Abstract
Background. Discrepancies between histology and serology results for Helicobacter pylori detection could be caused by a variety of factors, including a biopsy sampling error, expertise of the pathologist, natural loss of infection due to advanced atrophy, or a false-positive serology in the case of a previous infection, since antibodies may be present in blood following recovery from the infection. Aims. To identify true H. pylori-positive individuals in discrepant cases by serology and histology using real time polymerase chain reaction (RT-PCR) as a gold standard. Methods. Study subjects with discrepant histology and serology results were selected from the GISTAR pilot study data base in Latvia. Subjects having received previous H. pylori eradication therapy or reporting use of proton pump inhibitors, antibacterial medications, or bismuth containing drugs one month prior to upper endoscopy were excluded. We compared the discrepant cases to the corresponding results of RT-PCR performed on gastric biopsies. Results. In total, 97 individuals with discrepant results were identified: 81 subjects were serology-positive/histology-negative, while 16 were serology-negative/histology-positive. Among the serology-positive/histology-negative cases, 64/81 (79.0%) were false-positives by serology and, for the majority, inflammation was absent in all biopsies, while, in the serology-negative/histology-positive group, only 6.2% were proven false-positives by histology. Conclusions. Among this high H. pylori prevalent, middle-aged population, the majority of discrepant cases between serology and histology were due to false positive-serology, rather than false-negative histology. This confirms the available evidence that the choice of treatment should not be based solely on the serological results, but also after excluding previous, self-reported eradication therapy.
1. Introduction
The role of serology in Helicobacter pylori detection has been debated for decades. Already, the Maastricht II recommendations have suggested to abandon the use of serology for clinical purposes and to limit its use to epidemiological studies only [1]. Nonetheless, in many countries, it is the most widely used test for H. pylori detection today. The most recent Maastricht V/Florence guidelines [2] limit the use of serology to specific cases, for example, in atrophy, considering that the bacterial load could be significantly decreased in severe gastric mucosal atrophy. This was effectively demonstrated by Kokkola et al. in a study where there were significantly decreased H. pylori antibody titers in individuals with atrophic gastritis with negative histology and 13C-urea breath test after prescribing an eradication treatment [3]. Theoretically, under these circumstances, serology might indicate the true status of infection, while histology might fail to identify the presence of the bacterium [4]. However, advanced gastric atrophy and the total disappearance of H. pylori results in a false positive serology, since antibodies can be found for a prolonged period (up to five years), making it impossible to distinguish active from past infection [5,6].
Serology is still widely recommended in Asia as one of several noninvasive methods for mass screening strategies in populations with increased risk of gastric cancer [7]. The ABC (D) method proposed by Miki [8] combines the noninvasive detection of atrophy by pepsinogen detection with H. pylori detection based on serology. Contrary to the approach in Europe, testing with the ABC method (including H. pylori serology as a part of it) has been introduced in some gastric cancer primary screening settings in Japan and could be an effective tool for gastric cancer screening [9]. It is noteworthy that panel testing for pepsinogens and H. pylori serology (with or without gastrin-17 detection) has gained significant interest and applicability also in Europe during the last decade [10]. Therefore, in fact, the real clinical practice in Europe is significantly contradicting what is recommended in the European guidelines.
The German guidelines proposed probably the most pragmatic approach, by recommending that serological assessment of H. pylori could be used, while any positive test results have to be confirmed with another, more reliable, test (such as 13C-urea breath test, stool antigen test, or invasive methods such as histology, culture, or rapid urease test) prior to the prescription of an eradication therapy [11].
Histological analysis of H. pylori has been considered as the ‘gold standard’; however, certain limitations also apply for this method, and it can give imprecise results under certain conditions as well. Theoretically, a patchy distribution of H. pylori infection, technical issues including lack of specific staining, low microscope quality, as well as the insufficient expertise of the pathologists may lead to false negative results in histological analysis. The patchy distribution of bacteria was demonstrated in a study by Pichon et al. [12], analyzing 365 gastric biopsies from the stomachs of three patients after gastrectomy and showing that H. pylori was missed in 3% (11/365) of cultured biopsies. However, most importantly, a very low bacterial density resulting from severe atrophy or proton pump inhibitor (PPI) intake may significantly alter the detection of H. pylori microscopically. Some of the previous recommendations from expert pathologists in the field recommended to also include in the report the intensity of neutrophil infiltration, characterizing an active inflammation, particularly in PPI users.
