
Endoscopic Ultrasound Quality Metrics in Clinical Practice


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Demographics and Procedure Metrics
3.2. Indications
3.3. Outcomes: General
3.4. Outcomes: Malignancy
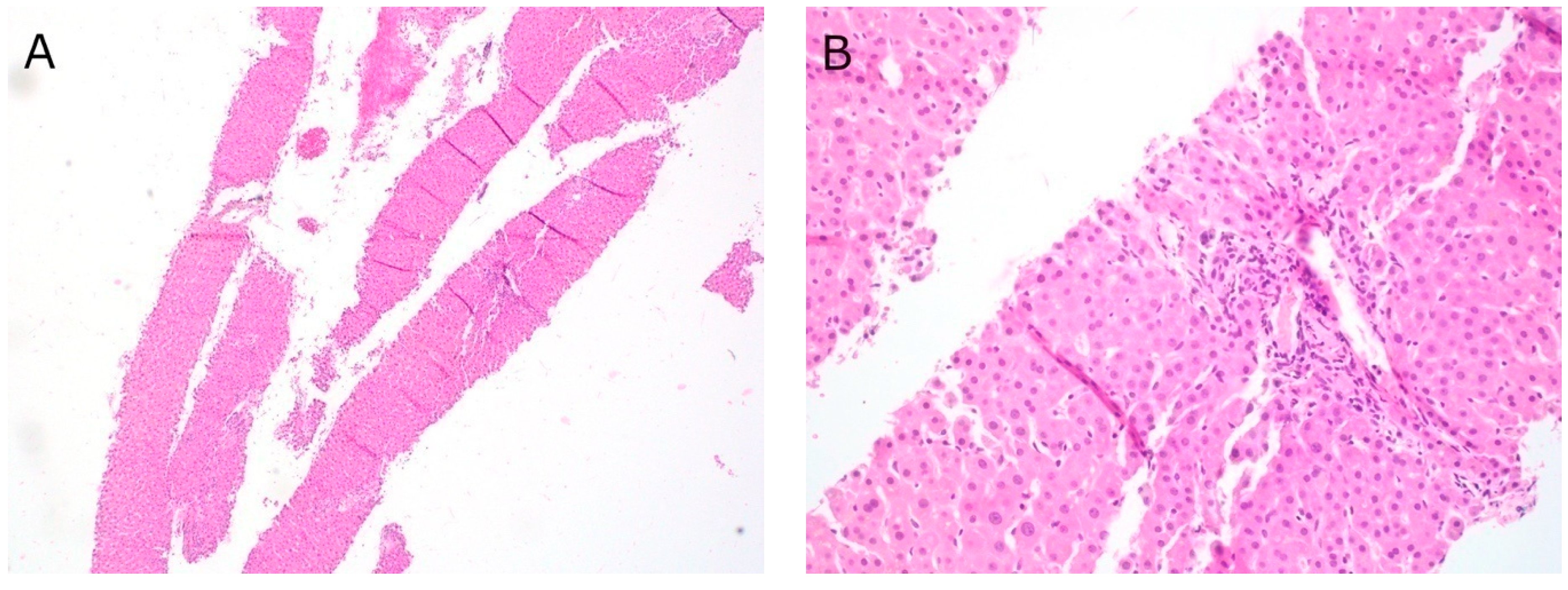
3.5. Outcomes: Liver Biopsy
3.6. Outcomes: Choledocholithiasis
3.7. Complications
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ainsworth, A.P.; Mortensen, M.B.; Durup, J.; Wamberg, P.A. Clinical impact of endoscopic ultrasonography at a county hospital. Endoscopy 2002, 34, 447–450. [Google Scholar] [CrossRef]
- Chong, A.K.; Caddy, G.R.; Desmond, P.V.; Chen, R.Y. Prospective study of the clinical impact of EUS. Gastrointest. Endosc. 2005, 62, 399–405. [Google Scholar] [CrossRef]
- Kalade, A.V.; Desmond, P.V.; Chen, R.Y. Experience of endoscopic ultrasound in an Australian tertiary hospital. ANZ J. Surg. 2006, 76, 1075–1080. [Google Scholar] [CrossRef] [PubMed]
- Wani, S.; Wallace, M.B.; Cohen, J.; Pike, I.M.; Adler, D.G.; Kochman, M.L.; Lieb, J.G., 2nd; Park, W.G.; Rizk, M.K.; Sawhney, M.S.; et al. Quality indicators for EUS. Gastrointest. Endosc. 2015, 81, 67–80. [Google Scholar] [CrossRef] [PubMed]
- Early, D.S.; Ben-Menachem, T.; Decker, G.A.; Evans, J.A.; Fanelli, R.D.; Fisher, D.A.; Fukami, N.; Hwang, J.H.; Jain, R.; Jue, T.L.; et al. Appropriate use of GI endoscopy. Gastrointest. Endosc. 2012, 75, 1127–1131. [Google Scholar] [CrossRef]
- Maple, J.T.; Ben-Menachem, T.; Anderson, M.A.; Appalaneni, V.; Banerjee, S.; Cash, B.D.; Fisher, L.; Harrison, M.E.; Fanelli, R.D.; Fukami, N.; et al. The role of endoscopy in the evaluation of suspected choledocholithiasis. Gastrointest. Endosc. 2010, 71, 1–9. [Google Scholar] [CrossRef]
- Buxbaum, J.L.; Abbas Fehmi, S.M.; Sultan, S.; Fishman, D.S.; Qumseya, B.J.; Cortessis, V.K.; Schilperoort, H.; Kysh, L.; Matsuoka, L.; Yachimski, P.; et al. ASGE guideline on the role of endoscopy in the evaluation and management of choledocholithiasis. Gastrointest. Endosc. 2019, 89, 1075–1105. [Google Scholar] [CrossRef] [PubMed]
- Lok, K.-H.; Lee, C.-K.; Yiu, H.-L.; Lai, L.; Szeto, M.-L.; Leung, S.-K. Current utilization and performance status of endoscopic ultrasound in a community hospital. J. Dig. Dis. 2008, 9, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Purohit, T.; Aoun, E.; Patel, Y.; Carleton, N.; Mitre, M.; Morrissey, S.; Dhawan, M.; Thakkar, S. Comparison of the outcomes of endoscopic ultrasound based on community hospital versus tertiary academic center settings. Dig. Dis. Sci. 2014, 59, 1925–1930. [Google Scholar] [CrossRef]
- Amin, M.B.; Edge, S.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. (Eds.) AJCC Cancer Staging Manual, 8th ed.; Springer International Publishing: Cham, Switzerland, 2017; ISBN 978-3-319-40617-6. [Google Scholar]
- Mocellin, S.; Marchet, A.; Nitti, D. EUS for the staging of gastric cancer: A meta-analysis. Gastrointest. Endosc. 2011, 73, 1122–1134. [Google Scholar] [CrossRef]
