
Pulmonary Sarcoidosis: Diagnosis and Differential Diagnosis


Abstract
:1. Introduction
2. Epidemiology and Definition
3. Clinical Features
4. Pulmonary Function Tests
5. Imaging
5.1. Chest Radiography
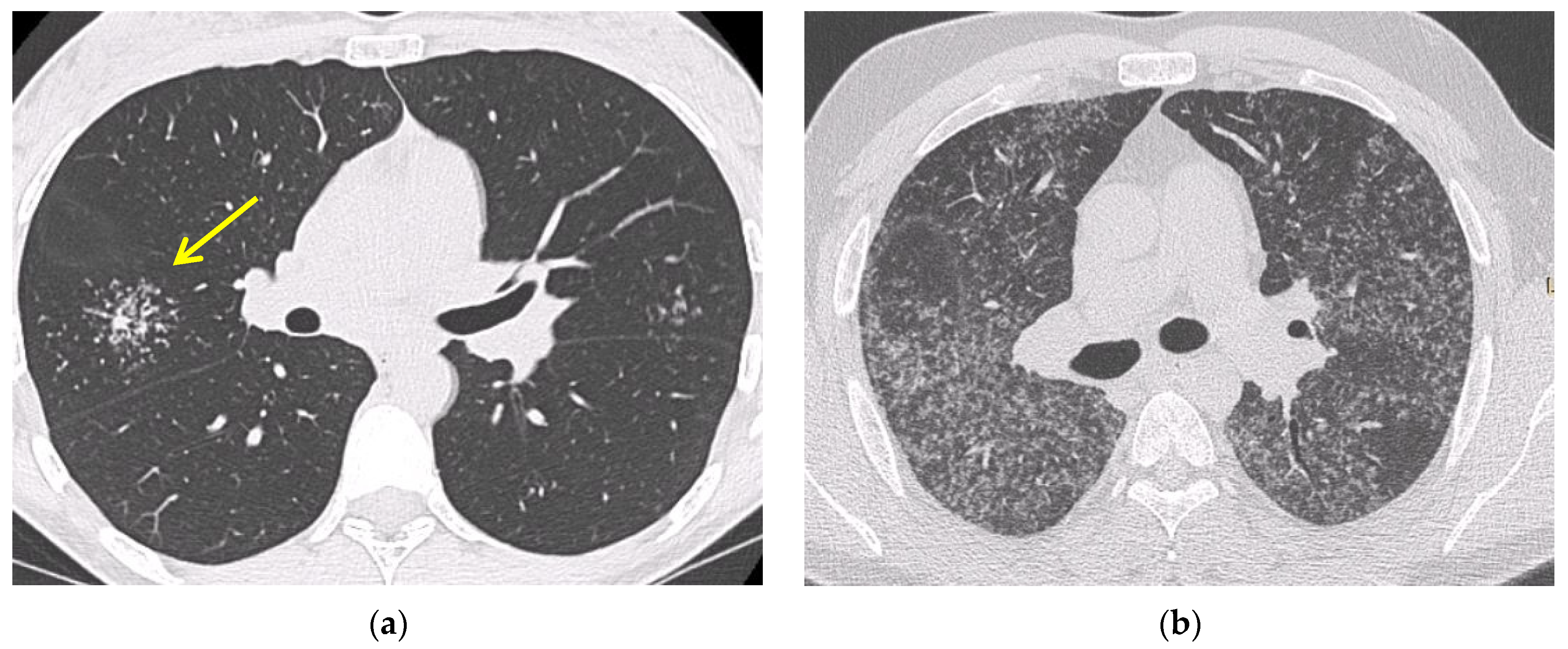
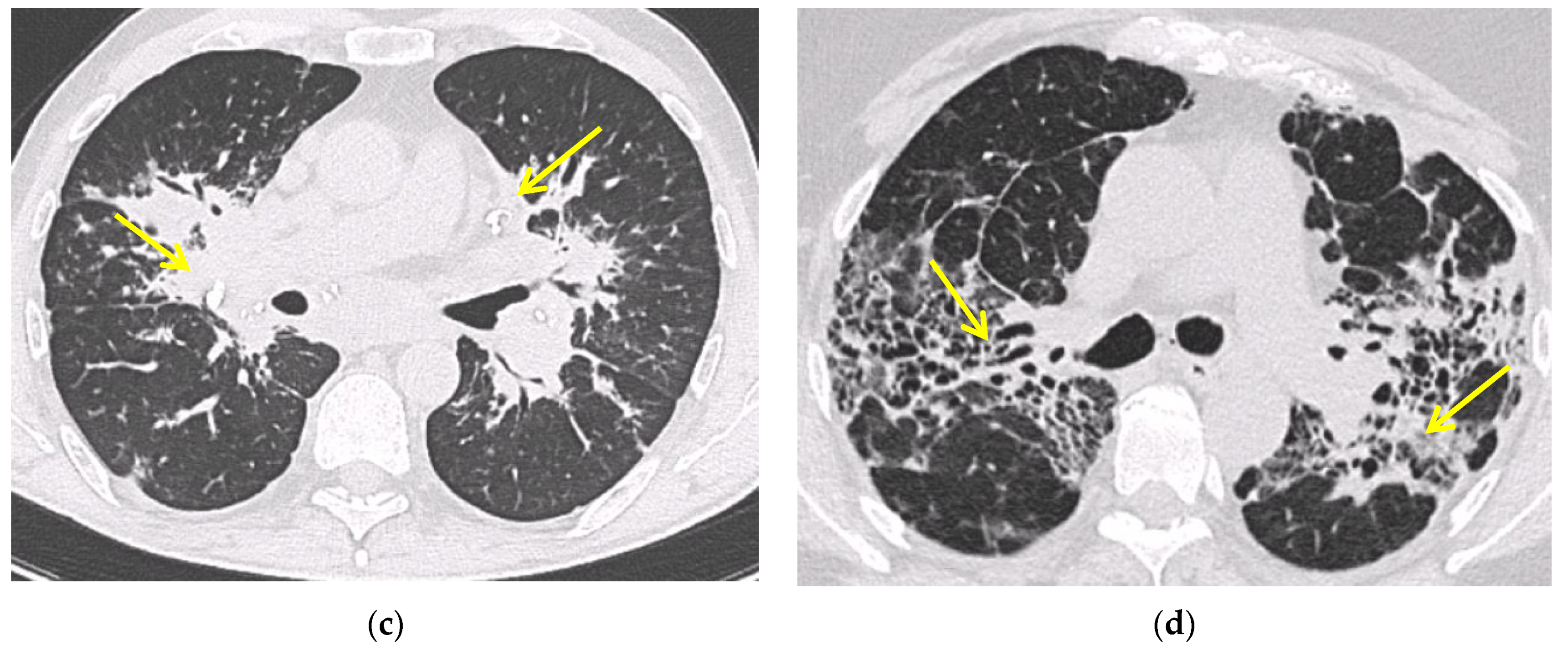
5.2. Computed Tomography (CT Scan)
5.3. Positron Emission Tomography (FDG PET/CT)
6. Confirmation of the Diagnosis
6.1. Fiberoptic Bronchoscopy
6.2. Bronchoalveolar Lavage
6.3. EBUS-TBNA
6.4. Transbronchial Lung Biopsy (TBLB)
6.5. Mediastinoscopy
6.6. Serological Biomarkers
7. Differential Diagnosis
7.1. Tuberculosis and Other Infectious Diseases
7.2. Occupational and Environmental Exposure: Chronic Beryllium Disease and Silicosis
7.3. Lymphoma, Cancer and Drug: The Sarcoid-like Reaction
7.4. Common Variable Immunodeficiency
7.5. Autoimmune Disorders
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Grunewald, J.; Spagnolo, P.; Wahlström, J.; Eklund, A. Immunogenetics of disease-causing inflammation in Sarcoidosis. Clin. Rev. Allergy Immunol. 2015, 49, 19–35. [Google Scholar] [CrossRef] [PubMed]
- American Thoracic Society. Statement on sarcoidosis. Am. J. Respir. Crit. Care Med. 1999, 160, 736–755. [Google Scholar] [CrossRef] [PubMed]
- Grunewald, J.; Grutters, J.C.; Arkema, E.V.; Saketkoo, L.A.; Moller, D.R.; Müller-Quernheim, J. Sarcoidosis. Nat. Rev. Dis. Prim. 2019, 5, 45. [Google Scholar] [CrossRef]
- Crouser, E.D.; Maier, L.A.; Wilson, K.C.; Bonham, C.A.; Morgenthau, A.S.; Patterson, K.C.; Abston, E.; Bernstein, R.C.; Blankstein, R.; Chen, E.S.; et al. Diagnosis and detection of Sarcoidosis. An official American Thoracic Society clinical practice guideline. Am. J. Respir. Crit. Care Med. 2020, 201, e26–e51. [Google Scholar] [CrossRef] [PubMed]
- Neville, E.; Walker, A.N.; James, D.G. Prognostic factors predicting the outcome of Sarcoidosis: An analysis of 818 patients. Q. J. Med. 1983, 52, 525–533. [Google Scholar]
- Gerke, A.K.; Judson, M.A.; Cozier, Y.C.; Culver, D.A.; Koth, L.L. Disease burden and variability in Sarcoidosis. Ann. Am. Thorac. Soc. 2017, 14, S421–S428. [Google Scholar] [CrossRef]
- Gerke, A.K. Morbidity and mortality in Sarcoidosis. Curr. Opin. Pulm. Med. 2014, 20, 472–478. [Google Scholar] [CrossRef] [Green Version]
- Baughman, R.P.; Barriuso, R.; Beyer, K.; Boyd, J.; Hochreiter, J.; Knoet, C.; Martone, F.; Quadder, B.; Richardson, J.; Spitzer, G.; et al. Sarcoidosis: Patient treatment priorities. ERJ Open Res. 2018, 4, 00141-2018. [Google Scholar] [CrossRef] [Green Version]
- Baughman, R.P.; Judson, M.A.; Wells, A. The indications for the treatment of Sarcoidosis: Wells law. Sarcoidosis Vasc. Diffus. Lung Dis. 2017, 34, 280–282. [Google Scholar] [CrossRef]
- Thomeer, M.J.; Costabel, U.; Rizzato, G.; Poletti, V.; Demedts, M. Comparison of registries of interstitial lung diseases in three European countries. Eur. Respir. J. 2001, 18, 114s–118s. [Google Scholar]
- Newman, L.S.; Rose, C.S.; Maier, L.A. Sarcoidosis. N. Engl. J. Med. 1997, 336, 1224–1234. [Google Scholar] [CrossRef]
- Arkema, E.V.; Cozier, Y.C. Epidemiology of Sarcoidosis: Current findings and future directions. Ther. Adv. Chronic Dis. 2018, 9, 227–240. [Google Scholar] [CrossRef]
- Jamilloux, Y.; Bonnefoy, M.; Valeyre, D.; Varron, L.; Broussolle, C.; Seve, P. Elderly-onset Sarcoidosis: Prevalence, clinical course, and treatment. Drugs Aging 2013, 30, 969–978. [Google Scholar] [CrossRef] [PubMed]
