Salivary Alpha-Amylase in Experimentally-Induced Muscle Pain


Abstract
:1. Introduction
2. Methods and Materials
2.1. Participants
2.2. Study Design
2.3. Saliva Collection
2.4. Salivary Alpha-Amylase
2.5. Statistics
3. Results
3.1. Data Overview
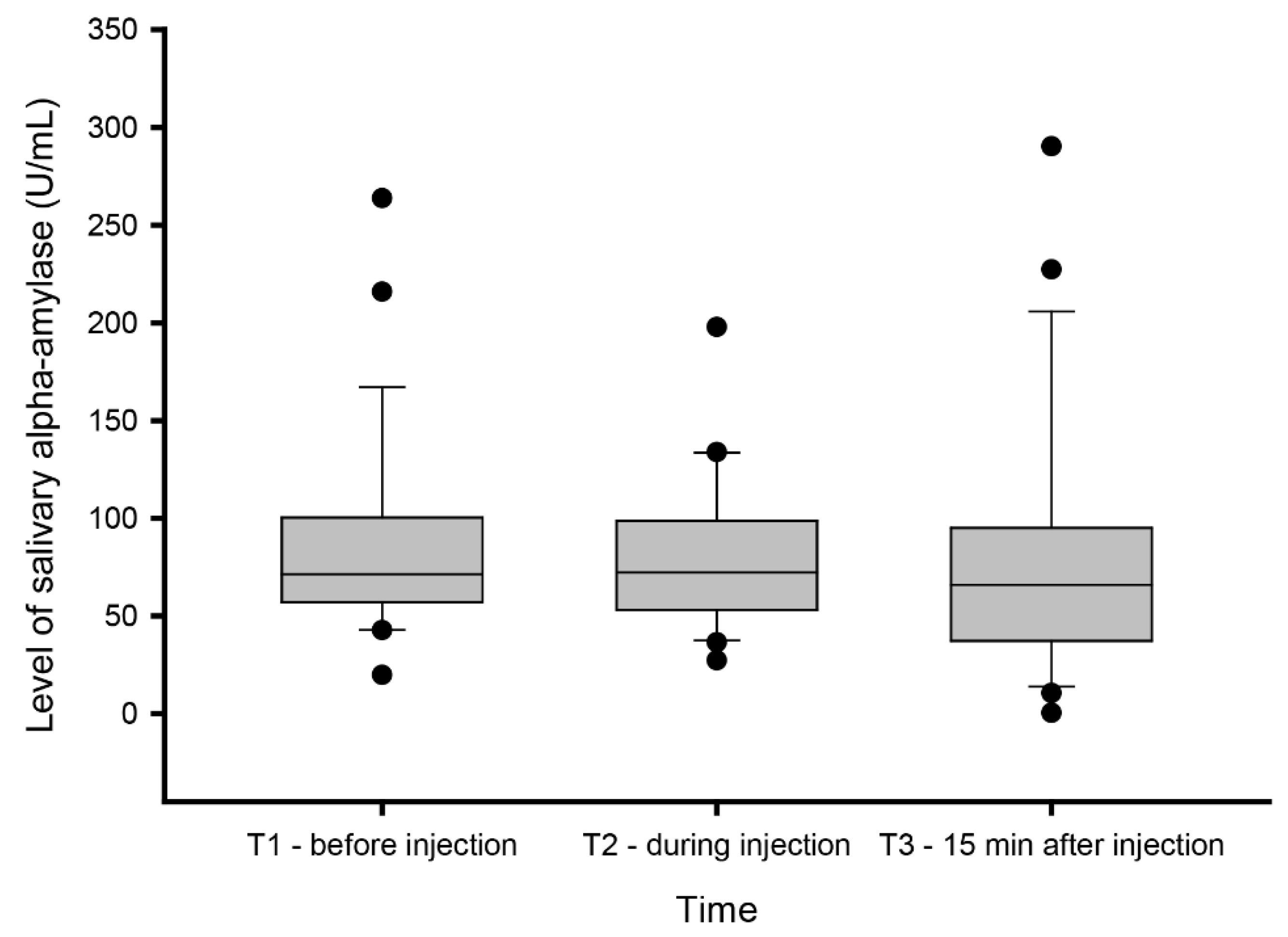
3.2. Changes in Salivary Alpha-Amylase Levels
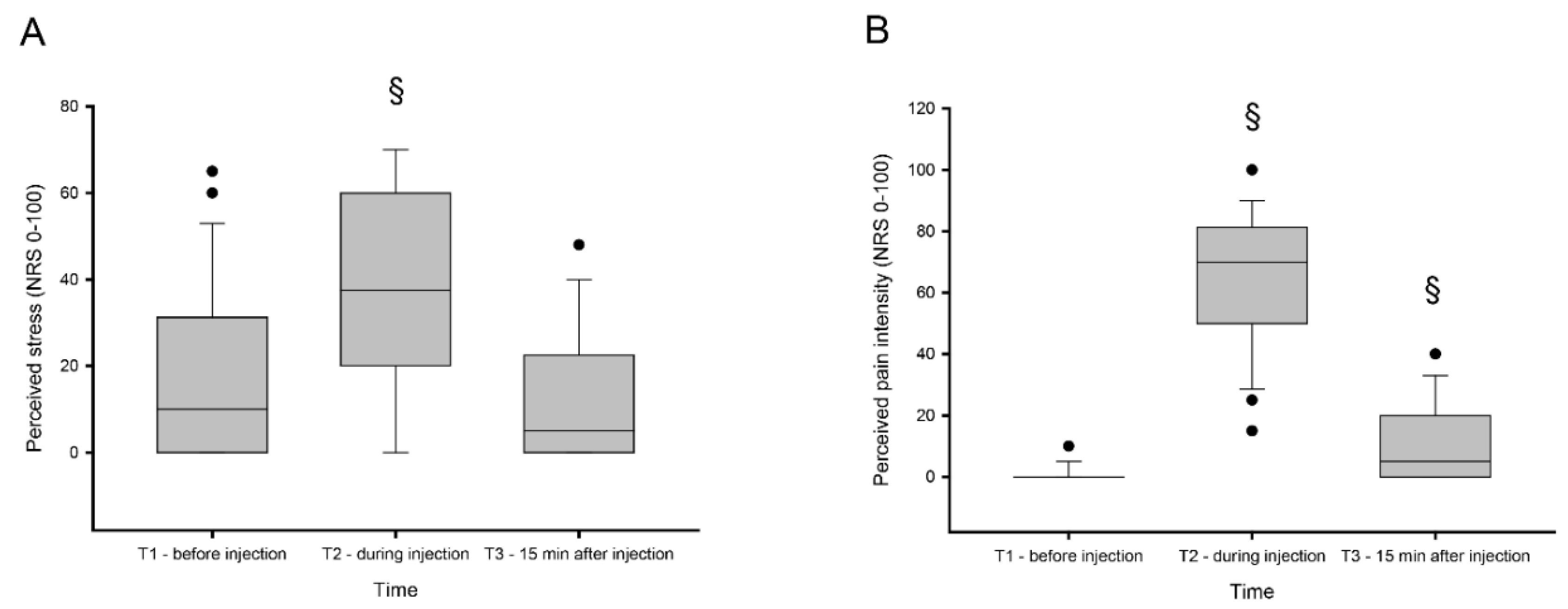
3.3. Changes in Perceived Stress and Pain Level
3.4. Correlation Analysis
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Schumacher, S.; Kirschbaum, C.; Fydrich, T.; Ströhle, A. Is salivary alpha-amylase an indicator of autonomic nervous system dysregulations in mental disorders?—A review of preliminary findings and the interactions with cortisol. Psychoneuroendocrinology 2013, 38, 729–743. [Google Scholar] [CrossRef]
- Fabian, T.K.; Hermann, P.; Beck, A.; Fejerdy, P.; Fabian, G. Salivary defense proteins: Their network and role in innate and acquired oral immunity. Int. J. Mol. Sci. 2012, 13, 4295–4320. [Google Scholar] [CrossRef]
- Nater, U.M.; Rohleder, N.; Gaab, J.; Berger, S.; Jud, A.; Kirschbaum, C.; Ehlert, U. Human salivary alpha-amylase reactivity in a psychosocial stress paradigm. Int. J. Psychophys. 2005, 55, 333–342. [Google Scholar] [CrossRef]
- Pedersen, A.M.; Bardow, A.; Jensen, S.B.; Nauntofte, B. Saliva and gastrointestinal functions of taste, mastication, swallowing and digestion. Oral Dis. 2002, 8, 117–129. [Google Scholar] [CrossRef]
- Silva Andrade, A.; Marcon Szymanski, M.; Hashizume, L.N.; Santos Mundstock, K.; Ferraz Goularte, J.; Hauber Gameiro, G. Evaluation of stress biomarkers and electrolytes in saliva of patients undergoing fixed orthodontic treatment. Miner. Stomatol. 2018, 67, 172–178. [Google Scholar]
- Kobayashi, F.Y.; Gavião, M.B.D.; Marquezin, M.C.S.; Fonseca, F.L.A.; Montes, A.B.M.; Barbosa, T.S.; Castelo, P.M. Salivary stress biomarkers and anxiety symptoms in children with and without temporomandibular disorders. Braz. Oral Res. 2017, 31, e78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wittwer, A.; Krummenacher, P.; La Marca, R.; Ehlert, U.; Folkers, G. Salivary Alpha-Amylase Correlates with Subjective Heat Pain Perception. Pain Med. (MaldenMass) 2016, 17, 1131–1136. [Google Scholar] [CrossRef] [Green Version]