Another important issue is the false-positive results of the histological assessment of H. pylori due to misinterpretation of other urease-containing bacteria than H. pylori, as published by Osaki et al. [13]. This could be diminished by using immunohistochemistry (IHC) in addition to Giemsa staining, since immunohistochemical staining with specific H. pylori antibodies shows the highest specificity for the detection of H. pylori. [14]. However, IHC is recommended only in individuals with active gastritis without H. pylori identification by histochemistry. To summarize, there are reasons why the ‘gold standard’ may still appear to be imperfect.
Thus, despite advances in H. pylori diagnostics, drawbacks for each method still exist, and it is important to select the best method for a H. pylori search and treat strategy, as well as for the diagnosis of infection in individuals with gastric atrophy, bleeding, or other medical conditions. Since serology is often used in individuals over 50 with a higher probability of having atrophic changes, it is important to identify whether histology or serology is more accurate.
Recently, a different molecular method for H. pylori identification, real-time PCR (RT-PCR), was developed and, at present, it is considered to be highly precise [15]. Detection of H. pylori by molecular biology methods could identify the presence of bacteria in culture-negative biopsies, as demonstrated by Pichon et al. [16]. Therefore, in doubtful cases, it could be used to confirm H. pylori diagnosis.
The primary objective was to identify true positive results in doubtful cases with RT-PCR, used arbitrarily as the gold standard, and the secondary objective was to investigate the reasons for discrepancies between serology and histology results.
2. Material and Methods
2.1. Study Design
The study was conducted using data from the gastric cancer prevention study by predicting atrophic gastritis (GISTAR) pilot study (http://www.gistar.eu (accessed on 10 December 2021)). The details of the pilot study [17] and the general study design are available elsewhere [18].
A standardized and quality-controlled approach to serology and pathology according to the GISTAR protocol allowed discrepancy issues to be addressed in a reliable way by selecting cases with different H. pylori statuses according to the serology and histology results from participants having undergone upper endoscopies. Furthermore, biopsy samples were analyzed with RT-PCR to identify the true H. pylori infection status.
2.2. Participants
Asymptomatic individuals (aged 40–64 years at inclusion), who had undergone upper digestive endoscopy according to the study protocol and had discrepancies between H. pylori serology and histology results were included in the analysis.
Individuals having self-reported H. pylori eradication therapy at any time-point or who reported the use of PPI, antibacterial medications, or bismuth-containing drugs one month prior to endoscopy were excluded, as recommended by the latest Maastricht guidelines [2]. Study design in flow-chart is shown in Figure 1.
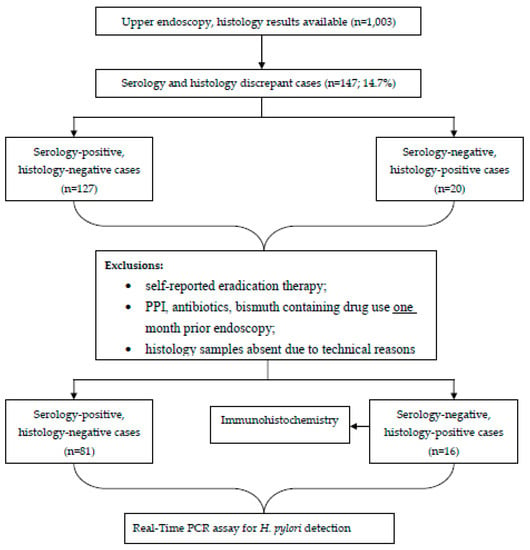
Figure 1.
Flow chart of the study design.
2.3. Serology
Blood samples were collected according to a study protocol described in detail elsewhere [17,18].