- Baughman, R.P.; Teirstein, A.S.; Judson, M.; Rossman, M.D.; Yeager, H.; Bresnitz, E.A.; DePalo, L.; Hunninghake, G.W.; Iannuzzi, M.C.; Johns, C.J.; et al. Clinical characteristics of patients in a case control study of Sarcoidosis. Am. J. Respir. Crit. Care Med. 2001, 164, 1885–1889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polverino, F.; Balestro, E.; Spagnolo, P. Clinical presentations, pathogenesis, and therapy of Sarcoidosis: State of the art. J. Clin. Med. 2020, 9, 2363. [Google Scholar] [CrossRef] [PubMed]
- Lacomis, D. Neurosarcoidosis. Curr. Neuropharmacol. 2011, 9, 429–436. [Google Scholar] [CrossRef]
- Trivieri, M.G.; Spagnolo, P.; Birnie, D.; Liu, P.; Drake, W.; Kovacic, J.C.; Baughman, R.; Fayad, Z.A.; Judson, M.A. Challenges in Cardiac and Pulmonary Sarcoidosis. J. Am. Coll. Cardiol. 2020, 76, 1878–1901. [Google Scholar] [CrossRef]
- Judson, M.A. Small fiber neuropathy in sarcoidosis: Something beneath the surface. Respir. Med. 2011, 105, 1–2. [Google Scholar] [CrossRef] [Green Version]
- Voortman, M.; Hendriks, C.M.R.; Elfferich, M.D.P.; Bonella, F.; Møller, J.; De Vries, J.; Costabel, U.; Drent, M. The Burden of Sarcoidosis symptoms from a patient perspective. Lung 2019, 197, 155–161. [Google Scholar] [CrossRef] [Green Version]
- Mañá, J.; Gómez-Vaquero, C.; Montero, A.; Salazar, A.; Marcoval, J.; Valverde, J.; Manresa, F.; Pujol, R. Löfgren’s syndrome revisited: A study of 186 patients. Am. J. Med. 1999, 107, 240–245. [Google Scholar] [CrossRef]
- Dua, A.; Manadan, A. Heerfordt’s syndrome, or uveoparotid fever. N. Engl. J. Med. 2013, 369, 458. [Google Scholar] [CrossRef] [Green Version]
- Danila, E.; Jurgauskienė, L.; Malickaite, R. BAL fluid cells and pulmonary function in different radiographic stages of newly diagnosed sarcoidosi. Adv. Med. Sci. 2008, 53, 228–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calaras, D.; Munteanu, O.; Scaletchi, V.; Simionica, I.; Botnaru, V. Ventilatory disturbances in patients with intrathoracic Sarcoidosis—A study from a functional and histological perspective. Sarcoidosis Vasc. Diffuse Lung Dis. 2017, 34, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Lynch, J.P.; Kazerooni, E.A.; Gay, S.E. Pulmonary Sarcoidosis. Clin. Chest Med. 1997, 18, 755–785. [Google Scholar] [CrossRef]
- Scadding, J.G. Prognosis of intrathoracic Sarcoidosis in England. A review of 136 cases after five years’ observation. Br. Med. J. 1961, 2, 1165–1172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, B.H.; Rosado-De-Christenson, M.L.; McAdams, H.P.; Fishback, N.F. Thoracic sarcoidosis: Radiologic-pathologic correlation. RadioGraphics 1995, 15, 421–437. [Google Scholar] [CrossRef] [Green Version]
- Judson, M.A. Sarcoidosis: Clinical presentation, diagnosis, and approach to treatment. Am. J. Med. Sci. 2008, 335, 26–33. [Google Scholar] [CrossRef]
- Spagnolo, P.; Sverzellati, N.; Wells, A.U.; Hansell, D.M. Imaging aspects of the diagnosis of sarcoidosis. Eur. Radiol. 2014, 24, 807–816. [Google Scholar] [CrossRef]
- Criado, E.; Sánchez, M.; Ramirez, J.; Arguis, P.; De Caralt, T.M.; Perea, R.J.; Xaubet, A. Pulmonary Sarcoidosis: Typical and atypical manifestations at high-resolution CT with pathologic correlation. RadioGraphics 2010, 30, 1567–1586. [Google Scholar] [CrossRef] [Green Version]
