
Choroidal Vascularity Features in Patients with Choroideremia and Cystoid Spaces


 , ,
, , 

Abstract
1. Introduction
2. Methods
2.1. Patients and Clinical Examination
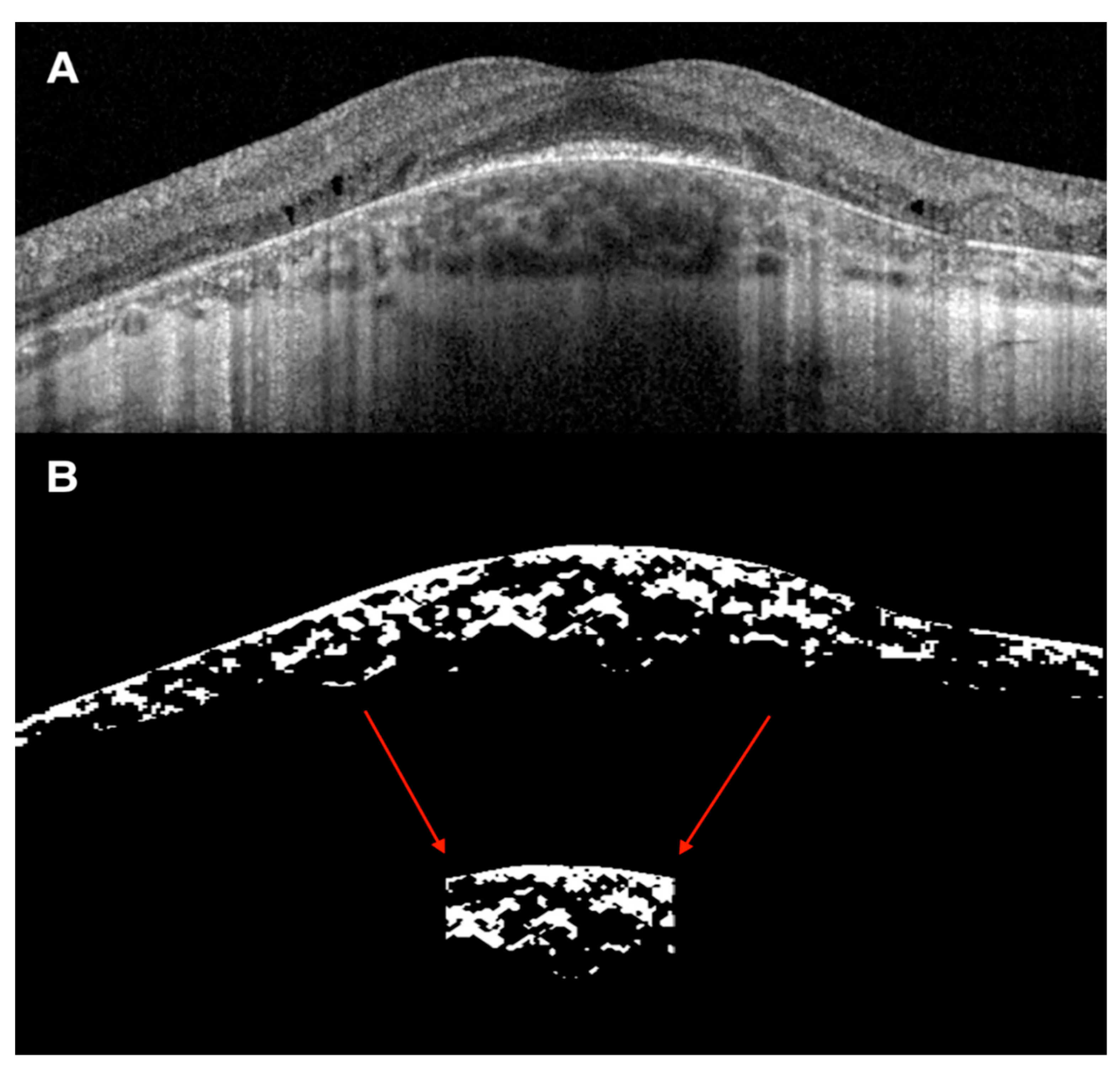
2.2. OCT Analysis of the Retina and Choroid
2.3. Statistical Analysis
3. Results
OCT Analysis of the Retina and Choroid
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mitsios, A.; Dubis, A.M.; Moosajee, M. Choroideremia: From genetic and clinical phenotyping to gene therapy and future treatments. Ther. Adv. Ophthalmol. 2018, 10, 2515841418817490. [Google Scholar] [CrossRef]
- Aleman, T.S.; Han, G.; Serrano, L.W.; Fuerst, N.M.; Charlson, E.S.; Pearson, D.J.; Chung, D.C.; Traband, A.; Pan, W.; Ying, G.S.; et al. Natural History of the Central Structural Abnormalities in Choroideremia: A Prospective Cross-Sectional Study. Ophthalmology 2017, 124, 359–373. [Google Scholar] [CrossRef] [PubMed]
- Sorsby, A.; Franceschetti, A.; Joseph, B.R.; Davey, J.B. Choroideremia: Clinical and genetic aspects. Br. J. Ophthalmol. 1952, 36, 547–581. [Google Scholar] [CrossRef]
- Xue, K.; Oldani, M.; Jolly, J.K.; Edwards, T.L.; Groppe, M.; Downes, S.M.; Maclaren, R.E. Correlation of optical coherence tomography and autofluorescence in the outer retina and choroid of patients with choroideremia. Investig. Ophthalmol. Vis. Sci. 2016, 57, 3674–3684. [Google Scholar] [CrossRef] [PubMed]
- Heon, E.; Alabduljalil, T.; McGuigan, D.B.; Cideciyan, A.V.; Li, S.; Chen, S.; Jacobson, S.G. Visual function and central retinal structure in choroideremia. Investig. Ophthalmol. Vis. Sci. 2016, 57, OCT377–OCT387. [Google Scholar] [CrossRef] [PubMed]
- Di Iorio, V.; Esposito, G.; De Falco, F.; Boccia, R.; Fioretti, T.; Colucci, R.; De Rosa, G.; Melillo, P.; Salvatore, F.; Simonelli, F.; et al. CHM/REP1 transcript expression and loss of visual function in patients affected by choroideremia. Investig. Ophthalmol. Vis. Sci. 2019, 60, 1547–1555. [Google Scholar] [CrossRef]
- Genead, M.A.; Fishman, G.A. Cystic macular oedema on spectral-domain optical coherence tomography in choroideremia patients without cystic changes on fundus examination. Eye 2011, 25, 84–90. [Google Scholar] [CrossRef]
- Murro, V.; Mucciolo, D.P.; Giorgio, D.; Sodi, A.; Passerini, I.; Bacci, G.; Bargiacchi, S.; Virgili, G.; Rizzo, S. Optical coherence tomography (OCT) features of cystoid spaces in choroideremia (CHM). Graefe’s Arch. Clin. Exp. Ophthalmol. 2019, 257, 2655–2663. [Google Scholar] [CrossRef]
- Agrawal, R.; Ding, J.; Sen, P.; Rousselot, A.; Chan, A.; Nivison-Smith, L.; Wei, X.; Mahajan, S.; Kim, R.; Mishra, C.; et al. Exploring choroidal angioarchitecture in health and disease using choroidal vascularity index. Prog. Retin. Eye Res. 2020, 77, 100829. [Google Scholar] [CrossRef]
