
Prediction of Hypertension Based on Facial Complexion


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Definition of Hypertension
2.3. Extraction of Facial Complexion Variables
2.3.1. Photography
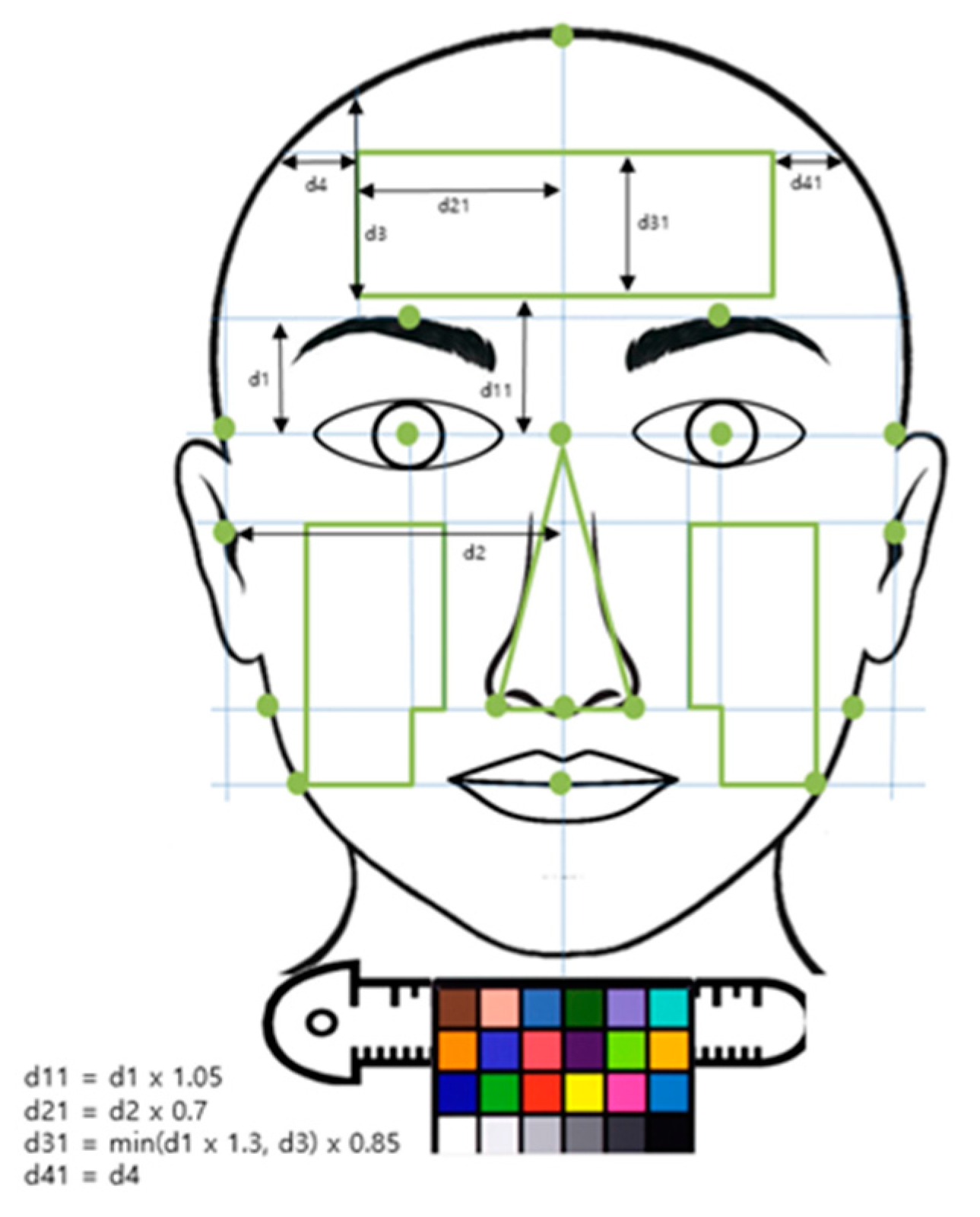
2.3.2. Image Processing
2.3.3. Extraction of Facial Complexion Variables
2.4. Statistical Analysis
2.4.1. Association Between Individual Complexion Variables and Hypertension
2.4.2. Prediction Models of Hypertension Using Combined Complexion Variables
3. Results
3.1. General Characteristics and Complexion Variables of the Subjects
3.2. Association Between Individual Complexion Variables and Hypertension
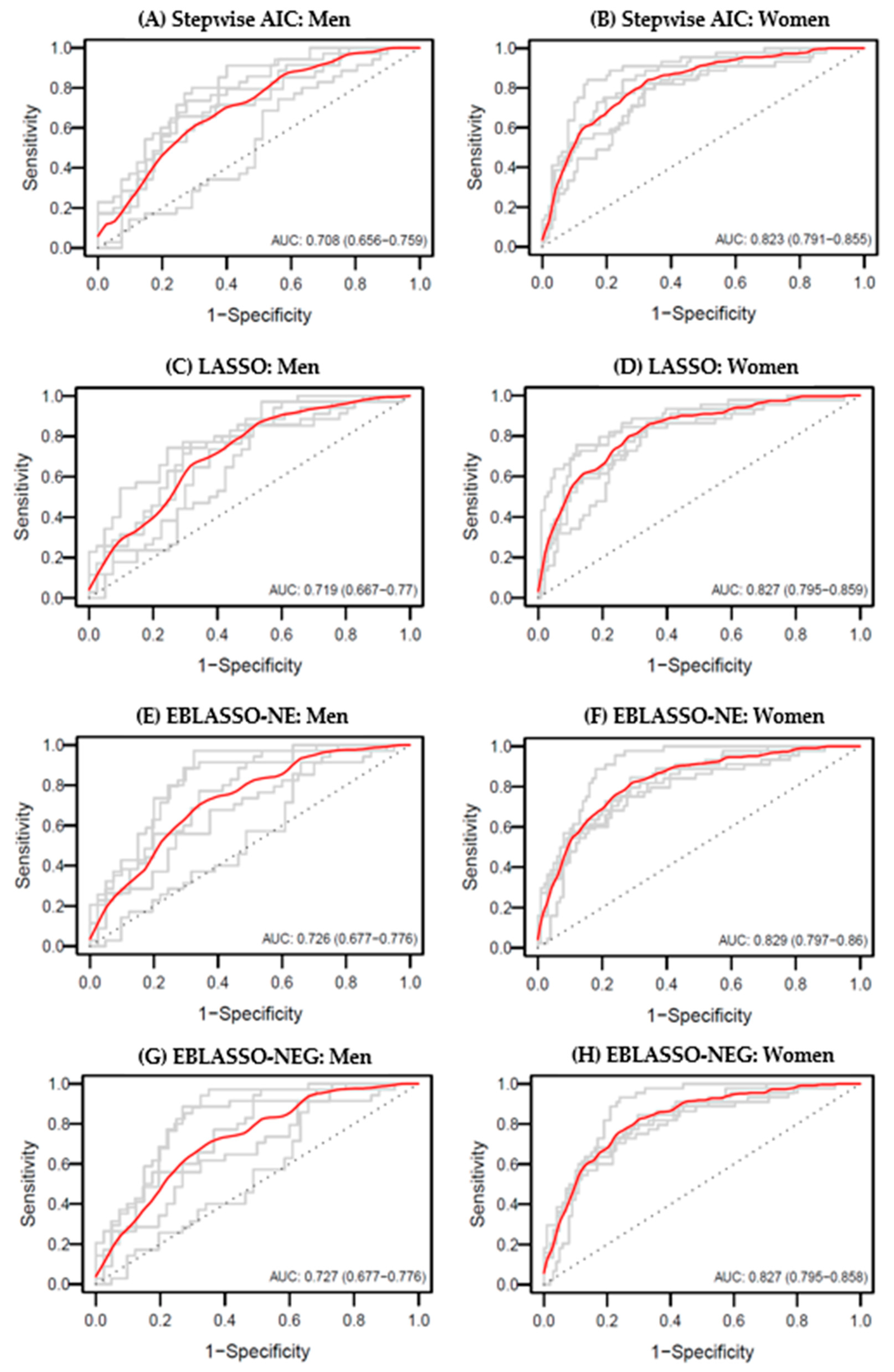
3.3. Comparison of the Predictive Powers for Hypertension Using Combined Complexion Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wolf-Maier, K.; Cooper, R.S.; Banegas, J.R.; Giampaoli, S.; Hense, H.W.; Joffres, M.; Kastarinen, M.; Poulter, N.; Primatesta, P.; Rodríguez-Artalejo, F.; et al. Hypertension prevalence and blood pressure levels in 6 European countries, Canada, and the United States. JAMA 2003, 289, 2363–2369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, R.B.; Suh, I.L.; Singh, V.P.; Chaithiraphan, S.; Laothavorn, P.; Sy, R.G.; Babilonia, N.A.; Rahman, A.R.A.; Sheikh, S.; Tomlinson, B.; et al. Hypertension and stroke in Asia: Prevalence, control and strategies in developing countries for prevention. J. Hum. Hypertens. 2000, 14, 749–763. [Google Scholar] [CrossRef] [Green Version]
- Ueshima, H.; Zhang, X.H.; Choudhury, S.R. Epidemiology of hypertension in China and Japan. J. Hum. Hypertens. 2000, 14, 765–769. [Google Scholar] [CrossRef] [Green Version]
- Hernandez-Hernandez, R.; Armas-Padilla, M.C.; Armas-Hernandez, M.J.; Velasco, M. Hypertension and cardiovascular health in Venezuela and Latin American countries. J. Hum. Hypertens. 2000, 14 (Suppl. 1), S2–S5. [Google Scholar] [CrossRef] [Green Version]
