
Detection and Severity Classification of COVID-19 in CT Images Using Deep Learning

 ,
,  , ,
, ,  ,
,  , , and
, , and
Abstract
:1. Introduction
1.1. Related Work
1.2. Motivation
2. Methodology
2.1. CT Datasets
2.2. Pre-Processing
2.3. Network Models for Lung and Lesion Segmentation and Classification
2.4. The Proposed Approach for COVI-19 Detection and Severity Classification
3. Experimental Setup
3.1. Data Preparation and Augmentation
3.2. Evaluation Criteria
4. Results and Discussion
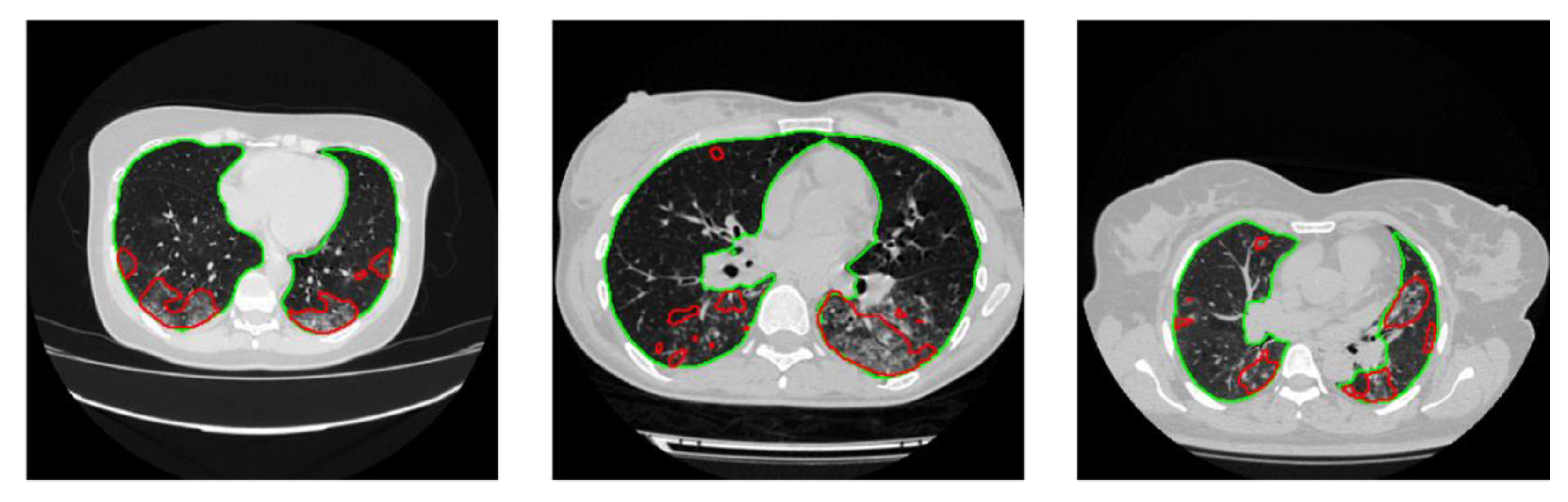
4.1. Lung Segmentation
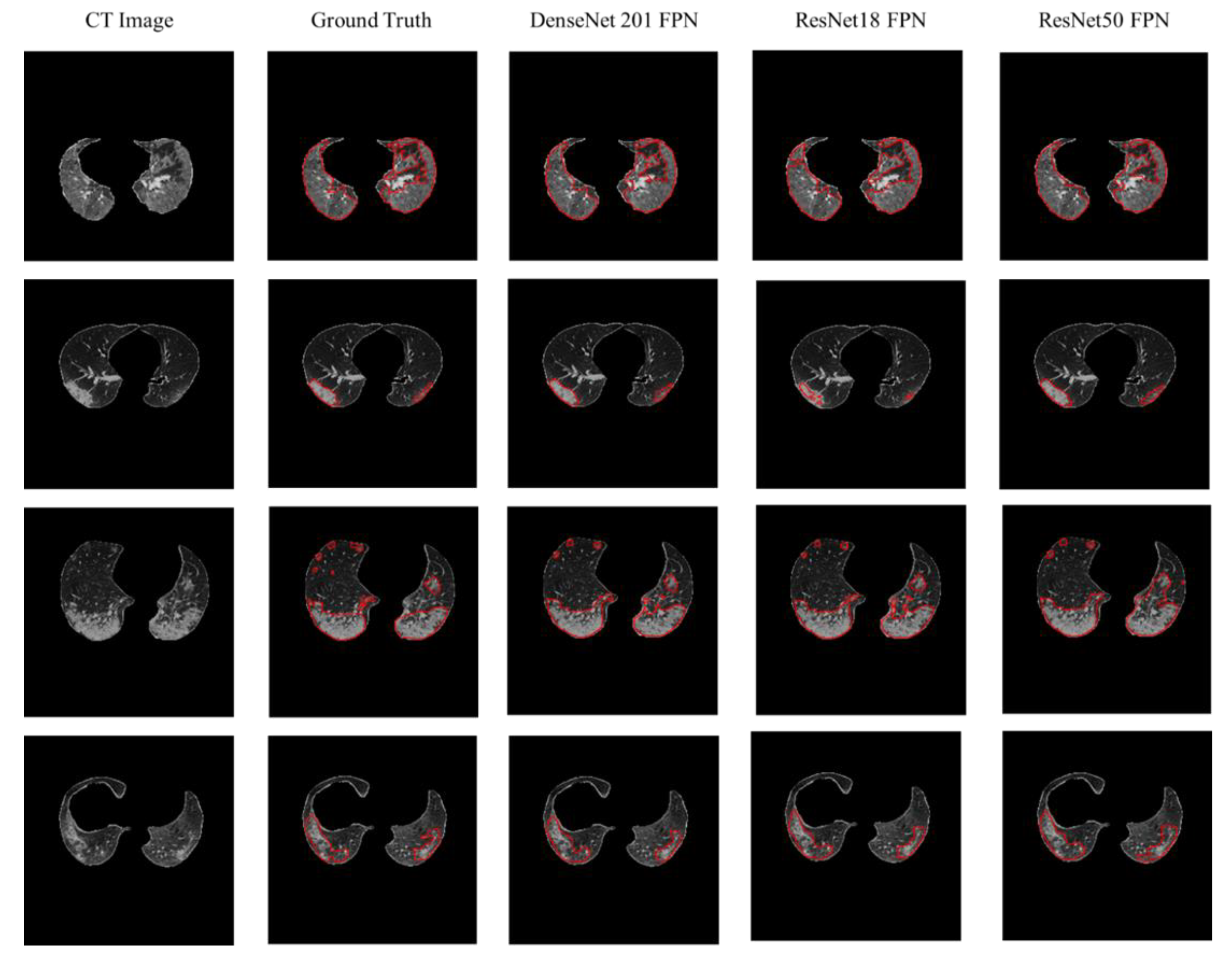
4.2. Lesion Segmentation
4.3. COVID-19 Detection
4.4. Severity Classification Using MosMedData Dataset
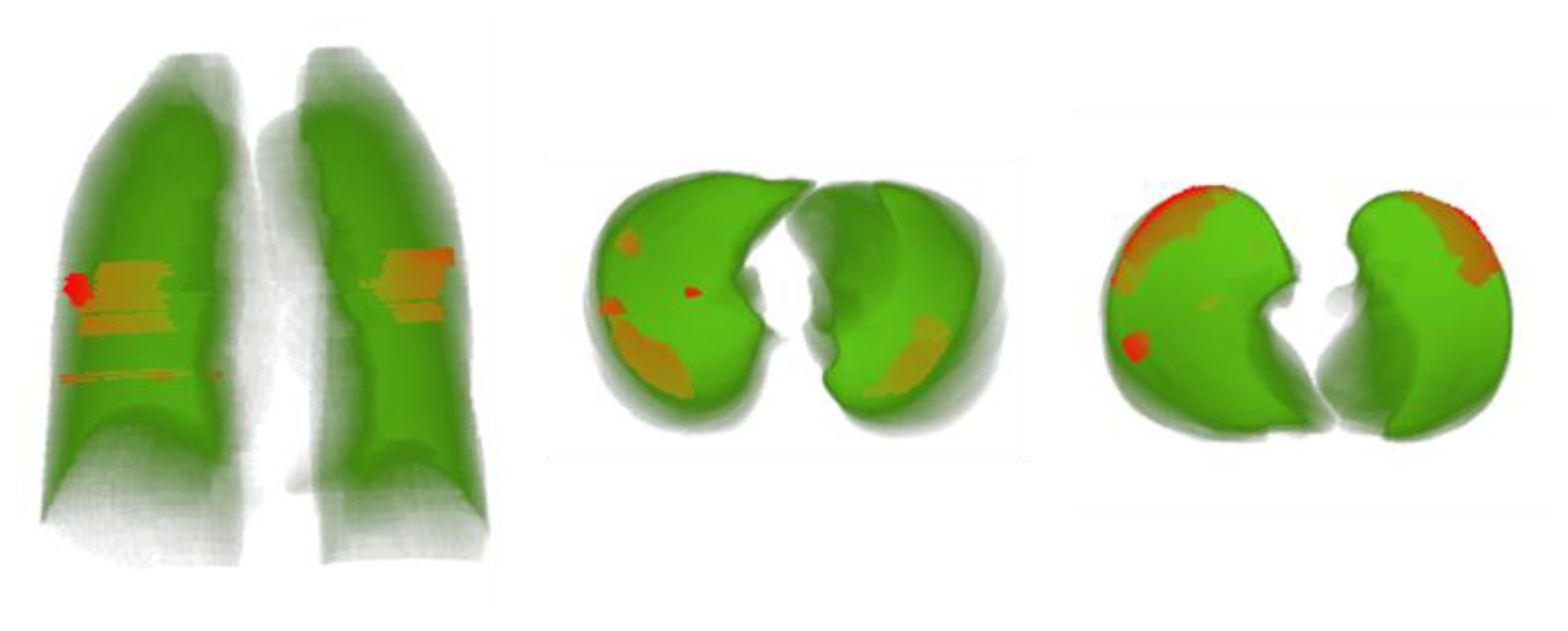
4.5. 3D Modeling of Lung Volume with Lesion Visualization
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Weekly Epidemiological Update on COVID-19, 15 December 2020; World Health Organization: Geneva, Switzerland, 2020; p. 21. [Google Scholar]
- Craw, P.; Balachandran, W. Isothermal nucleic acid amplification technologies for point-of-care diagnostics: A critical review. Lab Chip 2012, 12, 2469–2486. [Google Scholar] [CrossRef]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Eurosurveillance 2020, 25, 2000045. [Google Scholar] [CrossRef] [Green Version]
- Kakodkar, P.; Kaka, N.; Baig, M.N. A Comprehensive Literature Review on the Clinical Presentation, and Management of the Pandemic Coronavirus Disease 2019 (COVID-19). Cureus 2020, 12, e7560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubin, G.D.; Ryerson, C.J.; Haramati, L.B.; Sverzellati, N.; Kanne, J.P.; Raoof, S.; Schluger, N.W.; Volpi, A.; Yim, J.-J.; Martin, I.B.K.; et al. The Role of Chest Imaging in Patient Management during the COVID-19 Pandemic: A Multinational Consensus Statement from the Fleischner Society. Radiology 2020, 296, 172–180. [Google Scholar] [CrossRef] [Green Version]