- Lynch, J.P.; Ma, Y.L.; Koss, M.N.; White, E. Pulmonary Sarcoidosis. Semin. Respir. Crit. Care Med. 2007, 28, 053–074. [Google Scholar] [CrossRef]
- Patterson, K.C.; Strek, M.E. Pulmonary Fibrosis in Sarcoidosis. Clinical features and outcomes. Ann. Am. Thorac. Soc. 2013, 10, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Abehsera, M.; Valeyre, D.; Grenier, P.; Jaillet, H.; Battesti, J.P.; Brauner, M.W. Sarcoidosis with pulmonary Fibrosis. Am. J. Roentgenol. 2000, 174, 1751–1757. [Google Scholar] [CrossRef]
- Valeyre, D.; Nunes, H.; Bernaudin, J.-F. Advanced pulmonary sarcoidosis. Curr. Opin. Pulm. Med. 2014, 20, 488–495. [Google Scholar] [CrossRef]
- Keijsers, R.G.; Grutters, J.C. In which patients with Sarcoidosis is FDG PET/CT indicated? J. Clin. Med. 2020, 9, 890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maccarone, M.T. FDG-PET scan in Sarcoidosis: Clinical and imaging indications. Curr. Med. Imaging 2018, 15, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Mostard, R.; Vöö, S.; van Kroonenburgh, M.; Verschakelen, J.; Wijnen, P.; Nelemans, P.; Erckens, R.; Drent, M. Inflammatory activity assessment by F18 FDG-PET/CT in persistent symptomatic sarcoidosis. Respir. Med. 2011, 105, 1917–1924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soussan, M.; Augier, A.; Brillet, P.-Y.; Weinmann, P.; Valeyre, D. Functional imaging in extrapulmonary Sarcoidosis. Clin. Nucl. Med. 2014, 39, e146–e159. [Google Scholar] [CrossRef]
- Trisolini, R.; Baughman, R.P.; Spagnolo, P.; Culver, D.A. Endobronchial ultrasound-guided transbronchial needle aspiration in sarcoidosis: Beyond the diagnostic yield. Respirology 2019, 24, 531–542. [Google Scholar] [CrossRef] [PubMed]
- Shorr, A.F.; Torrington, K.G.; Hnatiuk, O.W. Endobronchial biopsy for Sarcoidosis. Chest 2001, 120, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Danila, E.; Jurgauskienė, L.; Norkūnienė, J.; Malickaitė, R. BAL fluid cells in newly diagnosed pulmonary sarcoidosis with different clinical activity. Upsala J. Med. Sci. 2009, 114, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Winterbauer, R.H.; Lammert, J.; Sellami, M.; Wu, R.; Corley, D.; Springmeyer, S.C. Bronchoalveolar lavage cell populations in the diagnosis of Sarcoidosis. Chest 1993, 104, 352–361. [Google Scholar] [CrossRef] [Green Version]
- Welker, L.; Jörres, R.; Costabel, U.; Magnussen, H. Predictive value of BAL cell differentials in the diagnosis of interstitial lung diseases. Eur. Respir. J. 2004, 24, 1000–1006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heron, M.; Slieker, W.A.; Zanen, P.; Van Lochem, E.G.; Hooijkaas, H.; Bosch, J.M.V.D.; Van Velzen-Blad, H. Evaluation of CD103 as a cellular marker for the diagnosis of pulmonary sarcoidosis. Clin. Immunol. 2008, 126, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Drent, M.; Jacobs, J.A.; De Vries, J.; Lamers, R.J.S.; Liem, I.H.; Wouters, E.F.M. Does the cellular bronchoalveolar lavage fluid profile reflect the severity of sarcoidosis? Eur. Respir. J. 1999, 13, 1338–1344. [Google Scholar] [CrossRef] [PubMed]