- Campos, M.J.; Raposo, N.R.; Ferreira, A.P.; Vitral, R.W. Salivary alpha-amylase activity: A possible indicator of pain-induced stress in orthodontic patients. Pain Med. (MaldenMass) 2011, 12, 1162–1166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nater, U.M.; Rohleder, N. Salivary alpha-amylase as a non-invasive biomarker for the sympathetic nervous system: Current state of research. Psychoneuroendocrinology 2009, 34, 486–496. [Google Scholar] [CrossRef] [PubMed]
- Gilman, S.C.; Fischer, G.J.; Biersner, R.J.; Thornton, R.D.; Miller, D.A. Human parotid alpha-amylase secretion as a function of chronic hyperbaric exposure. Undersea Biomed. Res. 1979, 6, 303–307. [Google Scholar]
- Wan, C.; Couture-Lalande, M.E.; Narain, T.A.; Lebel, S.; Bielajew, C. Salivary Alpha-Amylase Reactivity in Breast Cancer Survivors. Int. J. Environ. Res. Public Health 2016, 13, 353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vineetha, R.; Pai, K.M.; Vengal, M.; Gopalakrishna, K.; Narayanakurup, D. Usefulness of salivary alpha amylase as a biomarker of chronic stress and stress related oral mucosal changes—A pilot study. J. Clin. Exp. Dent. 2014, 6, e132–e137. [Google Scholar] [CrossRef] [Green Version]
- Granger, D.A.; Kivlighan, K.T.; el-Sheikh, M.; Gordis, E.B.; Stroud, L.R. Salivary alpha-amylase in biobehavioral research: Recent developments and applications. Ann. N. Y. Acad. Sci. 2007, 1098, 122–144. [Google Scholar] [CrossRef] [PubMed]
- Van Stegeren, A.; Rohleder, N.; Everaerd, W.; Wolf, O.T. Salivary alpha amylase as marker for adrenergic activity during stress: Effect of betablockade. Psychoneuroendocrinology 2006, 31, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Noto, Y.; Sato, T.; Kudo, M.; Kurata, K.; Hirota, K. The relationship between salivary biomarkers and state-trait anxiety inventory score under mental arithmetic stress: A pilot study. Anesth. Anal. 2005, 101, 1873–1876. [Google Scholar] [CrossRef]
- Takai, N.; Yamaguchi, M.; Aragaki, T.; Eto, K.; Uchihashi, K.; Nishikawa, Y. Effect of psychological stress on the salivary cortisol and amylase levels in healthy young adults. Arch. Oral Biol. 2004, 49, 963–968. [Google Scholar] [CrossRef]
- Bosch, J.A.; de Geus, E.J.; Veerman, E.C.; Hoogstraten, J.; Nieuw Amerongen, A.V. Innate secretory immunity in response to laboratory stressors that evoke distinct patterns of cardiac autonomic activity. Psycho. Med. 2003, 65, 245–258. [Google Scholar] [CrossRef]
