
Comparison of Humoral and Cellular CMV Immunity in Patients Awaiting Kidney Transplantation

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. ELISpot Assay
2.3. CMV Serostatus
2.4. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Azevedo, L.S.; Pierrotti, L.C.; Abdala, E.; Costa, S.F.; Strabelli, T.M.; Campos, S.V.; Ramos, J.F.; Latif, A.Z.; Litvinov, N.; Maluf, N.Z.; et al. Cytomegalovirus infection in transplant recipients. Clinics 2015, 70, 515–523. [Google Scholar] [CrossRef]
- Martin-Gandul, C.; Mueller, N.J.; Pascual, M.; Manuel, O. The Impact of Infection on Chronic Allograft Dysfunction and Allograft Survival After Solid Organ Transplantation. Am. J. Transplant. 2015, 15, 3024–3040. [Google Scholar] [CrossRef] [Green Version]
- Marcelin, J.R.; Beam, E.; Razonable, R.R. Cytomegalovirus infection in liver transplant recipients: Updates on clinical management. World J. Gastroenterol. 2014, 20, 10658–10667. [Google Scholar] [CrossRef] [PubMed]
- Godard, B.; Gazagne, A.; Gey, A.; Baptiste, M.; Vingert, B.; Pegaz-Fiornet, B.; Strompf, L.; Fridman, W.H.; Glotz, D.; Tartour, E. Optimization of an elispot assay to detect cytomegalovirus-specific CD8+ T lymphocytes. Hum. Immunol. 2004, 65, 1307–1318. [Google Scholar] [CrossRef]
- Korcakova, L. Cytomegalovirus antibodies: Review of results of repeated examinations in 208 hemodialyzed patients. Vnitr. Lek. 1995, 41, 454–457. [Google Scholar]
- Litjens, N.H.R.; Huang, L.; Dedeoglu, B.; Meijers, R.W.J.; Kwekkeboom, J.; Betjes, M.G.H. Protective Cytomegalovirus (CMV)-Specific T-Cell Immunity Is Frequent in Kidney Transplant Patients without Serum Anti-CMV Antibodies. Front. Immunol. 2017, 8, 1137. [Google Scholar] [CrossRef] [Green Version]
- Sester, M.; Leboeuf, C.; Schmidt, T.; Hirsch, H.H. The “ABC” of Virus-Specific T Cell Immunity in Solid Organ Transplantation. Am. J. Transplant. 2016, 16, 1697–1706. [Google Scholar] [CrossRef]
