
Clinical Significance of Histone Deacetylase (HDAC)-1, -2, -4 and -6 Expression in Salivary Gland Tumors


 , ,
, ,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Clinical Material
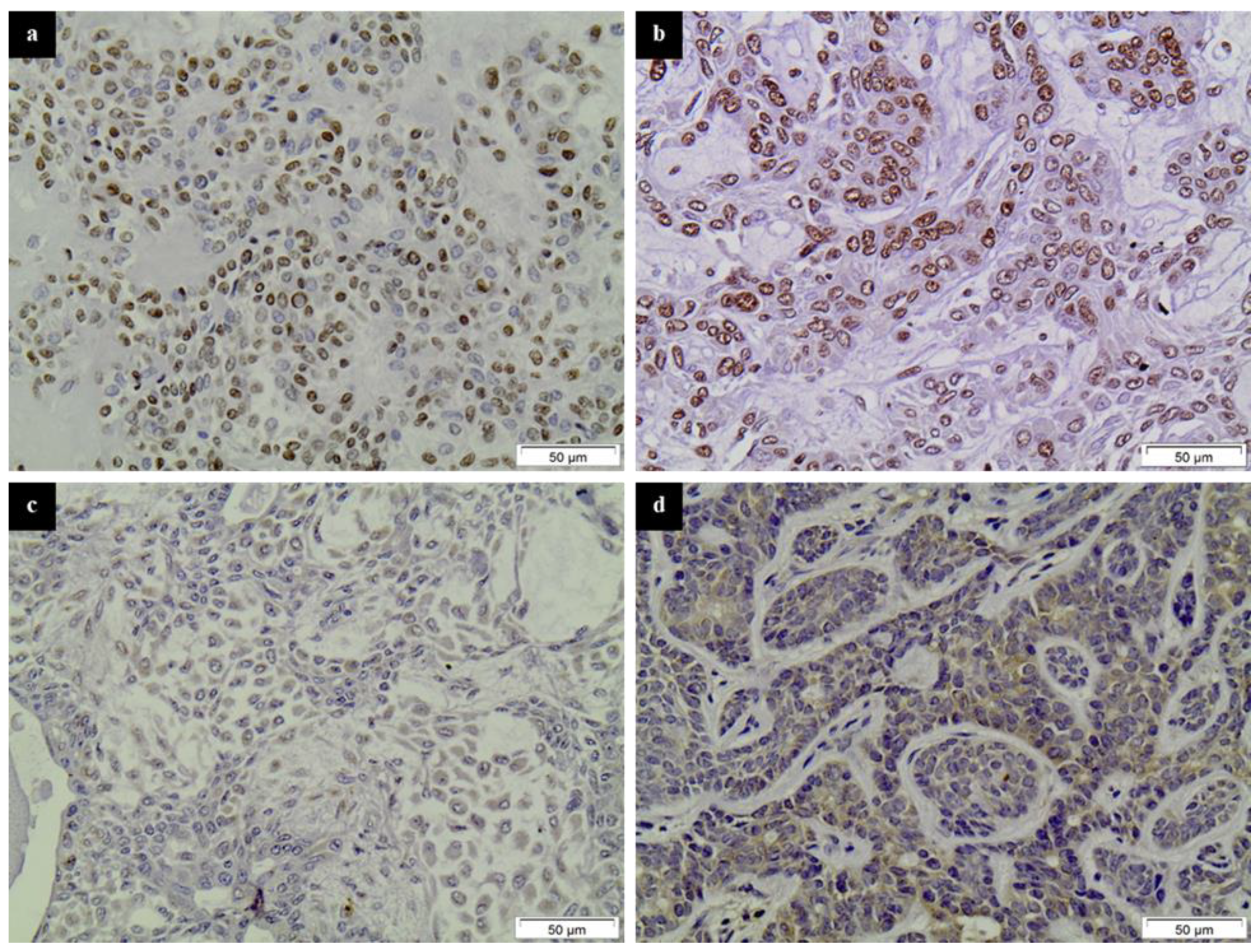
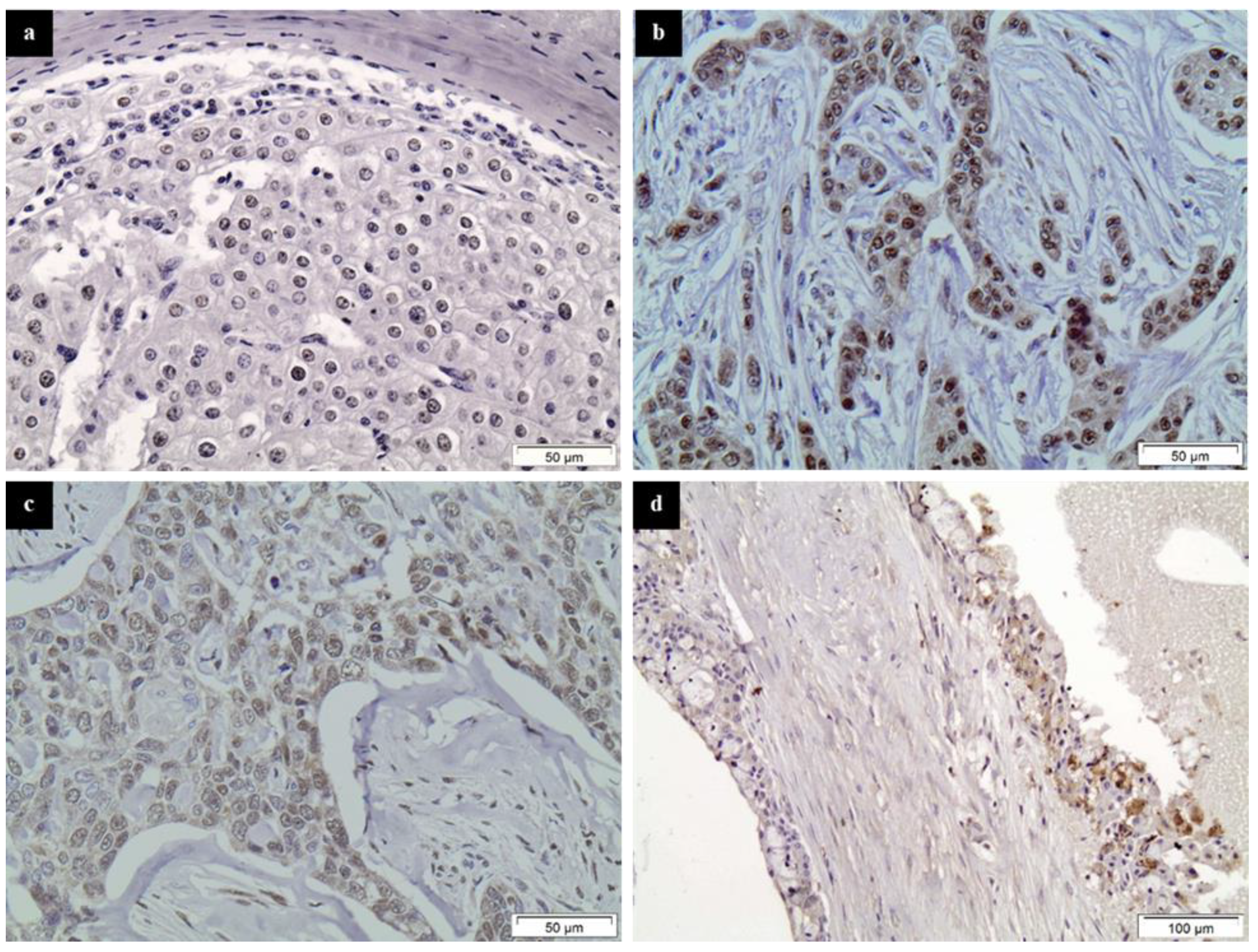
2.2. Immunohistochemistry
2.3. Evaluation of Immunohistochemistry
2.4. Statistical Analysis
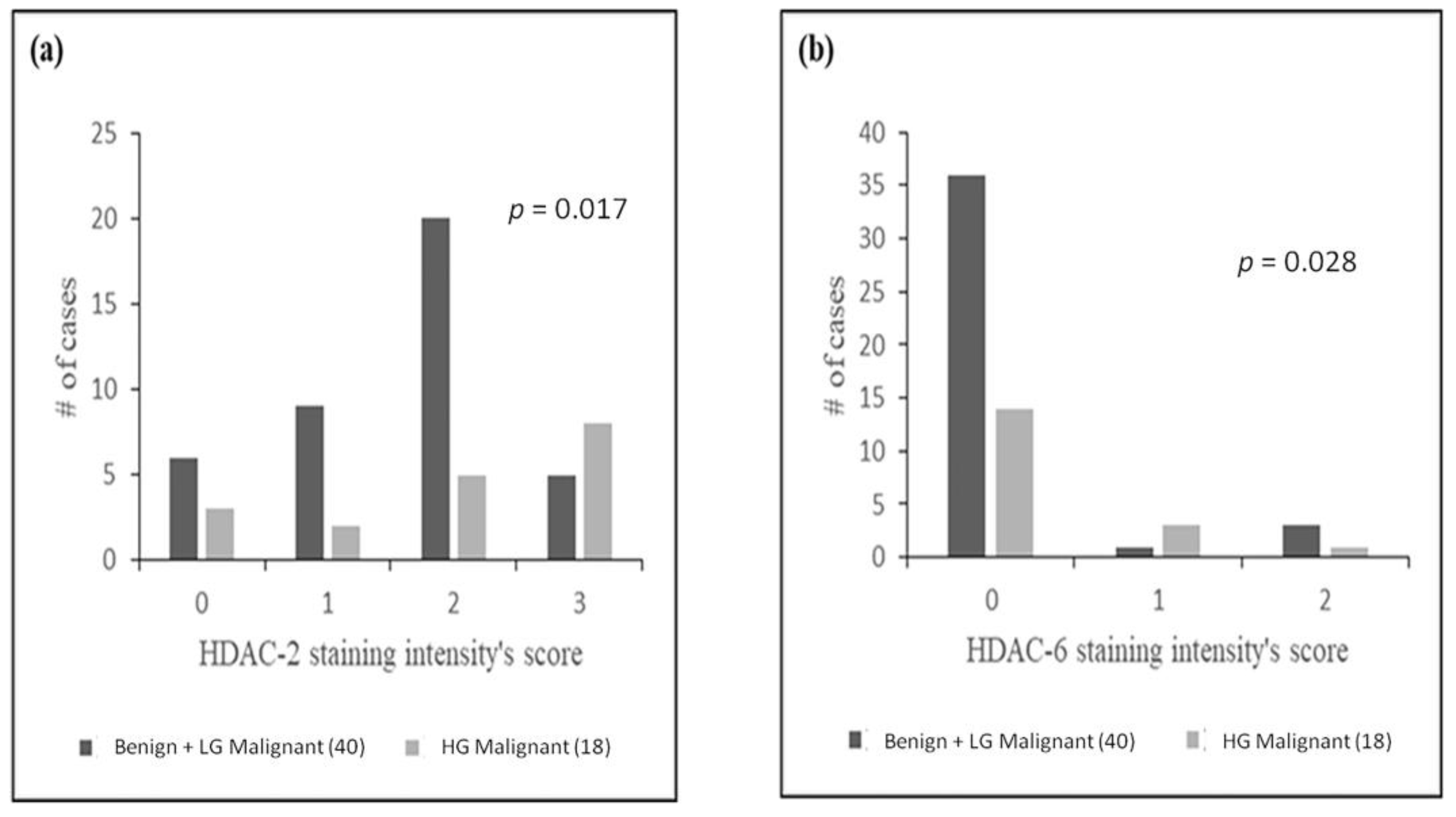
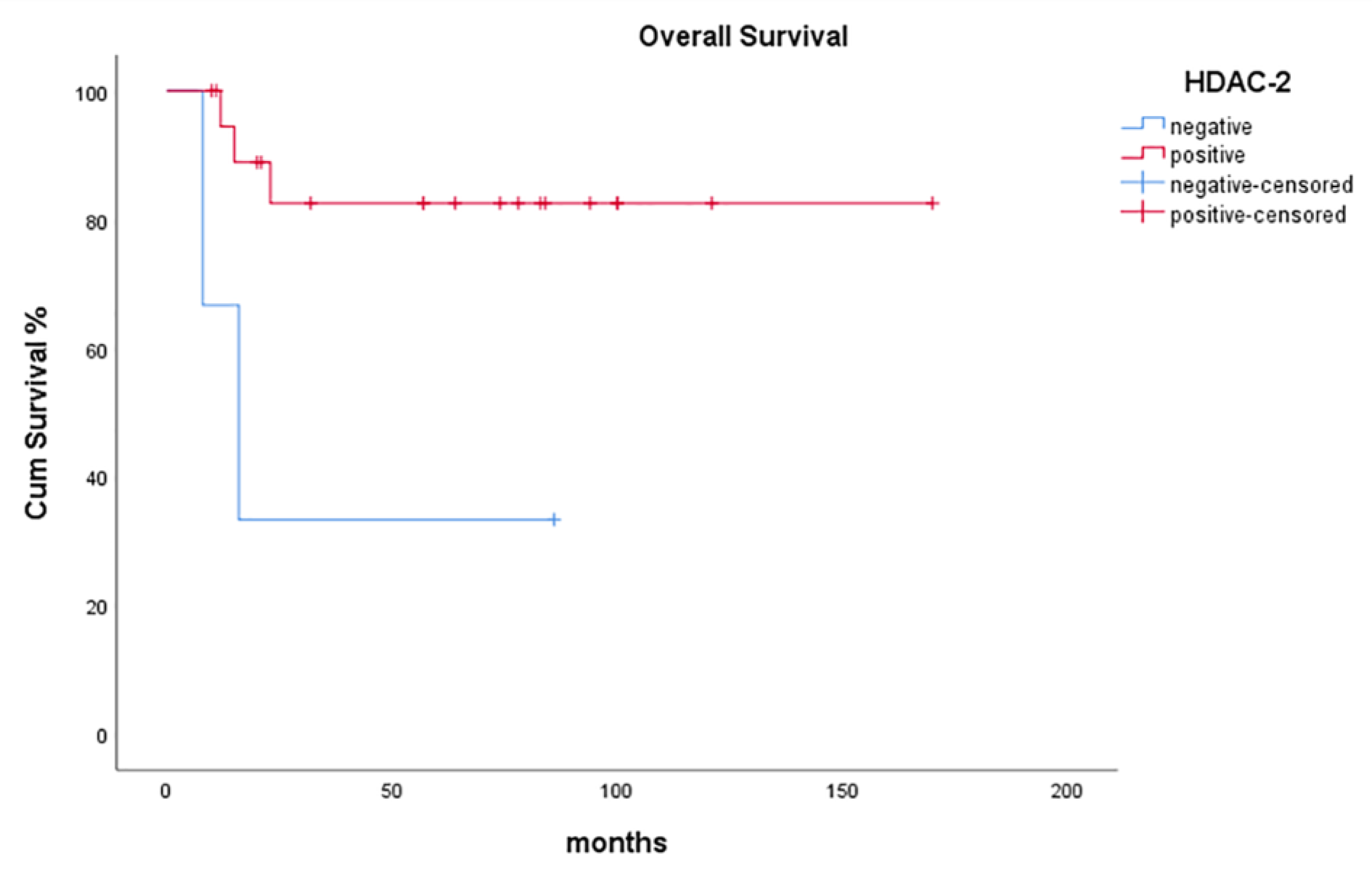
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Seifert, G.; Brocheriou, C.; Cardesa, A.; Eveson, J.W. World Health Organization (WHO) international histological classification of tumours tentative histological classification of salivary gland tumours. Pathol. Res. Pract. 1990, 186, 555–581. [Google Scholar] [CrossRef]
- EI-Naggar, J.; Chan, K.C.; Grandis, J.R.; Takata, T.; Pieter, J.; Slootweg, A.K. World Health Organization Classification of Head and Neck Tumours, 4th ed.; IARC Publications: Lyon, France, 2017; ISBN 9789283224389. [Google Scholar]
- Hellquist, H.; Paiva-Correia, A.; Poorten, V.V.; Quer, M.; Hernandez-Prera, J.C.; Andreasen, S.; Zbären, P.; Skalova, A.; Rinaldo, A.; Ferlito, A. Analysis of the clinical relevance of histological classification of benign epithelial salivary gland tumours. Adv. Ther. 2019, 36, 1950–1974. [Google Scholar] [CrossRef]
- Griffith, C.C.; Schmitt, A.C.; Little, J.L.; Magliocca, K.R. New developments in salivary gland pathology: Clinically useful ancillary testing and new potentially targetable molecular alterations. Arch. Pathol. Lab. Med. 2017, 141, 381–395. [Google Scholar] [CrossRef] [PubMed]
- Katabi, N.; Xu, B. Salivary gland neoplasms: Diagnostic approach with focus on patterns of recognition and useful ancillary tools. Diagn. Histopathol. 2018, 24, 180–188. [Google Scholar] [CrossRef]
- Theocharis, S.; Gribilas, G.; Giaginis, C.; Patsouris, E.; Klijanienko, J. Angiogenesis in salivary gland tumors: From clinical significance to treatment. Expert Opin. Ther. Targets 2015, 19, 807–819. [Google Scholar] [CrossRef] [PubMed]
- Yin, L.X.; Ha, P.K. Genetic alterations in salivary gland cancers. Cancer 2016, 122, 1822–1831. [Google Scholar] [CrossRef] [PubMed]
- Carlson, E.R.; Schlieve, T. Salivary gland malignancies. Oral Maxillofac. Surg. Clin. N. Am. 2019, 31, 125–144. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo-Pouso, A.I.; Pérez-Sayáns, M.; Bravo, S.B.; López-Jornet, P.; García-Vence, M.; Alonso-Sampedro, M.; Carballo, J.; García-García, A.; Zalewska, A. Protein-based salivary profiles as novel biomarkers for oral diseases. Dis. Markers 2018, 2018, 6141845. [Google Scholar] [CrossRef] [PubMed]
