Intraoperative Perfusion Assessment in Enhanced Reality Using Quantitative Optical Imaging: An Experimental Study in a Pancreatic Partial Ischemia Model †


 , , , , ,
, , , , ,  ,
,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animal Characteristics
2.2. Endovascular Pancreatic Embolization and Surgical Procedure
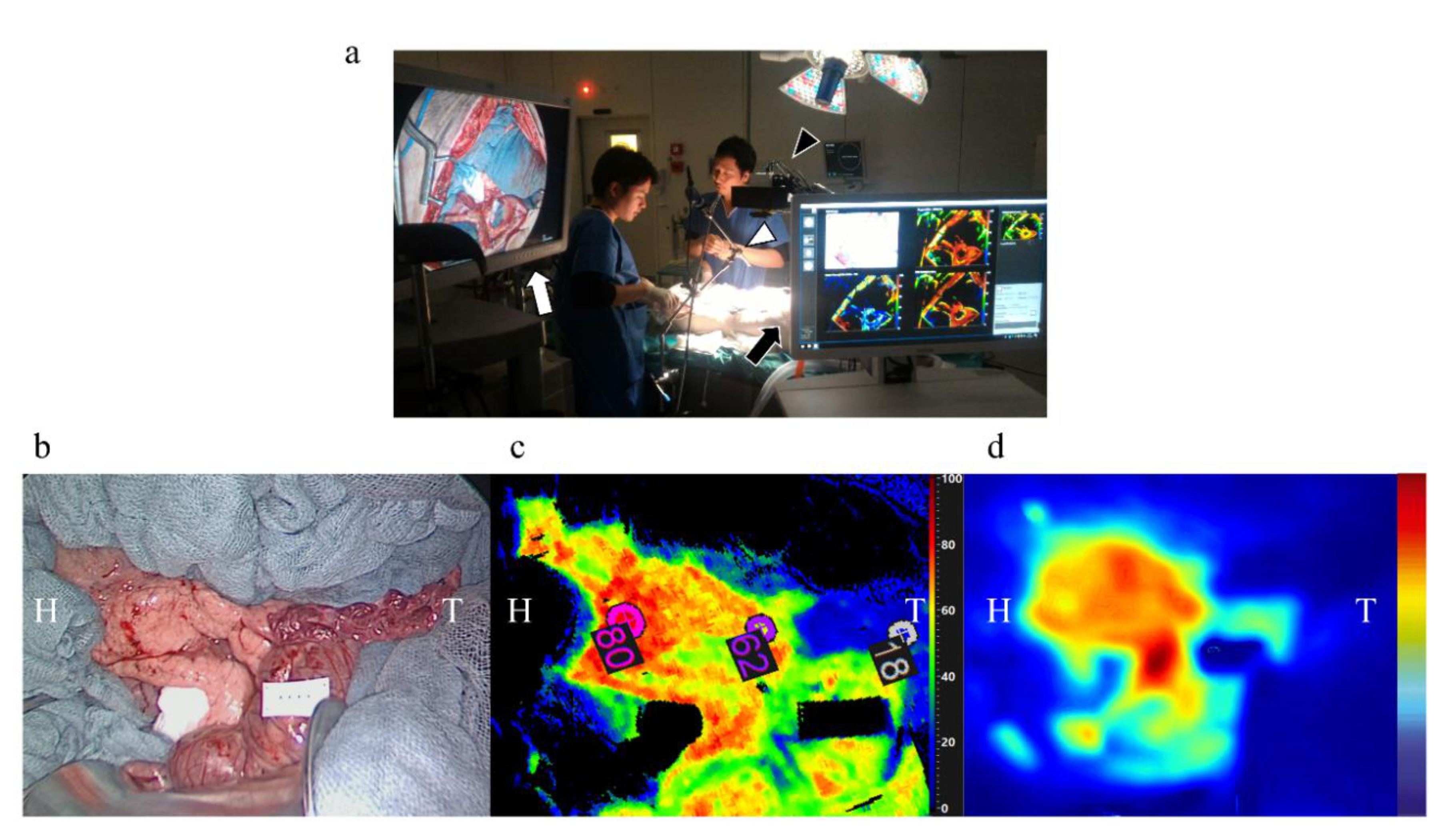
2.3. Quantitative Perfusion Assessment Steps
2.4. FLER (Fluorescence-Based Enhanced Reality)
2.5. Image Warping
2.6. Confocal Laser Endomicroscopy (CLE)
2.7. Local Capillary Lactate (LCL) Measurement
2.8. Mitochondrial Respiratory Chain Assessment
2.9. Histology
2.10. Prediction of Local Capillary Lactates from the FLER-Slope and HSI-StO2
2.11. Sample Size Calculation
2.12. Statistical Analysis
3. Results
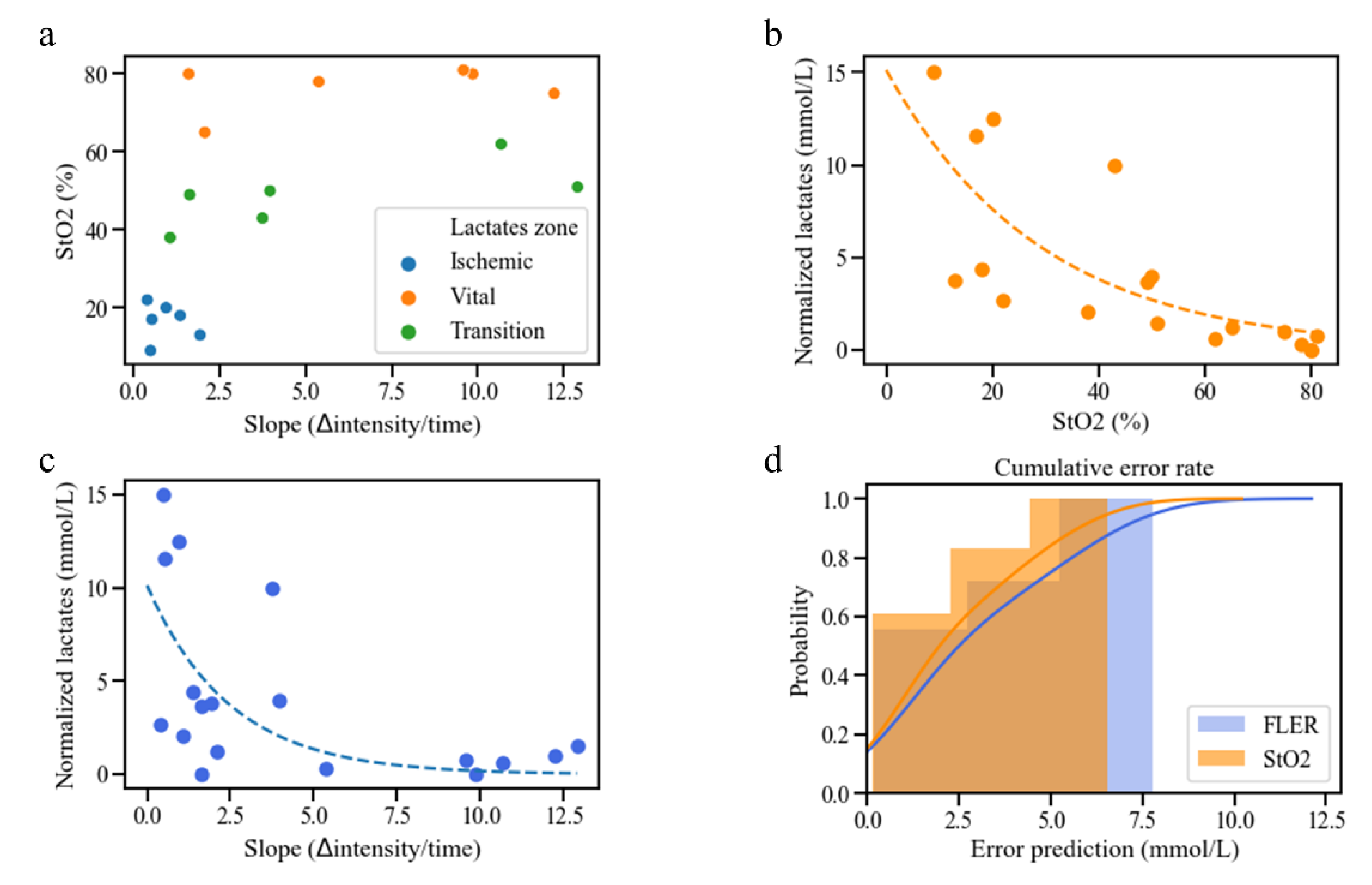
3.1. Correlation between HSI-StO2 and the FLER Slope
3.2. Local Capillary Lactate Values
3.3. Correlation between HSI, FLER and Local Capillary Lactate
3.4. Lactate Prediction Models Based on HSI-StO2 and the FLER Slope
- based on HSI-StO2:Predicted LCL = e−0.0343*HSI StO2+2.72 + Systemic Lactates
- based on the FLER slope:Predicted LCL = e−0.403*FLER slope+2.32 + Systemic Lactates
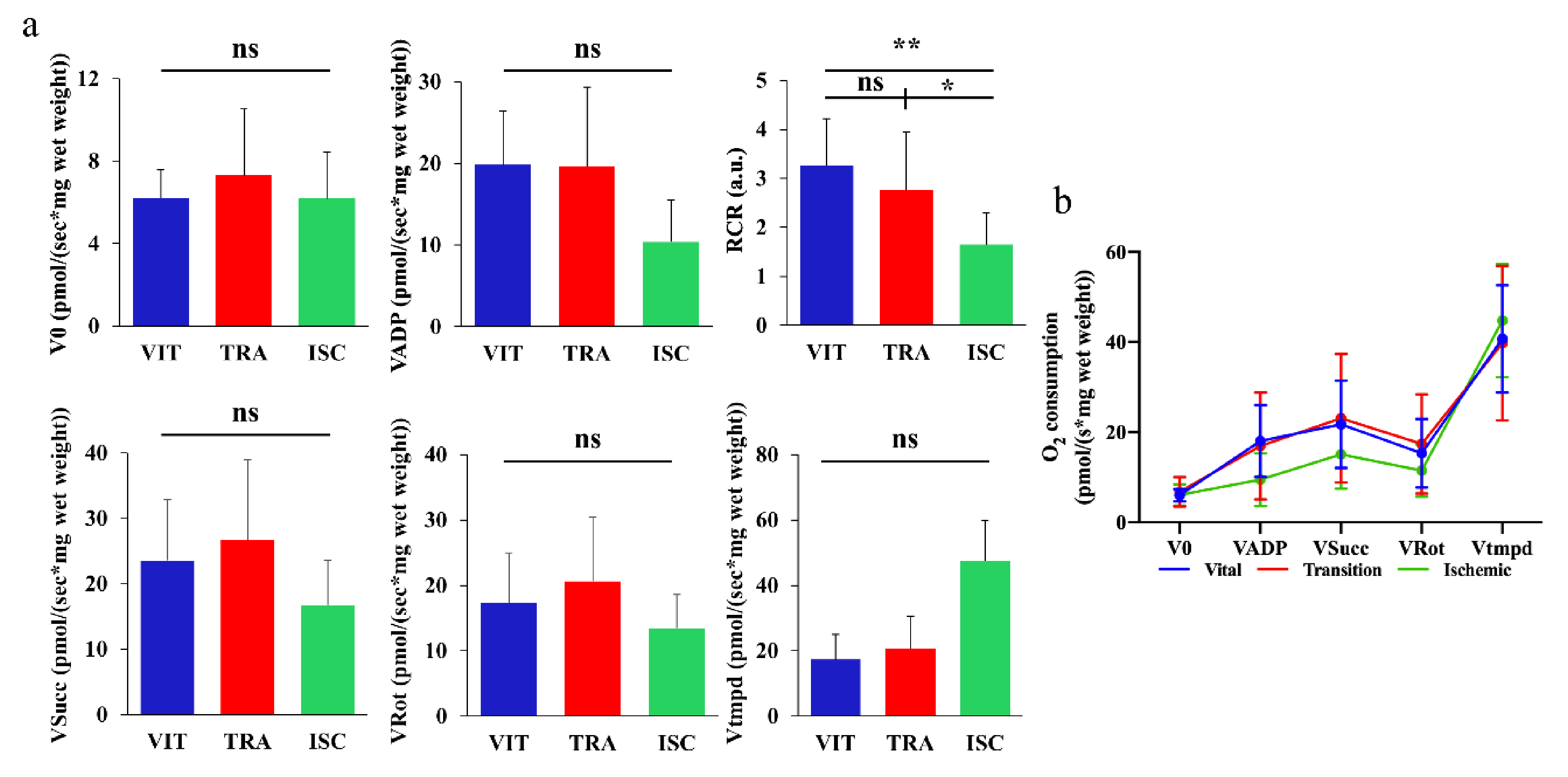
3.5. Mitochondrial Respiratory Chain Assessment
3.6. Confocal Laser Endomicroscopy (CLE) and Histological Findings
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harnoss, J.C.; Ulrich, A.B.; Harnoss, J.M.; Diener, M.K.; Büchler, M.W.; Welsch, T. Use and results of consensus definitions in pancreatic surgery: A systematic review. Surgery 2014, 155, 47–57. [Google Scholar] [CrossRef]
- Nagai, S.; Fujii, T.; Kodera, Y.; Kanda, M.; Sahin, T.T.; Kanzaki, A.; Hayashi, M.; Sugimoto, H.; Nomoto, S.; Takeda, S.; et al. Recurrence pattern and prognosis of pancreatic cancer after pancreatic fistula. Ann. Surg. Oncol. 2011, 18, 2329–2337. [Google Scholar] [CrossRef] [PubMed]
