Effectiveness of Strongyloides Recombinant IgG Immunoreactive Antigen in Detecting IgG and IgG4 Subclass Antibodies for Diagnosis of Human Strongyloidiasis Using Rapid Immunochromatographic Tests


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Parasite Antigens
2.2. Human Sera
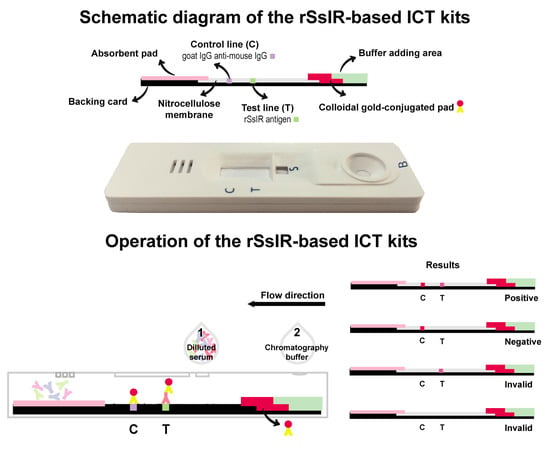
2.3. Immunochromatographic Test Kit
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ericsson, C.D.; Steffen, R.; Siddiqui, A.A.; Berk, S.L. Diagnosis of Strongyloides stercoralis infection. Clin. Infect. Dis. 2001, 33, 1040–1047. [Google Scholar] [CrossRef] [Green Version]
- Buonfrate, D.; Bisanzio, D.; Giorli, G.; Odermatt, P.; Fürst, T.; Greenaway, C.; French, M.; Reithinger, R.; Gobbi, F.; Montresor, A.; et al. The global prevalence of Strongyloides stercoralis infection. Pathogens 2020, 13, 468. [Google Scholar] [CrossRef] [PubMed]
- Casavechia, M.T.; Lonardoni, M.V.; Venazzi, E.A.; Campanerut-Sá, P.A.; da Costa Benalia, H.R.; Mattiello, M.F.; Menechini, P.V.; Dos Santos, C.A.; Teixeira, J.J. Prevalence and predictors associated with intestinal infections by protozoa and helminths in southern Brazil. Parasitol. Res. 2016, 115, 2321–2329. [Google Scholar] [CrossRef] [PubMed]
- Olsen, A.; van Lieshout, L.; Marti, H.; Polderman, T.; Polman, K.; Steinmann, P.; Stothard, R.; Thybo, S.; Verweij, J.J.; Magnussen, P. Strongyloidiasis—The most neglected of the neglected tropical diseases? Trans. R. Soc. Trop. Med. Hyg. 2009, 103, 967–972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thanchomnang, T.; Intapan, P.M.; Sanpool, O.; Rodpai, R.; Tourtip, S.; Yahom, S.; Kullawat, J.; Radomyos, P.; Thammasiri, C.; Maleewong, W. First molecular identification and genetic diversity of Strongyloides stercoralis and Strongyloides fuelleborni in human communities having contact with long-tailed macaques in Thailand. Parasitol. Res. 2017, 116, 1917–1923. [Google Scholar] [CrossRef]
- Krolewiecki, A.; Nutman, T.B. Strongyloidiasis: A neglected tropical disease. Infect. Dis. Clin. North. Am. 2019, 33, 135–151. [Google Scholar] [CrossRef]
- Buonfrate, D.; Formenti, F.; Perandin, F.; Bisoffi, Z. Novel approaches to the diagnosis of Strongyloides stercoralis infection. Clin. Microbiol. Infect. 2015, 21, 543–552. [Google Scholar] [CrossRef] [Green Version]
- Verweij, J.J.; Canales, M.; Polman, K.; Ziem, J.; Brienen, E.A.; Polderman, A.M.; van Lieshout, L. Molecular diagnosis of Strongyloides stercoralis in faecal samples using real-time PCR. Trans. R. Soc. Trop. Med. Hyg. 2009, 103, 342–346. [Google Scholar] [CrossRef]
- Janwan, P.; Intapan, P.M.; Thanchomnang, T.; Lulitanond, V.; Anamnart, W.; Maleewong, W. Rapid detection of Opisthorchis viverrini and Strongyloides stercoralis in human fecal samples using a duplex real-time PCR and melting curve analysis. Parasitol. Res. 2011, 109, 1593–1601. [Google Scholar] [CrossRef]