- To, V.S.H.; Chan, J.Y.W.; Tsang, R.K.Y.; Wei, W.I. Review of salivary gland neoplasms. ISRN Otolaryngol. 2012, 2012, 1–6. [Google Scholar] [CrossRef]
- Israel, Y.; Rachmiel, A.; Gourevich, K.; Nagler, R. Survival probabilities related to histology, grade and stage in patients with salivary gland tumors. Anticancer Res. 2019, 39, 641–647. [Google Scholar] [CrossRef]
- Chintakuntlawar, A.V.; Okuno, S.H.; Price, K.A. Systemic therapy for recurrent or metastatic salivary gland malignancies. Cancers Head Neck 2016, 1, 11. [Google Scholar] [CrossRef] [PubMed]
- Bell, D.; Hanna, E.Y. Salivary gland cancers: Biology and molecular targets for therapy. Curr. Oncol. Rep. 2012, 14, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Theocharis, S.; Tasoulas, J.; Masaoutis, C.; Kokkali, S.; Klijanienko, J. Salivary gland cancer in the era of immunotherapy: Can we exploit tumor microenvironment? Expert Opin. Ther. Targets 2020, 24, 1047–1059. [Google Scholar] [CrossRef] [PubMed]
- Rack, S.; Rahman, R.; Carter, L.; McKay, C.; Metcalf, R. Impact of tumour profiling on clinical trials in salivary gland cancer. Clin. Otolaryngol. 2019, 44, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Santos, E.S.; Ramos, J.C.; Normando, A.G.C.; Mariano, F.V.; Paes Leme, A.F. Epigenetic alterations in salivary gland tumors. Oral Dis. 2020, 26, 1610–1618. [Google Scholar] [CrossRef]
- Cheng, Y.Y.; Jin, H.C.; Chan, M.W.Y.; Chu, W.K.; Grusch, M. Epigenetic biomarkers in cancer. Dis. Markers 2018, 2018, 9864047. [Google Scholar] [CrossRef]
- Dawson, M.A.; Kouzarides, T. Cancer epigenetics: From mechanism to therapy. Cell 2012, 150, 12–27. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.F. Epigenomics in cancer management. Cancer Manag. Res. 2010, 2, 255–265. [Google Scholar] [CrossRef][Green Version]
- Esteller, M. Cancer epigenomics: DNA methylomes and histone-modification maps. Nat. Rev. Genet. 2007, 8, 286–298. [Google Scholar] [CrossRef]
- Seto, E.; Yoshida, M. Erasers of histone acetylation: The histone deacetylase enzymes. Cold Spring Harb. Perspect. Biol. 2014, 6, a018713. [Google Scholar] [CrossRef]
- Li, Y.; Seto, E. HDACs and HDAC inhibitors in cancer development and therapy. Cold Spring Harb. Perspect. Med. 2016, 6, a026831. [Google Scholar] [CrossRef] [PubMed]
- Wawruszak, A.; Kalafut, J.; Okon, E.; Czapinski, J.; Halasa, M.; Przybyszewska, A.; Miziak, P.; Okla, K.; Rivero-Muller, A.; Stepulak, A. Histone deacetylase inhibitors and phenotypical transformation of cancer cells. Cancers 2019, 11, 148. [Google Scholar] [CrossRef]
- Slootweg, P.J.; El-Naggar, A.K. World Health Organization—4th edition of Head and Neck Tumor Classification: Insight into the consequential modifications. Virchows Arch. 2018, 472, 311–313. [Google Scholar] [CrossRef]
