SE) | p-value | Coefficient (SE) | p-value | |
| Work London | ||||
| No | Ref | Ref | ||
| Yes | 0.06 (0.06) | 0.3 | 0.001 (0.07) | 0.99 |
| BMI | −0.05 (0.005) | <0.001 | 0.003 (0.006) | 0.6 |
| Age | −0.02 (0.005) | <0.001 | −0.02 (0.005) | 0.001 |
| HRT current use | ||||
| No | Ref | Ref | ||
| Yes | 0.11 (0.08) | 0.1 | 0.13 (0.08) | 0.1 |
| Age at menarche | 0.04 (0.02) | 0.04 | 0.03 | 0.07 |
| Menopausal status | ||||
| Pre-menopausal | Ref | Ref | ||
| Peri-menopausal | −0.16 (0.09) | 0.07 | −0.12 (0.09) | 0.2 |
| Post-menopausal | −0.18 (0.08) | 0.03 | −0.12 (0.09) | 0.2 |
| Parity | 0.04 (0.02) | 0.07 | −0.06 (0.02) | 0.01 |
| OC (ever use) | ||||
| No | Ref | |||
| Yes | −0.11 (0.07) | 0.1 | ||
| Hysterectomy | ||||
| No | Ref | |||
| Yes | 0.23 (0.10) | 0.02 | ||
| Smoker | ||||
| Never | Ref | |||
| Past | 0.06 (0.06) | 0.31 | ||
| Current | −0.23 (0.13) | 0.07 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perry, N.; Moss, S.; Dixon, S.; Milner, S.; Mokbel, K.; Lemech, C.; Arkenau, H.-T.; Duffy, S.; Pinker, K. Mammographic Breast Density and Urbanization: Interactions with BMI, Environmental, Lifestyle, and Other Patient Factors. Diagnostics 2020, 10, 418. https://doi.org/10.3390/diagnostics10060418
Perry N, Moss S, Dixon S, Milner S, Mokbel K, Lemech C, Arkenau H-T, Duffy S, Pinker K. Mammographic Breast Density and Urbanization: Interactions with BMI, Environmental, Lifestyle, and Other Patient Factors. Diagnostics. 2020; 10(6):418. https://doi.org/10.3390/diagnostics10060418
Chicago/Turabian StylePerry, Nick, Sue Moss, Steve Dixon, Sue Milner, Kefah Mokbel, Charlotte Lemech, Hendrik-Tobias Arkenau, Stephen Duffy, and Katja Pinker. 2020. "Mammographic Breast Density and Urbanization: Interactions with BMI, Environmental, Lifestyle, and Other Patient Factors" Diagnostics 10, no. 6: 418. https://doi.org/10.3390/diagnostics10060418
APA StylePerry, N., Moss, S., Dixon, S., Milner, S., Mokbel, K., Lemech, C., Arkenau, H.-T., Duffy, S., & Pinker, K. (2020). Mammographic Breast Density and Urbanization: Interactions with BMI, Environmental, Lifestyle, and Other Patient Factors. Diagnostics, 10(6), 418. https://doi.org/10.3390/diagnostics10060418