- Repetto, S.A.; Alba Soto, C.D.; Cazorla, S.I.; Tayeldin, M.L.; Cuello, S.; Lasala, M.B.; Tekiel, V.S.; González Cappa, S.M. An improved DNA isolation technique for PCR detection of Strongyloides stercoralis in stool samples. Acta. Trop. 2013, 126, 110–114. [Google Scholar] [CrossRef]
- Schär, F.; Odermatt, P.; Khieu, V.; Panning, M.; Duong, S.; Muth, S.; Marti, H.; Kramme, S. Evaluation of real-time PCR for Strongyloides stercoralis and hookworm as diagnostic tool in asymptomatic schoolchildren in Cambodia. Acta. Trop. 2013, 126, 89–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kristanti, H.; Meyanti, F.; Wijayanti, M.A.; Mahendradhata, Y.; Polman, K.; Chappuis, F.; Utzinger, J.; Becker, S.L.; Murhandarwati, E.E.H. Diagnostic comparison of Baermann funnel, Koga agar plate culture and polymerase chain reaction for detection of human Strongyloides stercoralis infection in Maluku, Indonesia. Parasitol. Res. 2018, 117, 3229–3235. [Google Scholar] [CrossRef] [PubMed]
- Formenti, F.; La Marca, G.; Perandin, F.; Pajola, B.; Romano, M.; Santucci, B.; Silva, R.; Giorli, G.; Bisoffi, Z.; Buonfrate, D. A diagnostic study comparing conventional and real-time PCR for Strongyloides stercoralis on urine and on faecal samples. Acta. Trop. 2019, 190, 284–287. [Google Scholar] [CrossRef] [PubMed]
- Northern, C.; Grove, D.I. Strongyloides stercoralis: Antigenic analysis of infective larvae and adult worms. Int. J. Parasitol. 1990, 20, 381–387. [Google Scholar] [CrossRef]
- Sato, Y.; Inoue, F.; Matsuyama, R.; Shiroma, Y. Immunoblot analysis of antibodies in human strongyloidiasis. Trans. R. Soc. Trop. Med. Hyg. 1990, 84, 403–406. [Google Scholar] [CrossRef]
- Conway, D.J.; Bailey, J.W.; Lindo, J.F.; Robinson, R.D.; Bundy, D.A.; Bianco, A.E. Serum IgG reactivity with 41-, 31-, and 28-kDa larval proteins of Strongyloides stercoralis in individuals with strongyloidiasis. J. Infect. Dis. 1993, 168, 784–787. [Google Scholar] [CrossRef]
- Conway, D.J.; Lindo, J.F.; Robinson, R.D.; Bundy, D.A.; Bianco, A.E. Strongyloides stercoralis: Characterization of immunodiagnostic larval antigens. Exp. Parasitol. 1994, 79, 99–105. [Google Scholar] [CrossRef]
- Atkins, N.S.; Conway, D.J.; Lindo, J.F.; Bailey, J.W.; Bundy, D.A. L3 antigen-specific antibody isotype responses in human strongyloidiasis: Correlations with larval output. Parasite. Immunol. 1999, 21, 517–526. [Google Scholar] [CrossRef]
- Sudre, A.P.; Siqueira, R.C.; Barreto, M.G.; Peralta, R.H.; Macedo, H.W.; Peralta, J.M. Identification of a 26-kDa protein fraction as an important antigen for application in the immunodiagnosis of strongyloidiasis. Parasitol. Res. 2007, 101, 1117–1123. [Google Scholar] [CrossRef]