- Gupta, R. Hypertension in India—Definition, prevalence and evaluation. J. Indian Med. Assoc. 1999, 97, 74–80. [Google Scholar]
- Halberstein, R.A. Blood pressure in the Caribbean. Hum. Biol. 1999, 71, 659–684. [Google Scholar] [PubMed]
- Kearney, P.M.; Whelton, M.; Reynolds, K.; Muntner, P.; Whelton, P.K.; He, J. Global burden of hypertension: Analysis of worldwide data. Lancet 2005, 365, 217–223. [Google Scholar] [CrossRef]
- Kim, J.A.; Kim, S.M.; Choi, Y.S.; Yoon, D.; Lee, J.S.; Park, H.S.; Kim, H.A.; Lee, J.; Oh, H.J.; Choi, K.M. The prevalence and risk factors associated with isolated untreated systolic hypertension in Korea: The Korean National Health and Nutrition Survey 2001. J. Hum. Hypertens. 2007, 21, 107–113. [Google Scholar] [CrossRef]
- Kim, B.G.; Park, J.T.; Ahn, Y.; Kimm, K.; Shin, C. Geographical difference in the prevalence of isolated systolic hypertension in middle-aged men and women in Korea: The Korean Health and Genome Study. J. Hum. Hypertens. 2005, 19, 877–883. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.S.; Jones, D.W.; Kim, S.J.; Hong, Y.P. Hypertension in Korea: A national survey. Am. J. Prev. Med. 1994, 10, 200–204. [Google Scholar] [CrossRef]
- Jo, I.; Ahn, Y.; Lee, J.; Shin, K.R.; Lee, H.K.; Shin, C. Prevalence, awareness, treatment, control and risk factors of hypertension in Korea: The Ansan study. J. Hypertens. 2001, 19, 1523–1532. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Yang, D.H.; Park, H.S.; Cho, Y.; Jun, J.E.; Park, W.H.; Chun, B.Y.; Shin, J.-Y.; Shin, D.H.; Lee, K.S.; et al. Incidence of Hypertension in Korea: 5-Year Follow-up Study. J. Korean Med. Sci. 2011, 26, 1286–1292. [Google Scholar] [CrossRef]
- Williams, D.R. Black-White differences in blood pressure: The role of social factors. Ethn. Dis. 1992, 2, 126–141. [Google Scholar] [PubMed]