Immunoglobulin G group antibodies to H. pylori infection (Helicobacter pylori IgG ELISA, Biohit Oyj, Helsinki, Finland) were measured in plasma using an automated ELISA instrument (Personal LAB., Adaltis, Guidonia Montecelio, Italy). The cut-off value for antibody positivity was ≥30.0 EUI. The sensitivity and specificity were 93.3% and 95.7%, respectively [19].
Pepsinogen levels (PgI/II) were detected by an ELISA system, the Gastropanel® (Biohit Oyj). Based on the manufacturer’s cut-off values, a decreased pepsinogen level was considered regarding whether the PgI/PgII ratio was ≤3.0 or the PgI was ≤30 ng/mL.
2.4. Histology
Five non-targeted (random) biopsy specimens for histology were obtained according to the updated Sydney system [20], stored in 10% formalin in separate vials (marked accordingly). From the paraffin-embedded biopsies, 3 μm thick sections were prepared and stained with hematoxylin and eosin and modified Giemsa stain.
Two gastrointestinal pathologists assessed the samples independently, and a consensus was used for the current analysis. The H. pylori detection was reported as positive if any of the biopsies provided a positive result for the presence of H. pylori type bacteria.
The presence of gastric atrophy was evaluated according to the Operative Link for Gastritis Assessment (OLGA) and Operative Link on Gastric Intestinal Metaplasia Assessment (OLGIM) systems [21]. Inflammation of gastric mucosa was evaluated by the presence of neutrophils. Inflammation was noted if a moderate presence of neutrophils was shown in at least one of five biopsy samples; conversely, it was considered absent if neutrophils were few or not detected in all biopsies.
2.5. Immunohistochemistry for H. pylori
IHC was performed only for RT-PCR positive samples to rule out false negative or false positive H. pylori. For the IHC examination, H. pylori was detected using FLEX, a polyclonal rabbit anti-Helicobacter pylori kit (Dako, Glostrup, Denmark). The slides were stained with an automated immunohistochemical technique using automated Ventana, Benchmark Ultra stainer (module; 311969).
The H. pylori detection was positive if the apical staining of gastric epithelium cell membranes was present.
2.6. Patient Grouping
The study groups were characterized in respect to the presence/absence of inflammation of gastric mucosa histologically and for the presence or absence of atrophy, namely based on OLGA and OLGIM staging systems and pepsinogen detection. Patients were divided into two groups without severe gastric atrophy (i.e., OLGA stage 0, I, or II) and with atrophy (i.e., OLGA stage III, IV, or OLGIM stage III, IV).
2.7. Molecular Biology Testing for H. pylori
H. pylori deoxyribonucleic acid detection in fresh frozen antral biopsy samples obtained from the major curvature was performed using an RT-PCR in Bordeaux, France. Samples were immediately transferred to sterile 2 mL vials, which contained a specific medium (25 g/L bovine serum albumin (BSA), 74 g/L saccharose, 3.7 mM KH2PO4, 6.9 mM K2HPO4, 3.6 mM sodium glutamate and water) to protect H. pylori and then stored at −80 °C. Biopsies were shipped to France using an international courier delivery company.
H. pylori DNA was isolated by using a QIAamp DNA mini kit (Qiagen SA, Courtaboeuf, France), with glyceraldehyde-3-phosphate dehydrogenase (GAPDH) as the control.
The RT-PCR was performed according to the method developed by Oleastro et al. [22].
2.8. Statistics
Statistical analysis was carried out using Microsoft Office Excel 2007, and a statistical package for the social sciences—IBM SPSS Statistics version 22.0.
Frequency distributions were evaluated for the categorical variables (RT-PCR and IHC results, inflammation presence, decreased pepsinogen levels, and gastric atrophy stage) in each group.
2.9. Ethical Approval
The GISTAR study protocol was approved by the Ethics Committee of the International Agency for Research on Cancer (IARC; reg. No. IEC 12-36) and the Central Medical Ethics Committee of Latvia.
The current study protocol was approved by the Committee on Ethics of Riga East Clinical University Hospital Support Foundation in Medical and Biomedical Research.
The study protocol is in agreement with the ethical guidelines of the 1975 Declaration of Helsinki. All study participants were required to provide a signed consent prior to the enrolment.