- Theocharis, S.; Klijanienko, J.; Giaginis, C.; Rodriguez, J.; Jouffroy, T.; Girod, A.; Alexandrou, P.; Sastre-Garau, X. Histone deacetylase-1 and -2 expression in mobile tongue squamous cell carcinoma: Associations with clinicopathological parameters and patients survival. J. Oral Pathol. Med. 2011, 40, 706–714. [Google Scholar] [CrossRef]
- Giaginis, C.; Alexandrou, P.; Delladetsima, I.; Giannopoulou, I.; Patsouris, E.; Theocharis, S. Clinical significance of histone deacetylase (HDAC)-1, HDAC-2, HDAC-4, and HDAC-6 expression in human malignant and benign thyroid lesions. Tumor Biol. 2014, 35, 61–71. [Google Scholar] [CrossRef]
- Jang, J.Y.; Choi, N.; Ko, Y.H.; Chung, M.K.; Son, Y.I.; Baek, C.H.; Baek, K.H.; Jeong, H.S. Treatment outcomes in metastatic and localized high-grade salivary gland cancer: High chance of cure with surgery and post-operative radiation in T1-2 N0 high-grade salivary gland cancer. BMC Cancer 2018, 18, 672. [Google Scholar] [CrossRef]
- Haderlein, M.; Scherl, C.; Semrau, S.; Lettmaier, S.; Uter, W.; Neukam, F.W.; Iro, H.; Agaimy, A.; Fietkau, R. High-grade histology as predictor of early distant metastases and decreased disease-free survival in salivary gland cancer irrespective of tumor subtype. Head Neck 2016, 38, E2041–E2048. [Google Scholar] [CrossRef] [PubMed]
- Mutze, K.; Langer, R.; Becker, K.; Ott, K.; Novotny, A.; Luber, B.; Hapfelmeier, A.; Göttlicher, M.; Höfler, H.; Keller, G. Histone deacetylase (HDAC) 1 and 2 expression and chemotherapy in gastric cancer. Ann. Surg. Oncol. 2010, 17, 3336–3343. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.; Min, S.K.; Park, H.R.; Kim, D.H.; Kwon, M.J.; Kim, L.S.; Ju, Y.S. Expression of histone deacetylases HDAC1, HDAC2, HDAC3, and HDAC6 in invasive ductal carcinomas of the breast. J. Breast Cancer 2014, 17, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Staberg, M.; Michaelsen, S.R.; Rasmussen, R.D.; Villingshøj, M.; Poulsen, H.S.; Hamerlik, P. Inhibition of histone deacetylases sensitizes glioblastoma cells to lomustine. Cell. Oncol. 2017, 40, 21–32. [Google Scholar] [CrossRef] [PubMed]
- Chrun, E.S.; Modolo, F.; Vieira, D.S.C.; Borges, L.S., Jr.; Castro, R.G.; Daniel, F.I. Immunoexpression of HDAC1, HDAC2, and HAT1 in actinic cheilitis and lip squamous cell carcinoma. Oral Dis. 2017, 23, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Zhang, Y.; Yang, L.H.; Mi, X.Y.; Dai, S.D.; Li, Q.C.; Xu, H.T.; Yu, J.H.; Li, G.; Zhao, J.; et al. hua X-radiation inhibits histone deacetylase 1 and 2, upregulates Axin expression and induces apoptosis in non-small cell lung cancer. Radiat. Oncol. 2012, 7, 183. [Google Scholar] [CrossRef] [PubMed]