- Whelton, P.K. Epidemiology of hypertension. Lancet 1994, 344, 101–106. [Google Scholar] [CrossRef]
- Lee, B.J.; Kim, J.Y. A Comparison of the Predictive Power of Anthropometric Indices for Hypertension and Hypotension Risk. PLoS ONE 2014, 9, e84897. [Google Scholar] [CrossRef]
- Gravlee, C.C.; Dressler, W.W.; Bernard, H.R. Skin Color, Social Classification, and Blood Pressure in Southeastern Puerto Rico. Am. J. Public Health 2005, 95, 2191–2197. [Google Scholar] [CrossRef] [PubMed]
- Mosley, J.D.; Appel, L.J.; Ashour, Z.; Coresh, J.; Whelton, P.K.; Ibrahim, M.M. Relationship between skin color and blood pressure in egyptian adults: Results from the national hypertension project. Hypertension 2000, 36, 296–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gravlee, C.C.; Dressler, W.W. Skin pigmentation, self-perceived color, and arterial blood pressure in Puerto Rico. Am. J. Hum. Biol. 2005, 17, 195–206. [Google Scholar] [CrossRef]
- Harburg, E.; Gleibermann, L.; Roeper, P.; Schork, M.A.; Schull, W.J. Skin color, ethnicity, and blood pressure I: Detroit blacks. Am. J. Public Health 1978, 68, 1177–1183. [Google Scholar] [CrossRef]
- Sweet, E.; McDade, T.W.; Kiefe, C.I.; Liu, K. Relationships between Skin Color, Income, and Blood Pressure among African Americans in the CARDIA Study. Am. J. Public Health 2007, 97, 2253–2259. [Google Scholar] [CrossRef] [PubMed]
- Dressler, W.W.; Balieiro, M.C.; Dos Santos, J.E. Culture, skin color, and arterial blood pressure in Brazil. Am. J. Hum. Biol. 1999, 11, 49–59. [Google Scholar] [CrossRef]