- Smits, F.J.; Molenaar, I.Q.; Besselink, M.G.; Rinkes, I.H.B.; van Eijck, C.H.; Busch, O.R.; van Santvoort, H.C. Early recognition of clinically relevant postoperative pancreatic fistula: A systematic review. HPB 2020, 22, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Mungroop, T.H.; van Rijssen, L.B.; van Klaveren, D.; Smits, F.J.; van Woerden, V.; Linnemann, R.J.; de Pastena, M.; Klomp-maker, S.; Marchegiani, G.; Ecker, B.L. Alternative fistula risk score for pancreatoduodenectomy (a-FRS): Design and international external validation. Ann. Surg. 2019, 269, 937–943. [Google Scholar] [CrossRef] [PubMed]
- Ratnayake, C.B.; Wells, C.I.; Kamarajah, S.K.; Loveday, B.; Sen, G.; French, J.J.; White, S.; Pandanaboyana, S. Critical appraisal of the techniques of pancreatic anastomosis following pancreaticoduodenectomy: A network meta-analysis. Int. J. Surg. 2019. [Google Scholar] [CrossRef] [PubMed]
- Strasberg, S.M.; Drebin, J.A.; Mokadam, N.A.; Green, D.W.; Jones, K.L.; Ehlers, J.P.; Linehan, D. Prospective trial of a blood supply-based technique of pancreaticojejunostomy: Effect on anastomotic failure in the Whipple procedure. J. Am. Coll. Surg. 2002, 194, 746–758. [Google Scholar] [CrossRef]
- Karliczek, A.; Harlaar, N.; Zeebregts, C.; Wiggers, T.; Baas, P.; Van Dam, G. Surgeons lack predictive accuracy for anastomotic leakage in gastrointestinal surgery. Int. J. Colorectal Dis. 2009, 24, 569–576. [Google Scholar] [CrossRef] [Green Version]
- Diana, M.; Noll, E.; Diemunsch, P.; Dallemagne, B.; Benahmed, M.A.; Agnus, V.; Soler, L.; Barry, B.; Namer, I.J.; Demartines, N. Enhanced-reality video fluorescence: A real-time assessment of intestinal viability. Ann. Surg. 2014, 259, 700–707. [Google Scholar] [CrossRef]
- Diana, M.; Agnus, V.; Halvax, P.; Liu, Y.Y.; Dallemagne, B.; Schlagowski, A.I.; Geny, B.; Diemunsch, P.; Lindner, V.; Marescaux, J. Intraoperative fluorescence-based enhanced reality laparoscopic real-time imaging to assess bowel perfusion at the anastomotic site in an experimental model. Br. J. Surg. 2015, 102, e169–e176. [Google Scholar] [CrossRef]