- Chee, A.; Khalil, M.; Stather, D.R.; MacEachern, P.; Field, S.; Tremblay, A. Cytologic assessment of endobronchial ultrasound-guided transbronchial needle aspirates in Sarcoidosis. J. Bronc.-Interv. Pulmonol. 2012, 19, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Kitamura, A.; Takiguchi, Y.; Kurosu, K.; Takigawa, N.; Saegusa, F.; Hiroshima, K.; Nakajima, T.; Tanabe, N.; Nakatani, Y.; Yoshino, I.; et al. Feasibility of cytological diagnosis of sarcoidosis with endobronchial US-guided transbronchial aspiration. Sarcoidosis Vasc. Diffus. Llung Dis. Off. J. WASOG 2012, 29, 82–89. [Google Scholar]
- Yasufuku, K.; Chiyo, M.; Sekine, Y.; Chhajed, P.N.; Shibuya, K.; Iizasa, T.; Fujisawa, T. Real-time endobronchial ultrasound-guided transbronchial needle aspiration of mediastinal and hilar lymph nodes. Chest 2004, 126, 122–128. [Google Scholar] [CrossRef] [Green Version]
- Von Bartheld, M.B.; Dekkers, O.; Szlubowski, A.; Eberhardt, R.; Herth, F.; Veen, J.C.C.M.I.; De Jong, Y.P.; van der Heijden, E.; Tournoy, K.G.; Claussen, M.; et al. Endosonography vs. conventional bronchoscopy for the diagnosis of Sarcoidosis. JAMA 2013, 309, 2457–2464. [Google Scholar] [CrossRef]
- Spagnolo, P.; Rossi, G.; Trisolini, R.; Sverzellati, N.; Baughman, R.P.; Wells, A.U. Pulmonary Sarcoidosis. Lancet Respir. Med. 2018, 6, 389–402. [Google Scholar] [CrossRef]
- Dhooria, S.; Agarwal, R.; Aggarwal, A.N.; Bal, A.; Gupta, N.; Gupta, D. Differentiating tuberculosis from sarcoidosis by sonographic characteristics of lymph nodes on endobronchial ultrasonography: A study of 165 patients. J. Thorac. Cardiovasc. Surg. 2014, 148, 662–667. [Google Scholar] [CrossRef] [Green Version]
- Trisolini, R.; Tinelli, C.; Cancellieri, A.; Paioli, D.; Alifano, M.; Boaron, M.; Patelli, M. Transbronchial needle aspiration in Sarcoidosis: Yield and predictors of a positive aspirate. J. Thorac. Cardiovasc. Surg. 2008, 135, 837–842. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, R.; Aggarwal, A.N.; Gupta, D. Efficacy and safety of conventional TBNA in Sarcoidosis: A systematic review and meta-analysis. Respir. Care 2012, 58, 683–693. [Google Scholar] [CrossRef] [Green Version]
- Gupta, D.; Dadhwal, D.S.; Agarwal, R.; Gupta, N.; Bal, A.; Aggarwal, A.N. Endobronchial ultrasound-guided transbronchial needle aspiration vs conventional transbronchial needle aspiration in the diagnosis of Sarcoidosis. Chest 2014, 146, 547–556. [Google Scholar] [CrossRef]
- Navani, N.; Booth, H.L.; Kocjan, G.; Falzon, M.; Capitanio, A.; Brown, J.M.; Porter, J.C.; Janes, S.M. Combination of endobronchial ultrasound-guided transbronchial needle aspiration with standard bronchoscopic techniques for the diagnosis of stage I and stage II pulmonary sarcoidosis. Respirology 2011, 16, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Sehgal, I.S.; Bal, A.; Dhooria, S.; Gupta, N.; Ram, B.; Aggarwal, A.N.; Behera, D.; Agarwal, R. Predictors of successful yield of transbronchial lung biopsy in patients with Sarcoidosis. J. Bronc.-Interv. Pulmonol. 2018, 25, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Plit, M.; Pearson, R.; Havryk, A.; Da Costa, J.; Chang, C.; Glanville, A.R. Diagnostic utility of endobronchial ultrasound-guided transbronchial needle aspiration compared with transbronchial and endobronchial biopsy for suspected sarcoidosis. Intern. Med. J. 2012, 42, 434–438. [Google Scholar] [CrossRef] [PubMed]