- Kim, J.-H.; Song, K.S.; Youn, Y.H.; Lee, Y.C.; Cheon, J.H.; Song, S.Y.; Chung, J.B. Clinicopathologic factors influence accurate endosonographic assessment for early gastric cancer. Gastrointest. Endosc. 2007, 66, 901–908. [Google Scholar] [CrossRef]
- Thosani, N.; Singh, H.; Kapadia, A.; Ochi, N.; Lee, J.H.; Ajani, J.; Swisher, S.G.; Hofstetter, W.L.; Guha, S.; Bhutani, M.S. Diagnostic accuracy of EUS in differentiating mucosal versus submucosal invasion of superficial esophageal cancers: A systematic review and meta-analysis. Gastrointest. Endosc. 2012, 75, 242–253. [Google Scholar] [CrossRef] [PubMed]
- Luo, L.-N.; He, L.-J.; Gao, X.-Y.; Huang, X.-X.; Shan, H.-B.; Luo, G.-Y.; Li, Y.; Lin, S.-Y.; Wang, G.-B.; Zhang, R.; et al. Endoscopic ultrasound for preoperative esophageal squamous cell carcinoma: A meta-analysis. PLoS ONE 2016, 11, e0158373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uberoi, A.S.; Bhutani, M.S. Has the role of EUS in rectal cancer staging changed in the last decade? Endosc. Ultrasound 2018, 7, 366–370. [Google Scholar] [PubMed]
- Tamburrino, D.; Riviere, D.; Yaghoobi, M.; Davidson, B.R.; Gurusamy, K.S. Diagnostic accuracy of different imaging modalities following computed tomography (CT) scanning for assessing the resectability with curative intent in pancreatic and periampullary cancer. Cochrane Database Syst. Rev. 2016, 9, CD011515. [Google Scholar] [CrossRef] [Green Version]
- Gress, F.G.; Hawes, R.H.; Savides, T.J.; Ikenberry, S.O.; Cummings, O.; Kopecky, K.; Sherman, S.; Wiersema, M.; Lehman, G.A. Role of EUS in the preoperative staging of pancreatic cancer: A large single-center experience. Gastrointest. Endosc. 1999, 50, 786–791. [Google Scholar] [CrossRef]
- Ahmad, N.A.; Lewis, J.D.; Ginsberg, G.G.; Rosato, E.F.; Morris, J.B.; Kochman, M.L. EUS in preoperative staging of pancreatic cancer. Gastrointest. Endosc. 2000, 52, 463–468. [Google Scholar] [CrossRef]
- Soriano, A.; Castells, A.; Ayuso, C.; Ayuso, J.R.; de Caralt, M.T.; Ginès, M.A.; Real, M.I.; Gilabert, R.; Quintó, L.; Trilla, A.; et al. Preoperative staging and tumor resectability assessment of pancreatic cancer: Prospective study comparing endoscopic ultrasonography, helical computed tomography, magnetic resonance imaging, and angiography. Am. J. Gastroenterol. 2004, 99, 492–501. [Google Scholar] [CrossRef] [PubMed]
- DeWitt, J.; Devereaux, B.; Chriswell, M.; McGreevy, K.; Howard, T.; Imperiale, T.F.; Ciaccia, D.; Lane, K.A.; Maglinte, D.; Kopecky, K.; et al. Comparison of endoscopic ultrasonography and multidetector computed tomography for detecting and staging pancreatic cancer. Ann. Intern. Med. 2004, 141, 753–763. [Google Scholar] [CrossRef] [Green Version]
- Savides, T.J.; Donohue, M.; Hunt, G.; Al-Haddad, M.; Aslanian, H.; Ben-Menachem, T.; Chen, V.K.; Coyle, W.; Deutsch, J.; DeWitt, J.; et al. EUS-guided FNA diagnostic yield of malignancy in solid pancreatic masses: A benchmark for quality performance measurement. Gastrointest. Endosc. 2007, 66, 277–282. [Google Scholar] [CrossRef]