- Sykes, A.M.; McCarthy, J.S. A coproantigen diagnostic test for Strongyloides infection. PLoS. Negl. Trop. Dis. 2011, 5, e955. [Google Scholar] [CrossRef] [PubMed]
- Levenhagen, M.A.; Costa-Cruz, J.M. Update on immunologic and molecular diagnosis of human strongyloidiasis. Acta Trop. 2014, 135, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Eamudomkarn, C.; Sithithaworn, P.; Sithithaworn, J.; Kaewkes, S.; Sripa, B.; Itoh, M. Comparative evaluation of Strongyloides ratti and S. stercoralis larval antigen for diagnosis of strongyloidiasis in an endemic area of opisthorchiasis. Parasitol. Res. 2015, 114, 2543–2551. [Google Scholar] [CrossRef] [PubMed]
- Rodpai, R.; Intapan, P.M.; Thanchomnang, T.; Sanpool, O.; Janwan, P.; Laummaunwai, P.; Wongkham, C.; Insawang, T.; Maleewong, W. Strongyloides stercoralis diagnostic polypeptides for human strongyloidiasis and their proteomic analysis. Parasitol. Res. 2016, 115, 4007–4012. [Google Scholar] [CrossRef] [PubMed]
- Sadaow, L.; Sanpool, O.; Rodpai, R.; Boonroumkaew, P.; Maleewong, W.; Intapan, P.M. Development of immunochromatographic device as a point-of-care tool for serodiagnosis of human strongyloidiasis cases. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 465–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravi, V.; Ramachandran, S.; Thompson, R.W.; Andersen, J.F.; Neva, F.A. Characterization of a recombinant immunodiagnostic antigen (NIE) from Strongyloides stercoralis L3-stage larvae. Mol. Biochem. Parasitol. 2002, 125, 73–81. [Google Scholar] [CrossRef]
- Ramanathan, R.; Burbelo, P.D.; Groot, S.; Iadarola, M.J.; Neva, F.A.; Nutman, T.B. A luciferase immunoprecipitation systems assay enhances the sensitivity and specificity of diagnosis of Strongyloides stercoralis infection. J. Infect. Dis. 2008, 198, 444–451. [Google Scholar] [CrossRef] [Green Version]
- Rascoe, L.N.; Price, C.; Shin, S.H.; McAuliffe, I.; Priest, J.W.; Handali, S. Development of Ss-NIE-1 recombinant antigen based assays for immunodiagnosis of strongyloidiasis. PLoS Negl. Trop. Dis. 2015, 10, e0003694. [Google Scholar] [CrossRef] [Green Version]
- Arifin, N.; Yunus, M.H.; Nolan, T.J.; Lok, J.B.; Noordin, R. Identification and preliminary evaluation of a novel recombinant protein for serodiagnosis of strongyloidiasis. Am. J. Trop. Med. Hyg. 2018, 98, 1165–1170. [Google Scholar] [CrossRef] [Green Version]
- Koga, K.; Kasuya, S.; Khamboonruang, C.; Sukhavat, K.; Ieda, M.; Takatsuka, N.; Kita, K.; Ohtomo, H. A modified agar plate method for detection of Strongyloides stercoralis. Am. J. Trop. Med. Hyg. 1991, 45, 518–521. [Google Scholar] [CrossRef]