- Higuchi, K.; Nanashima, A.; Hiyoshi, M.; Imamura, N.; Yano, K.; Hamada, T.; Tsuchimochi, Y.; Wada, T.; Tsuchiya, K.; Kawano, F.; et al. Resected Intrahepatic Cholangiocarcinoma with Anaphylactic Shock from a Preoperative Liver Function Test before Hepatectomy. Case Rep. Gastroenterol. 2019, 13, 140–143. [Google Scholar] [CrossRef]
- Speich, R.; Saesseli, B.; Hoffmann, U.; Neftel, K.A.; Reichen, J. Anaphylactoid reactions after indocyanine-green administration. Ann. Intern. Med. 1988, 109, 345–346. [Google Scholar] [CrossRef] [PubMed]
- Barberio, M.; Maktabi, M.; Gockel, I.; Rayes, N.; Jansen-Winkeln, B.; Köhler, H.; Rabe, S.M.; Seidemann, L.; Takoh, J.P.; Diana, M. Hyperspectral based discrimination of thyroid and parathyroid during surgery. Curr. Dir. Biomed. Eng. 2018, 4, 399–402. [Google Scholar] [CrossRef]
- Lu, G.; Fei, B. Medical hyperspectral imaging: A review. J. Biomed. Opt. 2014, 19, 010901. [Google Scholar] [CrossRef] [PubMed]
- Akbari, H.; Uto, K.; Kosugi, Y.; Kojima, K.; Tanaka, N. Cancer detection using infrared hyperspectral imaging. Cancer Sci. 2011, 102, 852–857. [Google Scholar] [CrossRef] [PubMed]
- Chin, J.A.; Wang, E.C.; Kibbe, M.R. Evaluation of hyperspectral technology for assessing the presence and severity of peripheral artery disease. J. Vasc. Surg. 2011, 54, 1679–1688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortega, S.; Fabelo, H.; Iakovidis, D.K.; Koulaouzidis, A.; Callico, G.M. Use of Hyperspectral/Multispectral Imaging in Gastroenterology. Shedding Some Different Light into the Dark. J. Clin. Med. 2019, 8, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansen-Winkeln, B.; Holfert, N.; Köhler, H.; Moulla, Y.; Takoh, J.; Rabe, S.; Mehdorn, M.; Barberio, M.; Chalopin, C.; Neumuth, T. Determination of the transection margin during colorectal resection with hyperspectral imaging (HSI). Int. J. Colorectal Dis. 2019, 34, 731–739. [Google Scholar] [CrossRef] [PubMed]