- Larson, S.; Cho, M.-C.; Tsioufis, K.; Yang, E. 2018 Korean society of hypertension guideline for the management of hypertension: A comparison of American, European, and Korean blood pressure guidelines. Eur. Heart J. 2020, 41, 1384–1386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, Y.J.; Do, J.-H.; Kim, H.; Kim, J.Y. Differences in Complexion between Cold- and Heat-Prescription Groups in Sasang Medicine. Evid. Based Complementary Altern. Med. 2017, 2017, 9701978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedman, J.; Hastie, T.; Tibshirani, R.; Simon, N.; Narasimhan, B.; Qian, J. Lasso and Elastic-Net Regularized Generalized Linear Models. Available online: https://glmnet.stanford.edu/ (accessed on 26 February 2021).
- Tibshirani, R. Regression Shrinkage and Selection via the Lasso. J. R. Stat. Soc. Ser. B (Methodol.) 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Hastie, T.; Qian, J. Glmnet Vignette. Available online: https://web.stanford.edu/~hastie/glmnet/glmnet_alpha.html (accessed on 27 February 2021).
- Huang, A.; Liu, D. EBglmnet Vignette. Available online: https://rdrr.io/cran/EBglmnet/f/ (accessed on 27 February 2021).
- Huang, A.; Xu, S.; Cai, X. Empirical Bayesian LASSO-logistic regression for multiple binary trait locus mapping. BMC Genet. 2013, 14, 5. [Google Scholar] [CrossRef] [Green Version]
- Park, T.; Casella, G. The Bayesian Lasso. J. Am. Stat. Assoc. 2008, 103, 681–686. [Google Scholar] [CrossRef]
- Huang, A.; Liu, D. Empirical Bayesian Lasso and Elastic Net Methods for Generalized Linear Models. Available online: http://search.r-project.org/library/EBglmnet/html/EBglmnet-package.html (accessed on 27 February 2021).
- LeDell, E.; Petersen, M.; van der Laan, M. Computationally efficient confidence intervals for cross-validated area under the ROC curve estimates. Electron. J. Stat. 2015, 9, 1583–1607. [Google Scholar] [CrossRef]
- LeDell, E.; Petersen, M.; Laan, M.v.d. Cross-Validated Area under the ROC Curve Confidence Intervals. Available online: https://rdrr.io/github/ledell/cvAUC/ (accessed on 27 February 2021).