- Jacob, M.; Bastos, H.N.; Mota, P.C.; Melo, N.; Cunha, R.; Pereira, J.M.; Guimarães, S.; Moura, C.S.; Morais, A. Diagnostic yield and safety of transbronchial cryobiopsy in Sarcoidosis. ERJ Open Res. 2019, 5, 00203-2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikhail, J.R.; Shepherd, M.; Mitchell, D.N. Mediastinal lymph node biopsy in Sarcoidosis. Laryngo-Rhino-Otologie 1979, 11, 5–8. [Google Scholar] [CrossRef]
- Reich, J.M.; Brouns, M.C.; O’Connor, E.A.; Edwards, M.J. Mediastinoscopy in patients with presumptive stage I Sarcoidosis. Chest 1998, 113, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Oki, M.; Saka, H.; Kitagawa, C.; Kogure, Y.; Murata, N.; Ichihara, S.; Moritani, S. Prospective study of endobronchial ultrasound–guided transbronchial needle aspiration of lymph nodes versus transbronchial lung biopsy of lung tissue for diagnosis of sarcoidosis. J. Thorac. Cardiovasc. Surg. 2012, 143, 1324–1329. [Google Scholar] [CrossRef] [Green Version]
- Costabel, U.; Bonella, F.; Ohshimo, S.; Guzman, J. Diagnostic modalities in Sarcoidosis: BAL, EBUS, and PET. Semin. Respir. Crit. Care Med. 2010, 31, 404–408. [Google Scholar] [CrossRef]
- Akyil, F.T.; Agca, M.; Ozturk, H.; Sonkaya, E.; Erdem, I.; Bulbul, E.U.; Ozbaki, F.; Yildiz, R.; Bekir, S.A.; Sevim, T. Correlation between the diagnostic yield from the bronchoalveolar lavage fluid analysis and clinicoradiological findings in Sarcoidosis. Turk. Thorac. J. 2020, 21, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Sheffield, E.A. Pathology of Sarcoidosis. Clin. Chest Med. 1997, 18, 741–754. [Google Scholar] [CrossRef]
- Kraaijvanger, R.; Janssen Bonás, M.; Vorselaars, A.D.M.; Veltkamp, M. Biomarkers in the Diagnosis and Prognosis of Sarcoidosis: Current Use and Future Prospects. Front. Immunol. 2020, 11, 1443. [Google Scholar] [CrossRef] [PubMed]
- Allen, R.K. A review of angiotensin converting enzyme in health and disease. Sarcoidosis 1991, 8, 95–100. [Google Scholar] [PubMed]
- Studdy, P.R.; Lapworth, R.; Bird, R. Angiotensin-converting enzyme and its clinical significance—A review. J. Clin. Pathol. 1983, 36, 938–947. [Google Scholar] [CrossRef] [Green Version]
- Rigat, B.; Hubert, C.; Alhenc-Gelas, F.; Cambien, F.; Corvol, P.; Soubrier, F. An insertion/deletion polymorphism in the angiotensin I-converting enzyme gene accounting for half the variance of serum enzyme levels. J. Clin. Investig. 1990, 86, 1343–1346. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, C.; Kambe, N.; Kishimoto, I.; Ueda-Hayakawa, I.; Okamoto, H. Serum soluble interleukin-2 receptor level is more sensitive than angiotensin-converting enzyme or lysozyme for diagnosis of sarcoidosis and may be a marker of multiple organ involvement. J. Dermatol. 2017, 44, 789–797. [Google Scholar] [CrossRef] [Green Version]
- Schimmelpennink, M.; Quanjel, M.; Vorselaars, A.; Wiertz, I.; Veltkamp, M.; Van Moorsel, C.; Grutters, J. Value of serum soluble interleukin-2 receptor as a diagnostic and predictive biomarker in sarcoidosis. Expert Rev. Respir. Med. 2020, 14, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Eurelings, L.E.M.; Miedema, J.R.; Dalm, V.A.S.H.; Van Daele, P.L.A.; Van Hagen, P.M.; Van Laar, J.A.M.; Dik, W.A. Sensitivity and specificity of serum soluble interleukin-2 receptor for diagnosing sarcoidosis in a population of patients suspected of sarcoidosis. PLoS ONE 2019, 14, e0223897. [Google Scholar] [CrossRef] [Green Version]
- Narula, N.; Iannuzzi, M. Sarcoidosis: Pitfalls and challenging mimickers. Front. Med. 2021, 7, 856. [Google Scholar] [CrossRef]