- Köhler, H.; Jansen-Winkeln, B.; Maktabi, M.; Barberio, M.; Takoh, J.; Holfert, N.; Moulla, Y.; Niebisch, S.; Diana, M.; Neumuth, T.; et al. Evaluation of hyperspectral imaging (HSI) for the measurement of ischemic conditioning effects of the gastric conduit during esophagectomy. Surg. Endosc. 2019, 33, 3775–3782. [Google Scholar] [CrossRef] [Green Version]
- Barberio, M.; Longo, F.; Fiorillo, C.; Seeliger, B.; Mascagni, P.; Agnus, V.; Lindner, V.; Geny, B.; Charles, A.-L.; Gockel, I. HYPerspectral Enhanced Reality (HYPER): A physiology-based surgical guidance tool. Surg. Endosc. 2020, 34, 1736–1744. [Google Scholar] [CrossRef]
- Urade, T.; Felli, E.; Barberio, M.; Al-Taher, M.; Felli, E.; Goffin, L.; Agnus, V.; Ettorre, G.M.; Marescaux, J.; Mutter, D.; et al. Hyperspectral enhanced reality (HYPER) for anatomical liver resection. Surg. Endosc. 2020. [Google Scholar] [CrossRef]
- Barberio, M.; Felli, E.; Seyller, E.; Longo, F.; Chand, M.; Gockel, I.; Geny, B.; Swanström, L.; Marescaux, J.; Agnus, V. Quantitative fluorescence angiography versus hyperspectral imaging to assess bowel ischemia: A comparative study in enhanced reality. Surgery 2020, 168, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Diana, M.; Dallemagne, B.; Chung, H.; Nagao, Y.; Halvax, P.; Agnus, V.; Soler, L.; Lindner, V.; Demartines, N.; Diemunsch, P.; et al. Probe-based confocal laser endomicroscopy and fluorescence-based enhanced reality for real-time assessment of intestinal microcirculation in a porcine model of sigmoid ischemia. Surg. Endosc. 2014, 28, 3224–3233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diana, M.; Noll, E.; Charles, A.L.; Diemunsch, P.; Geny, B.; Liu, Y.Y.; Marchegiani, F.; Schiraldi, L.; Agnus, V.; Lindner, V.; et al. Precision real-time evaluation of bowel perfusion: Accuracy of confocal endomicroscopy assessment of stoma in a controlled hemorrhagic shock model. Surg. Endosc. 2017, 31, 680–691. [Google Scholar] [CrossRef] [PubMed]