- Birgita, M. Face Color under Varying Illumination-Analysis and Applications; Department of Electrical and Information Engineering and Infotech Oulu, University of Oulu: Oulu, Finland, 2002. [Google Scholar]
- Stone, M.C. Hypertension. The influence of age, sex and other risk factors. J. R. Coll. Gen. Pract. Occas. Pap. 1980, 12, 6–10. [Google Scholar]
- Dua, S.; Bhuker, M.; Sharma, P.; Dhall, M.; Kapoor, S. Body Mass Index Relates to Blood Pressure among Adults. N. Am. J. Med Sci. 2014, 6, 89–95. [Google Scholar] [CrossRef] [Green Version]
- Mungreiphy, N.K.; Kapoor, S.; Sinha, R. Association between BMI, Blood Pressure, and Age: Study among Tangkhul Naga Tribal Males of Northeast India. J. Anthropol. 2011, 2011, 748147. [Google Scholar] [CrossRef] [Green Version]
- WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004, 363, 157–163. [Google Scholar] [CrossRef]
- Edwards, E.A.; Duntley, S.Q. The pigments and color of living human skin. Am. J. Anat. 1939, 65, 1–33. [Google Scholar] [CrossRef]
- Johnson, J.M. Physical training and the control of skin blood flow. Med. Sci. Sports Exerc. 1998, 30, 382–386. [Google Scholar] [CrossRef]
- Lee, H.Y.; Park, J.B. The Korean Society of Hypertension Guidelines for the Management of Hypertension in 2013: Its Essentials and Key Points. Pulse 2015, 3, 21–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russell, R.P. Side effects of calcium channel blockers. Hypertension 1988, 11, II42–II44. [Google Scholar] [CrossRef] [Green Version]
- Kitamura, K.; Kanasashi, M.; Suga, C.; Saito, S.; Yoshida, S.; Ikezawa, Z. Cutaneous reactions induced by calcium channel blocker: High frequency of psoriasiform eruptions. J. Dermatol. 1993, 20, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Hua, T.-C.; Chung, P.-I.; Chen, Y.-J.; Wu, L.-C.; Chen, Y.-D.; Hwang, C.-Y.; Chu, S.-Y.; Chen, C.-C.; Lee, D.-D.; Chang, Y.-T.; et al. Cardiovascular comorbidities in patients with rosacea: A nationwide case-control study from Taiwan. J. Am. Acad. Dermatol. 2015, 73, 249–254. [Google Scholar] [CrossRef]
- Boyle, E., Jr. Biological patterns in hypertension by race, sex, body weight, and skin color. JAMA 1970, 213, 1637–1643. [Google Scholar] [CrossRef] [PubMed]
- Keil, J.E.; Tyroler, H.A.; Sandifer, S.H.; Boyle, E. Hypertension: Effects of social class and racial admixture: The results of a cohort study in the black population of Charleston, South Carolina. Am. J. Public Health 1977, 67, 634–639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keil, J.E.; Sandifer, S.H.; Loadholt, C.B.; Boyle, J.E. Skin color and education effects on blood pressure. Am. J. Public Health 1981, 71, 532–534. [Google Scholar] [CrossRef]
- Ernst, F.A.; Jackson, I.; Robertson, R.M.; Nevels, H.; Watts, E. Skin tone, hostility, and blood pressure in young normotensive African Americans. Ethn. Dis. 1997, 7, 34–40. [Google Scholar]