- Rajagopala, S.; Sankari, S.; Kancherla, R.; Ramanathan, R.P.; Balalakshmoji, D. Miliary Sarcoidosis: Does it exist? A case series and systematic review of literature. Sarcoidosis Vasc. Diffus. Lung Dis. 2020, 37, 53–65. [Google Scholar] [CrossRef]
- Wang, S.; Chung, C.; Huang, T.; Tsai, W.; Peng, C.; Huang, K.; Perng, W.; Chian, C.; Chien, W.; Shen, C. Bidirectional association between tuberculosis and sarcoidosis. Respirology 2019, 24, 467–474. [Google Scholar] [CrossRef] [Green Version]
- Muller-Quernheim, J.; Gaede, K.I.; Fireman, E.; Zissel, G. Diagnoses of chronic beryllium disease within cohorts of sarcoidosis patients. Eur. Respir. J. 2006, 27, 1190–1195. [Google Scholar] [CrossRef] [Green Version]
- Newman, L.S.; Mroz, M.M.; Balkissoon, R.; Maier, L.A. Beryllium sensitization progresses to chronic Beryllium disease. Am. J. Respir. Crit. Care Med. 2005, 171, 54–60. [Google Scholar] [CrossRef] [Green Version]
- Barna, B.P.; Culver, D.A.; Yen-Lieberman, B.; Dweik, R.A.; Thomassen, M.J. Clinical application of Beryllium lymphocyte proliferation testing. Clin. Vaccine Immunol. 2003, 10, 990–994. [Google Scholar] [CrossRef] [Green Version]
- Marchiori, E.; Ferreira, A.; Saez, F.; Gabetto, J.M.; Souza, A.S.; Escuissato, D.L.; Gasparetto, E.L. Conglomerated masses of silicosis in sandblasters: High-resolution CT findings. Eur. J. Radiol. 2006, 59, 56–59. [Google Scholar] [CrossRef]
- Rafnsson, V.; Ingimarsson, O.; Hjalmarsson, I.; Gunnarsdottir, H. Association between exposure to crystalline silica and risk of sarcoidosis. Occup. Environ. Med. 1998, 55, 657–660. [Google Scholar] [CrossRef] [Green Version]
- Vihlborg, P.; Bryngelsson, I.-L.; Andersson, L.; Graff, P. Risk of sarcoidosis and seropositive rheumatoid arthritis from occupational silica exposure in Swedish iron foundries: A retrospective cohort study. BMJ Open 2017, 7, e016839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beijer, E.; Meek, B.; Kromhout, H.; Van Es, H.W.; Seldenrijk, K.; Drent, M.; Rooijackers, J.M.; Veltkamp, M. Sarcoidosis in a patient clinically diagnosed with silicosis; is silica associated sarcoidosis a new phenotype? Respir. Med. Case Rep. 2019, 28, 100906. [Google Scholar] [CrossRef] [PubMed]
- Thillai, M.; Atkins, C.P.; Crawshaw, A.; Hart, S.P.; Ho, L.-P.; Kouranos, V.; Patterson, K.C.; Screaton, N.J.; Whight, J.; Wells, A.U. BTS clinical statement on pulmonary Sarcoidosis. Thorax 2020, 76, 4–20. [Google Scholar] [CrossRef]
- Pastré, J.; Bouvry, D.; Juvin, K.; Benattia, A.; Annesi-Maesano, I.; Valeyre, D.; Nunes, H.; Israël-Biet, D. Sarcoidosis-like cancer-associated granulomatosis: Characteristics and a case-control comparison with Sarcoidosis. J. Clin. Med. 2021, 10, 1988. [Google Scholar] [CrossRef]
- Brincker, H. Sarcoid reactions in malignant tumours. Cancer Treat. Rev. 1986, 13, 147–156. [Google Scholar] [CrossRef]
- Murthi, M.; Yoshioka, K.; Cho, J.H.; Arias, S.; Danna, E.; Zaw, M.; Holt, G.; Tatsumi, K.; Kawasaki, T.; Mirsaeidi, M. Presence of concurrent sarcoid-like granulomas indicates better survival in cancer patients: A retrospective cohort study. ERJ Open Res. 2020, 6, 00061–02020. [Google Scholar] [CrossRef] [PubMed]