- Quint, K.; Agaimy, A.; Di Fazio, P.; Montalbano, R.; Steindorf, C.; Jung, R.; Hellerbrand, C.; Hartmann, A.; Sitter, H.; Neureiter, D.; et al. Clinical significance of histone deacetylases 1, 2, 3, and 7: HDAC2 is an independent predictor of survival in HCC. Virchows Arch. 2011, 459, 129–139. [Google Scholar] [CrossRef]
- Halkidou, K.; Gaughan, L.; Cook, S.; Leung, H.Y.; Neal, D.E.; Robson, C.N. Upregulation and nuclear recruitment of HDACl in hormone refractory prostate cancer. Prostate 2004, 59, 177–189. [Google Scholar] [CrossRef]
- Weichert, W.; Röske, A.; Gekeler, V.; Beckers, T.; Stephan, C.; Jung, K.; Fritzsche, F.R.; Niesporek, S.; Denkert, C.; Dietel, M.; et al. Histone deacetylases 1, 2 and 3 are highly expressed in prostate cancer and HDAC2 expression is associated with shorter PSA relapse time after radical prostatectomy. Br. J. Cancer 2008, 98, 604–610. [Google Scholar] [CrossRef]
- Weichert, W.; Denkert, C.; Noske, A.; Darb-Esfahani, S.; Dietel, M.; Kalloger, S.E.; Huntsman, D.G.; Köbel, M. Expression of class I histone deacetylases indicates poor prognosis in endometrioid subtypes of ovarian and endometrial carcinomas. Neoplasia 2008, 10, 1021–1027. [Google Scholar] [CrossRef]
- Poyet, C.; Jentsch, B.; Hermanns, T.; Schweckendiek, D.; Seifert, H.H.; Schmidtpeter, M.; Sulser, T.; Moch, H.; Wild, P.J.; Kristiansen, G. Expression of histone deacetylases 1, 2 and 3 in urothelial bladder cancer. BMC Clin. Pathol. 2014, 14, 2753–2760. [Google Scholar] [CrossRef]
- Suzuki, J.; Chen, Y.Y.; Scott, G.K.; DeVries, S.; Chin, K.; Benz, C.C.; Waldman, F.M.; Hwang, E.S. Protein acetylation and histone deacetylase expression associated with malignant breast cancer progression. Clin. Cancer Res. 2009, 15, 3163–3171. [Google Scholar] [CrossRef] [PubMed]
- Langer, R.; Mutze, K.; Becker, K.; Feith, M.; Ott, K.; Höfler, H.; Keller, G. Expression of class I histone deacetylases (HDAC1 and HDAC2) in oesophageal adenocarcinomas: An immunohistochemical study. J. Clin. Pathol. 2010, 63, 994–998. [Google Scholar] [CrossRef]
- Weichert, W.; Röske, A.; Gekeler, V.; Beckers, T.; Ebert, M.P.; Pross, M.; Dietel, M.; Denkert, C.; Röcken, C. Association of patterns of class I histone deacetylase expression with patient prognosis in gastric cancer: A retrospective analysis. Lancet Oncol. 2008, 9, 139–148. [Google Scholar] [CrossRef]
- Weichert, W.; Röske, A.; Niesporek, S.; Noske, A.; Buckendahl, A.C.; Dietel, M.; Gekeler, V.; Boehm, M.; Beckers, T.; Denkert, C. Class I histone deacetylase expression has independent prognostic impact in human colorectal cancer: Specific role of class I histone deacetylases in vitro and in vivo. Clin. Cancer Res. 2008, 14, 1669–1677. [Google Scholar] [CrossRef]