- Klag, M.J.; Whelton, P.K.; Coresh, J.; Grim, C.E.; Kuller, L.H. The association of skin color with blood pressure in US blacks with low socioeconomic status. JAMA 1991, 265, 599–602. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
| Variable Name | Description |
|---|---|
| Total_L* | L* value in the total face for lightness |
| Total_a* | a* value in the total face for green-red color components |
| Total_b* | b* value in the total face for blue-yellow color components |
| Fh_L* | L* value in the forehead for lightness |
| Fh_a* | a* value in the forehead for green-red color components |
| Fh_b* | b* value in the forehead for blue-yellow color components |
| Ch_L* | L* value in the cheek for lightness |
| Ch_a* | a* value in the cheek for green-red color components |
| Ch_b* | b* value in the cheek for blue-yellow color components |
| Ns_L* | L* value in the nose for lightness |
| Ns_a* | a* value in nose for green-red color components |
| Ns_b* | b* value in nose for blue-yellow color components |
| Variable | Men | Women | ||||
|---|---|---|---|---|---|---|
| Normal | Hypertensive | p-Value | Normal | Hypertensive | p-Value | |
| Subjects | 203 | 173 | − | 502 | 221 | − |
| Age | 43.36 ± 16.76 | 51.68 ± 13.05 | <0.001 | 43.85 ± 13.8 | 59.7 ± 12.64 | <0.001 |
| Height [cm] | 170.54 ± 6.42 | 170.62 ± 6.35 | 0.908 | 158.86 ± 5.67 | 155.54 ± 5.75 | <0.001 |
| Weight [kg] | 67.5 ± 9.83 | 73.44 ± 10.31 | <0.001 | 56.57 ± 8 | 59.94 ± 9.1 | <0.001 |
| BMI [kg/m2] | 23.18 ± 2.86 | 25.19 ± 2.89 | <0.001 | 22.42 ± 2.97 | 24.75 ± 3.27 | <0.001 |
| SBP [mmHg] | 115.03 ± 11.3 | 132.94 ± 15.53 | <0.001 | 110.45 ± 12.01 | 130.77 ± 16.39 | <0.001 |
| DBP [mmHg] | 73.02 ± 8.94 | 86.47 ± 11.13 | <0.001 | 70.98 ± 8.65 | 83.78 ± 11.44 | <0.001 |
| Receiving treatment (%) | − | 53.76 | − | − | 67.42 | − |
| Pulse rate [bpm] | 72.01 ± 9.96 | 70.97 ± 9.39 | 0.299 | 72.23 ± 9.62 | 75.06 ± 11.84 | 0.002 |
| Temperature [°C] | 36.28 ± 0.35 | 36.28 ± 0.35 | 0.921 | 36.38 ± 0.34 | 36.36 ± 0.4 | 0.500 |
| Total_L* | 60.98 ± 4.45 | 59.66 ± 4.13 | 0.003 | 65.73 ± 3.97 | 64.31 ± 4.81 | <0.001 |
| Total_a* | 13.9 ± 2.26 | 14.73 ± 2.32 | 0.001 | 11.57 ± 2.12 | 12.61 ± 2.25 | <0.001 |
| Total_b* | 21.24 ± 2.35 | 21.02 ± 2.35 | 0.369 | 20.87 ± 2.72 | 21.52 ± 2.85 | 0.004 |
| Fh_L* | 66.38 ± 5.31 | 65.01 ± 4.66 | 0.008 | 70.39 ± 4.94 | 69.48 ± 5.48 | 0.034 |
| Fh_a* | 12.78 ± 2.45 | 13.82 ± 2.35 | <0.001 | 9.94 ± 2.3 | 11.09 ± 2.43 | <0.001 |
| Fh_b* | 22.05 ± 2.7 | 22.04 ± 2.66 | 0.961 | 21.33 ± 3.07 | 22.12 ± 3.22 | 0.002 |
| Ch_L* | 57.32 ± 4.62 | 56.14 ± 4.26 | 0.011 | 62.46 ± 3.81 | 61 ± 4.79 | <0.001 |
| Ch_a* | 14.46 ± 2.32 | 15.16 ± 2.55 | 0.006 | 12.59 ± 2.17 | 13.49 ± 2.31 | <0.001 |