- Lindemann, M.; Witzke, O.; Lütkes, P.; Fiedler, M.; Kreuzfelder, E.; Philipp, T.; Roggendorf, M.; Grosse-Wilde, H. ELISpot assay as a sensitive tool to detect cellular immunity following influenza vaccination in kidney transplant recipients. Clin. Immunol. 2006, 120, 342–348. [Google Scholar] [CrossRef]
- Czerkinsky, C.; Andersson, G.; Ekre, H.P.; Nilsson, L.A.; Klareskog, L.; Ouchterlony, O. Reverse ELISPOT assay for clonal analysis of cytokine production. I. Enumeration of gamma-interferon-secreting cells. J. Immunol. Methods 1988, 110, 29–36. [Google Scholar] [CrossRef]
- Gliga, S.; Korth, J.; Krawczyk, A.; Wilde, B.; Horn, P.A.; Witzke, O.; Lindemann, M.; Fiedler, M. T-Track-CMV and QuantiFERON-CMV assays for prediction of protection from CMV reactivation in kidney transplant recipients. J. Clin. Virol. 2018, 105, 91–96. [Google Scholar] [CrossRef]
- Banas, B.; Steubl, D.; Renders, L.; Chittka, D.; Banas, M.C.; Wekerle, T.; Koch, M.; Witzke, O.; Muhlfeld, A.; Sommerer, C.; et al. Clinical validation of a novel enzyme-linked immunosorbent spot assay-based in vitro diagnostic assay to monitor cytomegalovirus-specific cell-mediated immunity in kidney transplant recipients: A multicenter, longitudinal, prospective, observational study. Transpl. Int. 2018, 31, 436–450. [Google Scholar] [CrossRef] [Green Version]
- Walker, S.; Fazou, C.; Crough, T.; Holdsworth, R.; Kiely, P.; Veale, M.; Bell, S.; Gailbraith, A.; McNeil, K.; Jones, S.; et al. Ex vivo monitoring of human cytomegalovirus-specific CD8+ T-cell responses using QuantiFERON-CMV. Transpl. Infect. Dis. 2007, 9, 165–170. [Google Scholar] [CrossRef]
- Ruan, Y.; Guo, W.; Liang, S.; Xu, Z.; Niu, T. Diagnostic performance of cytomegalovirus (CMV) immune monitoring with ELISPOT and QuantiFERON-CMV assay in kidney transplantation: A PRISMA-compliant article. Medicine 2019, 98, e15228. [Google Scholar] [CrossRef] [PubMed]