- Morine, Y.; Shimada, M.; Iwahashi, S.; Utsunomiya, T.; Imura, S.; Ikemoto, T.; Mori, H.; Hanaoka, J.; Miyake, H. Role of histone deacetylase expression in intrahepatic cholangiocarcinoma. Surgery 2012, 151, 412–419. [Google Scholar] [CrossRef]
- Hayashi, A.; Horiuchi, A.; Kikuchi, N.; Hayashi, T.; Fuseya, C.; Suzuki, A.; Konishi, I.; Shiozawa, T. Type-specific roles of histone deacetylase (HDAC) overexpression in ovarian carcinoma: HDAC1 enhances cell proliferation and HDAC3 stimulates cell migration with downregulation of E-cadherin. Int. J. Cancer 2010, 127, 1332–1346. [Google Scholar] [CrossRef] [PubMed]
- Krusche, C.A.; Wülfing, P.; Kersting, C.; Vloet, A.; Böcker, W.; Kiesel, L.; Beier, H.M.; Alfer, J. Histone deacetylase-1 and -3 protein expression in human breast cancer: A tissue microarray analysis. Breast Cancer Res. Treat. 2005, 90, 15–23. [Google Scholar] [CrossRef]
- Giaginis, C.; Damaskos, C.; Koutsounas, I.; Zizi-Serbetzoglou, A.; Tsoukalas, N.; Patsouris, E.; Kouraklis, G.; Theocharis, S. Histone deacetylase (HDAC)-1, -2, -4 and -6 expression in human pancreatic adenocarcinoma: Associations with clinicopathological parameters, tumor proliferative capacity and patients’ survival. BMC Gastroenterol. 2015, 15, 148. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.M.; Yang, Z.; Zhou, L.; Zhang, F.; Xie, H.Y.; Feng, X.W.; Wu, J.; Zheng, S.S. Identification of histone deacetylase 3 as a biomarker for tumor recurrence following liver transplantation in HBV-associated hepatocellular carcinoma. PLoS ONE 2010, 5, e14460. [Google Scholar] [CrossRef]
- Wilmott, J.S.; Colebatch, A.J.; Kakavand, H.; Shang, P.; Carlino, M.S.; Thompson, J.F.; Long, G.V.; Scolyer, R.A.; Hersey, P. Expression of the class 1 histone deacetylases HDAC8 and 3 are associated with improved survival of patients with metastatic melanoma. Mod. Pathol. 2015, 28, 884–894. [Google Scholar] [CrossRef]
- Milde, T.; Oehme, I.; Korshunov, A.; Kopp-Schneider, A.; Remke, M.; Northcott, P.; Deubzer, H.E.; Lodrini, M.; Taylor, M.D.; Von Deimling, A.; et al. HDAC5 and HDAC9 in medulloblastoma: Novel markers for risk stratification and role in tumor cell growth. Clin. Cancer Res. 2010, 16, 3240–3252. [Google Scholar] [CrossRef]
- Ouaïssi, M.; Sielezneff, I.; Silvestre, R.; Sastre, B.; Bernard, J.P.; Lafontaine, J.S.; Payan, M.J.; Dahan, L.; Pirrò, N.; Seitz, J.F.; et al. High histone deacetylase 7 (HDAC7) expression is significantly associated with adenocarcinomas of the pancreas. Ann. Surg. Oncol. 2008, 15, 2318–2328. [Google Scholar] [CrossRef] [PubMed]