- Aubart, F.C.; Lhote, R.; Amoura, A.; Valeyre, D.; Haroche, J.; Amoura, Z.; Lebrun-Vignes, B. Drug-induced sarcoidosis: An overview of the WHO pharmacovigilance database. J. Intern. Med. 2019, 288, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, A.; Sahni, S.; Vulisha, A.K.; Gumpeni, R.; Shah, R.; Talwar, A. Pulmonary manifestations of urothelial carcinoma of the bladder. Respir. Med. 2017, 128, 65–69. [Google Scholar] [CrossRef] [Green Version]
- Rubio-Rivas, M.; Moreira, C.; Marcoval, J. Sarcoidosis related to checkpoint and BRAF/MEK inhibitors in melanoma. Autoimmun. Rev. 2020, 19, 102587. [Google Scholar] [CrossRef]
- Keukeleire, S.D.; Schwarze, J.; Awada, G.; Everaert, H.; Van Binst, A.M.; Cras, L.; Neyns, B.; Aspeslagh, S. An atypical Sarcoid-like reaction during anti-protein death 1 treatment in a patient with metastatic melanoma. Melanoma Res. 2020, 30, 524–527. [Google Scholar] [CrossRef] [PubMed]
- Yousuf, H.; Mekki, R.; Khan, K.; Hussain, A. Pembrolizumab-induced Sarcoid-like reaction in a patient with lung cancer. Cureus 2020, 12, e12395. [Google Scholar] [CrossRef]
- Danlos, F.-X.; Pagès, C.; Baroudjian, B.; Vercellino, L.; Battistella, M.; Mimoun, M.; Jebali, M.; Bagot, M.; Tazi, A.; Lebbé, C. Nivolumab-induced Sarcoid-like granulomatous reaction in a patient with advanced melanoma. Chest 2016, 149, e133–e136. [Google Scholar] [CrossRef] [Green Version]
- Chopra, A.; Nautiyal, A.; Kalkanis, A.; Judson, M.A. Drug-induced Sarcoidosis-like reactions. Chest 2018, 154, 664–677. [Google Scholar] [CrossRef] [PubMed]
- Bhargava, S.; Perlman, D.; Allen, T.; Ritter, J.; Bhargava, M. Adalimumab induced pulmonary sarcoid reaction. Respir. Med. Case Rep. 2013, 10, 53–55. [Google Scholar] [CrossRef] [Green Version]
- Gîlcă, G.-E.; Diaconescu, S.; Bălan, G.G.; Timofte, O.; Ştefănescu, G. Sarcoidosis associated with infliximab therapy in ulcerative colitis: A case report. Medicine 2017, 96, e6156. [Google Scholar] [CrossRef] [PubMed]
- Ricciardi, B.F.; Nocon, A.A.; Jerabek, S.A.; Wilner, G.; Kaplowitz, E.; Goldring, S.R.; Purdue, P.E.; Perino, G. Histopathological characterization of corrosion product associated adverse local tissue reaction in hip implants: A study of 285 cases. BMC Clin. Pathol. 2016, 16, 3. [Google Scholar] [CrossRef] [Green Version]
- Ng, K.H.; Siar, C.H.; Ganesapillai, T. Sarcoid-like foreign body reaction in body piercing. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 1997, 84, 28–31. [Google Scholar] [CrossRef]
- Patuzzo, G.; Barbieri, A.; Tinazzi, E.; Veneri, D.; Argentino, G.; Moretta, F.; Puccetti, A.; Lunardi, C. Autoimmunity and infection in common variable immunodeficiency (CVID). Autoimmun. Rev. 2016, 15, 877–882. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Levinson, A.I. Granulomatous-lymphocytic interstitial lung disease (GLILD) in common variable immunodeficiency (CVID). Clin. Immunol. 2010, 134, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Korsten, P.; Tampe, B.; Konig, M.F.; Nikiphorou, E. Sarcoidosis and autoimmune diseases: Differences, similarities and overlaps. Curr. Opin. Pulm. Med. 2018, 24, 504–512. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.-H.; Chung, P.-I.; Wu, C.-Y.; Chen, Y.-T.; Chiu, Y.-W.; Chang, Y.-T.; Liu, H.-N. Comorbid autoimmune diseases in patients with sarcoidosis: A nationwide case-control study in Taiwan. J. Dermatol. 2016, 44, 423–430. [Google Scholar] [CrossRef]