- Salehi, S.; Abedi, A.; Balakrishnan, S.; Gholamrezanezhad, A. Coronavirus Disease 2019 (COVID-19): A Systematic Review of Imaging Findings in 919 Patients. Am. J. Roentgenol. 2020, 215, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.; Zhang, H.; Xie, J.; Lin, M.; Ying, L.; Pang, P.; Ji, W. Sensitivity of Chest CT for COVID-19: Comparison to RT-PCR. Radiology 2020, 296, E115–E117. [Google Scholar] [CrossRef] [PubMed]
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of chest CT and RT-PCR testing in coronavirus disease 2019 (COVID-19) in China: A report of 1014 cases. Radiology 2020, 296, E32–E40. [Google Scholar] [CrossRef] [Green Version]
- Shi, H.; Han, X.; Jiang, N.; Cao, Y.; Alwalid, O.; Gu, J.; Fan, Y.; Zheng, C. Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: A descriptive study. Lancet Infect. Dis. 2020, 20, 425–434. [Google Scholar] [CrossRef]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef]
- Dong, H.; Yang, G.; Liu, F.; Mo, Y.; Guo, Y. Automatic brain tumor detection and segmentation using U-Net based fully convolutional networks. In Proceedings of the Annual Conference on Medical Image Understanding and Analysis, Edinburgh, UK, 11–13 July 2017; pp. 506–517. [Google Scholar]
- Shen, L.; Margolies, L.R.; Rothstein, J.H.; Fluder, E.; McBride, R.; Sieh, W. Deep learning to improve breast cancer detection on screening mammography. Sci. Rep. 2019, 9, 12495. [Google Scholar] [CrossRef]
- Ardila, D.; Kiraly, A.P.; Bharadwaj, S.; Choi, B.; Reicher, J.J.; Peng, L.; Tse, D.; Etemadi, M.; Ye, W.; Corrado, G. End-to-end lung cancer screening with three-dimensional deep learning on low-dose chest computed tomography. Nat. Med. 2019, 25, 954–961. [Google Scholar] [CrossRef] [PubMed]
- Tahir, A.; Qiblawey, Y.; Khandakar, A.; Rahman, T.; Khurshid, U.; Musharavati, F.; Kiranyaz, S.; Chowdhury, M.E. Coronavirus: Comparing COVID-19, SARS and MERS in the eyes of AI. arXiv 2020, arXiv:1706.05587. [Google Scholar]