- Sudo, T.; Mimori, K.; Nishida, N.; Kogo, R.; Iwaya, T.; Tanaka, F.; Shibata, K.; Fujita, H.; Shirouzu, K.; Mori, M. Histone deacetylase 1 expression in gastric cancer. Oncol. Rep. 2011, 26, 777–782. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.H.; Seo, K.J.; An, C.H.; Kim, J.S.; Jeon, H.M. CD133 expression is correlated with chemoresistance and early recurrence of gastric cancer. J. Surg. Oncol. 2012, 106, 999–1004. [Google Scholar] [CrossRef]
- Lutz, L.; Fitzner, I.C.; Ahrens, T.; Geißler, A.L.; Makowiec, F.; Hopt, U.T.; Bogatyreva, L.; Hauschke, D.; Werner, M.; Lassmann, S. Histone modifiers and marks define heterogeneous groups of colorectal carcinomas and affect responses to HDAC inhibitors in vitro. Am. J. Cancer Res. 2016, 6, 664–676. [Google Scholar]
- Song, J.; Noh, J.H.; Lee, J.H.; Eun, J.W.; Ahn, Y.M.; Kim, S.Y.; Hyung Lee, S.; Park, W.S.; Yoo, N.J.; Lee, J.Y.; et al. Increased expression of histone deacetylase 2 is found in human gastric cancer. APMIS 2005, 113, 264–268. [Google Scholar] [CrossRef]
- Fritzsche, F.R.; Weichert, W.; Röske, A.; Gekeler, V.; Beckers, T.; Stephan, C.; Jung, K.; Scholman, K.; Denkert, C.; Dietel, M.; et al. Class I histone deacetylases 1, 2 and 3 are highly expressed in renal cell cancer. BMC Cancer 2008, 8, 381. [Google Scholar] [CrossRef]
- Shen, Y.F.; Wei, A.M.; Kou, Q.; Zhu, Q.Y.; Zhang, L. Histone deacetylase 4 increases progressive epithelial ovarian cancer cells via repression of p21 on fibrillar collagen matrices. Oncol. Rep. 2016, 35, 948–954. [Google Scholar] [CrossRef]
- Wang, L.; Zou, X.; Berger, A.D.; Twiss, C.; Peng, Y.; Li, Y.; Chiu, J.; Guo, H.; Satagopan, J.; Wilton, A.; et al. Increased expression of histone deacetylaces (HDACs) and inhibition of prostate cancer growth and invasion by HDAC inhibitor SAHA. Am. J. Transl. Res. 2009, 1, 62–71. [Google Scholar] [PubMed]
- Sakuma, T.; Uzawa, K.; Onda, T.; Shiiba, M.; Yokoe, H.; Shibahara, T.; Tanzawa, H. Aberrant expression of histone deacetylase 6 in oral squamous cell carcinoma. Int. J. Oncol. 2006, 29, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Suraweera, A.; O’Byrne, K.J.; Richard, D.J. Combination therapy with histone deacetylase inhibitors (HDACi) for the treatment of cancer: Achieving the full therapeutic potential of HDACi. Front. Oncol. 2018, 8, 92. [Google Scholar] [CrossRef]
- Wagner, V.P.; Martins, M.D.; Guimaraes, D.M.; Vasconcelos, A.C.; Meurer, L.; Vargas, P.A.; Fonseca, F.P.; Squarize, C.H.; Castilho, R.M. Reduced chromatin acetylation of malignant salivary gland tumors correlates with enhanced proliferation. J. Oral Pathol. Med. 2017, 46, 792–797. [Google Scholar] [CrossRef] [PubMed]
- Ahn, M.Y.; Yoon, J.H. Histone deacetylase 7 silencing induces apoptosis and autophagy in salivary mucoepidermoid carcinoma cells. J. Oral Pathol. Med. 2017, 46, 276–283. [Google Scholar] [CrossRef]
