
Loss of DUSP4 Expression as a Prognostic Biomarker in Clear Cell Renal Cell Carcinoma

 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection and Pathological Evaluation
2.2. Tissue Microarray Construction
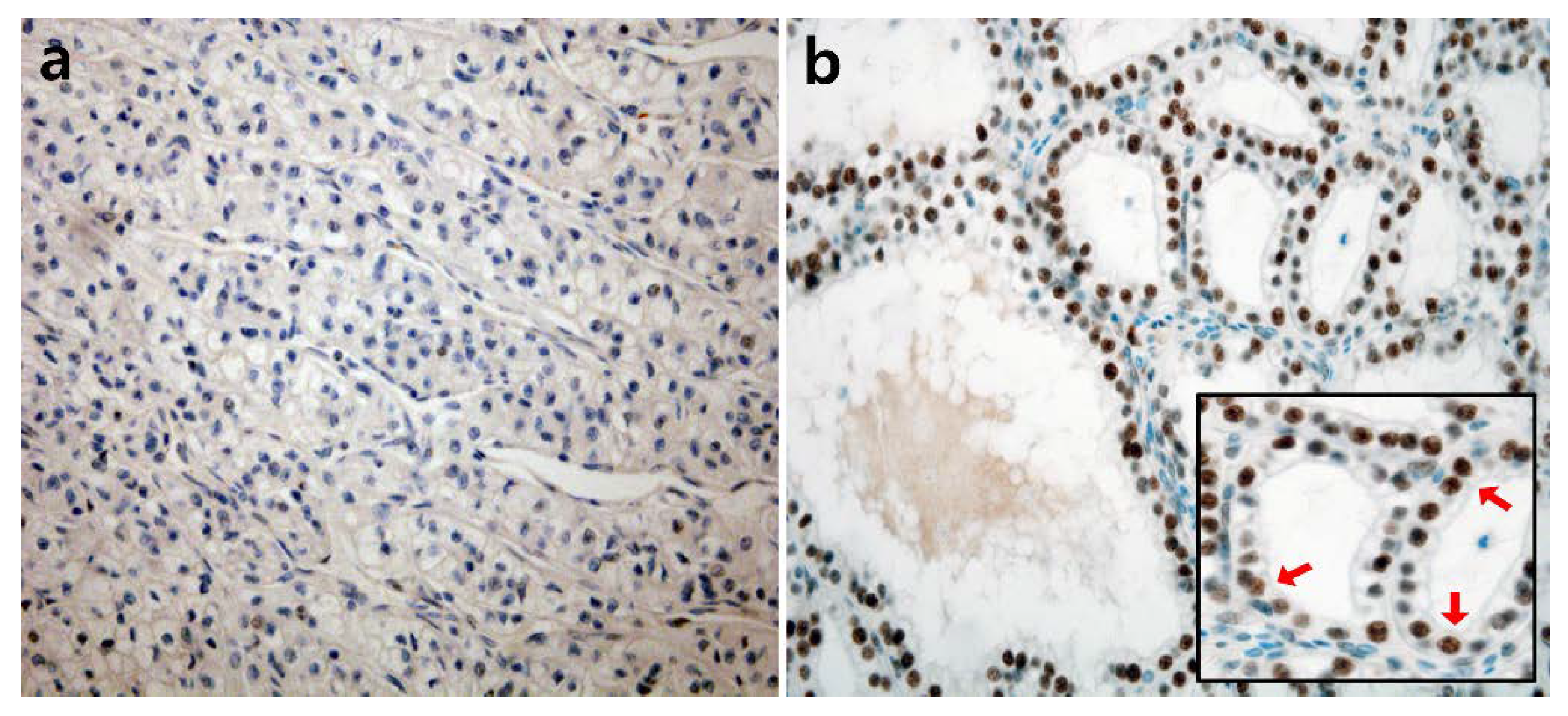
2.3. Immunohistochemical Staining and Interpretation
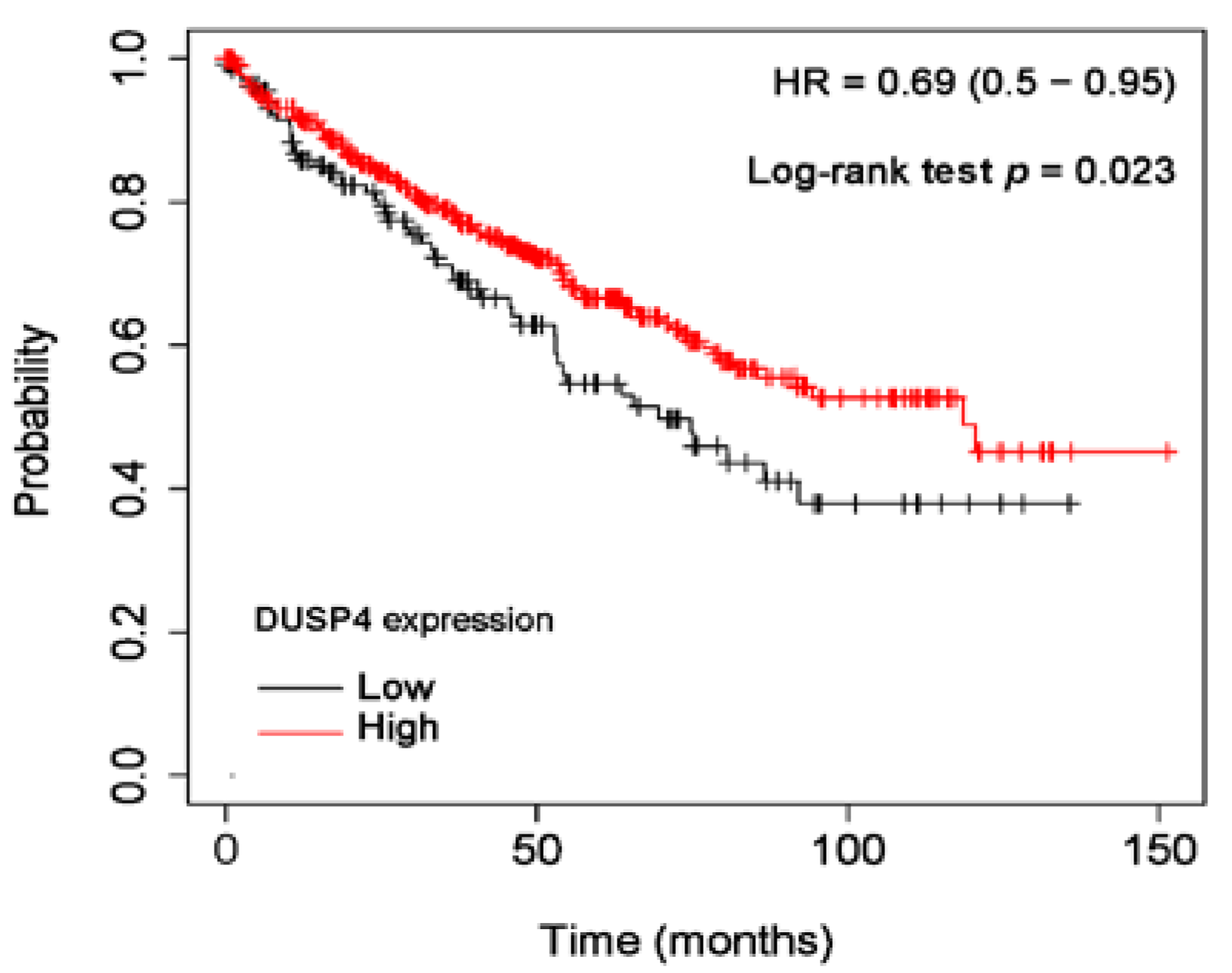
2.4. Online Analysis Based on the Cancer Genome Atlas
2.5. Statistical Analyses
3. Results
3.1. The Clinicopathological Characteristics of RCC Patients
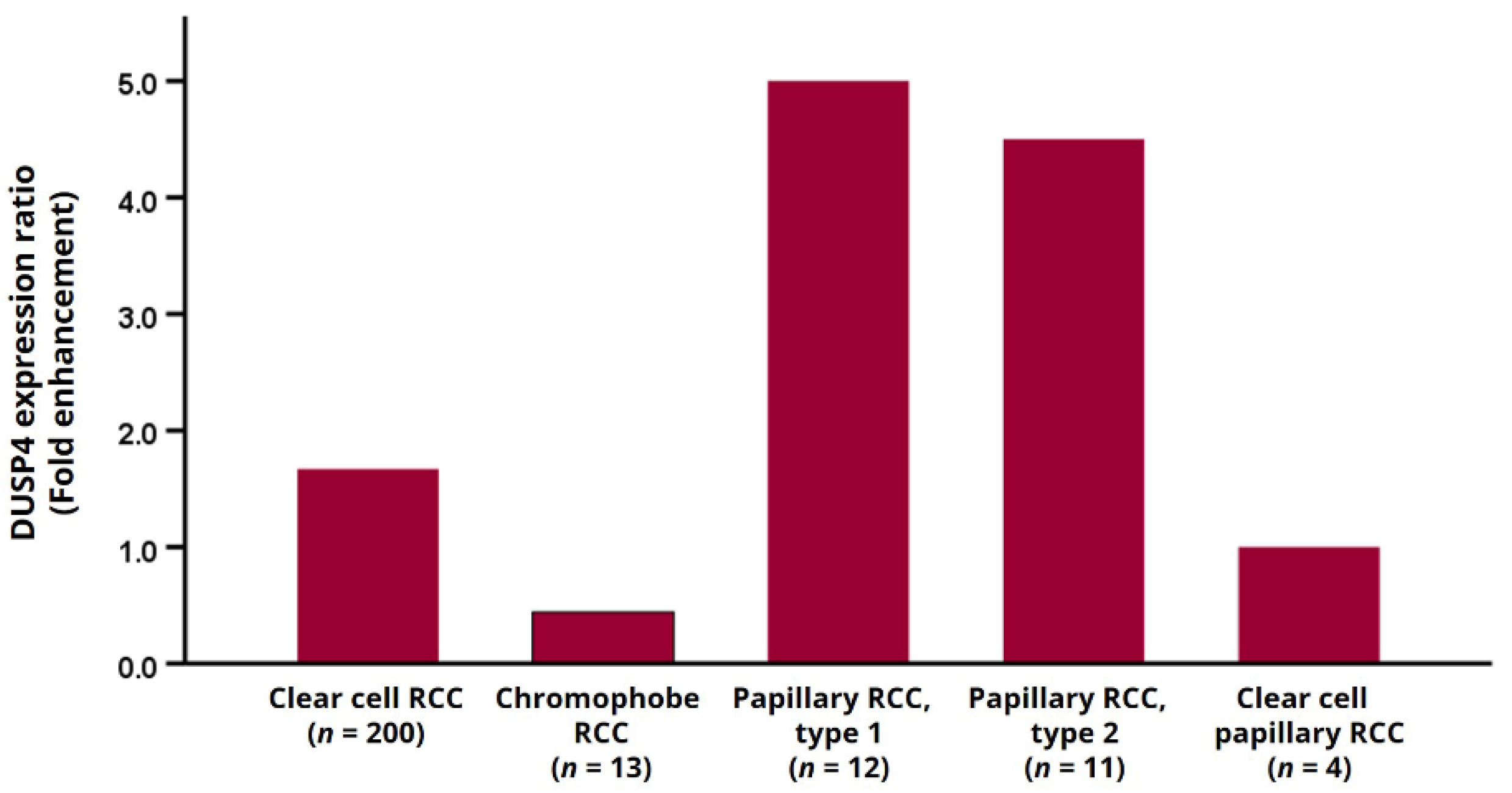
3.2. DUSP4 Expression Pattern According to Histological Subtype
3.3. DUSP4 Expression and Clinicopathological Characteristics in ccRCC Patients
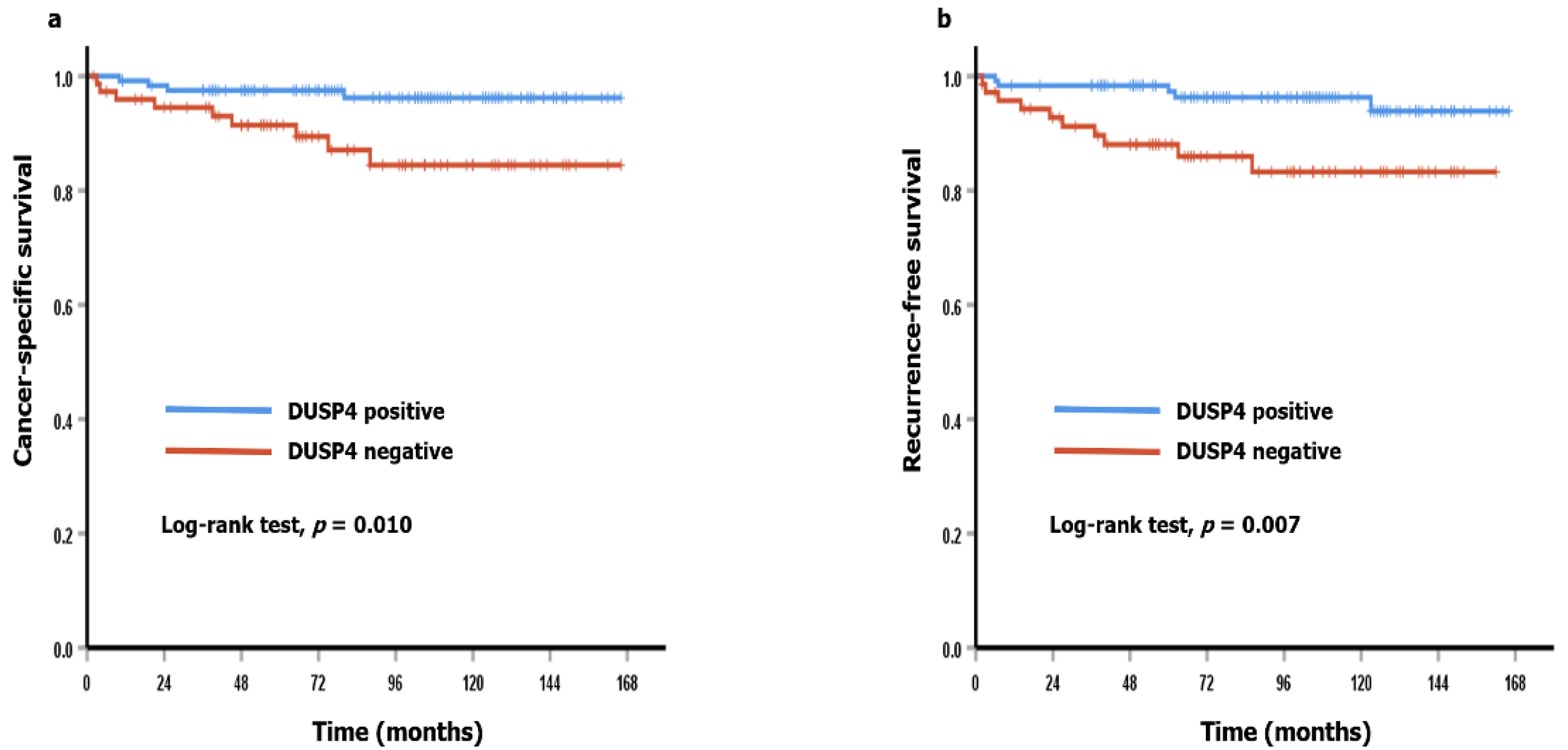
3.4. DUSP4 Expression and Clinicopathological Characteristics in ccRCC Patients
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Padala, S.A.; Barsouk, A.; Thandra, K.C.; Saginala, K.; Mohammed, A.; Vakiti, A.; Rawla, P.; Barsouk, A. Epidemiology of Renal Cell Carcinoma. World J. Oncol. 2020, 11, 79–87. [Google Scholar] [CrossRef]
- Linehan, W.M.; Schmidt, L.S.; Crooks, D.R.; Wei, D.; Srinivasan, R.; Lang, M.; Ricketts, C.J. The Metabolic Basis of Kidney Cancer. Cancer Discov. 2019, 9, 1006–1021. [Google Scholar] [CrossRef] [PubMed]
- Benej, M.; Pastorekova, S.; Pastorek, J. Carbonic Anhydrase IX: Regulation and Role in Cancer. In Carbonic Anhydrase: Mechanism, Regulation, Links to Disease, and Industrial Applications; Subcellular Biochemistry; Springer: Dordrecht, The Netherlands, 2013; Volume 75, pp. 199–219. [Google Scholar] [CrossRef]
- Rini, B.I.; Rathmell, W. Biological Aspects and Binding Strategies of Vascular Endothelial Growth Factor in Renal Cell Carcinoma. Clin. Cancer Res. 2007, 13, 741s–746s. [Google Scholar] [CrossRef] [PubMed][Green Version]