3. Results and Discussion
Overall, 147 (or 14.7%) out of 1003 study participants showed discrepant results between histology and serology with respect to H. pylori status. According to exclusion criteria, 97 samples were analyzed: 81 were serology-positive/histology-negative, while 16 were serology-negative/histology-positive.
Among serology-positive/histology-negative cases, 79.0% (64/81) were false positives by serology and 21.0% (17/81) were false negatives by histology, using RT-PCR as the gold standard. In the latter group, almost all RT-PCR positive individuals had no inflammation (16/17) in gastric biopsies, while only three had signs of gastric atrophy (OLGA/OLGIM stage III or IV) (Table 1).

Table 1.
Analysis for the total patient sample in Helicobacter pylori test discrepancy cases.
At the same time, gastric atrophy was present in 16/64 of the serology-positive/histology-negative and RT-PCR-negative individuals. On the other hand, in PCR-positive cases, almost all had a positive IHC result (15/17) apart from the two samples which were excluded due to technical reasons. The majority of the decreased pepsinogen I/II ratio levels were found in the first group with PCR-negative results for 16 out of 64. In this group, only four subjects (4/64) had gastric atrophy (by the OLGA staging system) and three had intestinal metaplasia (by the OLGIM staging system).
Among serology-negative/histology-positive cases, only one (or 6.2%) was a false positive by histology, while 93.8% (15/16) were false negatives by serology.
To specify, among RT-PCR positive individuals, 9 of 15 (60%) had gastric inflammation in at least one biopsy. In addition, all serology-negative/histology-positive individuals were IHC positive.
We are reporting here a study providing conclusive evidence on the frequently discussed issue of which method, i.e., histology or serology, is more reliable for the detection of current H. pylori. The obtained results show that, in the hands of an experienced pathologist, the pathology provides more reliable results than the serology. It must be noted that the study was possible due to the large number of individuals investigated in the GISTAR cohort, from which a sufficient number of discrepant cases could be selected.
In addition, the study has provided clear evidence on what was previously understood but has been frequently forgotten more recently in clinical practice, namely that the choice of the treatment should not be based solely on serology results, even if the particular individual has denied receiving previous H. pylori eradication treatment. In our study, 6.4% (n = 64/1003) of those who were H. pylori-positive according to serology were, in fact, negative for an active H. pylori infection, although they believed they had never received eradication therapy. This could be explained either by the fact that they did not recall receiving an eradication treatment, or by a parallel H. pylori elimination which occurred while being treated with antibiotics for another disease. It would not be acceptable to treat this high proportion of individuals who have no active infection with antibiotics based on serology. This is especially true in the 21st century, when an increasing burden of disease appears related to resistant bacteria. Therefore, we suggest that, in all cases, serological screening for H. pylori be confirmed with a UBT, a fecal antigen test, or an endoscopy-based test in case of positivity. This also applies to the test use in the ABC (D) method. Furthermore, serology should not be used in clinical patient management, except in very specific exceptional cases.
In the present study, based on the RT-PCR data used as reference, we tried to detect whether false serology or false pathology was responsible for an imprecise identification of H. pylori. Among this middle-aged population with a high H. pylori prevalence, the majority of the discrepant cases between serology and histology were due to false-positive serology, rather than false-negative histology.
In total, a discrepancy between serology and histology was observed in 14.7% of cases in our study sample. In a study by Kim et al. [23], discrepant results were observed in 18% (158/872) of subjects with gastric abnormalities (a structural or color change), and, similar to our study, the majority (81/97) were serology-positive–histology-negative. The authors also concluded that gastric adenocarcinoma/adenoma and low serum pepsinogen levels were independent risk factors for a negative histology in serology-positive subjects. Interestingly, follow-up studies with Giemsa staining at different sites of the stomach revealed that 75% of the serology-positive/histology-negative subjects with adenocarcinoma were H. pylori positive, while none of those with low serum levels revealed positive findings [23]. In our study, individuals with adenocarcinoma were already excluded from prior analyses, while gastric atrophy could be one of the reasons for discrepancy between serology and histology results.
