
Ethical Implications of Alzheimer’s Disease Prediction in Asymptomatic Individuals through Artificial Intelligence


Abstract
:1. Introduction
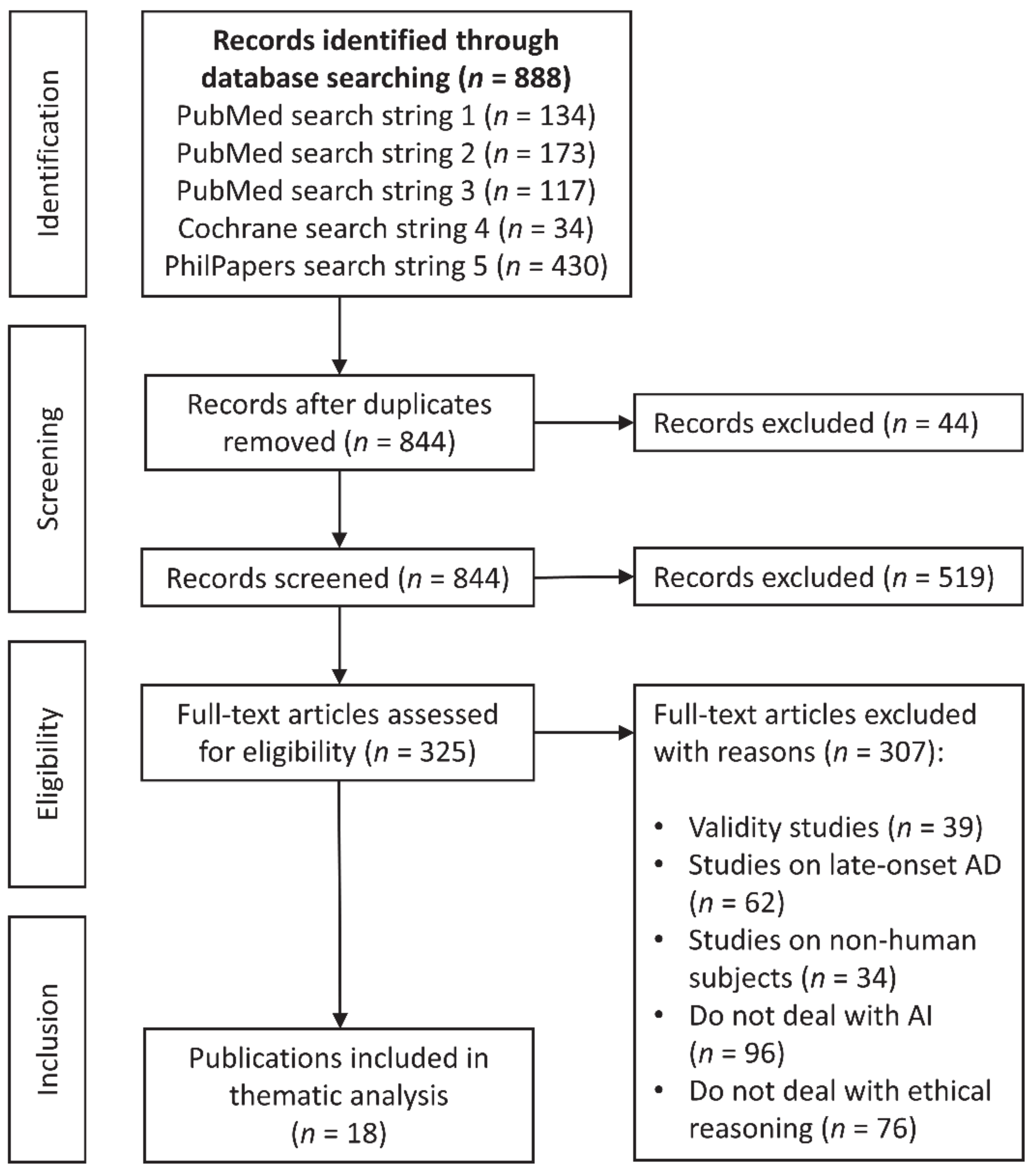
2. Materials and Methods
3. Results
3.1. Individual Benefits and Disadvantages
3.2. Social Benefits and Disadvantages
3.3. Right to Know vs. Right Not to Know
4. Discussion
- The test should be voluntary and based on informed consent.
- The test should be offered with proper counseling and professional support.