- Barberio, M.; Felli, E.; Pizzicannella, M.; Agnus, V.; Al-Taher, M.; Seyller, E.; Moulla, Y.; Jansen-Winkeln, B.; Gockel, I.; Marescaux, J.; et al. Quantitative serosal and mucosal optical imaging perfusion assessment in gastric conduits for esophageal surgery: An experimental study in enhanced reality. Surg. Endosc. 2020. [Google Scholar] [CrossRef] [PubMed]
- Barberio, M.; Felli, E.; Pop, R.; Pizzicannella, M.; Geny, B.; Lindner, V.; Baiocchini, A.; Jansen-Winkeln, B.; Moulla, Y.; Agnus, V.; et al. A Novel Technique to Improve Anastomotic Perfusion Prior to Esophageal Surgery: Hybrid Ischemic Preconditioning of the Stomach. Preclinical Efficacy Proof in a Porcine Survival Model. Cancers 2020, 12, 2977. [Google Scholar] [CrossRef]
- Kilkenny, C.; Browne, W.J.; Cuthill, I.C.; Emerson, M.; Altman, D.G. Improving bioscience research reporting: The ARRIVE guidelines for reporting animal research. Osteoarthr. Cartil. 2012, 20, 256–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaefer, S.; McPhail, T.; Warren, J. Image Deformation using Moving Least Squares. In ACM SIGGRAPH 2006 Papers; Association for Computing Machinery: New York, NY, USA, 2006; pp. 533–540. [Google Scholar] [CrossRef]
- Diana, M.; Noll, E.; Diemunsch, P.; Moussallieh, F.-M.; Namer, I.-J.; Charles, A.-L.; Lindner, V.; Agnus, V.; Geny, B.; Marescaux, J. Metabolism-guided bowel resection: Potential role and accuracy of instant capillary lactates to identify the optimal resection site. Surg. Innov. 2015, 22, 453–461. [Google Scholar] [CrossRef]
- Diana, M.; Pop, R.; Beaujeux, R.; Dallemagne, B.; Halvax, P.; Schlagowski, I.; Liu, Y.Y.; Diemunsch, P.; Geny, B.; Lindner, V.; et al. Embolization of arterial gastric supply in obesity (EMBARGO): An endovascular approach in the management of morbid obesity. proof of the concept in the porcine model. Obes. Surg. 2015, 25, 550–558. [Google Scholar] [CrossRef]
