
Radiomics and Machine Learning Can Differentiate Transient Osteoporosis from Avascular Necrosis of the Hip

 ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
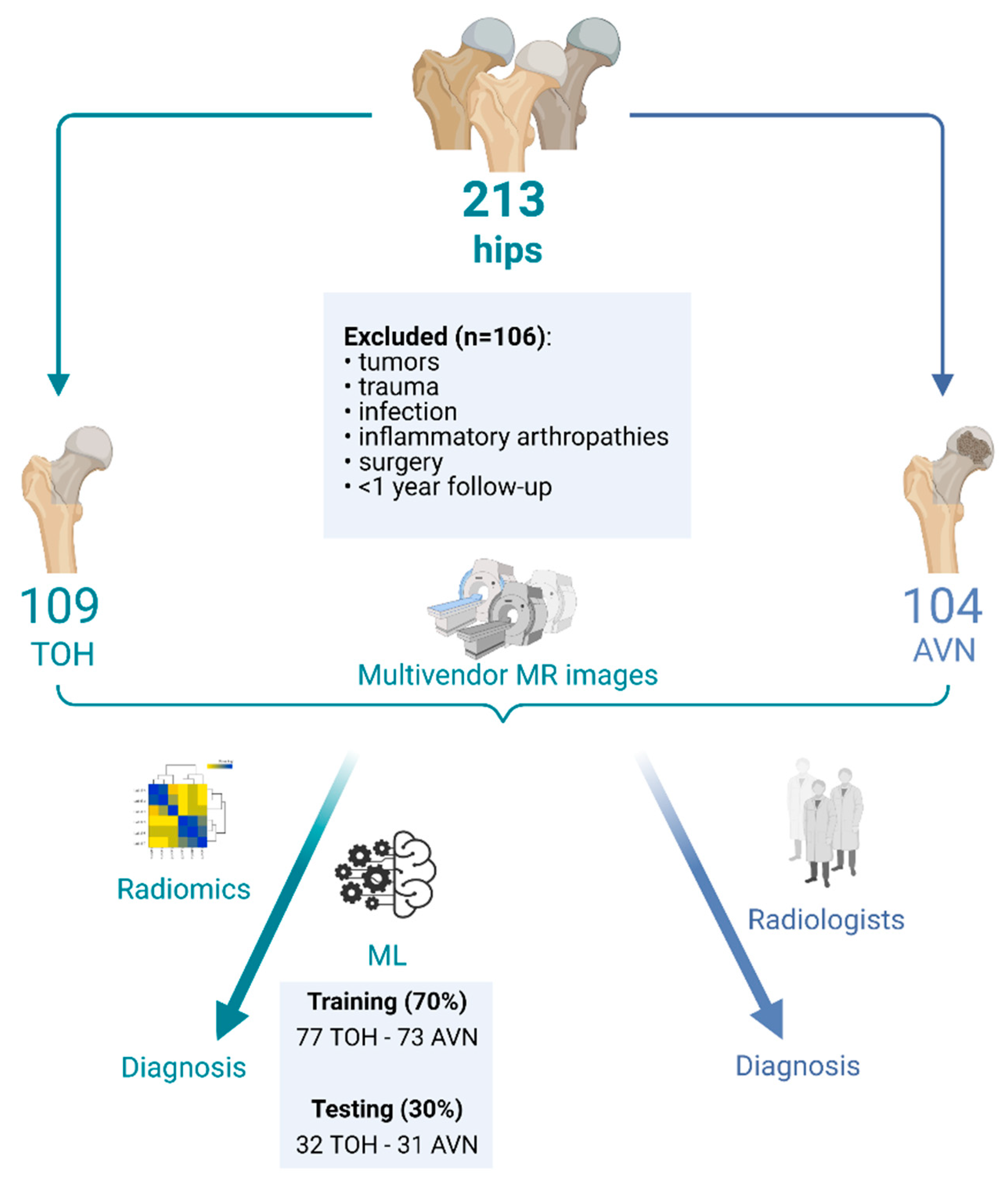
2.1. Patients
2.2. MR Imaging and Ground Truth Diagnosis
2.3. Radiomics Analysis and Machine Learning
2.4. Statistical Analysis
3. Results
3.1. Patient Demographics
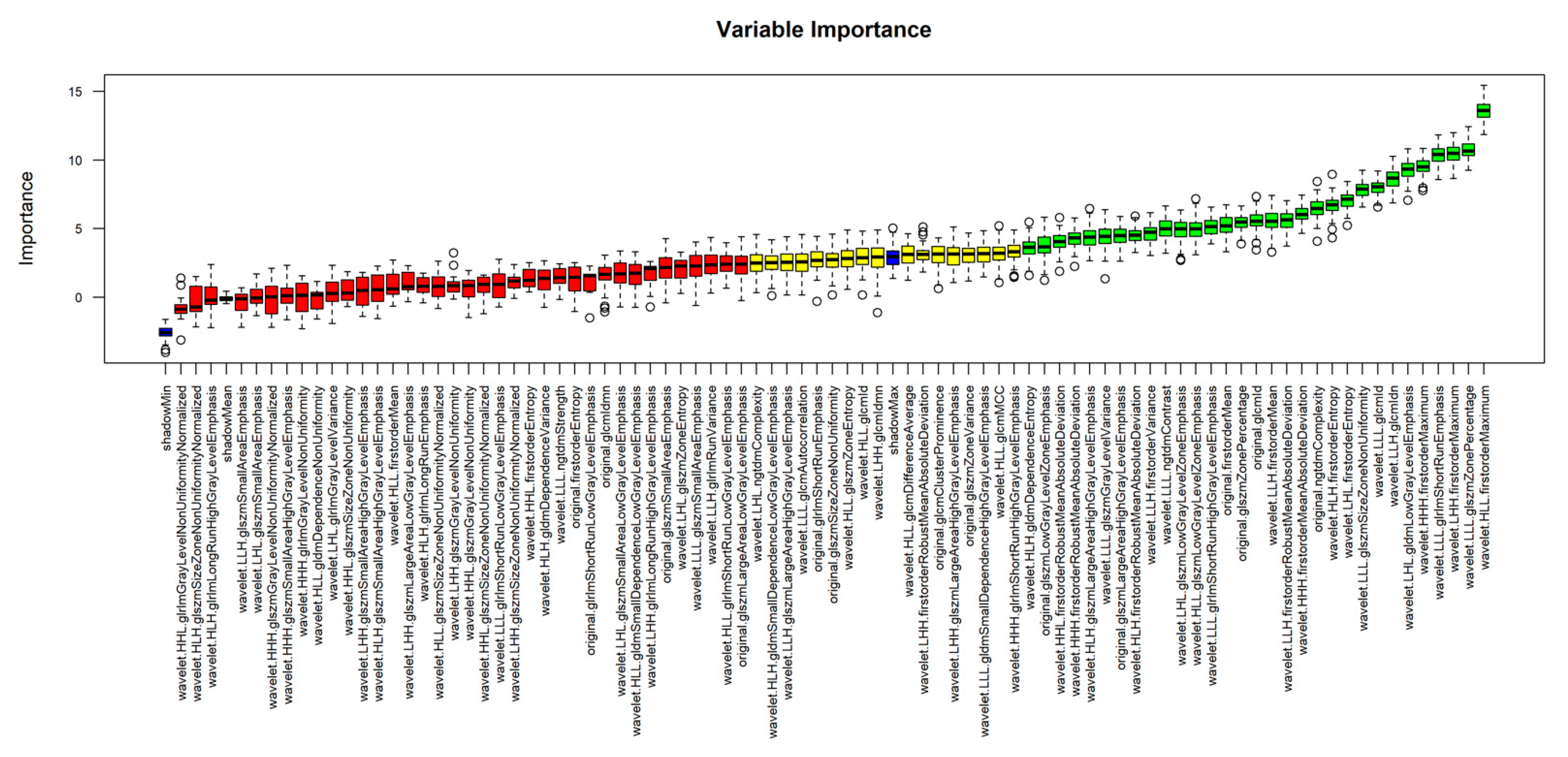
3.2. Radiomics Analysis and Machine Learning Model Development
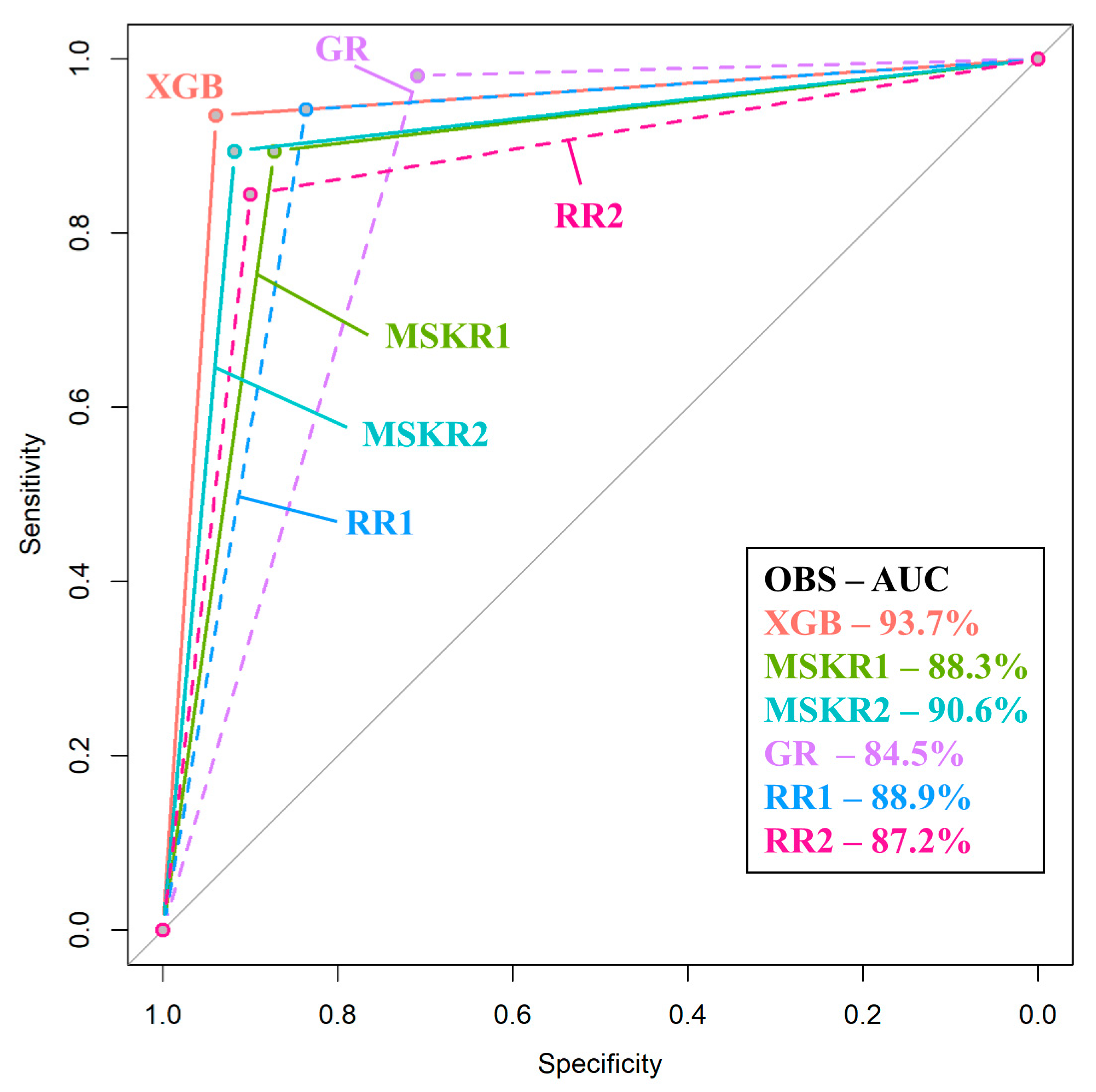
3.3. Comparison of Machine Learning to Radiologists
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Korompilias, A.V.; Karantanas, A.H.; Lykissas, M.G.; Beris, A.E. Bone marrow edema syndrome. Skelet. Radiol. 2009, 38, 425–436. [Google Scholar] [CrossRef]
- Klontzas, M.E.; Zibis, A.H.; Vassalou, E.E.; Karantanas, A.H. MRI of the Hip: Current Concepts on Bone Marrow Oedema. Hip Int. 2017, 27, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Meier, R.; Kraus, T.M.; Schaeffeler, C.; Torka, S.; Schlitter, A.M.; Specht, K.; Haller, B.; Waldt, S.; Rechl, H.; Rummeny, E.J.; et al. Bone marrow oedema on MR imaging indicates ARCO stage 3 disease in patients with AVN of the femoral head. Eur. Radiol. 2014, 24, 2271–2278. [Google Scholar] [CrossRef]
- Karantanas, A.H.; Drakonaki, E.E. The Role of MR Imaging in Avascular Necrosis of the Femoral Head. Semin. Musculoskelet. Radiol. 2011, 15, 281–300. [Google Scholar] [CrossRef] [PubMed]
- Klontzas, M.E.; Vassalou, E.E.; Zibis, A.H.; Bintoudi, A.S.; Karantanas, A.H. MR imaging of transient osteoporosis of the hip: An update on 155 hip joints. Eur. J. Radiol. 2015, 84, 431–436. [Google Scholar] [CrossRef]
- Balakrishnan, A.; Schemitsch, E.H.; Pearce, D.; McKee, M.D. Distinguishing transient osteoporosis of the hip from avascular necrosis. Can. J. Surg. 2003, 46, 187–192. [Google Scholar]