- McGuire, B.B.; Fitzpatrick, J.M. Biomarkers in renal cell carcinoma. Curr. Opin. Urol. 2009, 19, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-F.; Chuang, H.-C.; Tan, T.-H. Regulation of Dual-Specificity Phosphatase (DUSP) Ubiquitination and Protein Stability. Int. J. Mol. Sci. 2019, 20, 2668. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.; Raffi, F.A. Dual-Specificity Phosphatases in Immunity and Infection: An Update. Int. J. Mol. Sci. 2019, 20, 2710. [Google Scholar] [CrossRef]
- Huang, C.-Y.; Tan, T.-H. DUSPs, to MAP kinases and beyond. Cell Biosci. 2012, 2, 24. [Google Scholar] [CrossRef]
- Bermudez, O.; Pagès, G.; Gimond, C. The dual-specificity MAP kinase phosphatases: Critical roles in development and cancer. Am. J. Physiol. Cell Physiol. 2010, 299, C189–C202. [Google Scholar] [CrossRef]
- Xu, X.; Gao, F.; Wang, J.; Tao, L.; Ye, J.; Ding, L.; Ji, W.; Chen, X. MiR-122-5p inhibits cell migration and invasion in gastric cancer by down-regulating DUSP4. Cancer Biol. Ther. 2018, 19, 427–435. [Google Scholar] [CrossRef]
- Ratsada, P.; Hijiya, N.; Hidano, S.; Tsukamoto, Y.; Nakada, C.; Uchida, T.; Kobayashi, T.; Moriyama, M. DUSP4 is involved in the enhanced proliferation and survival of DUSP4-overexpressing cancer cells. Biochem. Biophys. Res. Commun. 2020, 528, 586–593. [Google Scholar] [CrossRef]
- Hu, N.; Tian, Y.; Song, Y.; Zang, L. miR-122-5p suppresses the oncogenesis of PTC by inhibiting DUSP4 expression. Mol. Med. Rep. 2021, 23, 368. [Google Scholar] [CrossRef]
- He, H.; Du, Z.; Lin, J.; Wu, W.; Yu, Y. DUSP4 inhibits autophagic cell death in PTC by inhibiting JNK–BCL2–Beclin1 signaling. Biochem. Cell Biol. 2021, 99, 1–8. [Google Scholar] [CrossRef]
- Zeng, X.; Zhu, C.; Zhu, X. DUSP4 promotes the carcinogenesis of CCRCC via negative regulation of autophagic death. Biosci. Biotechnol. Biochem. 2021, 85, 1839–1845. [Google Scholar] [CrossRef]
- Laczmanska, I.; Laczmanski, L.; Sasiadek, M.M. Expression Analysis of Tyrosine Phosphatase Genes at Different Stages of Renal Cell Carcinoma. Anticancer. Res. 2020, 40, 5667–5671. [Google Scholar] [CrossRef]