- The test should only be available to mature adults.
- The test results should not cause discrimination.
- Testing should be delayed if there is evidence that the results will lead to psychosocial harm.
- The test results are confidential and the property of the individual.
4.1. Autonomy
4.2. Beneficence
4.3. Non-Maleficence
4.4. Justice
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Towards a Dementia Plan. A WHO Guide; World Health Organization: Geneva, Switzerland, 2018; ISBN 978-92-4-151413-2. [Google Scholar]
- World Health Organization. Dementia. Available online: https://www.who.int/en/news-room/fact-sheets/detail/dementia (accessed on 25 February 2020).
- Graham, S.A.; Lee, E.E.; Jeste, D.V.; van Patten, R.; Twamley, E.W.; Nebeker, C.; Yamada, Y.; Kim, H.-C.; Depp, C.A. Artificial intelligence approaches to predicting and detecting cognitive decline in older adults: A conceptual review. Psychiatry Res. 2020, 284, 112732. [Google Scholar] [CrossRef] [Green Version]
- Uspenskaya-Cadoz, O.; Alamuri, C.; Wang, L.; Yang, M.; Khinda, S.; Nigmatullina, Y.; Cao, T.; Kayal, N.; O’Keefe, M.; Rubel, C. Machine Learning Algorithm Helps Identify Non-Diagnosed Prodromal Alzheimer’s Disease Patients in the General Population. J. Prev. Alzheimers. Dis. 2019, 6, 185–191. [Google Scholar] [CrossRef]
- Bazzari, F.H.; Abdallah, D.M.; El-Abhar, H.S. Pharmacological Interventions to Attenuate Alzheimer’s Disease Progression: The Story So Far. Curr. Alzheimer Res. 2019, 16, 261–277. [Google Scholar] [CrossRef]
- Cummings, J.; Lee, G.; Ritter, A.; Zhong, K. Alzheimer’s disease drug development pipeline: 2018. Alzheimer’s Dement. 2018, 4, 195–214. [Google Scholar] [CrossRef] [PubMed]
- Bruun, M.; Frederiksen, K.S.; Rhodius-Meester, H.F.M.; Baroni, M.; Gjerum, L.; Koikkalainen, J.; Urhemaa, T.; Tolonen, A.; Van Gils, M.; Rueckert, D.; et al. Impact of a clinical decision support tool on prediction of progression in early-stage dementia: A prospective validation study. Alzheimer’s Res. Ther. 2019, 11, 25. [Google Scholar] [CrossRef]
- Laske, C.; Sohrabi, H.R.; Frost, S.M.; López-de-Ipiña, K.; Garrard, P.; Buscema, M.; Dauwels, J.; Soekadar, S.R.; Mueller, S.; Linnemann, C.; et al. Innovative diagnostic tools for early detection of Alzheimer’s disease. Alzheimer’s Dement. 2015, 11, 561–578. [Google Scholar] [CrossRef]
- Gautam, R.; Sharma, M. Prevalence and Diagnosis of Neurological Disorders Using Different Deep Learning Techniques: A Meta-Analysis. J. Med. Syst. 2020, 44, 49. [Google Scholar] [CrossRef]
- Ding, Y.; Sohn, J.H.; Kawczynski, M.G.; Trivedi, H.; Harnish, R.; Jenkins, N.W.; Lituiev, D.; Copeland, T.P.; Aboian, M.S.; Mari Aparici, C.; et al. A Deep Learning Model to Predict a Diagnosis of Alzheimer Disease by Using 18F-FDG PET of the Brain. Radiology 2019, 290, 456–464. [Google Scholar] [CrossRef] [PubMed]
- Spasov, S.; Passamonti, L.; Duggento, A.; Liò, P.; Toschi, N. A parameter-efficient deep learning approach to predict conversion from mild cognitive impairment to Alzheimer’s disease. Neuroimage 2019, 189, 276–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitehouse, P.J. Ethical issues in early diagnosis and prevention of Alzheimer disease. Dialogues Clin. Neurosci. 2019, 21, 101–108. [Google Scholar]
- Dubois, B.; Padovani, A.; Scheltens, P.; Rossi, A.; Dell’Agnello, G. Timely Diagnosis for Alzheimer’s Disease: A Literature Review on Benefits and Challenges. J. Alzheimer’s Dis. 2016, 49, 617–631. [Google Scholar] [CrossRef] [Green Version]
- Lane, C.A.; Hardy, J.; Schott, J.M. Alzheimer’s disease. Eur. J. Neurol. 2018, 25, 59–70. [Google Scholar] [CrossRef]