- Harvey, E.J. Osteonecrosis and transient osteoporosis of the hip: Diagnostic and treatment dilemmas. Can. J. Surg. 2003, 46, 168–169. [Google Scholar]
- Trevisan, C.; Ortolani, S.; Monteleone, M.; Marinoni, E.C. Regional Migratory Osteoporosis: A Pathogenetic Hypothesis based on Three Cases and a Review of the Literature. Clin. Rheumatol. 2002, 21, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Geith, T.; Stellwag, A.-C.; Müller, P.E.; Reiser, M.; Baur-Melnyk, A. Is bone marrow edema syndrome a precursor of hip or knee osteonecrosis? Results of 49 patients and review of the literature. Diagn. Interv. Radiol. 2020, 26, 355–362. [Google Scholar] [CrossRef]
- Yamamoto, T.; Kubo, T.; Hirasawa, Y.; Noguchi, Y.; Iwamoto, Y.; Sueishi, K. A clinicopathologic study of transient osteoporosis of the hip. Skelet. Radiol. 1999, 28, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Al-Dourobi, K.; Corbaz, J.; Bauer, S.; Leumessi, E.N. Lower lumbar back pain occurring with transient hip osteoporosis: Complication of prolonged suffering and neck of femur fracture in a 24-year-old pregnant patient. BMJ Case Rep. 2021, 14, e238477. [Google Scholar] [CrossRef]
- Hong, C.S.; Bergen, M.A.; Watters, T.S. Transient osteoporosis of the hip after bariatric surgery. Arthroplasty Today 2019, 5, 32–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mannil, M.; Von Spiczak, J.; Manka, R.; Alkadhi, H. Texture analysis and machine learning for detecting myocardial infarction in noncontrast low-dose computed tomography: Unveiling the invisible. Investig. Radiol. 2018, 53, 338–343. [Google Scholar] [CrossRef]
- van Timmeren, J.E.; Cester, D.; Tanadini-Lang, S.; Alkadhi, H.; Baessler, B. Radiomics in medical imaging—“How-to” guide and critical reflection. Insights Imaging 2020, 11, 91. [Google Scholar] [CrossRef]