- Wagner, V.P.; Martins, M.D.; Martins, M.A.T.; Almeida, L.O.; Warner, K.A.; Nör, J.E.; Squarize, C.H.; Castilho, R.M. Targeting histone deacetylase and NFκB signaling as a novel therapy for mucoepidermoid carcinomas. Sci. Rep. 2018, 8, 2065. [Google Scholar] [CrossRef]
- Almeida, L.O.; Guimarães, D.M.; Martins, M.D.; Martins, M.A.T.; Warner, K.A.; Nör, J.E.; Castilho, R.M.; Squarize, C.H. Unlocking the chromatin of adenoid cystic carcinomas using HDAC inhibitors sensitize cancer stem cells to cisplatin and induces tumor senescence. Stem Cell Res. 2017, 21, 94–105. [Google Scholar] [CrossRef] [PubMed]
- Guimarães, D.M.; Almeida, L.O.; Martins, M.D.; Warner, K.A.; Silva, A.R.S.; Vargas, P.A.; Nunes, F.D.; Squarize, C.H.; Nör, J.E.; Castilho, R.M. Sensitizing mucoepidermoid carcinomas to chemotherapy by targeted disruption of cancer stem cells. Oncotarget 2016, 7, 42447–42460. [Google Scholar] [CrossRef]
- Yang, S.; Nan, P.; Li, C.; Lin, F.; Li, H.; Wang, T.; Zhou, C.; Zhang, X.; Meng, X.; Qian, H.; et al. Inhibitory effect of chidamide on the growth of human adenoid cystic carcinoma cells. Biomed. Pharmacother. 2018, 99, 608–614. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HDAC # OF CASES | HDAC-1 | HDAC-2 | HDAC-4 | HDAC-6 | ||||
|---|---|---|---|---|---|---|---|---|
| Positive (%) | High H-Score (%) | Positive (%) | High H-Score (%) | Positive (%) | High H-Score (%) | Positive (%) | High H-Score (%) | |
| TOTAL (58) | 14 (24.14%) | 4 (6.90%) | 49 (84.48%) | 44 (75.86%) | 24 (41.38%) | 13 (22.41%) | 8 (13.79%) | 4 (6.90%) |
| BENIGN (36) | 11 (30.56%) | 3 (8.33%) | 31 (86.11%) | 28 (77.78%) | 16 (44.44%) | 8 (22.22%) | 4 (11.11%) | 3 (8.33%) |
| PA (28) | 10 (35.71%) | 3 (10.71%) | 26 (92.86%) | 24 (85.71%) | 15 (53.57%) | 7 (25%) | 3 (10.71%) | 2 (7.14%) |
| WT (7) | 1 (14.29%) | 0 (0%) | 4 (57.14%) | 3 (42.86%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| BAD (1) | 0 (0%) | 0 (0%) | 1 (100%) | 1 (100%) | 1 (100%) | 1 (100%) | 1 (100%) | 1 (100%) |
| MALIGNANT (22) | 3 (13.64%) | 1 (4.55%) | 18 (81.82%) | 16 (72.73%) | 8 (36.36%) | 5 (22.73%) | 4 (18.18%) | 1 (4.55%) |
| MEC (3) | 1 (33.33%) | 1 (33.33%) | 3 (100%) | 3 (100%) | 2 (66.67%) | 2 (66.67%) | 1 (33.33%) | 0 (0%) |
| Low grade (1) | 0 (0%) | 0 (0%) | 1 (100%) | 1 (100%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| High grade (2) | 1 (50%) | 1 (50%) | 2 (100%) | 2 (100%) | 2 (100%) | 2 (100%) | 1 (50%) | 0 (0%) |
| ACC (4) | 1 (25%) | 0 (0%) | 4 (100%) | 4 (100%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Low grade (0) | - | 0 (0%) | - | - | - | - | - | - |