| Ch_b* | 20.77 ± 2.39 | 20.42 ± 2.46 | 0.169 | 20.64 ± 2.74 | 21.21 ± 2.87 | 0.012 |
| Ns_L* | 66 ± 5.15 | 64.69 ± 5.08 | 0.014 | 70.47 ± 5.45 | 68.66 ± 5.87 | <0.001 |
| Ns_a* | 15.68 ± 2.56 | 16.48 ± 2.65 | 0.003 | 11.68 ± 2.53 | 12.8 ± 2.82 | <0.001 |
| Ns_b* | 20.63 ± 2.43 | 20.51 ± 2.59 | 0.661 | 19.92 ± 3.03 | 20.71 ± 3.07 | 0.002 |
| Variable | Crude | Adjusted | ||||
|---|---|---|---|---|---|---|
| p-Value | OR (95% CI) | AUC (95% CI) | p-Value | OR (95% CI) | AUC (95% CI) | |
| Age | <0.001 | 1.741 (1.406–2.176) | 0.649 (0.595–0.704) | − | − | − |
| BMI | <0.001 | 2.202 (1.72–2.864) | 0.698 (0.645–0.75) | − | − | − |
| SBP | <0.001 | 6.032 (4.162–9.127) | 0.821 (0.774–0.868) | <0.001 | 5.526 (3.752–8.509) | 0.855 (0.817–0.893) |
| DBP | <0.001 | 5.07 (3.634–7.351) | 0.836 (0.789–0.883) | <0.001 | 6.115 (4.155–9.424) | 0.880 (0.845–0.915) |
| Total_L* | 0.004 | 0.703 (0.551–0.889) | 0.588 (0.531–0.646) | 0.434 | 0.899 (0.688–1.172) | 0.733 (0.683–0.782) |
| Total_a* | 0.001 | 1.491 (1.187–1.889) | 0.595 (0.538–0.652) | 0.741 | 1.046 (0.8–1.368) | 0.734 (0.684–0.783) |
| Total_b* | 0.368 | 0.9 (0.715–1.131) | 0.452 (0.394–0.51) | 0.189 | 0.846 (0.656–1.085) | 0.726 (0.676–0.775) |
| Fh_L* | 0.009 | 0.738 (0.585–0.925) | 0.579 (0.521–0.636) | 0.221 | 0.855 (0.665–1.097) | 0.733 (0.683–0.782) |
| Fh_a* | <0.001 | 1.663 (1.304–2.142) | 0.615 (0.559–0.672) | 0.343 | 1.148 (0.864–1.529) | 0.736 (0.687–0.785) |
| Fh_b* | 0.961 | 0.994 (0.792–1.248) | 0.435 (0.377–0.493) | 0.487 | 0.916 (0.713–1.174) | 0.723 (0.673–0.773) |
| Ch_L* | 0.012 | 0.744 (0.588–0.935) | 0.578 (0.52–0.636) | 0.762 | 0.96 (0.737–1.248) | 0.731 (0.682–0.78) |
| Ch_a* | 0.007 | 1.345 (1.089–1.672) | 0.578 (0.52–0.636) | 0.984 | 1.002 (0.784–1.279) | 0.732 (0.683–0.782) |
| Ch_b* | 0.168 | 0.853 (0.678–1.068) | 0.55 (0.491–0.608) | 0.100 | 0.813 (0.634–1.039) | 0.727 (0.677–0.777) |
| Ns_L* | 0.015 | 0.744 (0.583–0.942) | 0.583 (0.525–0.641) | 0.282 | 0.866 (0.665–1.124) | 0.734 (0.685–0.784) |
| Ns_a* | 0.003 | 1.479 (1.142–1.929) | 0.595 (0.538–0.652) | 0.932 | 1.013 (0.75–1.366) | 0.730 (0.681–0.78) |
| Ns_b* | 0.658 | 0.948 (0.749–1.199) | 0.466 (0.408–0.524) | 0.386 | 0.891 (0.686–1.155) | 0.724 (0.675–0.774) |
| Variable | Crude | Adjusted | ||||
|---|---|---|---|---|---|---|
| p-Value | OR (95% CI) | AUC (95% CI) | p-Value | OR (95% CI) | AUC (95% CI) | |
| Age | <0.001 | 3.832 (3.062–4.87) | 0.804 (0.769–0.838) | − | − | − |
| BMI | <0.001 | 2.127 (1.786–2.553) | 0.706 (0.665–0.747) | − | − | − |
| SBP | <0.001 | 6.417 (4.833–8.735) | 0.84 (0.805–0.874) | <0.001 | 4.824 (3.559–6.71) | 0.895 (0.871–0.919) |
| DBP | <0.001 | 5.584 (4.228–7.555) | 0.815 (0.776–0.853) | <0.001 | 5.257 (3.848–7.405) | 0.906 (0.883–0.928) |