- Fischer, S.; Doerr, J.M.; Strahler, J.; Mewes, R.; Thieme, K.; Nater, U.M. Stress exacerbates pain in the everyday lives of women with fibromyalgia syndrome—The role of cortisol and alpha-amylase. Psychoneuroendocrinology 2016, 63, 68–77. [Google Scholar] [CrossRef]
- Laurent, H.K.; Laurent, S.M.; Granger, D.A. Salivary nerve growth factor reactivity to acute psychosocial stress: A new frontier for stress research. Psycho. Med. 2013, 75, 744–750. [Google Scholar] [CrossRef]
- Ahmadi-Motamayel, F.; Shahriari, S.; Goodarzi, M.T.; Moghimbeigi, A.; Jazaeri, M.; Babaei, P. The relationship between the level of salivary alpha amylase activity and pain severity in patients with symptomatic irreversible pulpitis. Restor. Dent. Endod. 2013, 38, 141–145. [Google Scholar] [CrossRef]
- Bugdayci, G.; Yildiz, S.; Altunrende, B.; Yildiz, N.; Alkoy, S. Salivary alpha amylase activity in migraine patients. Auto. Neurosci. 2010, 155, 121–124. [Google Scholar] [CrossRef] [PubMed]
- Arai, Y.C.; Matsubara, T.; Shimo, K.; Osuga, T.; Ushida, T.; Suzuki, C.; Ohta, A.; Tohyama, Y.; Nishida, K.; Arakawa, M. Small correlation between salivary alpha-amylase activity and pain intensity in patients with cancer pain. Acta Anaesthesiol. Scand. 2009, 53, 408. [Google Scholar] [CrossRef] [PubMed]
- Shirasaki, S.; Fujii, H.; Takahashi, M.; Sato, T.; Ebina, M.; Noto, Y.; Hirota, K. Correlation between salivary alpha-amylase activity and pain scale in patients with chronic pain. Reg. Anesth. Pain Med. 2007, 32, 120–123. [Google Scholar] [CrossRef] [PubMed]
- Van Stegeren, A.H.; Wolf, O.T.; Kindt, M. Salivary alpha amylase and cortisol responses to different stress tasks: Impact of sex. Int. J. Psychophysiol. 2008, 69, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Jasim, H.; Carlsson, A.; Hedenberg-Magnusson, B.; Ghafouri, B.; Ernberg, M. Saliva as a medium to detect and measure biomarkers related to pain. Sci. Rep. 2018, 8, 3220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jasim, H.; Ghafouri, B.; Carlsson, A.; Hedenberg-Magnusson, B.; Ernberg, M. Daytime changes of salivary biomarkers involved in pain. J. Oral Rehabil. 2020, in press. [Google Scholar] [CrossRef] [Green Version]
- Jasim, H.; Olausson, P.; Hedenberg-Magnusson, B.; Ernberg, M.; Ghafouri, B. The proteomic profile of whole and glandular saliva in healthy pain-free subjects. Sci. Rep. 2016, 6, 39073. [Google Scholar] [CrossRef]