- Frisoni, G.B.; Boccardi, M.; Barkhof, F.; Blennow, K.; Cappa, S.; Chiotis, K.; Démonet, J.-F.; Garibotto, V.; Giannakopoulos, P.; Gietl, A.; et al. Strategic roadmap for an early diagnosis of Alzheimer’s disease based on biomarkers. Lancet Neurol. 2017, 16, 661–676. [Google Scholar] [CrossRef] [Green Version]
- Bundesärztekammer. Stellungnahme zum Umgang mit prädiktiven Tests auf das Risiko für die Alzheimer Krankheit. Dtsch. Arztebl. Ausg. A 2018, 115. [Google Scholar] [CrossRef]
- Topol, E.J. Welcoming new guidelines for AI clinical research. Nat. Med. 2020, 26, 1318–1320. [Google Scholar] [CrossRef] [PubMed]
- Schicktanz, S.; Perry, J.; Herten, B.; Stock Gissendanner, S. Demenzprädiktion als ethische Herausforderung: Stakeholder fordern Beratungsstandards für Deutschland. Nervenarzt 2021, 92, 66–68. [Google Scholar] [CrossRef] [PubMed]
- Smedinga, M.; Tromp, K.; Schermer, M.H.N.; Richard, E. Ethical Arguments Concerning the Use of Alzheimer’s Disease Biomarkers in Individuals with No or Mild Cognitive Impairment: A Systematic Review and Framework for Discussion. J. Alzheimer’s Dis. 2018, 66, 1309–1322. [Google Scholar] [CrossRef] [Green Version]
- Schweda, M.; Kögel, A.; Bartels, C.; Wiltfang, J.; Schneider, A.; Schicktanz, S. Prediction and Early Detection of Alzheimer’s Dementia: Professional Disclosure Practices and Ethical Attitudes. J. Alzheimer’s Dis. 2018, 62, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Ells, C.; Thombs, B.D. The ethics of how to manage incidental findings. Can. Med Assoc. J. 2014, 186, 655–656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franceschini, N.; Frick, A.; Kopp, J.B. Genetic Testing in Clinical Settings. Am. J. Kidney Dis. 2018, 72, 569–581. [Google Scholar] [CrossRef]
- Clarke, A.J.; Wallgren-Pettersson, C. Ethics in genetic counselling. J. Community Genet. 2018, 10, 3–33. [Google Scholar] [CrossRef] [Green Version]
- Bunnik, E.M.; Vernooij, M.W. Incidental findings in population imaging revisited. Eur. J. Epidemiol. 2016, 31, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erdmann, P.; Langanke, M.; Assel, H. Zufallsbefunde-Risikobewusstsein von Probanden und forschungsethische Konsequenzen. In Medizin und Technik: Risiken und Folgen technologischen Fortschritts; Steger, F., Ed.; Mentis: Münster, Germany, 2013; pp. 15–47. [Google Scholar]
- Quaid, K.A.; Murrell, J.R.; Hake, A.M.; Farlow, M.R.; Ghetti, B. Presymptomatic Genetic Testing with an APP Mutation in Early-Onset Alzheimer Disease: A Descriptive Study of Sibship Dynamics. J. Genet. Couns. 2000, 9, 327–341. [Google Scholar] [CrossRef] [PubMed]
- Arribas-Ayllon, M. The ethics of disclosing genetic diagnosis for Alzheimer’s disease: Do we need a new paradigm? Br. Med. Bull. 2011, 100, 7–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldman, J.S.; Hou, C.E. Early-onset Alzheimer disease: When is genetic testing appropriate? Alzheimer Dis. Assoc. Disord. 2004, 18, 65–67. [Google Scholar] [CrossRef]
- Beauchamp, T.L.; Childress, J.F. Principles of Biomedical Ethics, 8th ed.; Oxford University Press: New York, NY, USA, 2019; ISBN 9780190640873. [Google Scholar]
- Vanderschaeghe, G.; Dierickx, K.; Vandenberghe, R. Review of the Ethical Issues of a Biomarker-Based Diagnoses in the Early Stage of Alzheimer’s Disease. J. Bioethical Inq. 2018, 15, 219–230. [Google Scholar] [CrossRef] [PubMed]
- Angehrn, Z.; Sostar, J.; Nordon, C.; Turner, A.; Gove, D.; Karcher, H.; Keenan, A.; Mittelstadt, B.; Reydet-de Vulpillieres, F. Ethical and Social Implications of Using Predictive Modeling for Alzheimer’s Disease Prevention: A Systematic Literature Review. J. Alzheimer’s Dis. 2020, 76, 923–940. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Strech, D.; Sofaer, N. How to write a systematic review of reasons. J. Med. Ethics 2012, 38, 121–126. [Google Scholar] [CrossRef] [Green Version]