- Xu, X.; Jiang, X.; Ma, C.; Du, P.; Li, X.; Lv, S.; Yu, L.; Ni, Q.; Chen, Y.; Su, J.; et al. A Deep Learning System to Screen Novel Coronavirus Disease 2019 Pneumonia. Engineering 2020. [Google Scholar] [CrossRef]
- Huang, L.; Han, R.; Ai, T.; Yu, P.; Kang, H.; Tao, Q.; Xia, L. Serial Quantitative Chest CT Assessment of COVID-19: Deep-Learning Approach. Radiol. Cardiothorac. Imaging 2020, 2, e200075. [Google Scholar] [CrossRef] [Green Version]
- Fan, D.P.; Zhou, T.; Ji, G.P.; Zhou, Y.; Chen, G.; Fu, H.; Shen, J.; Shao, L. Inf-Net: Automatic COVID-19 Lung Infection Segmentation From CT Images. IEEE Trans. Med. Imaging 2020, 39, 2626–2637. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.; Xia, L.; Yan, F.; Wan, Z.; Shi, F.; Yuan, H.; Jiang, H.; Wu, D.; Sui, H.; Zhang, C.; et al. Diagnosis of Coronavirus Disease 2019 (COVID-19) With Structured Latent Multi-View Representation Learning. IEEE Trans. Med. Imaging 2020, 39, 2606–2614. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Zha, Y.; Li, W.; Wu, Q.; Li, X.; Niu, M.; Wang, M.; Qiu, X.; Li, H.; Yu, H.; et al. A Fully Automatic Deep Learning System for COVID-19 Diagnostic and Prognostic Analysis. Eur. Respir. J. 2020, 56, 2000775. [Google Scholar] [CrossRef]
- Harmon, S.A.; Sanford, T.H.; Xu, S.; Turkbey, E.B.; Roth, H.; Xu, Z.; Yang, D.; Myronenko, A.; Anderson, V.; Amalou, A.; et al. Artificial intelligence for the detection of COVID-19 pneumonia on chest CT using multinational datasets. Nat. Commun. 2020, 11, 4080. [Google Scholar] [CrossRef]
- Wang, Q.; Yang, D.; Li, Z.; Zhang, X.; Liu, C. Deep Regression via Multi-Channel Multi-Modal Learning for Pneumonia Screening. IEEE Access 2020, 8, 78530–78541. [Google Scholar] [CrossRef]
- Mei, X.; Lee, H.-C.; Diao, K.-y.; Huang, M.; Lin, B.; Liu, C.; Xie, Z.; Ma, Y.; Robson, P.M.; Chung, M.; et al. Artificial intelligence–enabled rapid diagnosis of patients with COVID-19. Nat. Med. 2020, 26, 1224–1228. [Google Scholar] [CrossRef]