- Sester, U.; Gartner, B.C.; Wilkens, H.; Schwaab, B.; Wossner, R.; Kindermann, I.; Girndt, M.; Meyerhans, A.; Mueller-Lantzsch, N.; Schafers, H.J.; et al. Differences in CMV-specific T-cell levels and long-term susceptibility to CMV infection after kidney, heart and lung transplantation. Am. J. Transplant. 2005, 5, 1483–1489. [Google Scholar] [CrossRef] [PubMed]
- Chanouzas, D.; Small, A.; Borrows, R.; Ball, S. Assessment of the T-SPOT.CMV interferon-gamma release assay in renal transplant recipients: A single center cohort study. PLoS ONE 2018, 13, e0193968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barabas, S.; Spindler, T.; Kiener, R.; Tonar, C.; Lugner, T.; Batzilla, J.; Bendfeldt, H.; Rascle, A.; Asbach, B.; Wagner, R.; et al. An optimized IFN-gamma ELISpot assay for the sensitive and standardized monitoring of CMV protein-reactive effector cells of cell-mediated immunity. BMC Immunol. 2017, 18, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, K.H.; Lee, H.J.; Chang, C.L.; Kim, E.J.; Lim, S.; Lee, S.J.; Ryu, J.H.; Yang, K.; Choi, B.H.; Lee, T.B.; et al. CMV specific T cell immunity predicts early viremia after liver transplantation. Transpl. Immunol. 2018, 51, 62–65. [Google Scholar] [CrossRef]
- Rogers, R.; Saharia, K.; Chandorkar, A.; Weiss, Z.F.; Vieira, K.; Koo, S.; Farmakiotis, D. Clinical experience with a novel assay measuring cytomegalovirus (CMV)-specific CD4+ and CD8+ T-cell immunity by flow cytometry and intracellular cytokine staining to predict clinically significant CMV events. BMC Infect. Dis. 2020, 20, 58. [Google Scholar]
- Thompson, G.; Boan, P.; Baumwol, J.; Chakera, A.; MacQuillan, G.; Swaminathan, S.; Lavender, M.; Flexman, J.; James, I.; John, M. Analysis of the QuantiFERON-CMV assay, CMV viraemia and antiviral treatment following solid organ transplantation in Western Australia. Pathology 2018, 50, 554–561. [Google Scholar] [CrossRef]
- Kumar, D.; Mian, M.; Singer, L.; Humar, A. An Interventional Study Using Cell-Mediated Immunity to Personalize Therapy for Cytomegalovirus Infection After Transplantation. Am. J. Transplant. 2017, 17, 2468–2473. [Google Scholar] [CrossRef]