- Rodrigues-Pinto, E.; Jalaj, S.; Grimm, I.S.; Baron, T.H. Impact of EUS-guided fine-needle biopsy sampling with a new core needle on the need for onsite cytopathologic assessment: A preliminary study. Gastrointest. Endosc. 2016, 84, 1040–1046. [Google Scholar] [CrossRef] [PubMed]
- Attili, F.; Rimbaş, M.; Fantin, A.; Fabbri, C.; Carrara, S.; Di Maurizio, L.; Gibiino, G.; Repici, A.; Inzani, F.; Gasbarrini, A.; et al. Performance of a new histology needle for EUS-guided fine needle biopsy: A retrospective multicenter study. Dig. Liver. Dis. 2018, 50, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Renelus, B.D.; Jamorabo, D.S.; Boston, I.; Briggs, W.M.; Poneros, J.M. Endoscopic ultrasound-guided fine needle biopsy needles provide higher diagnostic yield compared to endoscopic ultrasound-guided fine needle aspiration needles when sampling solid pancreatic lesions: A meta-analysis. Clin. Endosc. 2020. [Google Scholar] [CrossRef] [PubMed]
- Facciorusso, A.; Wani, S.; Triantafyllou, K.; Tziatzios, G.; Cannizzaro, R.; Muscatiello, N.; Singh, S. Comparative accuracy of needle sizes and designs for EUS tissue sampling of solid pancreatic masses: A network meta-analysis. Gastrointest. Endosc. 2019, 90, 893–903. [Google Scholar] [CrossRef] [PubMed]
- Ashat, M.; Klair, J.S.; Rooney, S.L.; Vishal, S.J.; Jensen, C.; Sahar, N.; Murali, A.R.; El-Abiad, R.; Gerke, H. Randomized controlled trial comparing the Franseen needle with the Fork-tip needle for EUS-guided fine-needle biopsy. Gastrointest. Endosc. 2020, 93, 140–150, published online ahead of print. [Google Scholar] [CrossRef]
- Mohan, B.P.; Shakhatreh, M.; Garg, R.; Ponnada, S.; Adler, D.G. Efficacy and safety of EUS-guided liver biopsy: A systematic review and meta-analysis. Gastrointest. Endosc. 2019, 89, 238–246. [Google Scholar] [CrossRef]
- Mok, S.R.S.; Diehl, D.L. The role of EUS in liver biopsy. Curr. Gastroenterol. Rep. 2019, 21, 6. [Google Scholar] [CrossRef]
- Shah, J.N.; Bhat, Y.M.; Hamerski, C.M.; Kane, S.D.; Binmoeller, K.F. Feasibility of nonradiation EUS-based ERCP in patients with uncomplicated choledocholithiasis (with video). Gastrointest. Endosc. 2016, 84, 764–769. [Google Scholar] [CrossRef]
- Zaheer, A.; Anwar, M.M.; Donohoe, C.; O’Keeffe, S.; Mushtaq, H.; Kelleher, B.; Clarke, E.; Kirca, M.; McKiernan, S.; Mahmud, N.; et al. The diagnostic accuracy of endoscopic ultrasound in suspected biliary obstruction and its impact on endoscopic retrograde cholangiopancreatography burden in real clinical practice: A consecutive analysis. Eur. J. Gastroenterol. Hepatol. 2013, 25, 850–857. [Google Scholar] [CrossRef]
- Meeralam, Y.; Al-Shammari, K.; Yaghoobi, M. Diagnostic accuracy of EUS compared with MRCP in detecting choledocholithiasis: A meta-analysis of diagnostic test accuracy in head-to-head studies. Gastrointest. Endosc. 2017, 86, 986–993. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| EUS n = 732 | |