- Zhou, L.; Li, Z.; Zhou, J.; Li, H.; Chen, Y.; Huang, Y.; Xie, D.; Zhao, L.; Fan, M.; Hashmi, S.; et al. A rapid, accurate and machine-agnostic segmentation and quantification method for CT-based covid-19 diagnosis. IEEE Trans. Med. Imaging 2020, 39, 2638–2652. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Liu, X.; Li, C.; Xu, Z.; Ruan, J.; Zhu, H.; Meng, T.; Li, K.; Huang, N.; Zhang, S. A noise-robust framework for automatic segmentation of covid-19 pneumonia lesions from ct images. IEEE Trans. Med. Imaging 2020, 39, 2653–2663. [Google Scholar] [CrossRef]
- Wang, X.; Deng, X.; Fu, Q.; Zhou, Q.; Feng, J.; Ma, H.; Liu, W.; Zheng, C. A Weakly-supervised Framework for COVID-19 Classification and Lesion Localization from Chest CT. IEEE Trans. Med. Imaging 2020, 39, 2615–2625. [Google Scholar] [CrossRef]
- Zhang, K.; Liu, X.; Shen, J.; Li, Z.; Sang, Y.; Wu, X.; Zha, Y.; Liang, W.; Wang, C.; Wang, K.; et al. Clinically Applicable AI System for Accurate Diagnosis, Quantitative Measurements, and Prognosis of COVID-19 Pneumonia Using Computed Tomography. Cell 2020, 181, 1423–1433.e11. [Google Scholar] [CrossRef]
- Chen, L.-C.; Papandreou, G.; Schroff, F.; Adam, H. Rethinking atrous convolution for semantic image segmentation. arXiv 2017, arXiv:1706.05587. [Google Scholar]
- Chaganti, S.; Grenier, P.; Balachandran, A.; Chabin, G.; Cohen, S.; Flohr, T.; Georgescu, B.; Grbic, S.; Liu, S.; Mellot, F.; et al. Automated Quantification of CT Patterns Associated with COVID-19 from Chest CT. Radiol. Artif. Intell. 2020, 2, e200048. [Google Scholar] [CrossRef] [PubMed]
- Shen, C.; Yu, N.; Cai, S.; Zhou, J.; Sheng, J.; Liu, K.; Zhou, H.; Guo, Y.; Niu, G. Quantitative computed tomography analysis for stratifying the severity of Coronavirus Disease 2019. J. Pharm. Anal. 2020, 10, 123–129. [Google Scholar] [CrossRef]
- Pu, J.; Leader, J.K.; Bandos, A.; Ke, S.; Wang, J.; Shi, J.; Du, P.; Guo, Y.; Wenzel, S.E.; Fuhrman, C.R.; et al. Automated quantification of COVID-19 severity and progression using chest CT images. Eur. Radiol. 2021, 31, 436–446. [Google Scholar] [CrossRef] [PubMed]