According to RT-PCR results, false positive serology was responsible for the majority (64/81) of discrepant cases. One of the explanations for serology-positive/histology-negative results could be a previously unreported infection or an infection not known by the study subjects (including H. pylori eradication as a result of antibiotic use for another purpose). Although we cannot completely rule out such cases, the interviewers were trained to ask about previous H. pylori eradication and any kind of drugs received (especially, antibiotics and PPI).
Furthermore, nonvalidated serological tests could be a cause of false positive serology. However, we used a highly accurate serological test (even the best among several tests), based on a large study by Burucoa et al. [19]. Moreover, the test was also validated in our study population [18]. However, it seems that even validated serology can encounter problems.
The majority of individuals with decreased pepsinogen levels were in the serology-positive/histology-negative group (19/21), while only two were in the serology-negative/histology-positive group. Similarly, all patients with atrophy were in the serology-positive/histology-negative group. Yet, the proportion of individuals with signs of atrophy (serological or histological) was small.
These data point to a possible loss of H. pylori due to gastric atrophy, which is also supported by a study led by Kim et al. [23]. Therefore, we can speculate that low serum pepsinogen levels might predict gastric mucosal atrophy, especially in H. pylori serology-positive cases. Accordingly, initial gastric atrophy could be one of the reasons for positive serology and negative histology in our sample.
Finally, false-positive results of histological assessment of H. pylori could also be considered, due to other urease-positive bacteria. Osaki et al. reported that several bacteria—Citrobacter freundii, Enterobacter cloacae, Klebsiella pneumoniae, Proteus mirabilis, Staphylococcus aureus [13] could be misinterpreted as H. pylori. Recently, South Korean scientists, using Giemsa stain, noted that Campylobacter hyointestinalis could also lead to false-positive H. pylori results [24]. However, in these cases, neutrophil activity is the essential and chronic inflammation is less present compared to H. pylori infection [24]. The only serology-negative/histology-positive but RT-PCR and IHC negative case could possibly be explained by the presence of Campylobacters.
Nevertheless, discrepant cases with positive histology but negative serology could be explained by an imperfect sensitivity of serology, rather than the potential presence of Helicobacters other than H. pylori, according to positive IHC analyses in the RT-PCR positive group.
Maastricht V guidelines have nevertheless considered that validated serology could be used for the search and treat strategy, since it is cheaper than UBT and not influenced by previously received treatment [2]. However, prescription of H. pylori eradication treatment based on the results of serology could lead to a high and unnecessary use of antibiotics. Therefore, based on our previous results from the pilot study, the main GISTAR study abandoned serology and switched to the use of UBT for H. pylori diagnosis [17].
In summary, our study confirms that serology should not be the first choice as a diagnostic tool for the prescription of H. pylori eradication treatment.
4. Conclusions
Among this middle-aged population with high H. pylori prevalence, the majority of discrepant cases between serology and histology were due to false-positive serology cases rather than false-negative histology cases.
Discrepant cases with positive histology but negative serology could be explained by an imperfect sensitivity of serology, more than the potential presence of Helicobacters other than H. pylori, according to positive IHC analyses in the RT-PCR positive group.
Author Contributions
Conceptualization, F.M., R.H., J.Y.P. and M.L.; methodology, F.M. and M.L.; software, S.S. (Sabine Skrebinska), I.D. and D.S.; validation, F.M., D.S. and M.L.; formal analysis, F.M., I.D., D.S., S.I., I.K., I.T., R.H., J.Y.P. and M.L.; investigation, I.L.-K., I.B., S.S. (Selga Savcenko), D.R., R.V., I.K., A.V., I.T. and C.A.; resources, M.L.; data curation, S.S. (Sabine Skrebinska), I.D., S.I., I.L.-K., I.B., S.S. (Selga Savcenko), D.R. and M.L.; writing-original draft preparation, S.S. (Sabine Skrebinska) and I.D.; writing—review and editing, all authors; visualization, S.S. (Sabine Skrebinska) , I.D. and M.L.; supervision, F.M., S.I. and M.L.; project administration, D.S.; funding acquisition, D.S. and M.L. All authors have read and agreed to the published version of the manuscript.