| High grade (4) | 1 (25%) | 0 (0%) | 4 (100%) | 4 (100%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| AcCC (5) | 0 (0%) | 0 (0%) | 3 (60%) | 2 (40%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Low grade (2) | 0 (0%) | 0 (0%) | 1 (50%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| High grade (3) | 0 (0%) | 0 (0%) | 2 (66.67%) | 2 (66.67%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| BAC (1) | 0 (0%) | 0 (0%) | 1 (100%) | 1 (100%) | 1 (100%) | 1 (100%) | 0 (0%) | 0 (0%) |
| Low grade (1) | 0 (0%) | 0 (0%) | 1 (100%) | 1 (100%) | 1 (100%) | 1 (100%) | 0 (0%) | 0 (0%) |
| High grade (0) | - | - | - | - | - | - | - | - |
| SDC (1) | 1 (100%) | 0 (0%) | 1 (100%) | 1 (100%) | 0 (0%) | 0 (0%) | 1 (100%) | 0 (0%) |
| Low grade (0) | - | - | - | - | - | - | - | - |
| High grade (1) | 1 (100%) | 0 (0%) | 1 (100%) | 1 (100%) | 0 (0%) | 0 (0%) | 1 (100%) | 0 (0%) |
| EMC (1) | 0 (0%) | 0 (0%) | 1 (100%) | 1 (100%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Low grade (0) | - | - | - | - | - | - | - | - |
| High grade (1) | 0 (0%) | 0 (0%) | 1 (100%) | 1 (100%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| SCC (7) | 0 (0%) | 0 (0%) | 5 (71.43%) | 4 (57.14%) | 5 (71.43%) | 2 (28.57%) | 2 (28.57%) | 1 (14.29%) |
| Low grade (0) | - | - | - | - | - | - | - | - |
| High grade (7) | 0 (0%) | 0 (0%) | 5 (71.43%) | 4 (57.14%) | 5 (71.43%) | 2 (28.57%) | 2 (28.57%) | 1 (14.29%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pouloudi, D.; Manou, M.; Sarantis, P.; Tsoukalas, N.; Tsourouflis, G.; Dana, E.; Karamouzis, M.V.; Klijanienko, J.; Theocharis, S. Clinical Significance of Histone Deacetylase (HDAC)-1, -2, -4 and -6 Expression in Salivary Gland Tumors. Diagnostics 2021, 11, 517. https://doi.org/10.3390/diagnostics11030517
Pouloudi D, Manou M, Sarantis P, Tsoukalas N, Tsourouflis G, Dana E, Karamouzis MV, Klijanienko J, Theocharis S. Clinical Significance of Histone Deacetylase (HDAC)-1, -2, -4 and -6 Expression in Salivary Gland Tumors. Diagnostics. 2021; 11(3):517. https://doi.org/10.3390/diagnostics11030517
Chicago/Turabian StylePouloudi, Despoina, Maria Manou, Panagiotis Sarantis, Nikolaos Tsoukalas, Gerasimos Tsourouflis, Eougken Dana, Michalis V. Karamouzis, Jerzy Klijanienko, and Stamatios Theocharis. 2021. "Clinical Significance of Histone Deacetylase (HDAC)-1, -2, -4 and -6 Expression in Salivary Gland Tumors" Diagnostics 11, no. 3: 517. https://doi.org/10.3390/diagnostics11030517
APA StylePouloudi, D., Manou, M., Sarantis, P., Tsoukalas, N., Tsourouflis, G., Dana, E., Karamouzis, M. V., Klijanienko, J., & Theocharis, S. (2021). Clinical Significance of Histone Deacetylase (HDAC)-1, -2, -4 and -6 Expression in Salivary Gland Tumors. Diagnostics, 11(3), 517. https://doi.org/10.3390/diagnostics11030517