- Gao, K.; Su, J.; Jiang, Z.; Zeng, L.-L.; Feng, Z.; Shen, H.; Rong, P.; Xu, X.; Qin, J.; Yang, Y.; et al. Dual-branch combination network (DCN): Towards accurate diagnosis and lesion segmentation of COVID-19 using CT images. Med. Image Anal. 2021, 67, 101836. [Google Scholar] [CrossRef]
- Chen, X.; Yao, L.; Zhang, Y. Residual Attention U-Net for Automated Multi-Class Segmentation of COVID-19 Chest CT Images. arXiv 2020, arXiv:2004.05645. [Google Scholar]
- Ouyang, X.; Huo, J.; Xia, L.; Shan, F.; Liu, J.; Mo, Z.; Yan, F.; Ding, Z.; Yang, Q.; Song, B.; et al. Dual-Sampling Attention Network for Diagnosis of COVID-19 From Community Acquired Pneumonia. IEEE Trans. Med. Imaging 2020, 39, 2595–2605. [Google Scholar] [CrossRef] [PubMed]
- Jin, C.; Chen, W.; Cao, Y.; Xu, Z.; Tan, Z.; Zhang, X.; Deng, L.; Zheng, C.; Zhou, J.; Shi, H.; et al. Development and evaluation of an artificial intelligence system for COVID-19 diagnosis. Nat. Commun. 2020, 11, 5088. [Google Scholar] [CrossRef] [PubMed]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Munich, Germany, 5–9 October 2015; pp. 234–241. [Google Scholar]
- Lin, T.-Y.; Dollár, P.; Girshick, R.; He, K.; Hariharan, B.; Belongie, S. Feature pyramid networks for object detection. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 2117–2125. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 26 June–1 July 2016; pp. 770–778. [Google Scholar]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Jun, M.; Cheng, G.; Yixin, W.; Xingle, A.; Jiantao, G.; Ziqi, Y.; Minqing, Z.; Xin, L.; Xueyuan, D.; Shucheng, C.; et al. COVID-19 CT Lung and Infection Segmentation Dataset. Zenodo 2020. [Google Scholar] [CrossRef]
- COVID-19 CT segmentation dataset. Available online: http://medicalsegmentation.com/covid19/ (accessed on 12 May 2021).
- Mader, K.S. Finding and Measuring Lungs in CT Data. Available online: https://www.kaggle.com/kmader/finding-lungs-in-ct-data (accessed on 12 May 2021).