- Amin, M.B.; American Joint Committee on Cancer; American Cancer Society (Eds.) AJCC Cancer Staging Manual; Springer: Chicago, IL, USA, 2017. [Google Scholar]
- Zlobec, I.; Steele, R.; Terracciano, L.; Jass, J.R.; Lugli, A. Selecting immunohistochemical cut-off scores for novel biomarkers of progression and survival in colorectal cancer. J. Clin. Pathol. 2007, 60, 1112–1116. [Google Scholar] [CrossRef]
- Pinto, A.; Monteiro, P.; Silva, G.; Ayres, J.; Soares, J. Prognostic Biomarkers in Renal Cell Carcinoma: Relevance of DNA Ploidy in Predicting Disease-Related Survival. Int. J. Biol. Markers 2005, 20, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Jang, S.M.; Ahn, H.; Sim, J.; Yi, K.; Chung, Y.; Han, H.; Rehman, A.; Chung, M.S.; Jang, K.; et al. Clinicopathological Significance of Dual-Specificity Protein Phosphatase 4 Expression in Invasive Ductal Carcinoma of the Breast. J. Breast Cancer 2015, 18, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Mazumdar, A.; Poage, G.M.; Shepherd, J.; Tsimelzon, A.; Hartman, Z.C.; Hollander, P.D.; Hill, J.; Zhang, Y.; Chang, J.; Hilsenbeck, S.G.; et al. Analysis of phosphatases in ER-negative breast cancers identifies DUSP4 as a critical regulator of growth and invasion. Breast Cancer Res. Treat. 2016, 158, 441–454. [Google Scholar] [CrossRef]
- Du, F.; Yu, L.; Wu, Y.; Wang, S.; Yao, J.; Zheng, X.; Xie, S.; Zhang, S.; Lu, X.; Liu, Y.; et al. miR-137 alleviates doxorubicin resistance in breast cancer through inhibition of epithelial-mesenchymal transition by targeting DUSP4. Cell Death Dis. 2019, 10, 922. [Google Scholar] [CrossRef] [PubMed]
- Armes, J.E.; Hammet, F.; De Silva, M.; Ciciulla, J.; Ramus, S.J.; Soo, W.-K.; Mahoney, A.; Yarovaya, N.; Henderson, M.A.; Gish, K.; et al. Candidate tumor-suppressor genes on chromosome arm 8p in early-onset and high-grade breast cancers. Oncogene 2004, 23, 5697–5702. [Google Scholar] [CrossRef] [PubMed]