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs. Health Sci. 2013, 15, 398–405. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Davis, D.S. Ethical issues in Alzheimer’s disease research involving human subjects. J. Med. Ethics 2017, 43, 852–856. [Google Scholar] [CrossRef] [PubMed]
- Erdmann, P.; Langanke, M. The Ambivalence of Early Diagnosis-Returning Results in Current Alzheimer Research. Curr. Alzheimer Res. 2018, 15, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Schermer, M.H.N.; Richard, E. On the reconceptualization of Alzheimer’s disease. Bioethics 2019, 33, 138–145. [Google Scholar] [CrossRef] [Green Version]
- Ivanoiu, A.; Engelborghs, S.; Hanseeuw, B. Early diagnosis of Alzheimer’s disease (with the announcement of the diagnosis). Rev. Prat. 2020, 70, 158–163. [Google Scholar] [PubMed]
- Vanderschaeghe, G.; Vandenberghe, R.; Dierickx, K. Stakeholders’ Views on Early Diagnosis for Alzheimer’s Disease, Clinical Trial Participation and Amyloid PET Disclosure: A Focus Group Study. J. Bioethical Inq. 2019, 16, 45–59. [Google Scholar] [CrossRef] [PubMed]
- Hughes, J.C.; Ingram, T.A.; Jarvis, A.; Denton, E.; Lampshire, Z.; Wernham, C. Consent for the diagnosis of preclinical dementia states: A review. Maturitas 2017, 98, 30–34. [Google Scholar] [CrossRef] [Green Version]
- Bortolotti, L.; Widdows, H. The right not to know: The case of psychiatric disorders. J. Med. Ethics 2011, 37, 673–676. [Google Scholar] [CrossRef] [Green Version]
- Mattsson, N.; Brax, D.; Zetterberg, H. To Know or Not to Know-Ethical Issues Related to Early Diagnosis of Alzheimer’s Disease. Int. J. Alzheimer’s Dis. 2010, 2010, 841941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebrahimighahnavieh, A.; Luo, S.; Chiong, R. Deep learning to detect Alzheimer’s disease from neuroimaging: A systematic literature review. Comput. Methods Programs Biomed. 2019, 187, 105242. [Google Scholar] [CrossRef]
- Stites, S.D.; Milne, R.; Karlawish, J. Advances in Alzheimer’s imaging are changing the experience of Alzheimer’s disease. Alzheimer’s Dement. 2018, 10, 285–300. [Google Scholar] [CrossRef]
- Milne, R.; Karlawish, J. Expanding engagement with the ethical implications of changing definitions of Alzheimer’s disease. Lancet Psychiatry 2017, 4, e6–e7. [Google Scholar] [CrossRef] [Green Version]
- World Federation of Neurology Research Group on Huntington’s Disease. Guidelines for the molecular genetics predictive test in Huntington’s disease. J. Med Genet. 1994, 31, 555–559. [Google Scholar]
- Kerwin, A. None Too Solid. Knowl. Creat. Diffus. Util. 1993, 15, 166–185. [Google Scholar] [CrossRef]
- Kraft, T.; Rott, H. Was ist Nichtwissen. In Das sogenannte Recht auf Nichtwissen: Normatives Fundament und anwendungspraktische Geltungskraft; Duttge, G., Lenk, C., Eds.; Mentis: Paderborn, Germany, 2019; pp. 21–48. ISBN 3957431344. [Google Scholar]
- Beauchamp, T.L. The ‘Four Principles’ Approach to Health Care Ethics. In Principles of Health Care Ethics, 2nd ed.; Ashcroft, R.E., Dawson, A., Draper, H., McMillan, J., Eds.; John Wiley & Sons: Chichester, UK; Hoboken, NJ, USA, 2007; pp. 3–10. ISBN 9780470842461. [Google Scholar]
- Bonotti, M. Food labels, autonomy, and the right (not) to know. Kennedy Inst. Ethics J. 2014, 24, 301–321. [Google Scholar] [CrossRef] [PubMed]
- Andorno, R. Foundations and implications of the right not to know. In Das sogenannte Recht auf Nichtwissen: Normatives Fundament und anwendungspraktische Geltungskraft; Duttge, G., Lenk, C., Eds.; Mentis: Paderborn, Germany, 2019; pp. 69–81. ISBN 3957431344. [Google Scholar]
- Cornett, P.F.; Hall, J.R. Issues in disclosing a diagnosis of dementia. Arch. Clin. Neuropsychol. 2008, 23, 251–256. [Google Scholar] [CrossRef] [Green Version]