- Morozov, S.P.; Andreychenko, A.E.; Pavlov, N.A.; Vladzymyrskyy, A.V.; Ledikhova, N.V.; Gombolevskiy, V.A.; Blokhin, I.A.; Gelezhe, P.B.; Gonchar, A.V.; Chernina, V.Y. MosMedData: Chest CT Scans With COVID-19 Related Findings Dataset. arXiv 2020, arXiv:2005.06465. [Google Scholar]
- Krebbs, M. Deep Learning With Python; CreateSpace Independent Publishing Platform: Scotts Valley, CA, USA, 2018. [Google Scholar]
- Wang, J.; Bao, Y.; Wen, Y.; Lu, H.; Luo, H.; Xiang, Y.; Li, X.; Liu, C.; Qian, D. Prior-Attention Residual Learning for More Discriminative COVID-19 Screening in CT Images. IEEE Trans. Med. Imaging 2020, 39, 2572–2583. [Google Scholar] [CrossRef] [PubMed]
- Goncharov, M.; Pisov, M.; Shevtsov, A.; Shirokikh, B.; Kurmukov, A.; Blokhin, I.; Chernina, V.; Solovev, A.; Gombolevskiy, V.; Morozov, S. CT-based COVID-19 Triage: Deep Multitask Learning Improves Joint Identification and Severity Quantification. arXiv 2020, arXiv:1706.05587. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dataset | Networks | Results | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Ref. | Non-COVIDScans (Subjects) | COVID-19 Scans (Subjects) | COVID-19 Classification | Lung Segmentation | Lesion Segmentation | Identification | Lung Segmentation [DSC] | Infection Segmentation [DSC] | 3D Visualization |
| [16] | - | 300 (126) | - | - | UNet | - | - | 84.81% | |
| [31] | 498 (498) | 1420 (704) | DCN | UNet | UNet | 89.62% Sens. 98.04% Spec. | 99.11% | 83.51% | |
| [32] | - | 110 (60) | - | - | UNet | - | - | 82.00% | |
| [33] | 1092 (628) | 1094 (960) | ResNet34 + Size-balanced Sampling | VB-Net | VB-Net | 86.9% Sens 90.1% Spec | 98.00% | 92.00% | |
| [20] | 1695 (1695) | 1029 (922) | 3D Densnet121 | 3D AH-Net | _ | 85.30% Sens. 90.10% Spec. | 95.00% | _ | |
| [34] | 6814 (5941) | 4542 (3084) | ResNet152 | UNet | - | 96.36% Sens. 80.09% Spec. | 92.55% | - | |
| [23] | _ | 201 (140) | - | - | 2.5D UNet | - | - | 78.30% | ✔ |
| [24] | - | 558 (558) | - | - | COPLE-Net | - | - | 80.72% | ✔ |
| Dataset Name | Task | # of Patients | # Images Used | Lung Mask | Lesion Mask |
|---|---|---|---|---|---|
| COVID-19 CT Lung and Infection Segmentation Dataset | Lung segmentation, lesion segmentation, and COVID-19 detection | COVID-19: 20 | 3520 | ✔ | ✔ |
| COVID-19 CT segmentation dataset | Lung segmentation | COVID-19: 9 | 829 | ✔ | |
| Finding and Measuring Lungs in CT Data (Kaggle) | Lung segmentation | Not available | 267 | ✔ | |
| MosMedData * | External Validation | 1110 | 46,411 | ✔ |
| Training Parameters | Lung Segmentation Model | Infection Segmentation Model |
|---|---|---|
| Batch size | 4 | 4 |
| Learning rate | 0.001 | 0.001 |
| Number of folds | 5 | 10 |
| Learning rate drop factor | 0.2 | 0.2 |
