Evaluation of FDG-PET/CT Use in Children with Suspected Infection or Inflammation

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. FDG-PET/CT Scanning Procedure
2.3. Data Sources
2.4. Diagnostic and Follow-Up Scans
2.5. Analysis
2.5.1. Diagnostic Accuracy and Reference Standard
2.5.2. Scan Consequence
2.5.3. Incidental Findings
2.5.4. Statistical Analysis
3. Results
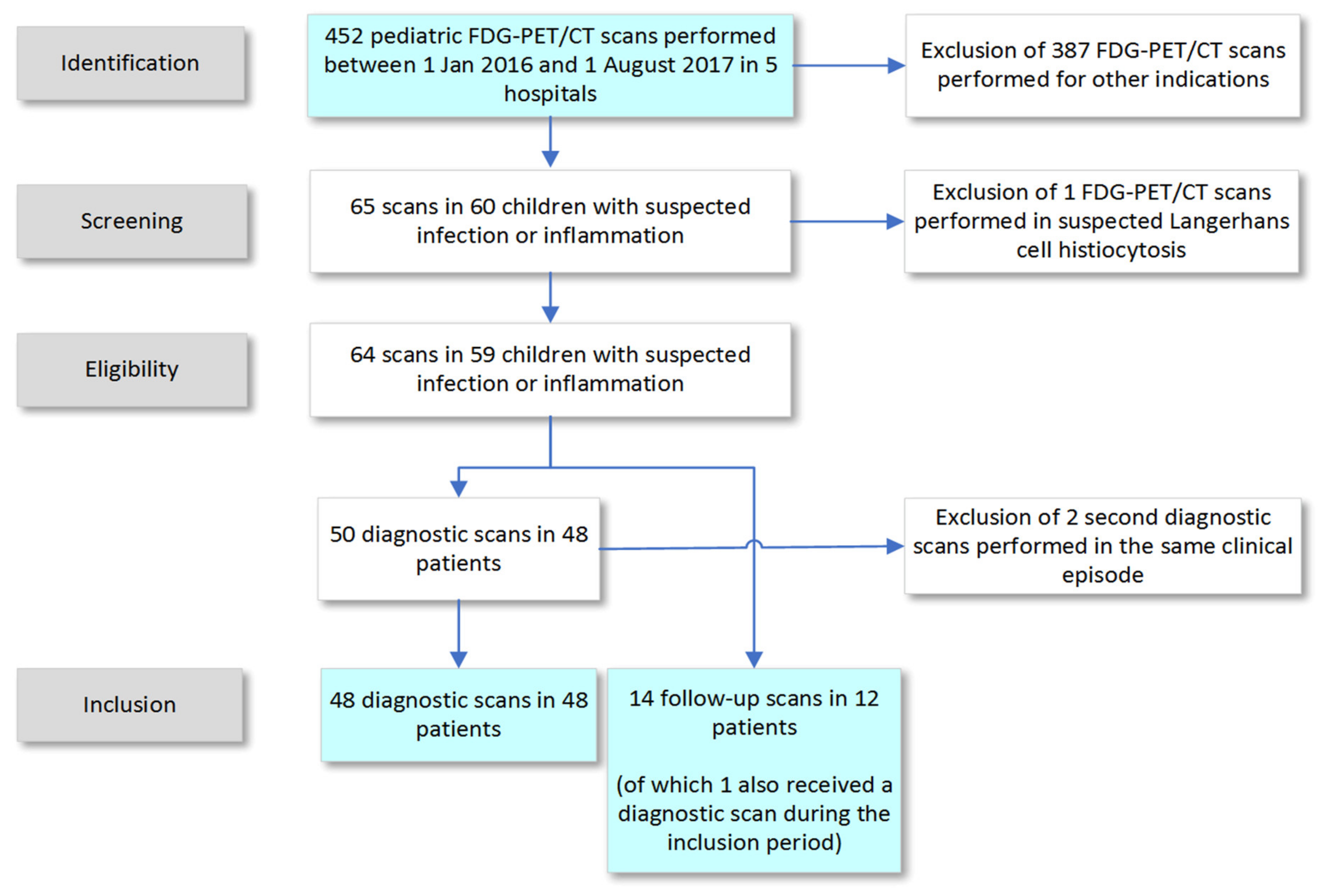
3.1. Selection Process
3.2. Diagnostic Scans
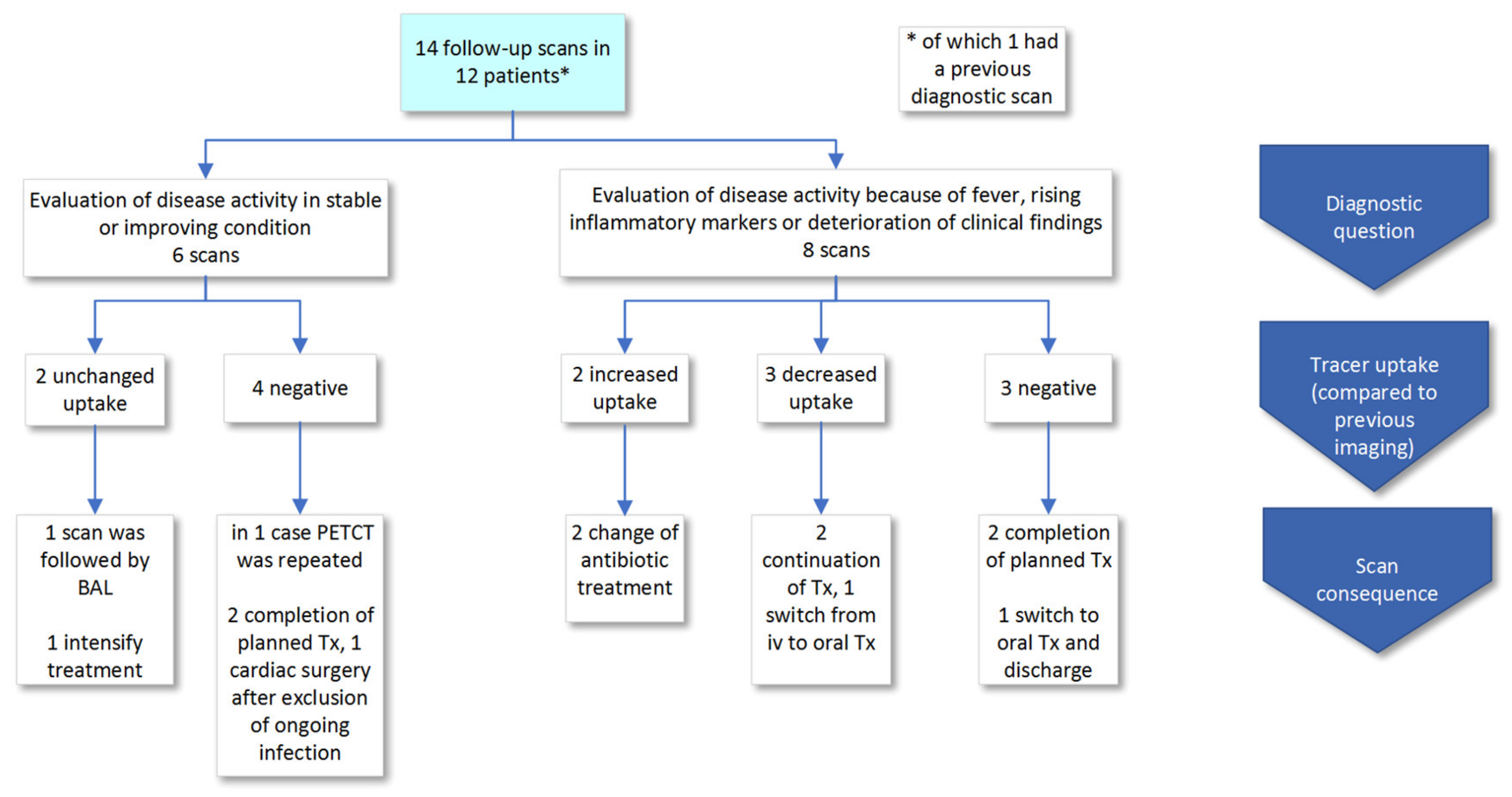
3.3. Follow-Up Scans
3.4. Relationship between CRP, Fever and Positive Scans
3.5. Incidental Findings
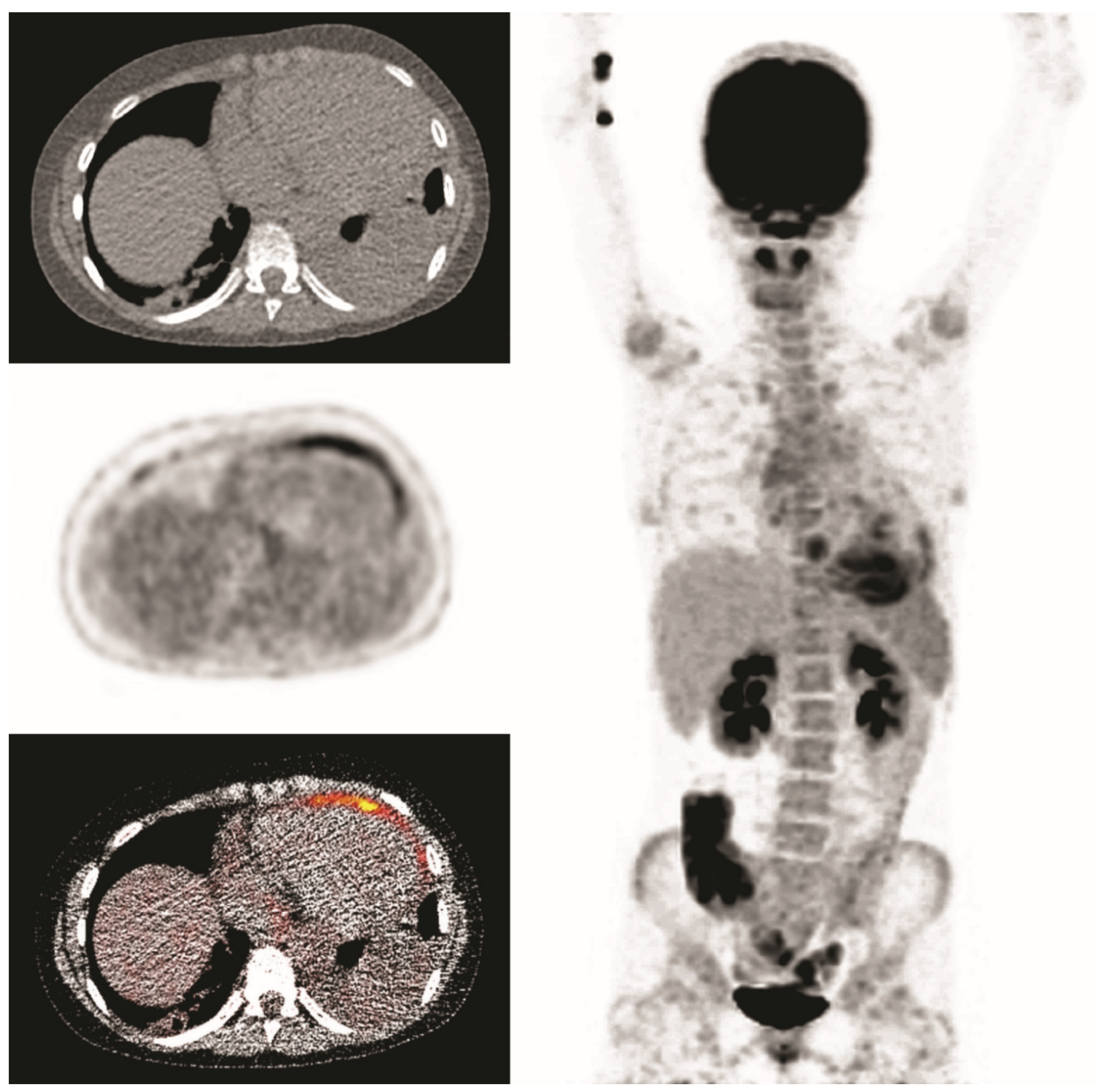
3.6. Clinical Examples
4. Discussion
5. Conclusions and Recommendation
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- EuroNet-Paediatric Hodgkin’s Lymphoma Group. Second International Inter-Group Study for Classical Hodgkin’s Lymphoma in Children and Adolescents, Imaging Manual. 2017. Available online: https://www.skion.nl/workspace/uploads/EuroNet-PHL-C2_Imaging_Manual_final3-0_2017-05-15.pdf (accessed on 15 August 2020).