- Balodis, I.M.; Wynne-Edwards, K.E.; Olmstead, M.C. The other side of the curve: Examining the relationship between pre-stressor physiological responses and stress reactivity. Psychoneuroendocrinology 2010, 35, 1363–1373. [Google Scholar] [CrossRef]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Groupdagger. J. Oral Fac. Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Maurer, D.M. Screening for depression. Am. Fam. Phys. 2012, 85, 139–144. [Google Scholar]
- Kroenke, K. Physical symptom disorder: A simpler diagnostic category for somatization-spectrum conditions. J. Psycho. Res. 2006, 60, 335–339. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Lowe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, N. The Borg Rating of Perceived Exertion (RPE) scale. Occup. Med. 2017, 67, 404–405. [Google Scholar] [CrossRef] [Green Version]
- Graven-Nielsen, T.; Arendt-Nielsen, L. Induction and assessment of muscle pain, referred pain, and muscular hyperalgesia. Curr. Pain Headache Rep. 2003, 7, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Al Sayegh, S.; Borgwardt, A.; Svensson, K.G.; Kumar, A.; Grigoriadis, A.; Christidis, N. Effects of Chronic and Experimental Acute Masseter Pain on Precision Biting Behavior in Humans. Front. Physiol. 2019, 10, 1369. [Google Scholar] [CrossRef]
- Louca, S.; Christidis, N.; Ghafouri, B.; Gerdle, B.; Svensson, P.; List, T.; Ernberg, M. Serotonin, glutamate and glycerol are released after the injection of hypertonic saline into human masseter muscles—A microdialysis study. J. Headache Pain 2014, 15, 89. [Google Scholar] [CrossRef] [Green Version]
- Christidis, N.; Ioannidou, K.; Milosevic, M.; Segerdahl, M.; Ernberg, M. Changes of hypertonic saline-induced masseter muscle pain characteristics, by an infusion of the serotonin receptor type 3 antagonist granisetron. J. Pain 2008, 9, 892–901. [Google Scholar] [CrossRef]
- Patchev, V.K.; Patchev, A.V. Experimental models of stress. Dialogues Clin. Neurosci. 2006, 8, 417–432. [Google Scholar]
- Freiman, S.V.; Onufriev, M.V.; Stepanichev, M.Y.; Moiseeva, Y.V.; Lazareva, N.A.; Gulyaeva, N.V. The stress effects of a single injection of isotonic saline solution: Systemic (blood) and central (frontal cortex and dorsal and ventral hippocampus). Neurochem. J. 2016, 10, 115–119. [Google Scholar] [CrossRef]
- Graven-Nielsen, T.; Arendt-Nielsen, L.; Mense, S. Fundamentals of musculoskeletal pain; IASP Press: Seattle, WA, USA, 2008. [Google Scholar]