- Papanikolaou, N.; Matos, C.; Koh, D.M. How to develop a meaningful radiomic signature for clinical use in oncologic patients. Cancer Imaging 2020, 20, 33. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.K.; Ha, H.I.; Park, S.-Y.; Han, J. Prediction of femoral osteoporosis using machine-learning analysis with radiomics features and abdomen-pelvic CT: A retrospective single center preliminary study. PLoS ONE 2021, 16, e0247330. [Google Scholar] [CrossRef]
- Gitto, S.; Cuocolo, R.; Albano, D.; Chianca, V.; Messina, C.; Gambino, A.; Ugga, L.; Cortese, M.C.; Lazzara, A.; Ricci, D.; et al. MRI radiomics-based machine-learning classification of bone chondrosarcoma. Eur. J. Radiol. 2020, 128, 109043. [Google Scholar] [CrossRef] [PubMed]
- Malinauskaite, I.; Hofmeister, J.; Burgermeister, S.; Neroladaki, A.; Hamard, M.; Montet, X.; Boudabbous, S. Radiomics and Machine Learning Differentiate Soft-Tissue Lipoma and Liposarcoma Better than Musculoskeletal Radiologists. Sarcoma 2020, 2020, 7163453. [Google Scholar] [CrossRef]
- Yin, P.; Mao, N.; Wang, S.; Sun, C.; Hong, N. Clinical-radiomics nomograms for pre-operative differentiation of sacral chordoma and sacral giant cell tumor based on 3D computed tomography and multiparametric magnetic resonance imaging. Br. J. Radiol. 2019, 92, 20190155. [Google Scholar] [CrossRef]
- Hong, J.H.; Jung, J.-Y.; Jo, A.; Nam, Y.; Pak, S.; Lee, S.-Y.; Park, H.; Lee, S.E.; Kim, S. Development and Validation of a Radiomics Model for Differentiating Bone Islands and Osteoblastic Bone Metastases at Abdominal CT. Radiology 2021, 299, 626–632. [Google Scholar] [CrossRef]
- Malizos, K.N.; Karantanas, A.H.; Varitimidis, S.E.; Dailiana, Z.H.; Bargiotas, K.; Maris, T. Osteonecrosis of the femoral head: Etiology, imaging and treatment. Eur. J. Radiol. 2007, 63, 16–28. [Google Scholar] [CrossRef] [PubMed]