- Vaidyanathan, S.; Patel, C.; Scarsbrook, A.; Chowdhury, F.U. FDG PET/CT in infection and inflammation—Current and emerging clinical applications. Clin. Radiol. 2015, 70, 787–800. [Google Scholar] [CrossRef] [PubMed]
- Parisi, M.T.; Otjen, J.P.; Stanescu, A.L.; Shulkin, B.L. Radionuclide Imaging of Infection and Inflammation in Children: A Review. Semin. Nucl. Med. 2018, 48, 148–165. [Google Scholar] [CrossRef] [PubMed]
- Bharucha, T.; Rutherford, A.; Skeoch, S.; Alavi, A.; Brown, M.; Galloway, J.; Miller, R.; Llewelyn, M.J.; Jenkins, N.; Lambourne, J.; et al. Diagnostic yield of FDG-PET/CT in fever of unknown origin: A systematic review, meta-analysis, and Delphi exercise. Clin. Radiol. 2017, 72, 764–771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, L.; Cheng, M.-F.; Jou, S.-T.; Ko, C.-L.; Huang, J.-Y.; Tzen, K.-Y.; Yen, R.-F. Search of Unknown Fever Focus Using PET in Critically Ill Children with Complicated Underlying Diseases. Pediatr. Crit. Care Med. 2016, 17, e58–e65. [Google Scholar] [CrossRef] [PubMed]
- Blokhuis, G.J.; Bleeker-Rovers, C.P.; Diender, M.G.; Oyen, W.J.; Draaisma, J.M.T.; De Geus-Oei, L.-F. Diagnostic value of FDG-PET/(CT) in children with fever of unknown origin and unexplained fever during immune suppression. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1916–1923. [Google Scholar] [CrossRef] [PubMed]
- Däbritz, J.; Jasper, N.; Wittkowski, H.; Löffler, M.; Weckesser, M.; Foell, D. Diagnostic value of 18F-FDG-PET and PET-CT in children with fever of unknown origin or unexplained signs of inflammation. Pediatr. Rheumatol. 2008, 6, P127. [Google Scholar] [CrossRef] [Green Version]
- Pijl, J.P.; Kwee, T.C.; Legger, G.; Peters, H.J.; Armbrust, W.; Schölvinck, E.; Glaudemans, A.W. Role of FDG-PET/CT in children with fever of unknown origin. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1596–1604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kouijzer, I.J.; Mulders-Manders, C.M.; Bleeker-Rovers, C.P.; Oyen, W.J. Fever of Unknown Origin: The Value of FDG-PET/CT. Semin. Nucl. Med. 2018, 48, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Adams, S.J.; Rakheja, R.; Bryce, R.; Babyn, P.S. Incidence and Economic Impact of Incidental Findings on 18F-FDG PET/CT Imaging. Can. Assoc. Radiol. J. 2018, 69, 63–70. [Google Scholar] [CrossRef] [PubMed]
- National Health Care Institute. Zorginstituut Nederland, Based on Registered Health Care Billings Provided by the Dutch Health Authority (NZa); National Health Care Institute: The Netherlands, 2019. [Google Scholar]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2014, 42, 328–354. [Google Scholar] [CrossRef] [PubMed]
- Dosage Card, version 5.7.2016; Medicine, E.A.o.N. Available online: https://www.eanm.org/publications/dosage-card/ (accessed on 15 August 2020).
- Boellaard, R.; Willemsen, A.T.; Arends, B.; Visser, E.P. EARL Procedure for Assessing PET/CT System Specific Patient FDG Activity Preparations for Quantitative FDG PET/CT Studies. Available online: http://earl.eanm.org/html/img/pool/EARL-procedure-for-optimizing-FDG-activity-for-quantitative-FDG-PET-studies_version_1_1.pdf (accessed on 15 August 2020).