- Gröschl, B.; Bettstetter, M.; Giedl, C.; Woenckhaus, M.; Edmonston, T.; Hofstädter, F.; Dietmaier, W. Expression of the MAP kinase phosphatase DUSP4 is associated with microsatellite instability in colorectal cancer (CRC) and causes increased cell proliferation. Int. J. Cancer 2013, 132, 1537–1546. [Google Scholar] [CrossRef] [PubMed]
- Ichimanda, M.; Hijiya, N.; Tsukamoto, Y.; Uchida, T.; Nakada, C.; Akagi, T.; Etoh, T.; Iha, H.; Inomata, M.; Takekawa, M.; et al. Downregulation of dual-specificity phosphatase 4 enhances cell proliferation and invasiveness in colorectal carcinomas. Cancer Sci. 2018, 109, 250–258. [Google Scholar] [CrossRef]
- Xu, W.; Chen, B.; Ke, D.; Chen, X. DUSP4 directly deubiquitinates and stabilizes Smad4 protein, promoting proliferation and metastasis of colorectal cancer cells. Aging 2020, 12, 17634–17646. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Wang, Q.; Cao, L.; Tang, Y.; Yao, M.; Bi, H.; Huang, Y.; Sun, G.; Song, J. Nicotine-derived NNK induces the stemness enrichment of CRC cells through regulating the balance of DUSP4-ERK1/2 feedback loop. Ecotoxicol. Environ. Saf. 2021, 214, 112057. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Qiu, S.; Xie, L.; Liu, C.; Sun, S. Nimbolide suppresses non-small cell lung cancer cell invasion and migration via manipulation of DUSP4 expression and ERK1/2 signaling. Biomed. Pharmacother. 2017, 92, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.-C.; Yang, Y.-F.; Chiou, J.; Tsai, H.-F.; Fang, C.-Y.; Yang, C.-J.; Chen, C.-L.; Hsiao, M. Nonenzymatic function of Aldolase A downregulates miR-145 to promote the Oct4/DUSP4/TRAF4 axis and the acquisition of lung cancer stemness. Cell Death Dis. 2020, 11, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Ma, B.; Shi, R.; Yang, S.; Zhou, L.; Qu, N.; Liao, T.; Wang, Y.; Ji, Q. DUSP4/MKP2 overexpression is associated with BRAFV600E mutation and aggressive behavior of papillary thyroid cancer. OncoTargets Ther. 2016, 9, 2255–2263. [Google Scholar] [CrossRef]