- Degenhardt, F.; Seifert, S.; Szymczak, S. Evaluation of variable selection methods for random forests and omics data sets. Brief. Bioinform. 2019, 20, 492–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kursa, M.; Rudnicki, W. Feature Selection with the Boruta Package. J. Stat. Softw. 2010, 36, i11. [Google Scholar] [CrossRef] [Green Version]
- Morshid, A.; Elsayes, K.M.; Khalaf, A.M.; Elmohr, M.M.; Yu, J.; Kaseb, A.O.; Hassan, M.; Mahvash, A.; Wang, Z.; Hazle, J.D.; et al. A Machine Learning Model to Predict Hepatocellular Carcinoma Response to Transcatheter Arterial Chemoembolization. Radiol. Artif. Intell. 2019, 1, e180021. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Chen, Y.; Huang, Q.; Lui, S.; Huang, X.; Shi, Y.; Xu, X.; Sweeney, J.A.; Gong, Q. Psychoradiologic Utility of MR Imaging for Diagnosis of Attention Deficit Hyperactivity Disorder: A Radiomics Analysis. Radiology 2018, 287, 620–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mongan, J.; Moy, L.; Kahn, C.E. Checklist for Artificial Intelligence in Medical Imaging (CLAIM): A Guide for Authors and Reviewers. Radiol. Artif. Intell. 2020, 2, e200029. [Google Scholar] [CrossRef] [Green Version]
- Bentejac, C.; Csörgő, A.; Martínez-Muñoz, G. A comparative analysis of XGboost. arXiv 2019, arXiv:1911.01914. [Google Scholar]
- Chen, T.; Guestrin, C. XGBoost: A scalable tree boosting system. arXiv 2016, arXiv:1603.02754. [Google Scholar]
- Wang, Y.; Ni, X.S. A Xgboost Risk Model via Feature Selection and Bayesian Hyper-Parameter Optimization. Int. J. Database Manag. Syst. 2019, 11, 1–17. [Google Scholar] [CrossRef]
- Dorogush, E.V.; Ershov, V.; Gulin, A. CatBoost: Gradient boosting with categorical features support. arXiv 2018, arXiv:1810.11363. [Google Scholar]
- Shakir, H.; Rasheed, H.; Khan, T.M.R. Radiomic feature selection for lung cancer classifiers. J. Intell. Fuzzy Syst. 2020, 38, 5847–5855. [Google Scholar] [CrossRef] [Green Version]