- Manuel, O.; Husain, S.; Kumar, D.; Zayas, C.; Mawhorter, S.; Levi, M.E.; Kalpoe, J.; Lisboa, L.; Ely, L.; Kaul, D.R.; et al. Assessment of cytomegalovirus-specific cell-mediated immunity for the prediction of cytomegalovirus disease in high-risk solid-organ transplant recipients: A multicenter cohort study. Clin. Infect. Dis. 2013, 56, 817–824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, D.; Chin-Hong, P.; Kayler, L.; Wojciechowski, D.; Limaye, A.P.; Osama Gaber, A.; Ball, S.; Mehta, A.K.; Cooper, M.; Blanchard, T.; et al. A prospective multicenter observational study of cell-mediated immunity as a predictor for cytomegalovirus infection in kidney transplant recipients. Am. J. Transplant. 2019, 19, 2505–2516. [Google Scholar] [CrossRef]
- Lisboa, L.F.; Kumar, D.; Wilson, L.E.; Humar, A. Clinical utility of cytomegalovirus cell-mediated immunity in transplant recipients with cytomegalovirus viremia. Transplantation 2012, 93, 195–200. [Google Scholar] [CrossRef]
- Chiereghin, A.; Potena, L.; Borgese, L.; Gibertoni, D.; Squarzoni, D.; Turello, G.; Petrisli, E.; Piccirilli, G.; Gabrielli, L.; Grigioni, F.; et al. Monitoring of Cytomegalovirus (CMV)-Specific Cell-Mediated Immunity in Heart Transplant Recipients: Clinical Utility of the QuantiFERON-CMV Assay for Management of Posttransplant CMV Infection. J. Clin. Microbiol. 2018, 56, e01040-17. [Google Scholar] [CrossRef] [Green Version]
- Banas, B.; Steubl, D.; Renders, L.; Wekerle, T.; Koch, M.; Witzke, O.; Muhlfeld, A.; Sommerer, C.; Habicht, A.; Hugo, C.; et al. Clinical Validation of T-Track (R) Cmv to Assess the Functionality of Cmv-Specific Cell-Mediated Immunity in Kidney Transplant Recipients. Transplant. Int. 2016, 29, 20. [Google Scholar]