- Smith, A.P.; Beattie, B.L. Disclosing a Diagnosis of Alzheimer’s Disease: Patient and Family Experiences. Can. J. Neurol. Sci. 2001, 28, S67–S71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lenk, C.; Duttge, G.; Flatau, L.; Frommeld, D.; Poser, W.; Reitt, M.; Schulze, T.; Weber, A.; Zoll, B. A look into the future? Patients’ and health care staff’s perception and evaluation of genetic information and the right not to know. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2019, 180, 576–588. [Google Scholar] [CrossRef]
- Jha, A.; Tabet, N.; Orrell, M. To tell or not to tell-comparison of older patients’ reaction to their diagnosis of dementia and depression. Int. J. Geriatr. Psychiatry 2001, 16, 879–885. [Google Scholar] [CrossRef]
- Davies, B. The right not to know and the obligation to know. J. Med. Ethics 2020, 300–303. [Google Scholar] [CrossRef]
- Porteri, C.; Galluzzi, S.; Geroldi, C.; Frisoni, G.B. Diagnosis disclosure of prodromal Alzheimer disease-ethical analysis of two cases. Can. J. Neurol. Sci. 2010, 37, 67–75. [Google Scholar] [CrossRef] [Green Version]
- Marzban, E.N.; Teipel, S.J.; Buerger, K.; Fliessbach, K.; Heneka, M.T.; Kilimann, I.; Laske, C.; Peters, O.; Priller, J.; Schneider, A.; et al. P3-361: Explainable Convolutional Networks and multimodal Imaging Data: The next Step towards using Artificial Intelligence as diagnostic Tool for early Detection of Alzheimer’s Disease. Alzheimer’s Dement. 2019, 15, P1083–P1084. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. In Proposed Regulatory Framework for Modifications to Artificial Intelligence/Machine Learning (AI/ML)-Based Software as a Medical Device (SaMD): Discussion Paper and Request for Feedback. Available online: https://www.fda.gov/media/122535/download (accessed on 10 March 2020).
- Jo, T.; Nho, K.; Saykin, A.J. Deep Learning in Alzheimer’s Disease: Diagnostic Classification and Prognostic Prediction Using Neuroimaging Data. Front. Aging Neurosci. 2019, 11, 220. [Google Scholar] [CrossRef] [Green Version]
- Cohen, I.G. Informed Consent and Medical Artificial Intelligence: What to Tell the Patient? Georget. Law J. 2020, 108, 1425–1469. [Google Scholar] [CrossRef]
- Schmidhuber, M. Neuroimaging für eine frühe Diagnose der Alzheimer-Demenz. In Neuroimaging und Neuroökonomie: Grundlagen, ethische Fragestellungen, soziale und rechtliche Relevanz; Ach, J.S., Lüttenberg, B., Nossek, A., Eds.; Lit Verlag: Berlin, Germany, 2015; pp. 103–118. [Google Scholar]
- Paulsen, J.S.; Nance, M.; Kim, J.-I.; Carlozzi, N.E.; Panegyres, P.K.; Erwin, C.; Goh, A.; McCusker, E.; Williams, J.K. A review of quality of life after predictive testing for and earlier identification of neurodegenerative diseases. Prog. Neurobiol. 2013, 110, 2–28. [Google Scholar] [CrossRef] [Green Version]
- Martín Noguerol, T.; Paulano-Godino, F.; Martín-Valdivia, M.T.; Menias, C.O.; Luna, A. Strengths, Weaknesses, Opportunities, and Threats Analysis of Artificial Intelligence and Machine Learning Applications in Radiology. J. Am. Coll. Radiol. 2019, 16, 1239–1247. [Google Scholar] [CrossRef] [PubMed]
- London, A.J. Artificial Intelligence and Black-Box Medical Decisions: Accuracy versus Explainability. Hastings Center Rep. 2019, 49, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Weikert, T.; Cyriac, J.; Yang, S.; Nesic, I.; Parmar, V.; Stieltjes, B. A Practical Guide to Artificial Intelligence-Based Image Analysis in Radiology. Investig. Radiol. 2020, 55, 1–7. [Google Scholar] [CrossRef]
- Evans, J.P.; Skrzynia, C.; Burke, W. The complexities of predictive genetic testing. BMJ 2001, 322, 1052–1056. [Google Scholar] [CrossRef] [Green Version]
- Alzheimer’s Disease International. World Alzheimer Report 2019. Available online: https://www.alz.co.uk/research/world-report-2019 (accessed on 25 February 2020).