- Elkins, D.B.; Haswell-Elkins, M.; Anderson, R.M. The epidemiology and control of intestinal helminths in the Pulicat Lake region of Southern India. I. Study design and pre- and post-treatment observations on Ascaris lumbricoides infection. Trans. R. Soc. Trop. Med. Hyg. 1986, 80, 774–792. [Google Scholar] [CrossRef]
- Intapan, P.M.; Khotsri, P.; Kanpittaya, J.; Chotmongkol, V.; Maleewong, W.; Morakote, N. Evaluation of IgG4 and total IgG antibodies against cysticerci and peptide antigens for the diagnosis of human neurocysticercosis by ELISA. Asian. Pac. J. Allergy Immunol. 2008, 26, 237–244. [Google Scholar] [PubMed]
- Galen, R.S. Predictive value and efficiency of laboratory testing. Pediatr. Clin. N. Am. 1980, 27, 861–869. [Google Scholar] [CrossRef]
- Cohen, J.F.; Korevaar, D.A.; Altman, D.G.; Bruns, D.E.; Gatsonis, C.A.; Hooft, L.; Irwig, L.; Levine, D.; Reitsma, J.B.; de Vet, H.C.; et al. STARD 2015 guidelines for reporting diagnostic accuracy studies: Explanation and elaboration. BMJ Open 2016, 14, e012799. [Google Scholar] [CrossRef] [PubMed]
- Porto, A.F.; Neva, F.A.; Bittencourt, H.; Lisboa, W.; Thompson, R.; Alcântara, L.; Carvalho, E.M. HTLV-1 decreases Th2 type of immune response in patients with strongyloidiasis. Parasite. Immunol. 2001, 23, 503–507. [Google Scholar] [CrossRef]
- Iriemenam, N.C.; Sanyaolu, A.O.; Oyibo, W.A.; Fagbenro-Beyioku, A.F. Strongyloides stercoralis and the immune response. Parasitol. Int. 2010, 59, 9–14. [Google Scholar] [CrossRef]
- Arifin, N.; Hanafiah, K.M.; Ahmad, H.; Noordin, R. Serodiagnosis and early detection of Strongyloides stercoralis infection. J. Microbiol. Immunol. Infect. 2019, 52, 371–378. [Google Scholar] [CrossRef]
- Hamano, H.; Kawa, S.; Horiuchi, A.; Unno, H.; Furuya, N.; Akamatsu, T.; Fukushima, M.; Nikaido, T.; Nakayama, K.; Usuda, N.; et al. High serum IgG4 concentrations in patients with sclerosing pancreatitis. N. Engl. J. Med. 2001, 344, 732–738. [Google Scholar] [CrossRef]
- Norsyahida, A.; Riazi, M.; Sadjjadi, S.M.; Muhammad Hafiznur, Y.; Low, H.C.; Zeehaida, M.; Noordin, R. Laboratory detection of strongyloidiasis: IgG-, IgG4- and IgE-ELISAs and cross-reactivity with lymphatic filariasis. Parasite Immunol. 2013, 35, 174–179. [Google Scholar] [CrossRef]
- Hagan, P.; Blumenthal, U.J.; Dunn, D.; Simpson, A.J.; Wilkins, H.A. Human IgE, IgG4 and resistance to reinfection with Schistosoma haematobium. Nature 1991, 17, 243–245. [Google Scholar] [CrossRef]
- Demeure, C.E.; Rihet, P.; Abel, L.; Ouattara, M.; Bourgois, A.; Dessein, A.J. Resistance to Schistosoma mansoni in humans: Influence of the IgE/IgG4 balance and IgG2 in immunity to reinfection after chemotherapy. J. Infect. Dis. 1993, 168, 1000–1008. [Google Scholar] [CrossRef]