- Iovino, C.; Pellegrini, M.; Bernabei, F.; Borrelli, E.; Sacconi, R.; Govetto, A.; Vagge, A.; Di Zazzo, A.; Forlini, M.; Finocchio, L.; et al. Choroidal Vascularity Index: An In-Depth Analysis of This Novel Optical Coherence Tomography Parameter. J. Clin. Med. 2020, 9, 595. [Google Scholar] [CrossRef]
- Murro, V.; Mucciolo, D.P.; Giorgio, D.; Passerini, I.; Cipollini, F.; Virgili, G.; Giansanti, F.; Sodi, A. Choroidal Vascularity Index in young Choroideremia patients. Retina 2020. [Google Scholar] [CrossRef] [PubMed]
- Iovino, C.; Au, A.; Hilely, A.; Violanti, S.; Peiretti, E.; Gorin, M.B.; Sarraf, D. Evaluation of the Choroid in Eyes With Retinitis Pigmentosa and Cystoid Macular Edema. Investig. Opthalmol. Vis. Sci. 2019, 60, 5000–5006. [Google Scholar] [CrossRef] [PubMed]
- Esposito, G.; De Falco, F.; Tinto, N.; Testa, F.; Vitagliano, L.; Tandurella, I.C.M.; Iannone, L.; Rossi, S.; Rinaldi, E.; Simonelli, F.; et al. Comprehensive mutation analysis (20 families) of the choroideremia gene reveals a missense variant that prevents the binding of REP1 with rab geranylgeranyl transferase. Hum. Mutat. 2011, 32, 1460–1469. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, R.; Wei, X.; Goud, A.; Vupparaboina, K.K.; Jana, S.; Chhablani, J. Influence of scanning area on choroidal vascularity index measurement using optical coherence tomography. Acta Ophthalmol. 2017, 95, e770–e775. [Google Scholar] [CrossRef]
- Rasheed, M.A.; Sahoo, N.K.; Goud, A.; Vupparaboina, K.K.; Chhablani, J. Qualitative comparison of choroidal vascularity measurement algorithms. Indian J. Ophthalmol. 2018, 66, 1785–1789. [Google Scholar]
- Iovino, C.; Au, A.; Chhablani, J.; Parameswarappa, D.C.; Rasheed, M.A.; Cennamo, G.; Cennamo, G.; Montorio, D.; Ho, A.C.; Xu, D.; et al. Choroidal Anatomic Alterations After Photodynamic Therapy for Chronic Central Serous Chorioretinopathy: A Multicenter Study. Am. J. Ophthalmol. 2020, 217, 104–113. [Google Scholar] [CrossRef]
- Iovino, C.; Chhablani, J.; Rasheed, M.A.; Tatti, F.; Bernabei, F.; Pellegrini, M.; Giannaccare, G.; Peiretti, E. Effects of different mydriatics on the choroidal vascularity in healthy subjects. Eye 2020. [Google Scholar] [CrossRef]
- Salvatore, S.; Fishman, G.A.; Genead, M.A. Treatment of cystic macular lesions in hereditary retinal dystrophies. Surv. Ophthalmol. 2013, 58, 560–584. [Google Scholar] [CrossRef]
- Khan, K.N.; Islam, F.; Moore, A.T.; Michaelides, M. Clinical and Genetic Features of Choroideremia in Childhood. Ophthalmology 2016, 123, 2158–2165. [Google Scholar] [CrossRef]