- Erlangsen, A.; Stenager, E.; Conwell, Y.; Andersen, P.K.; Hawton, K.; Benros, M.E.; Nordentoft, M.; Stenager, E. Association Between Neurological Disorders and Death by Suicide in Denmark. JAMA 2020, 323, 444–454. [Google Scholar] [CrossRef] [PubMed]
- Almqvist, E.W.; Bloch, M.; Brinkman, R.; Craufurd, D.; Hayden, R.M. A worldwide assessment of the frequency of suicide, suicide attempts, or psychiatric hospitalization after predictive testing for Huntington disease. Am. J. Hum. Genet. 1999, 64, 1293–1304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bird, T.D. Outrageous fortune: The risk of suicide in genetic testing for Huntington disease. Am. J. Hum. Genet. 1999, 64, 1289–1292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geis, J.R.; Brady, A.P.; Wu, C.C.; Spencer, J.; Ranschaert, E.; Jaremko, J.L.; Langer, S.G.; Kitts, A.B.; Birch, J.; Shields, W.F.; et al. Ethics of Artificial Intelligence in Radiology: Summary of the Joint European and North American Multisociety Statement. Can. Assoc. Radiol. J. 2019, 70, 329–334. [Google Scholar] [CrossRef] [Green Version]
- Morley, J.; Floridi, L.; Kinsey, L.; Elhalal, A. From What to How: An Initial Review of Publicly Available AI Ethics Tools, Methods and Research to Translate Principles into Practices. Sci. Eng. Ethics 2019. [Google Scholar] [CrossRef] [Green Version]
- Brady, A.P.; Neri, E. Artificial Intelligence in Radiology-Ethical Considerations. Diagnostics 2020, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiraishi, J.; Li, Q.; Appelbaum, D.; Doi, K. Computer-aided diagnosis and artificial intelligence in clinical imaging. Semin. Nucl. Med. 2011, 41, 449–462. [Google Scholar] [CrossRef] [PubMed]
- Holm, E.A. In defense of the black box. Science 2019, 364, 26–27. [Google Scholar] [CrossRef]
- Alexander, A.; Jiang, A.; Ferreira, C.; Zurkiya, D. An Intelligent Future for Medical Imaging: A Market Outlook on Artificial Intelligence for Medical Imaging. J. Am. Coll. Radiol. 2020, 17, 165–170. [Google Scholar] [CrossRef] [Green Version]
- Topol, E.J. Deep medicine. How Artificial Intelligence Can Make Healthcare Human Again, 1st ed.; Basic Books: New York, NY, USA, 2019; ISBN 9781541644632. [Google Scholar]
- Heilinger, J.-C. Cosmopolitan responsibility. In Global Injustice, Relational Equality, and Individual Agency, 1st ed.; De Gruyter: Berlin, Germany, 2020; ISBN 9783110600780. [Google Scholar]

{kind=link}
| Authors | Title | Type of Study | Date |
|---|---|---|---|
| Smedinga, Tromp, Schermer, Richard | Ethical Arguments Concerning the Use of Alzheimer’s Disease Biomarkers in Individuals with No or Mild Cognitive Impairment: A Systematic Review and Framework for Discussion | Systematic Review | 2018 |
| Vanderschaeghe, Dierickx, Vandenberghe | Review of the Ethical Issues of a Biomarker-Based Diagnoses in the Early Stage of Alzheimer’s Disease | Systematic Review | 2018 |
| Milne, Karlawish | Expanding engagement with the ethical implications of changing definitions of Alzheimer’s disease | Correspondence (conceptual) | 2017 |
| Whitehouse | Ethical issues in early diagnosis and prevention of Alzheimer disease | Original Article (conceptual) | 2019 |
| Vanderschaeghe, Vandenberghe, Dierickx | Stakeholders’ Views on Early Diagnosis for Alzheimer’s Disease, Clinical Trial Participation and Amyloid PET Disclosure: A Focus Group Study | Focus Group (qualitative) | 2019 |
| Erdmann, Langanke | The Ambivalence of Early Diagnosis—Returning Results in Current Alzheimer Research | Risk-Benefit-Assessment (conceptual) | 2018 |
| Schermer, Richard | On the reconceptualization of Alzheimer’s disease | Original Work (conceptual) | 2019 |
| Hughes, Ingram, Jarvis, et al. | Consent for the diagnosis of preclinical dementia states: A review | Review | 2017 |
| Davis | Ethical issues in Alzheimer’s disease research involving human subjects | Original Work (conceptual) | 2017 |