| Max epochs | 50 | 50 |
| Epochs patience | 5 | 5 |
| Epochs stopping criteria | 10 | 10 |
| Optimizer | Adam | Adam |
| Function Loss | NLLLoss | NLLLoss |
| Task | Lung Segmentation | Lesion Segmentation |
|---|---|---|
| # of Samples | 4616 | 3520 |
| Training Samples | 2955 | 2553 |
| Augmented training samples | 11,820 | 9012 |
| Validation samples | 923 | 563 |
| Test samples | 738 | 704 |
| Network | Accuracy (%) | IoU (%) | DSC (%) |
|---|---|---|---|
| UNet | 99.70 ± 0.16 | 95.04 ± 0.63 | 96.61 ± 0.52 |
| ResNet18 UNet | 99.70 ± 0.16 | 95.01 ± 0.63 | 96.84 ± 0.5 |
| ResNet50 UNet | 99.70 ± 0.16 | 95.03 ± 0.63 | 96.8 ± 0.51 |
| ResNet152 UNet | 99.70 ± 0.16 | 94.95 ± 0.63 | 96.69 ± 0.52 |
| DenseNet 121 UNet | 99.70 ± 0.16 | 95.35 ± 0.61 | 97.11 ± 0.48 |
| DenseNet 161 UNet | 99.69 ± 0.16 | 95.10 ± 0.62 | 97.19 ± 0.48 |
| DenseNet 201 UNet | 94.88 ± 0.64 | 94.88 ± 0.64 | 97.00 ± 0.49 |
| ResNet18 FPN | 99.65 ± 0.17 | 93.6 ± 0.71 | 95.76 ± 0.58 |
| ResNet50 FPN | 99.65 ± 0.17 | 93.39 ± 0.72 | 95.52 ± 0.6 |
| ResNet152 FPN | 99.66 ± 0.17 | 93.92 ± 0.69 | 96.00 ± 0.57 |
| DenseNet 121 FPN | 99.67 ± 0.16 | 94.53 ± 0.66 | 96.55 ± 0.53 |
| DenseNet 161 FPN | 99.66 ± 0.17 | 94.05 ± 0.68 | 96.11 ± 0.56 |
| DenseNet t201 FPN | 99.67 ± 0.17 | 94.35 ± 0.67 | 96.39 ± 0.54 |
| Network | Accuracy (%) | IoU (%) | DSC (%) |
|---|---|---|---|
| UNet | 99.82 ± 0.18 | 90.2 ± 0.72 | 92.52 ± 0.6 |
| ResNet18 UNet | 99.82 ± 0.18 | 90.69 ± 0.72 | 92.97 ± 0.58 |
| ResNet50 UNet | 98.56 ± 0.18 | 89.09 ± 0.72 | 91.44 ± 0.58 |
| ResNet152 UNet | 99.8 ± 0.18 | 88.41 ± 0.72 | 90.80 ± 0.59 |
| DenseNet121 UNet | 99.81 ± 0.18 | 90.58 ± 0.7 | 92.88 ± 0.55 |
| DenseNet161 UNet | 99.82 ± 0.18 | 90.86 ± 0.71 | 93.07 ± 0.55 |
| DenseNet201 UNet | 99.82 ± 0.73 | 91.13 ± 0.73 | 93.36 ± 0.56 |
| ResNet18 FPN | 99.81 ± 0.2 | 91.45 ± 0.81 | 93.80 ± 0.67 |
| ResNet50 FPN | 99.81 ± 0.2 | 91.46 ± 0.82 | 93.82 ± 0.68 |
| ResNet152 FPN | 99.8 ± 0.19 | 90.66 ± 0.79 | 93.05 ± 0.65 |
| DenseNet121 FPN | 99.68 ± 0.19 | 89.09 ± 0.75 | 91.02 ± 0.6 |
| DenseNet161 FPN | 99.81 ± 0.19 | 91.11 ± 0.78 | 93.45 ± 0.64 |
| DenseNet201 FPN | 99.81 ± 0.19 | 91.85 ± 0.76 | 94.13 ± 0.62 |
| Network | Accuracy (%) | Precision (%) | Sensitivity (%) | F1-Score (%) | Specificity (%) |
|---|---|---|---|---|---|
| UNet | 95.23 ± 0.7 | 84.92 ± 1.18 | 99.35 ± 0.27 | 91.57 ± 0.92 | 93.77 ± 0.8 |
| ResNet18 UNet | 94.6 ± 0.75 | 84.03 ± 1.21 | 99.78 ± 0.15 | 91.32 ± 0.93 | 92.46 ± 0.87 |
| ResNet50 UNet | 95.66 ± 0.67 | 85.91 ± 1.15 | 99.69 ± 0.18 | 92.29 ± 0.88 | 94.24 ± 0.77 |
| ResNet152 UNet | 95.68 ± 0.67 | 86.06 ± 1.14 | 99.56 ± 0.22 | 92.32 ± 0.88 | 94.31 ± 0.77 |
| DenseNet121 UNet | 95.86 ± 0.66 | 86.59 ± 1.13 | 99.53 ± 0.23 | 92.61 ± 0.86 | 94.57 ± 0.75 |
