
Mesonephric-Like Carcinosarcoma of the Ovary Associated with Low-Grade Serous Carcinoma: A Case Report

 , , , , ,
, , , , ,  , and
, and
Abstract
:1. Introduction
2. Case Presentation
2.1. Clinical History
2.2. Pathological Findings
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- McFarland, M.; Quick, C.M.; McCluggage, W.G. Hormone receptor-negative, thyroid transcription factor 1-positive uterine and ovarian adenocarcinomas: Report of a series of mesonephric-like adenocarcinomas. Histopathology 2016, 68, 1013–1020. [Google Scholar] [CrossRef] [PubMed]
- Mueller, I.; Kametriser, G.; Jacobs, V.R.; Bogner, G.; Staudach, A.; Koch, H.; Wolfrum-Ristau, P.; Schausberger, C.; Fischer, T.; Sedlmayer, F. Mesonephric adenocarcinoma of the vagina: Diagnosis and multimodal treatment of a rare tumor and analysis of worldwide experience. Strahlenther. Onkol. 2016, 192, 668–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horn, L.C.; Hohn, A.K.; Krucken, I.; Stiller, M.; Obeck, U.; Brambs, C.E. Mesonephric-like adenocarcinomas of the uterine corpus: Report of a case series and review of the literature indicating poor prognosis for this subtype of endometrial adenocarcinoma. J. Cancer Res. Clin. Oncol. 2020, 146, 971–983. [Google Scholar] [CrossRef] [PubMed]
- Huffman, J.W. Mesonephric remnants in the cervix. Am. J. Obstet. Gynecol. 1948, 56, 23–40. [Google Scholar] [CrossRef]
- Ferry, J.A.; Scully, R.E. Mesonephric remnants, hyperplasia, and neoplasia in the uterine cervix. A study of 49 cases. Am. J. Surg. Pathol. 1990, 14, 1100–1111. [Google Scholar] [CrossRef] [PubMed]
- WHO Classification of Tumours EB. Female Genital Tumours, 5th ed; WHO Classification of Tumours Series; International Agency for Research on Cancer: Lyon, France, 2020; Volume 4, Available online: https://tumourclassification.iarc.who.int/chapters/34 (accessed on 3 May 2021).
- Seay, K.; Akanbi, T.; Bustamante, B.; Chaudhary, S.; Goldberg, G.L. Mesonephric-like adenocarcinoma of the ovary with co-existent endometriosis: A case report and review of the literature. Gynecol. Oncol. Rep. 2020, 34, 100657. [Google Scholar] [CrossRef] [PubMed]
- McCluggage, W.G.; Vosmikova, H.; Laco, J. Ovarian Combined Low-grade Serous and Mesonephric-like Adenocarcinoma: Further Evidence for A Mullerian Origin of Mesonephric-like Adenocarcinoma. Int. J. Gynecol. Pathol. 2020, 39, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Dundr, P.; Gregova, M.; Nemejcova, K.; Bartu, M.; Hajkova, N.; Hojny, J.; Struzinska, I.; Fischerova, D. Ovarian mesonephric-like adenocarcinoma arising in serous borderline tumor: A case report with complex morphological and molecular analysis. Diagn. Pathol. 2020, 15, 91. [Google Scholar] [CrossRef] [PubMed]
- Mirkovic, J.; McFarland, M.; Garcia, E.; Sholl, L.M.; Lindeman, N.; MacConaill, L.; Dong, F.; Hirsch, M.; Nucci, M.R.; Quick, C.M.; et al. Targeted Genomic Profiling Reveals Recurrent KRAS Mutations in Mesonephric-like Adenocarcinomas of the Female Genital Tract. Am. J. Surg. Pathol. 2018, 42, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Chapel, D.B.; Joseph, N.M.; Krausz, T.; Lastra, R.R. An Ovarian Adenocarcinoma With Combined Low-grade Serous and Mesonephric Morphologies Suggests a Mullerian Origin for Some Mesonephric Carcinomas. Int. J. Gynecol. Pathol. 