- Gan, S.; Ye, R.; Ha, Y.; Xiong, Y.; Li, R.; Di, X.; Zou, Z.; Sun, Y.; Zhang, Z. Prediction Biomarkers Associated with Lymph Node Metastasis and Prognosis were Identified in Papillary Thyroid Carcinoma via Integrated Bioinformatics Analysis. Comb. Chem. High Throughput Screen. 2021, 24, 1395–1409. [Google Scholar] [CrossRef]
- Menyhart, O.; Budczies, J.; Munkácsy, G.; Esteva, F.; Szabó, A.; Miquel, T.P.; Győrffy, B. DUSP4 is associated with increased resistance against anti-HER2 therapy in breast cancer. Oncotarget 2017, 8, 77207–77218. [Google Scholar] [CrossRef]
- Kang, X.; Li, M.; Zhu, H.; Lu, X.; Miao, J.; Du, S.; Xia, X.; Guan, W. DUSP4 promotes doxorubicin resistance in gastric cancer through epithelial-mesenchymal transition. Oncotarget 2017, 8, 94028–94039. [Google Scholar] [CrossRef]
- Park, S.; Hwang, C.Y.; Cho, S.; Lee, D.; Gong, J.; Lee, S.; Nam, S.; Cho, K. Systems analysis identifies potential target genes to overcome cetuximab resistance in colorectal cancer cells. FEBS J. 2019, 286, 1305–1318. [Google Scholar] [CrossRef]
- Chen, X.; Tan, W.; Li, W.; Li, W.; Zhu, S.; Zhong, J.; Shang, C.; Chen, Y. miR-1226-3p Promotes Sorafenib Sensitivity of Hepatocellular Carcinoma via Downregulation of DUSP4 Expression. J. Cancer 2019, 10, 2745–2753. [Google Scholar] [CrossRef]
- Cheng, G.; Li, Y.; Liu, Z.; Song, X. The microRNA-429/DUSP4 axis regulates the sensitivity of colorectal cancer cells to nintedanib. Mol. Med. Rep. 2021, 23, 228. [Google Scholar] [CrossRef]
- Balko, J.M.; Cook, R.S.; Vaught, D.B.; Kuba, M.G.; Miller, T.W.; Bhola, N.E.; E Sanders, M.; Granja-Ingram, N.M.; Smith, J.J.; Meszoely, I.M.; et al. Profiling of residual breast cancers after neoadjuvant chemotherapy identifies DUSP4 deficiency as a mechanism of drug resistance. Nat. Med. 2012, 18, 1052–1059. [Google Scholar] [CrossRef]
- Gupta, A.; Towers, C.; Willenbrock, F.; Brant, R.; Hodgson, D.R.; Sharpe, A.; Smith, P.; Cutts, A.; Schuh, A.; Asher, R.; et al. Dual-specificity protein phosphatase DUSP4 regulates response to MEK inhibition in BRAF wild-type melanoma. Br. J. Cancer 2020, 122, 506–516. [Google Scholar] [CrossRef]