|---|---|
| Age (years), mean (range) | 51.0 (15–92) |
| Gender | |
| Male, n (%) | 284 (38.8%) |
| Female, n (%) | 448 (61.2%) |
| Procedures | |
| Single-session ERCP | 342 (46.7%) |
| Number of FNA/FNB performed, n (%) | 106 (14.5%) |
| Procedure urgency | |
| Elective, n (%) | 364 (49.7%) |
| Urgent, n (%) | 349 (47.7%) |
| Emergent, n (%) | 19 (2.6%) |
| Intervention successful, n (%) | 715 (97.7%) |
| Sedation-related procedure termination, n (%) | 1 (0.1%) |
| Complications | 3 (0.4%) |
| Quality Metric | ||
|---|---|---|
| Study Cohort, %, (n) | ASGE/ACG | |
| Pre-procedure quality metrics | ||
| Performed for indication | 95.8% (701/732) | >80% |
| Prophylactic antibiotics for FNA of cyst | 100% (14/14) | >98% |
| Intra-procedure quality metrics | ||
| Photo or video documentation | 97.5% (714/732) | N/A |
| Documentation of sedation-related events | 100% (732/732) | >98% |
| Documentation of appropriate structures | 100% (732/732) | >98% |
| Staging by AJCC | 100% (91/91) | >98% |
| Diagnostic rate of adequate sample in all solid lesion sampling | 87.9% (80/91) | ≥85% |
| Diagnostic rate for malignancy, FNA/FNB of pancreatic mass | 75.8% (25/33) | ≥70% |
| Sensitivity for malignancy, FNA/FNB of pancreatic mass | 96.2% (25/26) | ≥85% |
| Post-procedure quality metrics | ||
| Plan for specimen follow-up | 100% (106/106) | >98% |
| Indication | %, (n) |
|---|---|
| Benign | 62.7% (459/732) |
| Stone | 44.7% (327/732) |
| Pancreatitis | 6.4% (47/732) |
| Biliary tree | 5.2% (38/732) |
| Liver | 2.6% (19/732) |
| Abscess | 1.2% (9/732) |
| Incontinence | 1.0% (7/732) |
| Other | 1.6% (12/732) |
| Malignancy | 37.3% (273/732) |
| Gastric | 9.0% (66/732) |
| Pancreatic mass | 8.3% (61/732) |
| Rectal | 6.6% (48/732) |
| Pancreatic cyst | 3.3% (24/732) |
| Esophageal | 2.9% (21/732) |
| Biliary tree | 2.9% (21/732) |
| Extraluminal | 2.0% (15/732) |
| Small bowel | 1.9% (14/732) |
| Mediastinum | 0.4% (3/732) |
| Detection Rate, %, (n) | Sensitivity, %, (n) | Sample Adequacy, %, (n) | |
|---|---|---|---|
| Overall | 75.8% (25/33) | 96.2% (25/26) | 90.9% (30/33) |
| 1st collection period predominantly FNA | 46.2% (6/13) | 85.7% (6/7) | 76.9% (10/13) |
| 2nd collection period predominantly FNB | 95.0% (19/20) | 100.0% (19/19) | 100.0% (20/20) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ku, L.; Hou, L.A.; Eysselein, V.E.; Reicher, S. Endoscopic Ultrasound Quality Metrics in Clinical Practice. Diagnostics 2021, 11, 242. https://doi.org/10.3390/diagnostics11020242
Ku L, Hou LA, Eysselein VE, Reicher S. Endoscopic Ultrasound Quality Metrics in Clinical Practice. Diagnostics. 2021; 11(2):242. https://doi.org/10.3390/diagnostics11020242
Chicago/Turabian StyleKu, Lawrence, Linda A. Hou, Viktor E. Eysselein, and Sofiya Reicher. 2021. "Endoscopic Ultrasound Quality Metrics in Clinical Practice" Diagnostics 11, no. 2: 242. https://doi.org/10.3390/diagnostics11020242