- Feine, J.S. Treating chronic pain: How do we measure success? New York State Dent. J. 2000, 66, 34–38. [Google Scholar]
- Ohrbach, R.; Dworkin, S.F. Five-year outcomes in TMD: Relationship of changes in pain to changes in physical and psychological variables. Pain 1998, 74, 315–326. [Google Scholar] [CrossRef]
- Slade, G.D.; Ohrbach, R.; Greenspan, J.D.; Fillingim, R.B.; Bair, E.; Sanders, A.E.; Dubner, R.; Diatchenko, L.; Meloto, C.B.; Smith, S.; et al. Painful Temporomandibular Disorder: Decade of Discovery from OPPERA Studies. J. Dent. Res. 2016, 95, 1084–1092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schultz, J.; Uddin, Z.; Singh, G.; Howlader, M.M.R. Glutamate sensing in biofluids: Recent advances and research challenges of electrochemical sensors. Analyst 2020, 145, 321–347. [Google Scholar] [CrossRef] [PubMed]
- Ernberg, M. Masticatory Muscle Pain Biomarkers. In Orofacial Pain Biomarkers; Goulet, J., Velly, A., Eds.; Springer: Berlin/Heidelberg, Germany, 2017; pp. 79–93. [Google Scholar]
- Gerdle, B.; Ghafouri, B.; Ernberg, M.; Larsson, B. Chronic musculoskeletal pain: Review of mechanisms and biochemical biomarkers as assessed by the microdialysis technique. J. Pain Res. 2014, 7, 313–326. [Google Scholar] [CrossRef] [Green Version]
- Rudy, T.E.; Turk, D.C.; Kubinski, J.A.; Zaki, H.S. Differential treatment responses of TMD patients as a function of psychological characteristics. Pain 1995, 61, 103–112. [Google Scholar] [CrossRef]
- Suvinen, T.I.; Reade, P.C.; Hanes, K.R.; Kononen, M.; Kemppainen, P. Temporomandibular disorder subtypes according to self-reported physical and psychosocial variables in female patients: A re-evaluation. J. Oral Rehabil. 2005, 32, 166–173. [Google Scholar] [CrossRef]
- Vlaeyen, J.W.; Morley, S. Cognitive-behavioral treatments for chronic pain: What works for whom? Clin. J. Pain 2005, 21, 1–8. [Google Scholar] [CrossRef]
- Villemure, C.; Bushnell, C.M. Cognitive modulation of pain: How do attention and emotion influence pain processing? Pain 2002, 95, 195–199. [Google Scholar] [CrossRef]
- Bushnell, M.C.; Duncan, G.H.; Hofbauer, R.K.; Ha, B.; Chen, J.I.; Carrier, B. Pain perception: Is there a role for primary somatosensory cortex? Proc. Natl. Acad. Sci. USA 1999, 96, 7705–7709. [Google Scholar] [CrossRef] [Green Version]