- Schmid, C.A.; Robinson, M.; Scheifinger, N.A.; Müller, S.; Cogliatti, S.; Tzankov, A.; Müller, A. DUSP4 deficiency caused by promoter hypermethylation drives JNK signaling and tumor cell survival in diffuse large B cell lymphoma. J. Exp. Med. 2015, 212, 775–792. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Li, M.D. Establishment of a Strong Link between Smoking and Cancer Pathogenesis through DNA Methylation Analysis. Sci. Rep. 2017, 7, 1811. [Google Scholar] [CrossRef] [PubMed]
- Eichenauer, T.; Bannenberg, D.C.; Kluth, M.; Wittmer, C.; Büscheck, F.; Möller, K.; Dum, D.; Fraune, C.; Hube-Magg, C.; Möller-Koop, C.; et al. 8p deletions in renal cell carcinoma are associated with unfavorable tumor features and poor overall survival. Urol. Oncol. Semin. Orig. Investig. 2020, 38, 43.e13–43.e20. [Google Scholar] [CrossRef] [PubMed]
- Chitale, D.; Gong, Y.; Taylor, B.S.; Broderick, S.; Brennan, C.; Somwar, R.; Golas, B.; Wang, L.; Motoi, N.; Szoke, J.; et al. An integrated genomic analysis of lung cancer reveals loss of DUSP4 in EGFR-mutant tumors. Oncogene 2009, 28, 2773–2783. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.; Crowther, J.; Pastor, T.; Asbagh, L.A.; Baietti, M.F.; De Troyer, M.; Vazquez, I.; Talebi, A.; Renzi, F.; Dehairs, J.; et al. Loss of Chromosome 8p Governs Tumor Progression and Drug Response by Altering Lipid Metabolism. Cancer Cell 2016, 29, 751–766. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Case No. (%) |
|---|---|
| Age, median (range, year) | 58 (25–85) |
| Sex | |
| Male | 167 (68.4%) |
| Female | 77 (31.5%) |
| Tumor size, mean (range, cm) | 3.8 (0.7–15.5) |
| Histological subtype (by WHO classification, 2016) | |
| Clear cell RCC | 200 (82.0%) |
| Chromophobe RCC | 13 (5.3%) |
| Papillary RCC, type 1 | 12 (4.9%) |
| Papillary RCC, type 2 | 11 (4.5%) |