- Schlagowski, A.I.; Singh, F.; Charles, A.L.; Gali Ramamoorthy, T.; Favret, F.; Piquard, F.; Geny, B.; Zoll, J. Mitochondrial uncoupling reduces exercise capacity despite several skeletal muscle metabolic adaptations. J. Appl. Physiol. 2014, 116, 364–375. [Google Scholar] [CrossRef] [Green Version]
- Ederlé, C.; Charles, A.L.; Khayath, N.; Poirot, A.; Meyer, A.; Clere-Jehl, R.; Andres, E.; De Blay, F.; Geny, B. Mitochondrial Function in Peripheral Blood Mononuclear Cells (PBMC) Is Enhanced, Together with Increased Reactive Oxygen Species, in Severe Asthmatic Patients in Exacerbation. J. Clin. Med. 2019, 8, 1613. [Google Scholar] [CrossRef] [Green Version]
- Virtanen, P.; Gommers, R.; Oliphant, T.E.; Haberland, M.; Reddy, T.; Cournapeau, D.; Burovski, E.; Peterson, P.; Weckesser, W.; Bright, J. SciPy 1.0: Fundamental algorithms for scientific computing in Python. Nat. Methods 2020, 17, 261–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathur, A.; Pitt, H.A.; Marine, M.; Saxena, R.; Schmidt, C.M.; Howard, T.J.; Nakeeb, A.; Zyromski, N.J.; Lillemoe, K.D. Fatty pancreas: A factor in postoperative pancreatic fistula. Ann. Surg. 2007, 246, 1058–1064. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, M.; Takahashi, S.; Kobayashi, T.; Kojima, M.; Gotohda, N.; Satake, M.; Ochiai, A.; Konishi, M. Pancreatic perfusion data and post-pancreaticoduodenectomy outcomes. J. Surg. Res. 2015, 194, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Macchi, V.; Picardi, E.E.E.; Porzionato, A.; Morra, A.; Bardini, R.; Loukas, M.; Tubbs, R.S.; De Caro, R. Anatomo-radiological patterns of pancreatic vascularization, with surgical implications: Clinical and anatomical study. Clin. Anat. 2017, 30, 614–624. [Google Scholar] [CrossRef] [PubMed]
- Skandalakis, L.J.; Rowe, J.S., Jr.; Gray, S.W.; Skandalakis, J.E. Surgical embryology and anatomy of the pancreas. Surg. Clin. N. Am. 1993, 73, 661–697. [Google Scholar] [CrossRef]