| Schweda, Kögel, Bartels, Wiltfang, Schneider, Schicktanz | Prediction and Early Detection of Alzheimer’s Dementia: Professional Disclosure Practices and Ethical Attitudes | Survey (qualitative and quantitative) | 2017 |
| Stites, Milne, Karlawish | Advances in Alzheimer’s imaging are changing the experience of Alzheimer’s disease | Narrative Review (conceptual) | 2018 |
| Angehrn, Sostar, et al. | Ethical and Social Implications of Using Predictive Modeling for Alzheimer’s Disease Prevention: A Systematic Literature Review | Systematic Review | 2020 |
| Ivanoiu, Engelborghs, Hanseeuw | Early diagnosis of Alzheimer’s disease (with the announcement of the diagnosis) | Original Work (conceptual) | 2020 |
| Mattsson, Brax, Zetterberg | To Know or Not to Know—Ethical Issues Related to Early Diagnosis of Alzheimer’s Disease | Original Work (conceptual) | 2010 |
| Frisoni, Boccardi, Barkhof, et al. | Strategic roadmap for an early diagnosis of Alzheimer’s disease based on biomarkers | Whitepaper | 2017 |
| Ebrahimighahnavieh, Luo, Chiong | Deep learning to detect Alzheimer’s disease from neuroimaging: A systematic literature review | Systematic Review | 2019 |
| Graham, Lee, Jeste, et al. | Artificial intelligence approaches to predicting and detecting cognitive decline in older adults: A conceptual review | Conceptual Review | 2020 |
| Gautam, Sharma | Prevalence and Diagnosis of Neurological Disorders Using Different Deep Learning Techniques: A Meta-Analysis | Systematic Meta Review | 2020 |
| Use Cases | Ethical Assessments | Source |
|---|---|---|
| (1) research | protected by good clinical practice research frameworks, ethics approvals by ethics committees, and informed consent | [15,19,36] |
| (1a) symptomatic patients actively seeking support | benefits of early detection outweigh potential adverse effects | [37] |
| (1b) asymptomatic volunteers which consent to predictive testing | potential adverse effects overweigh the benefits, therefore restrictive disclosure policy according to the “principle of caution” | [37] |
| (2) screening everyone | “turning everyone into patients” and “patients-in-waiting” | [31,38] |
| (3) screening those with known risk factors | partial exclusion of patients and “patients-in-waiting” | [31,38] |
| (4) psychological screening before screening | partial exclusion of potential patients | [31] |
| (5) voluntary access to screening for everyone | considered ethically justified to disclose biomarker results on request | [31,39] |
| (5a) symptomatic patients actively seeking support | benefits of early detection outweigh potential adverse effects | [37] |
| (5b) asymptomatic patients actively seeking support | considered ethically unjustified to disclose biomarker results | [39] |
| Themes | Argument | Source |
|---|---|---|
| Benefits | resolving uncertainty of one’s risk is beneficial when it brings clinically meaningful information and the subject is willing to know his risk or diagnosis | [19,31,37] |
| knowing one’s risk enables future planning | [19,20,31,37,38,40] | |
| knowing one’s risk enables promotion of research and control of the disease’s progression | [19,20,38] | |
| knowing one’s risk enables change of unhealthy lifestyle | [37,41] | |
| Right to know | good communication requires a physician to determine whether an individual wishes disclosure based on personal preferences | [19,30,38,41,42] |
| respect for the individual’s autonomy and empowerment | [37,41] | |
| clarity, informing family members, and planning for the future | [40,43] | |
| Slippery-slope-argument | voluntary screening is justified since commercial genetic testing for AD is already available | [31,36] |
| Economy | cost-effectiveness is a requirement for predictive tests and future hypothetical preventive treatment, but opinions are divided whether tests would save money or increase costs | [19,20,31] |
| restriction of tests beyond research use cases that are used for profit in individuals for whom a risk assessment is not indicated | [15] |
| Themes | Argument | Source |
|---|---|---|