2018, 37, 448–459. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, Y.; Akagi, A.; Izumi, K.; Kishi, Y. Carcinosarcoma of the uterine body of mesonephric origin. Pathol. Int. 1995, 45, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Meguro, S.; Yasuda, M.; Shimizu, M.; Kurosaki, A.; Fujiwara, K. Mesonephric adenocarcinoma with a sarcomatous component, a notable subtype of cervical carcinosarcoma: A case report and review of the literature. Diagn. Pathol. 2013, 8, 74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roma, A.A. Mesonephric carcinosarcoma involving uterine cervix and vagina: Report of 2 cases with immunohistochemical positivity For PAX2, PAX8, and GATA-3. Int. J. Gynecol. Pathol. 2014, 33, 624–629. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, B.; Silva, R.; Dias, R.; Patricio, V. Carcinosarcoma of the uterine cervix: A rare pathological finding originating from mesonephric remnants. BMJ Case Rep. 2019, 12. [Google Scholar] [CrossRef] [PubMed]
- Howitt, B.E.; Nucci, M.R. Mesonephric proliferations of the female genital tract. Pathology 2018, 50, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Howitt, B.E.; Emori, M.M.; Drapkin, R.; Gaspar, C.; Barletta, J.A.; Nucci, M.R.; McCluggage, W.G.; Oliva, E.; Hirsch, M.S. GATA3 Is a Sensitive and Specific Marker of Benign and Malignant Mesonephric Lesions in the Lower Female Genital Tract. Am. J. Surg. Pathol. 2015, 39, 1411–1419. [Google Scholar] [CrossRef] [PubMed]
- Kenny, S.L.; McBride, H.A.; Jamison, J.; McCluggage, W.G. Mesonephric adenocarcinomas of the uterine cervix and corpus: HPV-negative neoplasms that are commonly PAX8, CA125, and HMGA2 positive and that may be immunoreactive with TTF1 and hepatocyte nuclear factor 1-beta. Am. J. Surg. Pathol. 2012, 36, 799–807. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Low-Grade Serous Component | Mesonephric-Like Component | Sarcomatous Component | |
|---|---|---|---|
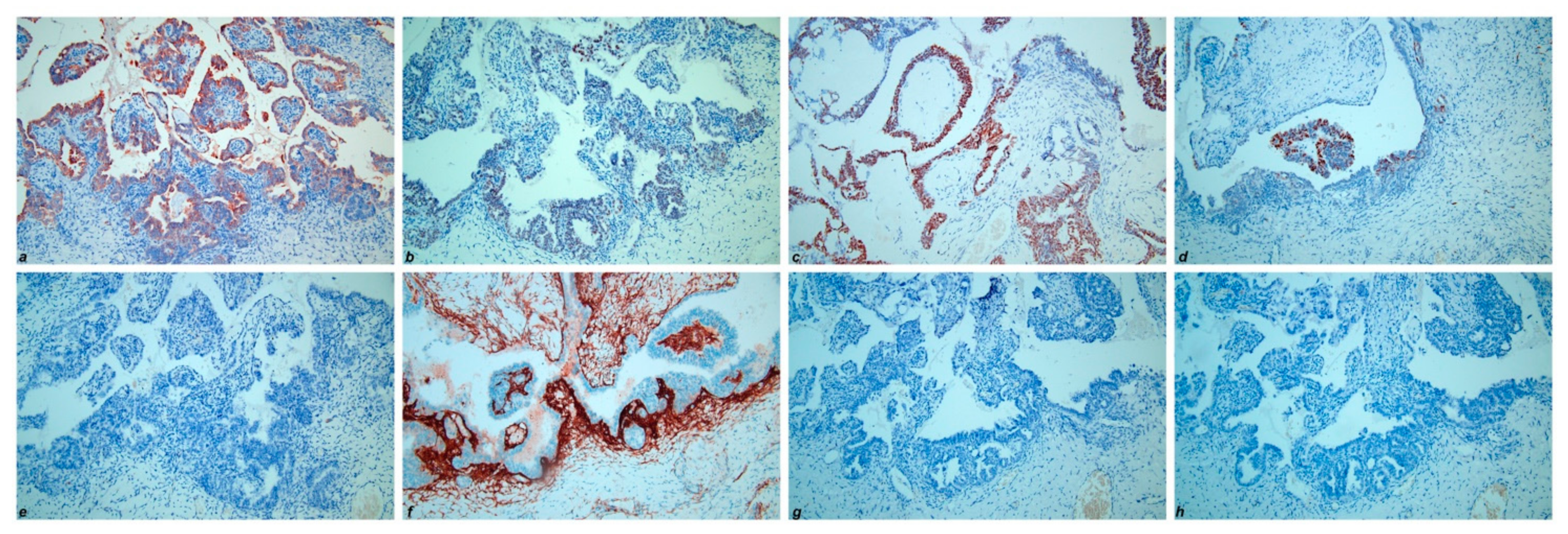
| CK7 | + | + | + |
| PAX8 | + | + | + |
| ER | + | - | - |
| PR | + | - | - |
| Calretinin | - | + | + |
| CD10 | - | + | + |
| TTF-1 | - | + | + |
| GATA-3 | - | + | + |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
d’Amati, A.; Pezzuto, F.; Serio, G.; Marzullo, A.; Fortarezza, F.; Lettini, T.; Cazzato, G.; Cormio, G.; Resta, L. Mesonephric-Like Carcinosarcoma of the Ovary Associated with Low-Grade Serous Carcinoma: A Case Report. Diagnostics 2021, 11, 827. https://doi.org/10.3390/diagnostics11050827
d’Amati A, Pezzuto F, Serio G, Marzullo A, Fortarezza F, Lettini T, Cazzato G, Cormio G, Resta L. Mesonephric-Like Carcinosarcoma of the Ovary Associated with Low-Grade Serous Carcinoma: A Case Report. Diagnostics. 2021; 11(5):827. https://doi.org/10.3390/diagnostics11050827
Chicago/Turabian Styled’Amati, Antonio, Federica Pezzuto, Gabriella Serio, Andrea Marzullo, Francesco Fortarezza, Teresa Lettini, Gerardo Cazzato, Gennaro Cormio, and Leonardo Resta. 2021. "Mesonephric-Like Carcinosarcoma of the Ovary Associated with Low-Grade Serous Carcinoma: A Case Report" Diagnostics 11, no. 5: 827. https://doi.org/10.3390/diagnostics11050827