| Total_L* | <0.001 | 0.677 (0.558–0.817) | 0.58 (0.533–0.627) | 0.007 | 0.746 (0.601–0.921) | 0.830 (0.798–0.862) |
| Total_a* | <0.001 | 1.727 (1.434–2.09) | 0.639 (0.595–0.683) | 0.018 | 1.302 (1.047–1.622) | 0.828 (0.797–0.86) |
| Total_b* | 0.004 | 1.252 (1.076–1.46) | 0.571 (0.525–0.616) | 0.560 | 1.056 (0.88–1.267) | 0.824 (0.792–0.856) |
| Fh_L* | 0.028 | 0.823 (0.691–0.977) | 0.539 (0.492–0.585) | 0.020 | 0.789 (0.645–0.962) | 0.829 (0.797–0.861) |
| Fh_a* | <0.001 | 1.785 (1.472–2.176) | 0.646 (0.602–0.689) | 0.010 | 1.342 (1.073–1.685) | 0.828 (0.796–0.86) |
| Fh_b* | 0.002 | 1.273 (1.093–1.485) | 0.57 (0.525–0.616) | 0.668 | 1.041 (0.867–1.252) | 0.824 (0.791–0.856) |
| Ch_L* | <0.001 | 0.65 (0.531–0.791) | 0.593 (0.546–0.639) | 0.017 | 0.763 (0.609–0.95) | 0.829 (0.797–0.861) |
| Ch_a* | <0.001 | 1.557 (1.304–1.867) | 0.616 (0.572–0.66) | 0.060 | 1.223 (0.992–1.51) | 0.827 (0.795–0.859) |
| Ch_b* | 0.011 | 1.221 (1.048–1.425) | 0.562 (0.516–0.607) | 0.473 | 1.069 (0.89–1.285) | 0.824 (0.792–0.856) |
| Ns_L* | <0.001 | 0.707 (0.593–0.838) | 0.588 (0.542–0.633) | 0.004 | 0.752 (0.617–0.913) | 0.83 (0.799–0.862) |
| Ns_a* | <0.001 | 1.681 (1.379–2.057) | 0.617 (0.572–0.662) | 0.007 | 1.381 (1.096–1.748) | 0.829 (0.798–0.861) |
| Ns_b* | 0.002 | 1.274 (1.097–1.487) | 0.57 (0.524–0.615) | 0.606 | 1.049 (0.877–1.258) | 0.824 (0.792–0.856) |
| Variable Subset Selection Method | Number of Selected Variables | Selected Variables | AUC (95% CI) |
|---|---|---|---|
| Men | |||
| Stepwise AIC | 3 | BMI, Age, Ch_b* | 0.708 (0.656–0.759) |
| LASSO | 3 | BMI, Age, Fh_a* | 0.719 (0.667–0.77) |
| EBLASSO-NE | 5 | BMI, Age, Fh_L*, Fh_a*, Ch_b* | 0.726 (0.677–0.776) |
| EBLASSO-NEG | 2 | BMI, Age | 0.727 (0.677–0.776) |
| Women | |||
| Stepwise AIC | 6 | BMI, Age, Total_L*, Fh_L*, Fh_a*, Ch_L* | 0.823 (0.791–0.855) |
| LASSO | 6 | BMI, Age, Total_L*, Fh_a*, Ns_L*, Ns_a* | 0.827 (0.795–0.859) |
| EBLASSO-NE | 6 | BMI, Age, Total_L*, Fh_a*, Ns_L*, Ns_a* | 0.829 (0.797–0.86) |
| EBLASSO-NEG | 4 | BMI, Age, Fh_a*, Ns_L* | 0.827 (0.795–0.858) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ang, L.; Lee, B.J.; Kim, H.; Yim, M.H. Prediction of Hypertension Based on Facial Complexion. Diagnostics 2021, 11, 540. https://doi.org/10.3390/diagnostics11030540
Ang L, Lee BJ, Kim H, Yim MH. Prediction of Hypertension Based on Facial Complexion. Diagnostics. 2021; 11(3):540. https://doi.org/10.3390/diagnostics11030540
Chicago/Turabian StyleAng, Lin, Bum Ju Lee, Honggie Kim, and Mi Hong Yim. 2021. "Prediction of Hypertension Based on Facial Complexion" Diagnostics 11, no. 3: 540. https://doi.org/10.3390/diagnostics11030540
APA StyleAng, L., Lee, B. J., Kim, H., & Yim, M. H. (2021). Prediction of Hypertension Based on Facial Complexion. Diagnostics, 11(3), 540. https://doi.org/10.3390/diagnostics11030540