- Hamerla, G.; Meyer, H.-J.; Schob, S.; Ginat, D.T.; Altman, A.; Lim, C.T.; Gihr, G.A.; Horvath-Rizea, D.; Hoffmann, K.-T.; Surov, A. Comparison of machine learning classifiers for differentiation of grade 1 from higher gradings in meningioma: A multicenter radiomics study. Magn. Reson. Imaging 2019, 63, 244–249. [Google Scholar] [CrossRef]
- Nazari, M.; Shiri, I.; Zaidi, H. Radiomics-based machine learning model to predict risk of death within 5-years in clear cell renal cell carcinoma patients. Comput. Biol. Med. 2021, 129, 104135. [Google Scholar] [CrossRef]
- Delong, E.R.; Delong, D.M.; Clarke-Pearson, D.L. Comparing the Areas under Two or More Correlated Receiver Operating Characteristic Curves: A Nonparametric Approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Geith, T.; Niethammer, T.; Milz, S.; Dietrich, O.; Reiser, M.; Baur-Melnyk, A. Transient Bone Marrow Edema Syndrome versus Osteonecrosis: Perfusion Patterns at Dynamic Contrast-enhanced MR Imaging with High Temporal Resolution Can Allow Differentiation. Radiology 2017, 283, 478–485. [Google Scholar] [CrossRef] [PubMed]
- Mallat, S.; Zhong, S. Characterization of signals from multiscale edges. IEEE Trans. Pattern Anal. Mach. Intell. 1992, 14, 710–732. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Ma, S.; Liu, H.; Gong, Y. An edge detection approach based on directional wavelet transform. Comput. Math. Appl. 2009, 57, 1265–1271. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | AVN Hips | TOH Hips | |
|---|---|---|---|
| Number of hips | 213 | 104 | 109 |
| Age | 44.76 ± 12.53 years | 43.74 ± 14.77 years | 45.77 ± 10.3 years |
| Side | 94R–119L | 56L–48R | 63L–46R |
| Sex * | 61F–113M | 38F–29M | 23F–84M |
| Performance Measure | XGB | CB | SVM |
|---|---|---|---|
| AUC (95% CI) | 93.74% (87.7–99.8%) | 92.1% (85.4–98.8%) | 87.4% (79.1–95.6%) |