- Chung, J.H.; Cox, C.W.; Montner, S.M.; Adegunsoye, A.; Oldham, J.M.; Husain, A.N.; Vij, R.; Noth, I.; Lynch, D.A.; Strek, M.E. CT features of the usual interstitial Pneumonia pattern: Differentiating connective tissue disease-associated interstitial lung disease from idiopathic pulmonary fibrosis. Am. J. Roentgenol. 2018, 210, 307–313. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Sensitivity | Specificity | Diagnostic Yield | References | |
|---|---|---|---|---|
| EBB | 46.2% | 85.7% | 30–70% | [39] |
| TBLB | 37% | 100% | 50–75% | [52,60] |
| EBUS/TBNA | 83–93% | 100% | 77–84% | [48,61] |
| Mediastinoscopy | 100% | 100% | 82–100% | [58] |
| BAL (CD4/CD8 ≥ 3.5) | 53–59% | 93–96% | 56% | [41,62] |
| Sarcoidosis | Tuberculosis | CBD and Silicosis | Sarcoid-like Reactions (SLRs) | |
|---|---|---|---|---|
| Clinical presentation | Often asymptomatic May be an occasional diagnosis Dry cough, dyspnea Weight loss Fever | Weight loss Cough Purulent sputum Hemoptysis Fever | Dry cough and dyspnea | Often Asymptomatic |
| Exposure history | Undefined | Recent travel to endemic countries, contact with TB patient | History of work/environment exposure to beryllium or silica | Drugs, malignancy or medical device implantation |
| Radiological findings or localizations | Bilateral and symmetrical hilar lymphadenopathy Perilymphatic and peribronchovascular nodules Cavitation (rare) | Hilar lymphadenopathy (often asymmetrical) Cavitation (frequent) Randomly distributed nodules | Bilateral hilar lymphadenopathy (CBD); lymph nodes may have an egg-shell appearance (silicosis) | It depends on the underlying cause (i.e., lymph nodes near solid tumors) |
| Laboratory | Hypercalcemia and hypercalciuria Elevated serum levels of ACE Elevated levels of sIL-2R Peripheral lymphopenia Mantoux test: anergic | Mantoux test: positive IGRA: positive ACE levels may be elevated | Mantoux test: negative ACE levels may be elevated | It depends on the underlying cause ACE may occasionally be elevated Mantoux test: negative |
| Histopathology | Nonnecrotizing granulomas | Necrotizing granulomas | Nonnecrotizing granulomas Sclerotic nodules Silica particles | Indistinguishable from sarcoid granulomas |
| Bronchoscopy and BALF | Lymphocytosis CD4+/CD8+ ratio generally > 3.5 | Culture positive for mycobacterium tuberculosis | Lymphocytosis Positive BeLPT (CBD) | Variable based on the underlying cause |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bernardinello, N.; Petrarulo, S.; Balestro, E.; Cocconcelli, E.; Veltkamp, M.; Spagnolo, P. Pulmonary Sarcoidosis: Diagnosis and Differential Diagnosis. Diagnostics 2021, 11, 1558. https://doi.org/10.3390/diagnostics11091558
Bernardinello N, Petrarulo S, Balestro E, Cocconcelli E, Veltkamp M, Spagnolo P. Pulmonary Sarcoidosis: Diagnosis and Differential Diagnosis. Diagnostics. 2021; 11(9):1558. https://doi.org/10.3390/diagnostics11091558
Chicago/Turabian StyleBernardinello, Nicol, Simone Petrarulo, Elisabetta Balestro, Elisabetta Cocconcelli, Marcel Veltkamp, and Paolo Spagnolo. 2021. "Pulmonary Sarcoidosis: Diagnosis and Differential Diagnosis" Diagnostics 11, no. 9: 1558. https://doi.org/10.3390/diagnostics11091558
APA StyleBernardinello, N., Petrarulo, S., Balestro, E., Cocconcelli, E., Veltkamp, M., & Spagnolo, P. (2021). Pulmonary Sarcoidosis: Diagnosis and Differential Diagnosis. Diagnostics, 11(9), 1558. https://doi.org/10.3390/diagnostics11091558