- Ferrer, J.; Scott , W.E., III; Weegman, B.P.; Suszynski, T.M.; Sutherland, D.E.; Hering, B.J.; Papas, K.K. Pig pancreas anatomy: Implications for pancreas procurement, preservation, and islet isolation. Transplantation 2008, 86, 1503. [Google Scholar] [CrossRef] [Green Version]
- Eriksson, S.; Nilsson, J.; Lindell, G.; Sturesson, C. Laser speckle contrast imaging for intraoperative assessment of liver microcirculation: A clinical pilot study. Med. Devices 2014, 7, 257–261. [Google Scholar] [CrossRef] [Green Version]
- Ambrus, R.; Strandby, R.B.; Svendsen, L.B.; Achiam, M.P.; Steffensen, J.F.; Søndergaard Svendsen, M.B. Laser Speckle Contrast Imaging for Monitoring Changes in Microvascular Blood Flow. Eur. Surg. Res. 2016, 56, 87–96. [Google Scholar] [CrossRef]
- Klijn, E.; Niehof, S.; de Jonge, J.; Gommers, D.; Ince, C.; van Bommel, J. The effect of perfusion pressure on gastric tissue blood flow in an experimental gastric tube model. Anesth. Analg. 2010, 110, 541–546. [Google Scholar] [CrossRef]
- Ambrus, R.; Svendsen, L.B.; Secher, N.H.; Rünitz, K.; Frederiksen, H.J.; Svendsen, M.B.; Siemsen, M.; Kofoed, S.C.; Achiam, M.P. A reduced gastric corpus microvascular blood flow during Ivor-Lewis esophagectomy detected by laser speckle contrast imaging technique. Scand. J. Gastroenterol. 2017, 52, 455–461. [Google Scholar] [CrossRef]
- Ambrus, R.; Achiam, M.P.; Secher, N.H.; Svendsen, M.B.S.; Rünitz, K.; Siemsen, M.; Svendsen, L.B. Evaluation of Gastric Microcirculation by Laser Speckle Contrast Imaging During Esophagectomy. J. Am. Coll. Surg. 2017, 225, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Heeman, W.; Steenbergen, W.; van Dam, G.; Boerma, E.C. Clinical applications of laser speckle contrast imaging: A review. J. Biomed. Opt. 2019, 24, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Urso, A.; Agnus, V.; Barberio, M.; Seeliger, B.; Marchegiani, F.; Charles, A.L.; Geny, B.; Marescaux, J.; Mutter, D.; Diana, M. Computer-assisted quantification and visualization of bowel perfusion using fluorescence-based enhanced reality in left-sided colonic resections. Surg. Endosc. 2020. [Google Scholar] [CrossRef]