- Yunus, M.H.; Arifin, N.; Balachandra, D.; Anuar, N.S.; Noordin, R. Lateral flow dipstick test for serodiagnosis of strongyloidiasis. Am. J. Trop. Med. Hyg. 2019, 101, 432–435. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Types | Number of Positive/Total Number of rSsIR-Based IgG ICT Kits | Number of Positive/Total Number of rSsIR-Based IgG4 ICT Kits | |
|---|---|---|---|
| Proven strongyloidiasis | 55/60 | 47/60 | |
| Healthy controls | 0/30 | 0/30 | |
| Other infections | |||
| Giardiasis | 2/5 | 2/5 | |
| Amoebiasis | 2/5 | 1/5 | |
| Blastocystosis | 2/5 | 1/5 | |
| Hookworm infections | 1/5 | 2/5 | |
| Ascariasis | 0/5 | 0/5 | |
| Trichuriasis | 0/5 | 0/5 | |
| Trichinellosis | 2/5 | 2/5 | |
| Angiostrongyliasis | 1/5 | 2/5 | |
| Gnathostomiasis | 1/5 | 0/5 | |
| Capillariasis | 1/5 | 1/5 | |
| Opisthorchiasis | 0/5 | 0/5 | |
| Fascioliasis | 1/5 | 2/5 | |
| Taeniasis | 1/5 | 0/5 | |
| Cysticercosis | 1/5 | 0/5 | |
| Sparganosis | 2/5 | 3/5 | |
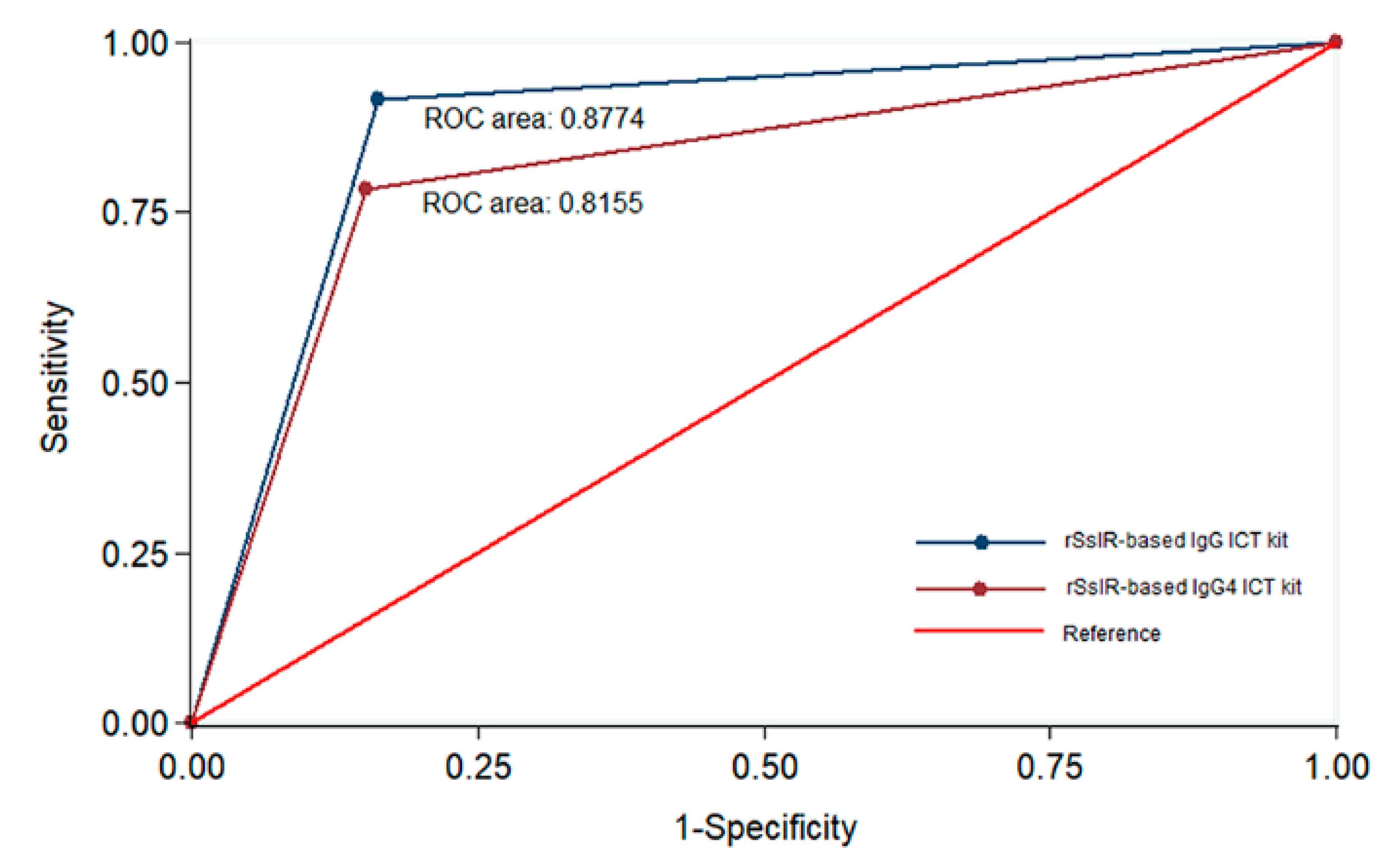
| Accuracy (%) [95% CI] | 86.7 [80.5–91.5] | 82.4 [75.7–87.9] | |
| Sensitivity (%) [95% CI] | 91.7 [81.6–97.2] | 78.3 [65.8–87.9] | |
| Specificity (%) [95% CI] | 83.8 [75.3–90.3] | 84.8 [76.4–91.0] | |
| Positive predictive value (%) [95% CI] | 76.4 [64.9–85.6] | 74.6 [62.1–84.7] | |
| Negative predictive value (%) [95% CI] | 94.6 [87.9–98.2] | 87.3 [79.2–93.0] | |
| Test Type and Results | rSsIR-Based IgG4 ICT Kit | ||
|---|---|---|---|
| rSsIR-Based IgG ICT Kit | Number of Positive | Number of Negative | Total |
| Number of Positive | 59 | 13 | 72 |
| Number of Negative | 4 | 89 | 93 |
| Total | 63 | 102 | 165 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boonroumkaew, P.; Sadaow, L.; Sanpool, O.; Rodpai, R.; Thanchomnang, T.; Phupiewkham, W.; Intapan, P.M.; Maleewong, W. Effectiveness of Strongyloides Recombinant IgG Immunoreactive Antigen in Detecting IgG and IgG4 Subclass Antibodies for Diagnosis of Human Strongyloidiasis Using Rapid Immunochromatographic Tests. Diagnostics 2020, 10, 615. https://doi.org/10.3390/diagnostics10090615
Boonroumkaew P, Sadaow L, Sanpool O, Rodpai R, Thanchomnang T, Phupiewkham W, Intapan PM, Maleewong W. Effectiveness of Strongyloides Recombinant IgG Immunoreactive Antigen in Detecting IgG and IgG4 Subclass Antibodies for Diagnosis of Human Strongyloidiasis Using Rapid Immunochromatographic Tests. Diagnostics. 2020; 10(9):615. https://doi.org/10.3390/diagnostics10090615
Chicago/Turabian StyleBoonroumkaew, Patcharaporn, Lakkhana Sadaow, Oranuch Sanpool, Rutchanee Rodpai, Tongjit Thanchomnang, Weeraya Phupiewkham, Pewpan M. Intapan, and Wanchai Maleewong. 2020. "Effectiveness of Strongyloides Recombinant IgG Immunoreactive Antigen in Detecting IgG and IgG4 Subclass Antibodies for Diagnosis of Human Strongyloidiasis Using Rapid Immunochromatographic Tests" Diagnostics 10, no. 9: 615. https://doi.org/10.3390/diagnostics10090615