| Lack of disease modifying treatment | knowing one’s risk or diagnosis does not alter the disease | [19,30,31] |
| general screening is only considered useful if effective treatment options are available | [19,20] | |
| predictive testing is only seen as ethically acceptable in research because predictive value is unclear and preventive measures are not available | [19,38] | |
| Accuracy | although predictive AI systems have a high accuracy, there is no social consensus about which predictive power is sufficient | [3,9,31,44] |
| no clinical use before regulatory approval because of the risk of false-negative and false-positive diagnoses, no consensus about sufficiency of predictive power, amyloid cascade hypothesis is contested in research, patients may not understand the predictive value and undergo therapeutic misconception | [12,30,31,38,40] | |
| false-negative diagnoses may lead to false reassurance and exclusion from treatment or clinical trials | [15,31,37] | |
| false-positive diagnoses may lead to over-diagnosis, over-treatment, inappropriate inclusion in clinical trials, invasive biomarker testing can be harmful | [15,31,37] | |
| Risks | avoidance of psychosocial harm because of distress, anxiety, remaining post-testing uncertainty, possible false-positive or false-negative diagnoses, stigmatization (public stigma, self-stigma, spillover stigma), discrimination in health insurance and at work | [19,20,30,31,38,40,41,45,46] |
| avoidance of harm to third parties because of family burdens, social burdens (isolation, discrimination, and social rejection) | [40,41,45] | |
| avoidance of harm to subjects and third-parties because of “rational suicide” based on financial reasons and to reduce family burden | [30] | |
| Right not to know | wish not to know because of anxiety and disease modifying treatments are not available | [19,30,40,41] |
| avoidance of forced information because it violates respect for autonomy | [20] | |
| Explicability | patient’s different degrees of understanding the disease and the uncertainty of preclinical risk assessment entail a challenging communication of diagnosis or risk assessment | [12,30,31,40,45] |
| demand for the transparency of the “diagnostic decision” due to involvement of AI/ML (machine learning) systems and black box algorithms | [3] | |
| demand for governance models for patient’s data, data security, infrastructure for gathering and managing data, accountability, algorithm bias, passive surveillance tools, and regulatory approval | [3] | |
| Threats for social rights | need for international agreements on the protection of subjects that underwent a biomarker test like in the case of genetic privacy | [36,45] |
| worries that health insurances deny coverage or charge higher premiums | [19,20,30,36,45] | |
| worries about employment discrimination, exclusion from medical decision making, or the withdrawal of one’s driving license | [3,20,30,45,46] | |
| Training | demand for structured training of physicians to counsel patients about AI/ML systems | [15,45] |
| Guidelines and standardization | demand for guidelines about information and disclosure practice | [15,20,36] |
| demand for standardization of test methods, threshold values, data protection | [15,20] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ursin, F.; Timmermann, C.; Steger, F. Ethical Implications of Alzheimer’s Disease Prediction in Asymptomatic Individuals through Artificial Intelligence. Diagnostics 2021, 11, 440. https://doi.org/10.3390/diagnostics11030440
Ursin F, Timmermann C, Steger F. Ethical Implications of Alzheimer’s Disease Prediction in Asymptomatic Individuals through Artificial Intelligence. Diagnostics. 2021; 11(3):440. https://doi.org/10.3390/diagnostics11030440
Chicago/Turabian StyleUrsin, Frank, Cristian Timmermann, and Florian Steger. 2021. "Ethical Implications of Alzheimer’s Disease Prediction in Asymptomatic Individuals through Artificial Intelligence" Diagnostics 11, no. 3: 440. https://doi.org/10.3390/diagnostics11030440