- Fugazza, A.; Gaiani, F.; Carra, M.C.; Brunetti, F.; Lévy, M.; Sobhani, I.; Azoulay, D.; Catena, F.; de’Angelis, G.L.; de’Angelis, N. Confocal laser endomicroscopy in gastrointestinal and pancreatobiliary diseases: A systematic review and meta-analysis. Biomed. Res. Int. 2016, 2016, 4638683. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wakabayashi, T.; Barberio, M.; Urade, T.; Pop, R.; Seyller, E.; Pizzicannella, M.; Mascagni, P.; Charles, A.-L.; Abe, Y.; Geny, B.; et al. Intraoperative Perfusion Assessment in Enhanced Reality Using Quantitative Optical Imaging: An Experimental Study in a Pancreatic Partial Ischemia Model. Diagnostics 2021, 11, 93. https://doi.org/10.3390/diagnostics11010093
Wakabayashi T, Barberio M, Urade T, Pop R, Seyller E, Pizzicannella M, Mascagni P, Charles A-L, Abe Y, Geny B, et al. Intraoperative Perfusion Assessment in Enhanced Reality Using Quantitative Optical Imaging: An Experimental Study in a Pancreatic Partial Ischemia Model. Diagnostics. 2021; 11(1):93. https://doi.org/10.3390/diagnostics11010093
Chicago/Turabian StyleWakabayashi, Taiga, Manuel Barberio, Takeshi Urade, Raoul Pop, Emilie Seyller, Margherita Pizzicannella, Pietro Mascagni, Anne-Laure Charles, Yuta Abe, Bernard Geny, and et al. 2021. "Intraoperative Perfusion Assessment in Enhanced Reality Using Quantitative Optical Imaging: An Experimental Study in a Pancreatic Partial Ischemia Model" Diagnostics 11, no. 1: 93. https://doi.org/10.3390/diagnostics11010093
APA StyleWakabayashi, T., Barberio, M., Urade, T., Pop, R., Seyller, E., Pizzicannella, M., Mascagni, P., Charles, A.-L., Abe, Y., Geny, B., Baiocchini, A., Kitagawa, Y., Marescaux, J., Felli, E., & Diana, M. (2021). Intraoperative Perfusion Assessment in Enhanced Reality Using Quantitative Optical Imaging: An Experimental Study in a Pancreatic Partial Ischemia Model. Diagnostics, 11(1), 93. https://doi.org/10.3390/diagnostics11010093