- Gliga, S.; Fiedler, M.; Dornieden, T.; Achterfeld, A.; Paul, A.; Horn, P.A.; Herzer, K.; Lindemann, M. Comparison of Three Cellular Assays to Predict the Course of CMV Infection in Liver Transplant Recipients. Vaccines 2021, 9, 88. [Google Scholar] [CrossRef]
- Lindemann, M.; Schuett, P.; Moritz, T.; Ottinger, H.D.; Opalka, B.; Seeber, S.; Nowrousian, M.R.; Grosse-Wilde, H. Cellular in vitro immune function in multiple myeloma patients after high-dose chemotherapy and autologous peripheral stem cell transplantation. Leukemia 2005, 19, 490–492. [Google Scholar] [CrossRef] [PubMed]
- Yan, Z.; Maecker, H.T.; Brodin, P.; Nygaard, U.C.; Lyu, S.C.; Davis, M.M.; Nadeau, K.C.; Andorf, S. Aging and CMV discordance are associated with increased immune diversity between monozygotic twins. Immun. Ageing 2021, 18, 5. [Google Scholar] [CrossRef]
- Zielinski, M.; Tarasewicz, A.; Zielinska, H.; Jankowska, M.; Moszkowska, G.; Debska-Slizien, A.; Rutkowski, B.; Trzonkowski, P. CD28 positive, cytomegalovirus specific cytotoxic T lymphocytes as a novel biomarker associated with cytomegalovirus viremia in kidney allorecipients. J. Clin. Virol. 2016, 83, 17–25. [Google Scholar] [CrossRef]
- Ducloux, D.; Legendre, M.; Bamoulid, J.; Rebibou, J.M.; Saas, P.; Courivaud, C.; Crepin, T. ESRD-associated immune phenotype depends on dialysis modality and iron status: Clinical implications. Immun. Ageing 2018, 15, 16. [Google Scholar] [CrossRef]
- Betjes, M.G.; Huisman, M.; Weimar, W.; Litjens, N.H. Expansion of cytolytic CD4+CD28- T cells in end-stage renal disease. Kidney Int. 2008, 74, 760–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Group | Absolute Number or Median (Range) |
|---|---|---|
| Sex | Male | 38 |
| Female | 25 | |
| Age (years) | 54 (19–78) | |
| Renal disease | Diabetic glomerulosclerosis | 8 |
| Chronic glomerulonephritis | 16 | |
| Nephrosclerosis | 11 | |
| Polycystic kidney disease | 6 | |
| Tubulointerstitial nephritis | 4 | |
| Congenital anomalies | 1 | |
| Autoimmune disease | 4 | |
| Amyloidosis | 1 | |