| DenseNet161 UNet | 95.61 ± 0.68 | 85.9 ± 1.15 | 99.26 ± 0.28 | 92.1 ± 0.89 | 94.35 ± 0.76 |
| DenseNet201 UNet | 95.93 ± 0.65 | 86.67 ± 1.12 | 99.64 ± 0.2 | 92.7 ± 0.86 | 94.63 ± 0.74 |
| ResNet18 FPN | 95.74 ± 0.67 | 86.25 ± 1.14 | 99.4 ± 0.26 | 92.36 ± 0.88 | 94.46 ± 0.76 |
| ResNet50 FPN | 95.77 ± 0.66 | 86.29 ± 1.14 | 99.45 ± 0.24 | 92.4 ± 0.88 | 94.49 ± 0.75 |
| ResNet152 FPN | 98.44 ± 0.41 | 95.07 ± 0.72 | 99.48 ± 0.24 | 97.23 ± 0.54 | 98.04 ± 0.46 |
| DenseNet121 FPN | 97.16 ± 0.55 | 91.67 ± 0.91 | 99 ± 0.33 | 95.19 ± 0.71 | 96.43 ± 0.61 |
| DenseNet161 FPN | 97.05 ± 0.56 | 90.62 ± 0.96 | 98.91 ± 0.34 | 94.58 ± 0.75 | 96.39 ± 0.62 |
| DenseNet201 FPN | 98.96 ± 0.34 | 96.47 ± 0.61 | 99.64 ± 0.2 | 98.03 ± 0.46 | 98.72 ± 0.37 |
| Class | Infection (%) | Accuracy (%) | Precision (%) | Sensitivity (%) | F1-Score (%) | Specificity (%) |
|---|---|---|---|---|---|---|
| CT0 | Healthy | 98.92 ± 1.27 | 100 ± 0 | 95.28 ± 2.61 | 97.58 ± 1.89 | 100 ± 0 |
| CT1 | 0 < x < 25 | 96.67 ± 1.35 | 95.89 ± 1.49 | 98.83 ± 0.81 | 97.34 ± 1.21 | 93.19 ± 1.89 |
| CT2 | 25 < x < 50 | 95.23 ± 3.74 | 83.96 ± 6.43 | 71.2 ± 7.94 | 77.06 ± 7.37 | 98.27 ± 2.28 |
| CT3 | 50 < x < 75 | 97.3 ± 4.74 | 63.64 ± 14.06 | 77.78 ± 12.15 | 70 ± 13.39 | 98.12 ± 3.97 |
| CT4 | 75 < x < 100 | 100 ± 0 | 100 ± 0 | 100 ± 0 | 100 ± 0 | 100 ± 0 |
| Average | - | 97.05 ± 1 | 94.18 ± 1.38 | 94.05 ± 1.39 | 94 ± 1.4 | 95.53 ± 1.22 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qiblawey, Y.; Tahir, A.; Chowdhury, M.E.H.; Khandakar, A.; Kiranyaz, S.; Rahman, T.; Ibtehaz, N.; Mahmud, S.; Maadeed, S.A.; Musharavati, F.; et al. Detection and Severity Classification of COVID-19 in CT Images Using Deep Learning. Diagnostics 2021, 11, 893. https://doi.org/10.3390/diagnostics11050893
Qiblawey Y, Tahir A, Chowdhury MEH, Khandakar A, Kiranyaz S, Rahman T, Ibtehaz N, Mahmud S, Maadeed SA, Musharavati F, et al. Detection and Severity Classification of COVID-19 in CT Images Using Deep Learning. Diagnostics. 2021; 11(5):893. https://doi.org/10.3390/diagnostics11050893
Chicago/Turabian StyleQiblawey, Yazan, Anas Tahir, Muhammad E. H. Chowdhury, Amith Khandakar, Serkan Kiranyaz, Tawsifur Rahman, Nabil Ibtehaz, Sakib Mahmud, Somaya Al Maadeed, Farayi Musharavati, and et al. 2021. "Detection and Severity Classification of COVID-19 in CT Images Using Deep Learning" Diagnostics 11, no. 5: 893. https://doi.org/10.3390/diagnostics11050893
APA StyleQiblawey, Y., Tahir, A., Chowdhury, M. E. H., Khandakar, A., Kiranyaz, S., Rahman, T., Ibtehaz, N., Mahmud, S., Maadeed, S. A., Musharavati, F., & Ayari, M. A. (2021). Detection and Severity Classification of COVID-19 in CT Images Using Deep Learning. Diagnostics, 11(5), 893. https://doi.org/10.3390/diagnostics11050893