| Others * | 8 (3.3%) |
| Histologic grade (WHO/ISUP grade in clear and papillary RCC) | |
| Grade 1 | 29 (13.0%) |
| Grade 2 | 113 (50.7%) |
| Grade 3 | 65 (29.1%) |
| Grade 4 | 16 (7.2%) |
| Vascular invasion | |
| Absent | 208 (85.2%) |
| Present | 36 (14.8%) |
| Tumor necrosis | |
| Absent | 205 (84.0%) |
| Present | 39 (16.0%) |
| Sarcomatoid features | |
| Absent | 228 (93.4%) |
| Present | 16 (6.6%) |
| pT category | |
| pT1 | 184 (75.4%) |
| pT2 | 12 (4.9%) |
| pT3 | 47 (19.3%) |
| pT4 | 1 (0.4%) |
| pN category | |
| pN0 | 240 (98.4%) |
| pN1 | 4 (1.6%) |
| Histological Subtypes | DUSP4 Expression | |
|---|---|---|
| Negative (%) (n = 90) | Positive (%) (n = 154) | |
| Clear cell RCC | 75 (37.5%) | 125 (62.5%) |
| Chromophobe RCC | 9 (69.2%) | 4 (30.8%) |
| Papillary RCC, type 1 | 2 (16.7%) | 10 (83.3%) |
| Papillary RCC, type 2 | 2 (18.2%) | 9 (81.8%) |
| Clear cell papillary RCC | 2 (50%) | 2 (50%) |
| Collecting duct carcinoma | 0 (0%) | 1 (100%) |
| Acquired cystic disease-associated RCC | 0 (0%) | 3 (100%) |
| Variables | DUSP4 Expression | p Value | |
|---|---|---|---|
| Negative (%) | Positive (%) | ||
| Age | 0.033 | ||
| <65 years | 43 (32.3%) | 90 (67.7%) | |
| ≥65 years | 32 (47.8%) | 35 (55.2%) | |
| Sex | 0.968 | ||
| Female | 23 (37.7%) | 38 (62.3%) | |
| Male | 52 (37.4%) | 87 (62.6%) | |
| WHO/ISUP grade | <0.001 | ||
| Grade 1 and 2 | 33 (26.4%) | 92 (73.6%) | |
| Grade 3 and 4 | 42 (56.0%) | 33 (44.0%) | |
| Tumor necrosis | <0.001 | ||
| Absent | 53 (31.9%) | 113 (68.1%) | |
| Present | 22 (64.7%) | 12 (35.3%) | |
| Sarcomatoid feature | 0.064 | ||
| Absent | 67 (35.8%) | 120 (64.2%) | |
| Present | 8 (61.5%) | 5 (38.5%) | |
| pT category | <0.001 | ||
| pT1 and pT2 | 48 (30.6%) | 109 (69.4%) | |
| pT3 and pT4 | 27 (62.8%) | 16 (37.2%) | |
| pN category | 0.684 | ||
| pN0 | 74 (37.6%) | 123 (62.4%) | |
| pN1 | 1 (33.3%) | 2 (66.6%) | |
| Variables | Cancer-Specific Survival | Recurrence-Free Survival | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | |
| DUSP4 expression (positive vs. negative) | 4.170 | 1.283–13.559 | 0.018 | 3.972 | 1.355–11.643 | 0.012 |
| Age group (<65 vs. ≥65) | 2.047 | 0.741–5.655 | 0.167 | 2.089 | 0.756–5.772 | 0.156 |
| Sex (female vs. male) | 1.720 | 0.485–6.097 | 0.401 | 2.829 | 0.638–12.537 | 0.171 |
| WHO/ISUP grade (I and II vs. III and IV) | 13.423 | 3.009–59.870 | 0.001 | 3.237 | 1.147–9.138 | 0.027 |
| Tumor necrosis (absent vs. present) | 16.355 | 5.177–51.667 | <0.001 | 6.136 | 2.207–17.064 | 0.001 |
| Sarcomatoid feature (absent vs. present) | 20.318 | 7.316–56.432 | <0.001 | 3.726 | 0.840–16.519 | 0.083 |
| pT category (pT1–2 vs. pT3–4) | 55.296 | 7.267–420.728 | <0.001 | 18.732 | 5.275–66.520 | <0.001 |
| pN category (pN0 vs. pN1) | 54.804 | 13.264–226.446 | <0.001 | 95.664 | 8.674–1055.014 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bang, S.; Jee, S.; Son, H.; Wi, Y.C.; Kim, H.; Park, H.; Myung, J.; Shin, S.-J.; Paik, S.S. Loss of DUSP4 Expression as a Prognostic Biomarker in Clear Cell Renal Cell Carcinoma. Diagnostics 2021, 11, 1939. https://doi.org/10.3390/diagnostics11101939
Bang S, Jee S, Son H, Wi YC, Kim H, Park H, Myung J, Shin S-J, Paik SS. Loss of DUSP4 Expression as a Prognostic Biomarker in Clear Cell Renal Cell Carcinoma. Diagnostics. 2021; 11(10):1939. https://doi.org/10.3390/diagnostics11101939
Chicago/Turabian StyleBang, Seongsik, Seungyun Jee, Hwangkyu Son, Young Chan Wi, Hyunsung Kim, Hosub Park, Jaekyung Myung, Su-Jin Shin, and Seung Sam Paik. 2021. "Loss of DUSP4 Expression as a Prognostic Biomarker in Clear Cell Renal Cell Carcinoma" Diagnostics 11, no. 10: 1939. https://doi.org/10.3390/diagnostics11101939
APA StyleBang, S., Jee, S., Son, H., Wi, Y. C., Kim, H., Park, H., Myung, J., Shin, S.-J., & Paik, S. S. (2021). Loss of DUSP4 Expression as a Prognostic Biomarker in Clear Cell Renal Cell Carcinoma. Diagnostics, 11(10), 1939. https://doi.org/10.3390/diagnostics11101939