| Sensitivity | 93.55% | 90.32% | 83.87% |
| Specificity | 93.94% | 93.94% | 90.91% |
| PPV | 93.55% | 93.33% | 89.66% |
| NPV | 93.94% | 91.18% | 85.71% |
| p-value | <0.001 | ||
| Performance Measure | XGB | MSKR1 | MSKR2 | GR | RR1 | RR2 |
|---|---|---|---|---|---|---|
| AUC (95% CI) | 93.74% (87.7–99.8%) | 90.6% (86.7–94.5%) | 88.3% (84–92.7%) | 84.5% (80–89%) | 88.9% (84.8–93.1%) | 87.2% (82.7–91.7%) |
| Sensitivity | 93.55% | 89.42% | 89.42% | 98.08% | 94.23% | 84.47% |
| Specificity | 93.94% | 91.82% | 87.27% | 70.91% | 83.64% | 90% |
| PPV | 93.55% | 91.18% | 86.92% | 76.12% | 84.48% | 88.78% |
| NPV | 93.94% | 90.18% | 89.72% | 97.50% | 93.88% | 86.09% |
| p-value * | 0.39 | 0.15 | 0.017 ** | 0.19 | 0.08 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klontzas, M.E.; Manikis, G.C.; Nikiforaki, K.; Vassalou, E.E.; Spanakis, K.; Stathis, I.; Kakkos, G.A.; Matthaiou, N.; Zibis, A.H.; Marias, K.; et al. Radiomics and Machine Learning Can Differentiate Transient Osteoporosis from Avascular Necrosis of the Hip. Diagnostics 2021, 11, 1686. https://doi.org/10.3390/diagnostics11091686
Klontzas ME, Manikis GC, Nikiforaki K, Vassalou EE, Spanakis K, Stathis I, Kakkos GA, Matthaiou N, Zibis AH, Marias K, et al. Radiomics and Machine Learning Can Differentiate Transient Osteoporosis from Avascular Necrosis of the Hip. Diagnostics. 2021; 11(9):1686. https://doi.org/10.3390/diagnostics11091686
Chicago/Turabian StyleKlontzas, Michail E., Georgios C. Manikis, Katerina Nikiforaki, Evangelia E. Vassalou, Konstantinos Spanakis, Ioannis Stathis, George A. Kakkos, Nikolas Matthaiou, Aristeidis H. Zibis, Kostas Marias, and et al. 2021. "Radiomics and Machine Learning Can Differentiate Transient Osteoporosis from Avascular Necrosis of the Hip" Diagnostics 11, no. 9: 1686. https://doi.org/10.3390/diagnostics11091686