| Reflux nephropathy | 1 | |
| Thrombotic microangiopathy | 0 | |
| Other/not specified | 11 | |
| Patients on dialysis | 50 | |
| Time on dialysis (months) | 19 (1–175) | |
| Peritoneal dialysis | 19 | |
| Hemodialysis | 31 | |
| Preemptive patients | 13 | |
| eGFR (mL/min/1.73 m²) | 10.8 (3.8–23) | |
| Prior kidney transplantation | 7 | |
| Prior liver transplantation | 2 | |
| Immunosuppressive drugs | CNI | 6 |
| Steroids | 9 | |
| MPA | 3 | |
| ATG | 2 | |
| Azathioprine | 2 | |
| Hydroxychloroquine | 1 |
| Covariate | Group | CMV IE-1 1 Median (Range) | CMV pp65 1 Median (Range) |
|---|---|---|---|
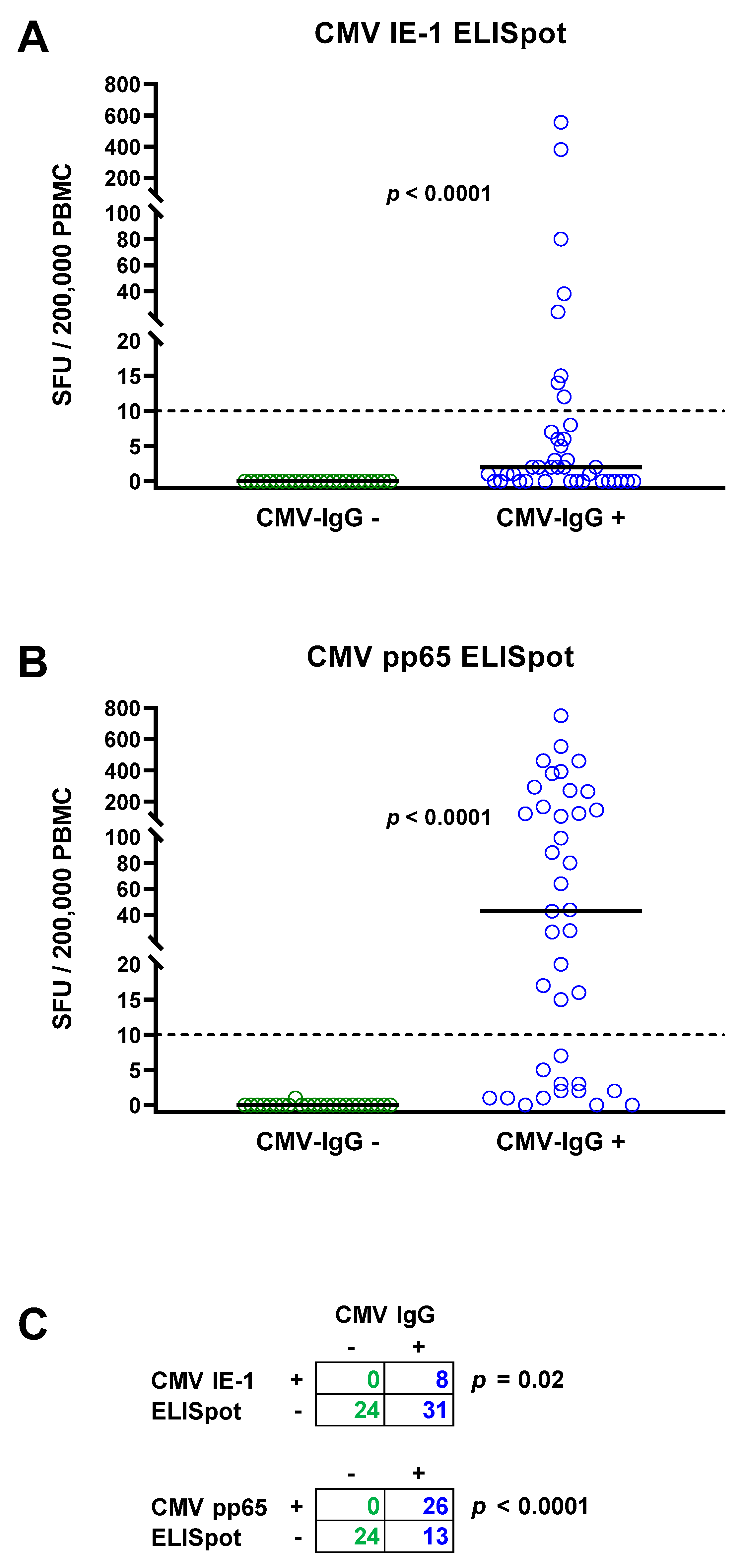
| CMV IgG | Negative (n = 24) | 0 (0–0) | 0 (0–1) |
| Positive (n = 39) | 2 (0–555) | 43 (0–750) | |
| p | <0.0001 | <0.0001 | |
| CMV IgM | Negative (n = 61) | 0 (0–555) | 2 (0–750) |
| Positive 2 (n = 2) | 2 (2–2) | 231 (1–461) | |
| p | 0.2 | 0.3 | |
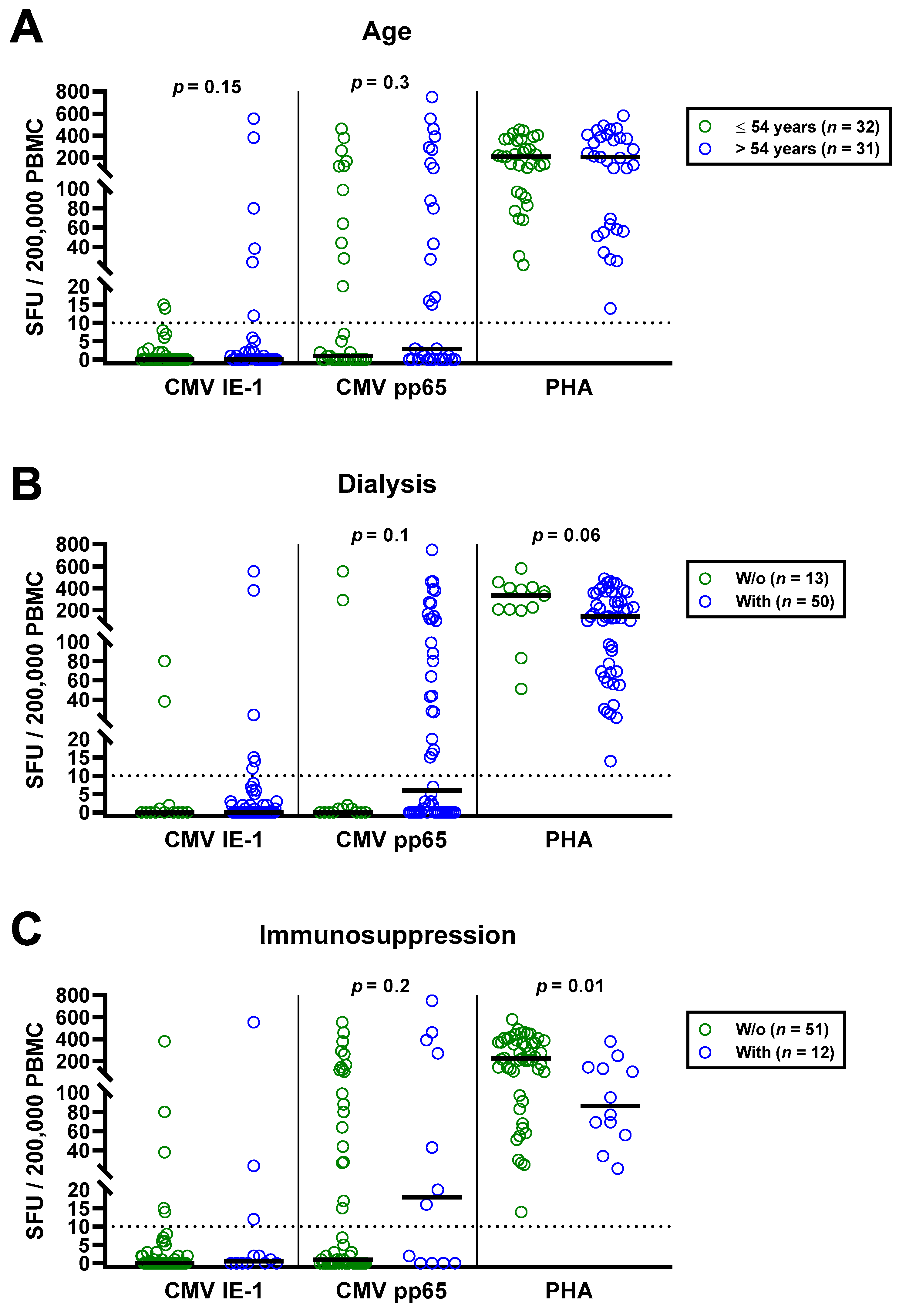
| Sex | Male (n = 38) | 0 (0–381) | 3 (0–750) |
| Female (n = 25) | 0 (0–555) | 1 (0–392) | |
| p | 0.9 | 0.6 | |
| Dialysis | No (n = 13) | 0 (0–80) | 0 (0–553) |
| Yes (n = 50) | 0 (0–555) | 6 (0–750) | |
| p | 0.5 | 0.1 | |
| Prior kidney transplantation | No (n = 7) | 0 (0–555) | 2 (0–553) |
| Yes (n = 56) | 0 (0–24) | 2 (0–750) | |
| p | 0.7 | 0.9 | |
| Immunosuppressive therapy | No (n = 51) | 0 (0–381) | 1 (0–553) |
| Yes (n = 12) | 0.5 (0–555) | 18 (0–750) | |
| p | 0.4 | 0.2 |
| No. | Sex | Age | Dialysis | Prior Tx | CNI | Steroids 1 | MPA | ATG | Others | CMV PCR | CMV IgG | CMV IE-1 | CMV pp65 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (ng/mL) | (mg) | (mg) | (IU/mL) | (SFU) | (SFU) | ||||||||
| 1 | m | 52 | HD | 1 LTx | 6.7 | - | 2000 | - | - | <65 | 1 | 2 | 461 |
| 2 | f | 56 | PD | 1 LTx | 6.7 | - | - | - | - | <65 | 1 | 1 | 16 |
| 3 | m | 46 | HD | 3 KTx | 4 | 10 | - | 01/2016 | - | n.t. | 1 | 0 | 20 |
| 4 | f | 55 | HD | 2 KTx | 4 | 2.5 | - | - | - | n.t. | 1 | 24 | 43 |