- Abouzied, M.M.; Crawford, E.S.; Nabi, H.A. 18F-FDG imaging: Pitfalls and artifacts. J. Nucl. Med. Technol. 2005, 33, 145. [Google Scholar] [PubMed]
- Shammas, A.; Lim, R.; Charron, M. Pediatric FDG PET/CT: Physiologic Uptake, Normal Variants, and Benign Conditions1. Radiographics 2009, 29, 1467–1486. [Google Scholar] [CrossRef] [PubMed]
- Kouijzer, I.J.; Blokhuis, G.J.; Draaisma, J.M.T.; Oyen, W.J.; De Geus-Oei, L.-F.; Bleeker-Rovers, C.P. 18F-FDG PET/CT in Detecting Metastatic Infection in Children. Clin. Nucl. Med. 2016, 41, 278–281. [Google Scholar] [CrossRef] [PubMed]
- Schonau, V.; Vogel, K.; Englbrecht, M.; Wacker, J.; Schmidt, D.; Manger, B.; Kuwert, T.; Schett, G. The value of 18F-FDG-PET/CT in identifying the cause of fever of unknown origin (FUO) and inflammation of unknown origin (IUO): Data from a prospective study. Ann. Rheum. Dis. 2018, 77, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Manohar, K.; Mittal, B.R.; Jain, S.; Sharma, A.; Kalra, N.; Bhattacharya, A.; Varma, S. F-18 FDG-PET/CT in evaluation of patients with fever of unknown origin. Jpn. J. Radiol. 2013, 31, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, M.; Nihashi, T.; Gafter-Gvili, A.; García-Gómez, F.J.; Andres, E.; Blockmans, D.; Iwata, M.; Terasawa, T. Association of 18F-FDG PET or PET/CT results with spontaneous remission in classic fever of unknown origin. Medicine 2018, 97, e12909. [Google Scholar] [CrossRef] [PubMed]
- Ball, J.R.; Balogh, E.P. Improving Diagnosis in Health Care: Highlights of a Report from the National Academies of Sciences, Engineering, and Medicine. Ann. Intern. Med. 2015, 164, 59. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | % | Median (IQR) | |
|---|---|---|---|
| Characteristics | |||
| Patients | 59 | ||
| Age at first scan (yrs) | 12 (5–15) | ||
| Female | 37 | (63) | |
| No of FDG-PET/CT scans | 64 | ||
| diagnostic scans | 50 | (73) | |
| follow up scans | 14 | (27) | |
| >1 scan, No of patients | 4 | ||
| Amsterdam University Medical Center | 21 | (33) | |
| University Medical Center Utrecht | 17 | (27) | |
| Erasmus University Medical Center | 19 | (30) | |
| Leiden University Medical Center | 5 | (8) | |
| Alrijne Hospital Leiderdorp | 2 | (3) |
| n | % | Median (IQR) | |
|---|---|---|---|
| Diagnostic scans and patients | 48 | ||
| CRP in week before scan (mg/L) | 46 | (96) | 44 (9–120) |
| Fever > 38.3 in week before scan | 19 | (40) | |
| Preceding diagnostics | |||
| Serology (any lab test) | 48 | (100) | |
| Radiology | |||
| Chest X ray | 26 | (54) | |
| Other radiological examination | 14 | (29) | |
| Ultrasonography | 37 | (77) | |
| MRI | 17 | (35) | |
| CT | 11 | (23) | |
| Bone Scintigraphy | 1 | (2) | |
| Microbiology | |||
| Blood culture | 34 | (71) | |
| Urine culture | 15 | (31) | |
| Sputum/nose/throat culture | 12 | (25) | |
| Faeces culture/PCR testing | 13 | (27) | |
| Joint fluid culture | 2 | (4) | |
| Cerebrospinal fluid culture | 6 | (13) | |
| Cytology/histology | 12 | (25) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ropers, F.G.; van Mossevelde, R.M.P.; Bleeker-Rovers, C.P.; van Velden, F.H.P.; van Assema, D.M.E.; Adam, J.A.; Lam, M.G.E.H.; Tolboom, N.; Dekkers, O.M.; de Geus-Oei, L.-F.; et al. Evaluation of FDG-PET/CT Use in Children with Suspected Infection or Inflammation. Diagnostics 2020, 10, 715. https://doi.org/10.3390/diagnostics10090715
Ropers FG, van Mossevelde RMP, Bleeker-Rovers CP, van Velden FHP, van Assema DME, Adam JA, Lam MGEH, Tolboom N, Dekkers OM, de Geus-Oei L-F, et al. Evaluation of FDG-PET/CT Use in Children with Suspected Infection or Inflammation. Diagnostics. 2020; 10(9):715. https://doi.org/10.3390/diagnostics10090715
Chicago/Turabian StyleRopers, Fabienne G., Robin M. P. van Mossevelde, Chantal P. Bleeker-Rovers, Floris H. P. van Velden, Danielle M. E. van Assema, Judit A. Adam, Marnix G. E. H. Lam, Nelleke Tolboom, Olaf M. Dekkers, Lioe-Fee de Geus-Oei, and et al. 2020. "Evaluation of FDG-PET/CT Use in Children with Suspected Infection or Inflammation" Diagnostics 10, no. 9: 715. https://doi.org/10.3390/diagnostics10090715
APA StyleRopers, F. G., van Mossevelde, R. M. P., Bleeker-Rovers, C. P., van Velden, F. H. P., van Assema, D. M. E., Adam, J. A., Lam, M. G. E. H., Tolboom, N., Dekkers, O. M., de Geus-Oei, L.-F., & Frings, V. (2020). Evaluation of FDG-PET/CT Use in Children with Suspected Infection or Inflammation. Diagnostics, 10(9), 715. https://doi.org/10.3390/diagnostics10090715