- Pellegrini, M.; Bernabei, F.; Mercanti, A.; Sebastiani, S.; Peiretti, E.; Iovino, C.; Casini, G.; Loiudice, P.; Scorcia, V.; Giannaccare, G. Short-term choroidal vascular changes after aflibercept therapy for neovascular age-related macular degeneration. Graefe’s Arch. Clin. Exp. Ophthalmol. 2020. [Google Scholar] [CrossRef]
- Giannaccare, G.; Pellegrini, M.; Sebastiani, S.; Bernabei, F.; Moscardelli, F.; Iovino, C.; Napoli, P.E.; Campos, E. Choroidal vascularity index quantification in geographic atrophy using binarization of enhanced-depth imaging optical coherence tomographic scans. Retina 2020, 40, 960–965. [Google Scholar] [CrossRef]
- Wei, X.; Mishra, C.; Kannan, N.B.; Holder, G.E.; Khandelwal, N.; Kim, R.; Agrawal, R. Choroidal structural analysis and vascularity index in retinal dystrophies. Acta Ophthalmol. 2019, 97, e116–e121. [Google Scholar] [CrossRef] [PubMed]
- Makiyama, Y.; Oishi, A.; Otani, A.; Ogino, K.; Nakagawa, S.; Kurimoto, M.; Yoshimura, N. Prevalence and spatial distribution of cystoid spaces in retinitis pigmentosa: Investigation with spectral domain optical coherence tomography. Retina 2014, 34, 981–988. [Google Scholar] [CrossRef]
- Sergouniotis, P.I.; Davidson, A.E.; Lenassi, E.; Devery, S.R.; Moore, A.T.; Webster, A.R. Retinal structure, function, and molecular pathologic features in gyrate atrophy. Ophthalmology 2012, 119, 596–605. [Google Scholar] [CrossRef]
- Murro, V.; Mucciolo, D.P.; Sodi, A.; Passerini, I.; Giorgio, D.; Virgili, G.; Rizzo, S. Novel clinical findings in autosomal recessive NR2E3-related retinal dystrophy. Graefe’s Arch. Clin. Exp. Ophthalmol. 2019, 257, 9–22. [Google Scholar] [CrossRef]
- Goldberg, N.R.; Greenberg, J.P.; Laud, K.; Tsang, S.; Freund, K.B. Outer retinal tubulation in degenerative retinal disorders. Retina 2013, 33, 1871–1876. [Google Scholar] [CrossRef]
- Dolz-Marco, R.; Litts, K.M.; Tan, A.C.S.; Freund, K.B.; Curcio, C.A. The Evolution of Outer Retinal Tubulation, a Neurodegeneration and Gliosis Prominent in Macular Diseases. Ophthalmology 2017, 124, 1353–1367. [Google Scholar] [CrossRef]
- Mandadi, S.K.R.; Iovino, C.; Sacconi, R.; Querques, G.; Peiretti, E.; Singh, S.R.; Chhablani, J. Outer retinal tubulations in central serous chorioretinopathy associated with choroidal neovascularisation. Eur. J. Ophthalmol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Ganesh, A.; Stroh, E.; Manayath, G.J.; Al-Zuhaibi, S.; Levin, A.V. Macular cysts in retinal dystrophy. Curr. Opin. Ophthalmol. 2011, 22, 332–339. [Google Scholar] [CrossRef]
- Jiramongkolchai, K.; Bhatti, M.T.; Proia, A.; Freedman, S.F.; El-Dairi, M.A. Formation of macular inner nuclear layer cysts in optic atrophy. Investig. Ophthalmol. Vis. Sci. 2016, 57, 989–991. [Google Scholar] [CrossRef] [PubMed]