- Rode, S.; Salkovskis, P.M.; Jack, T. An experimental study of attention, labelling and memory in people suffering from chronic pain. Pain 2001, 94, 193–203. [Google Scholar] [CrossRef]
- Haythornthwaite, J.A.; Benrud-Larson, L.M. Psychological aspects of neuropathic pain. Clin. J. Pain 2000, 16 (Suppl. 2), S101–S105. [Google Scholar] [CrossRef] [PubMed]
- Meagher, M.W.; Arnau, R.C.; Rhudy, J.L. Pain and emotion: Effects of affective picture modulation. Psychosom. Med. 2001, 63, 79–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keogh, E.; Ellery, D.; Hunt, C.; Hannent, I. Selective attentional bias for pain-related stimuli amongst pain fearful individuals. Pain 2001, 91, 91–100. [Google Scholar] [CrossRef]
- Fillingim, R.B. Sex, gender, and pain: Women and men really are different. Curr. Rev. Pain 2000, 4, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Hashmi, J.A.; Davis, K.D. Deconstructing sex differences in pain sensitivity. Pain 2014, 155, 10–13. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Males | Females | Statistics |
|---|---|---|---|
| Number of participants | 13 | 13 | |
| Age (years) | 23.7 ± 2.7 | 23.8 ± 2.8 | Z = 0.26; p = 0.80 |
| Baseline pain (NRS) | 0 (0) | 0 (0) | Z = 0.31; p = 0.76 |
| Baseline stress (NRS) | 0 (20) | 15 (38) | Z = 1.64; p = 0.09 |
| PHQ-9 Score (0–27) | 3 (3) | 3 (6) | Z = −0.01; p = 0.94 |
| PHQ-15 Score (0–30) | 2 (3) | 3 (3) | Z = 1.44; p = 0.15 |
| STAI-STAIT | 47 (7) | 46 /7) | Z = −0.28; p = 0.78 |
| STAI-TRAIT | 46 (6) | 46 (8) | Z = −0.36; p = 0.72 |
| RPE (0–10) | 2 (2) | 2 (1) | Z = 1.38; p = 0.17 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Christidis, N.; Baghernejad, P.; Deyhim, A.; Jasim, H. Salivary Alpha-Amylase in Experimentally-Induced Muscle Pain. Diagnostics 2020, 10, 722. https://doi.org/10.3390/diagnostics10090722
Christidis N, Baghernejad P, Deyhim A, Jasim H. Salivary Alpha-Amylase in Experimentally-Induced Muscle Pain. Diagnostics. 2020; 10(9):722. https://doi.org/10.3390/diagnostics10090722
Chicago/Turabian StyleChristidis, Nikolaos, Pegah Baghernejad, Aylin Deyhim, and Hajer Jasim. 2020. "Salivary Alpha-Amylase in Experimentally-Induced Muscle Pain" Diagnostics 10, no. 9: 722. https://doi.org/10.3390/diagnostics10090722
APA StyleChristidis, N., Baghernejad, P., Deyhim, A., & Jasim, H. (2020). Salivary Alpha-Amylase in Experimentally-Induced Muscle Pain. Diagnostics, 10(9), 722. https://doi.org/10.3390/diagnostics10090722