| 5 | m | 55 | HD | 2 KTx | 5 | - | 01/2007 | - | <65 | 1 | 12 | 750 | |
| 6 | f | 32 | PD | 1 KTx | 3 | 5 | 1000 | - | - | n.t. | 1 | 2 | 2 |
| 7 | m | 21 | PD | 1 KTx | 4 | 5 | 1000 | - | - | <65 | 0 | 0 | 0 |
| 8 | m | 49 | PD | 1 KTx | - | 5 | - | - | - | n.t. | 0 | 0 | 0 |
| 9 | f | 40 | HD | 1 KTx | - | 5 | - | - | - | n.t. | 0 | 0 | 0 |
| 10 | m | 61 | PD | - | - | 2.5 | - | - | 100 mg AZA | n.t. | 0 | 0 | 0 |
| 11 | f | 69 | PD | - | - | 2.5 | - | - | 100 mg AZA | n.t. | 1 | 0 | 271 |
| 12 | f | 63 | PD | - | - | - | - | - | 400 mg HCQ | n.t. | 1 | 555 | 392 |
| Covariate | Group | CMV IE-1 1 Median (Range) | CMV pp65 1 Median (Range) |
|---|---|---|---|
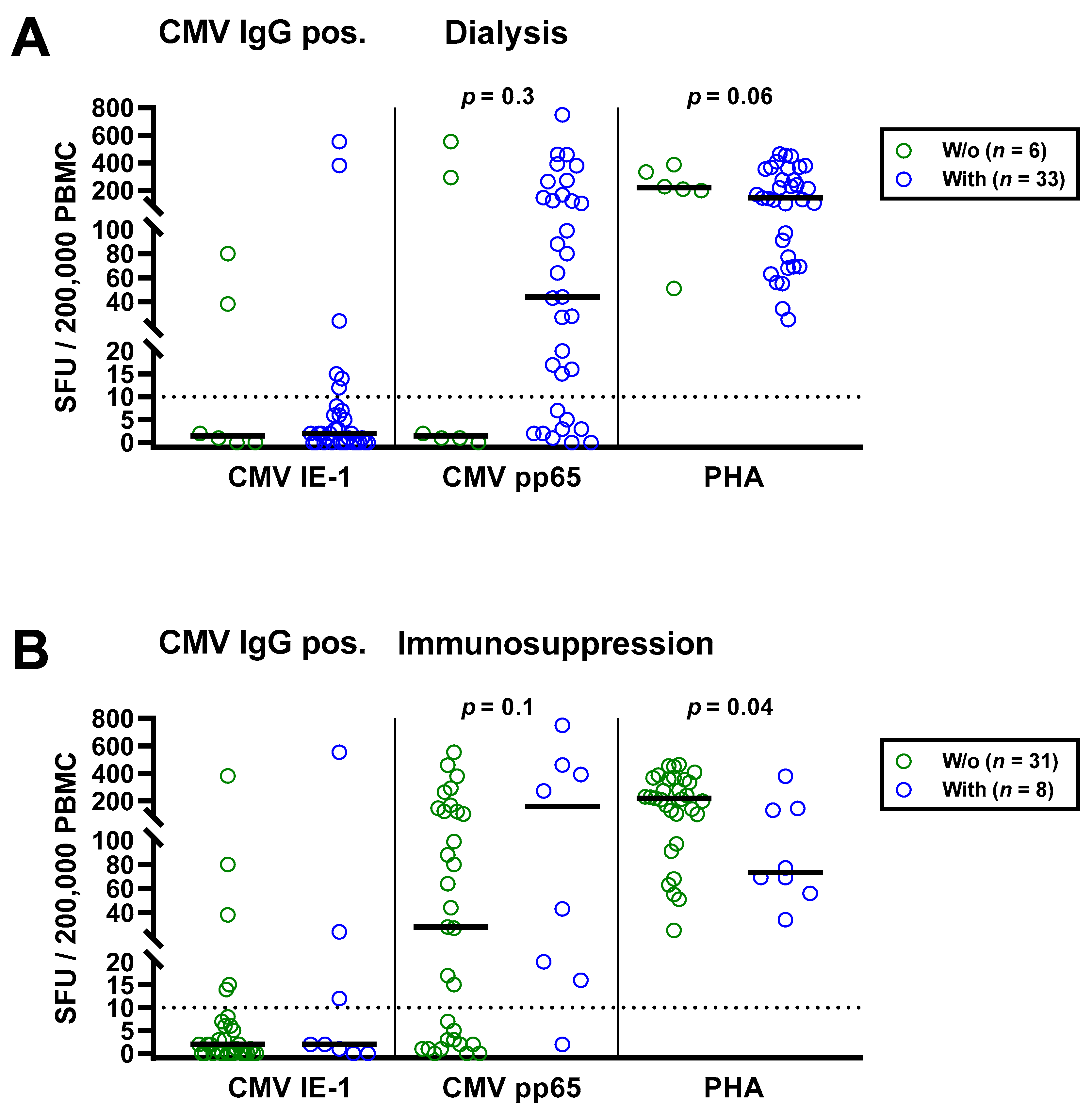
| Dialysis | No (n = 6) | 1.5 (0–80) | 1.5 (0–553) |
| Yes (n = 33) | 2 (0–555) | 44 (0–750) | |
| p | 0.8 | 0.3 | |
| Immunosuppressive therapy | No (n = 31) | 2 (0–381) | 28 (0–553) |
| Yes (n = 8) | 2 (0–555) | 157 (2–750) | |
| p | 0.5 | 0.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lindemann, M.; Wilde, B.; Friebus-Kardash, J.; Gäckler, A.; Witzke, O.; Dittmer, U.; Horn, P.A.; Kribben, A.; Mülling, N.; Eisenberger, U. Comparison of Humoral and Cellular CMV Immunity in Patients Awaiting Kidney Transplantation. Diagnostics 2021, 11, 1688. https://doi.org/10.3390/diagnostics11091688
Lindemann M, Wilde B, Friebus-Kardash J, Gäckler A, Witzke O, Dittmer U, Horn PA, Kribben A, Mülling N, Eisenberger U. Comparison of Humoral and Cellular CMV Immunity in Patients Awaiting Kidney Transplantation. Diagnostics. 2021; 11(9):1688. https://doi.org/10.3390/diagnostics11091688
Chicago/Turabian StyleLindemann, Monika, Benjamin Wilde, Justa Friebus-Kardash, Anja Gäckler, Oliver Witzke, Ulf Dittmer, Peter A. Horn, Andreas Kribben, Nils Mülling, and Ute Eisenberger. 2021. "Comparison of Humoral and Cellular CMV Immunity in Patients Awaiting Kidney Transplantation" Diagnostics 11, no. 9: 1688. https://doi.org/10.3390/diagnostics11091688