- Hirakawa, H.; Iijima, H.; Gohdo, T.; Tsukahara, S. Optical coherence tomography of cystoid macular edema associated with retinitis pigmentosa. Am. J. Ophthalmol. 1999, 128, 185–191. [Google Scholar] [CrossRef]
- Wolfensberger, T.J.; Mahieu, I.; Jarvis-Evans, J.; Boulton, M.; Carter, N.D.; Nogradi, A.; Hollande, E.; Bird, A.C. Membrane-bound carbonic anhydrase in human retinal pigment epithelium. Investig. Ophthalmol. Vis. Sci. 1994, 35, 3401–3407. [Google Scholar]
- Moldow, B.; Sander, B.; Larsen, M.; Lund-Andersen, H. Effects of acetazolamide on passive and active transport of fluorescein across the normal BRB. Investig. Ophthalmol. Vis. Sci. 1999, 40, 1770–1775. [Google Scholar]
- Testa, F.; Di Iorio, V.; Gallo, B.; Marchese, M.; Nesti, A.; De Rosa, G.; Melillo, P.; Simonelli, F. Carbonic anhydrase inhibitors in patients with X-linked retinoschisis: Effects on macular morphology and function. Ophthalmic Genet. 2019, 40, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Genead, M.A.; McAnany, J.J.; Fishman, G.A. Topical dorzolamide for treatment of cystoid macular edema in patients with choroideremia. Retina 2012, 32, 826–833. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| ID | Presence of Cystoid Spaces | CHM Pathogenic Variant (NM_000390.3; NP_000381.1) |
|---|---|---|
| P1 | YES | c.940 + 1G > T |
| P2 | YES | c.1-?_*3450+?del |
| P3 | YES | c.1520A > G (p.His507Arg) |
| P4 | YES | Deletion encompassing exons 6 and 7 |
| P5 | YES | c.1414-?_1510+?del |
| P6 | YES | c.1414-?_1510+?del |
| P7 | YES | c.1166 + 1G > C |
| P8 | YES | c.1166 + 1G > C |
| P9 | YES | c.315_318del (p.Ser105Argfs) |
| P10 | YES | c.580_581ins (p.Asp184Glufs) |
| P11 | YES | c.1029delG (p.Met343llefs) |
| P12 | YES | c.106 + 1G > T (p.Gly17Glufs37*) |
| P13 | YES | c.877C > T (p.Arg293*) |
| P14 | YES | c.877C > T (p.Arg293*) |
| P15 | YES | c.1651delTACTT |
| P16 | YES | c.(?_49 + 1)_(1609 + 1_1610-1)del |
| P17 | YES | c.877C > T (p.Arg293*) |
| P18 | NO | Deletion encompassing exons 6 and 7 |
| P19 | NO | Deletion encompassing exons 6 and 7 |
| P20 | NO | c.525_526del(p.Glu177Lysfs) |
| P21 | NO | c.580_581ins (p.Asp184Glufs) |
| P22 | NO | c.941-2A > G |
| P23 | NO | c.969T > A (p.Tyr323*) |
| P24 | NO | c.808C > T(p.Arg270*) |
| P25 | NO | c.969T > A (p.Tyr323*) |
| P26 | NO | c.(?_49 + 1)_(1609 + 1_1610-1)del |
| P27 | NO | c.1350-1G > A |
| P28 | NO | c.969T > A (p.Tyr323*) |
| P29 | NO | c.820-2A > G |
| P30 | NO | c.1245-?_1962 + del*(p.Cys416*) |
| P31 | NO | c.31S_318del, p. Ser10Sfs |
| P32 | NO | c.315_318del |
| P33 | NO | c.1029delG (p.Met343llefs) |
| CHM Eyes with CSs (n = 17) | CHM Eyes without CSs (n = 16) | p-Value | B–H Adjusted α | |
|---|---|---|---|---|
| Age (Avg ± STD) | 37.3 ± 11.6 | 31.4 ± 16.7 | 0.25 | 0.020 |
| BCVA (LogMAR, Avg ± STD) | 0.11 ± 0.20 | 0.20 ± 0.57 | 0.54 | 0.043 |
| Central macular thickness (μm, Avg ± STD) | 272.3 ± 57.7 | 232.1 ± 69.3 | 0.08 | 0.007 |
| Sub-foveal choroidal thickness (μm, Avg ± STD) | 187.9 ± 71.9 | 215.6 ± 67.9 | 0.26 | 0.023 |
| Ellipsoid zone integrity in the foveal region (#, %) | 8 (47.1%) | 12 (75.0%) | 0.16 | 0.013 |
| External limiting membrane integrity in the foveal region (#, %) | 11 (64.7%) | 12 (75.0%) | 0.71 | 0.050 |
| Tubulation (#, %) | 17 (100%) | 11 (68.7%) | 0.02 | 0.003 |
| Choroidal Parameters for the Total 6 mm Scan | CHM Eyes With CSs (n = 17) | CHM Eyes Without CSs (n = 16) | p-Value | B–H Adjusted α |
|---|---|---|---|---|
| Choroidal Vascularity Index (%, Avg ± STD) | 68.1 ± 4.4 | 66.4 ± 4.0 | 0.28 | 0.034 |
| Total Choroidal Area for (mm2, Avg ± STD) | 0.89 ± 0.43 | 1.09 ± 0.59 | 0.28 | 0.030 |
| Luminal Choroidal Area (mm2, Avg ± STD) | 0.61 ± 0.29 | 0.71 ± 0.38 | 0.36 | 0.037 |
| Stromal Choroidal Area (mm2, Avg ± STD) | 0.29 ± 0.15 | 0.37 ± 0.22 | 0.21 | 0.017 |
| Choroidal Parameters for the 1500 μm under the fovea | ||||
| Choroidal Vascularity Index (%, Avg ± STD) | 70.4 ± 6.1 | 67.4 ± 5.0 | 0.14 | 0.010 |
| Total Choroidal Area for (mm2, Avg ± STD) | 0.28 ± 0.13 | 0.31 ± 0.15 | 0.61 | 0.047 |
| Luminal Choroidal Area (mm2, Avg ± STD) | 0.18 ± 0.09 | 0.2 ± 0.1 | 0.52 | 0.040 |
| Stromal Choroidal Area (mm2, Avg ± STD) | 0.08 ± 0.05 | 0.1 ± 0.06 | 0.26 | 0.024 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iovino, C.; Di Iorio, V.; Testa, F.; Bombace, V.; Melillo, P.; Vupparaboina, K.K.; Chhablani, J.; Simonelli, F. Choroidal Vascularity Features in Patients with Choroideremia and Cystoid Spaces. Diagnostics 2021, 11, 382. https://doi.org/10.3390/diagnostics11030382
Iovino C, Di Iorio V, Testa F, Bombace V, Melillo P, Vupparaboina KK, Chhablani J, Simonelli F. Choroidal Vascularity Features in Patients with Choroideremia and Cystoid Spaces. Diagnostics. 2021; 11(3):382. https://doi.org/10.3390/diagnostics11030382
Chicago/Turabian StyleIovino, Claudio, Valentina Di Iorio, Francesco Testa, Viviana Bombace, Paolo Melillo, Kiran Kumar Vupparaboina, Jay Chhablani, and Francesca Simonelli. 2021. "Choroidal Vascularity Features in Patients with Choroideremia and Cystoid Spaces" Diagnostics 11, no. 3: 382. https://doi.org/10.3390/diagnostics11030382
APA StyleIovino, C., Di Iorio, V., Testa, F., Bombace, V., Melillo, P., Vupparaboina, K. K., Chhablani, J., & Simonelli, F. (2021). Choroidal Vascularity Features in Patients with Choroideremia and Cystoid Spaces. Diagnostics, 11(3), 382. https://doi.org/10.3390/diagnostics11030382