Funding
The work is funded by ERDF (European Regional Development Fund) within the framework of 2nd part of measure 1.1.1.1. ‘Practical Studies’, project ID Nr. 1.1.1.1/18/A/184.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. The Ethics Committee of IARC has approved the study protocol 26 March 2013 and the relevant protocol updates 2 October 2015. reg. No. IEC 12-36; the Ethics Committee of Riga East University Hospital Support foundation has approved the protocol 3 October 2013, reg. No. 14-A/13, and the Central Medical Ethics Committee in Latvia has approved the protocol 9 December 2013, reg. No. 01-29.1/11.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
The study was funded in part by the Fundamental and Applied Research Project Program in Latvia, project No. lzp-2018/1-0135 “Research on implementation of a set of measures for prevention of gastric cancer mortality by eradication H. pylori and timely recognition of precancerous lesions”. We acknowledge the entire GISTAR study team as well as the infrastructure provided by the Digestive Diseases Centre GASTRO for endoscopy and the Academic Histology Laboratory for pathology infrastructures. Our acknowledgements also to Biohit Oyj, Finland, for their support with laboratory reagents.
Conflicts of Interest
The authors declare no conflict of interest.
Disclaimer
Where authors are identified as personnel of the International Agency for Research on Cancer/World Health Organization, the authors alone are responsible for the views expressed in this article and they do not necessarily represent the decisions, policy or views of the International Agency for Research on Cancer/World Health Organization.
References
- Malfertheiner, P.; Mégraud, F.; O’Morain, C.; Hungin, A.P.S.; Jones, R.; Axon, A.; Graham, D.Y.; Tytgat, G. Current concepts in the management of Helicobacter pylori infection—The Maastricht 2-2000 Consensus Report. Aliment. Pharm. 2002, 16, 167–180. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.A.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.T.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut 2016, 66, 6–30. [Google Scholar] [CrossRef]
- Kokkola, A.; Rautelin, H.; Puolakkainen, P.; Sipponen, P.; Färkkilä, M.; Haapiainen, R.; Kosunen, T.U. Positive result by serology indicates active Helicobacter pylori infection in patients with atrophic gastritis. J. Clin. Microbiol. 1998, 36, 1808–1810. [Google Scholar] [CrossRef] [PubMed]
- Karnes, W.E., Jr.; Samloff, I.M.; Siurala, M.; Kekki, M.; Sipponen, P.; Kim, S.W.; Walsh, J.H. Positive serum antibody and negative tissue staining for Helicobacter pylori in subjects with atrophic body gastritis. Gastroenterology 1991, 101, 167–174. [Google Scholar] [CrossRef]
- Miernyk, K.M.; Bruden, D.L.; Bruce, M.G.; McMahon, B.J.; Hennessy, T.W.; Peters, H.V.; Hurlburt, D.A.; Sacco, F.; Parkinson, A.J. Dynamics of Helicobacter pylori-specific immunoglobulin G for 2 years after successful eradication of Helicobacter pylori infection in an American Indian and Alaska Native population. Clin. Vaccine Immunol. 2007, 14, 85–86. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Veijola, L.; Oksanen, A.; Linnala, A.; Sipponen, P.; Rautelin, H. Persisting chronic gastritis and elevated Helicobacter pylori antibodies after successful eradication therapy. Helicobacter 2007, 12, 605–608. [Google Scholar] [CrossRef] [PubMed]
- Liou, J.-M.; Malfertheiner, P.; Lee, Y.-C.; Sheu, B.-S.; Sugano, K.; Cheng, H.-C.; Yeoh, K.-G.; Hsu, P.-I.; Goh, K.-L.; Mahachai, V.; et al. Screening and eradication of Helicobacter pylori for gastric cancer prevention: The Taipei global consensus. Gut 2020, 69, 2093. [Google Scholar] [CrossRef] [PubMed]
- Miki, K. Gastric cancer screening by combined assay for serum anti-Helicobacter pylori IgG antibody and serum pepsinogen levels—”ABC method”. Jpn. Acad. Ser. B Phys. Biol. Sci. 2011, 87, 405–414. [Google Scholar] [CrossRef]
- Sasazuki, S. The ABC Method and Gastric Cancer: Evidence From Prospective Studies. J. Epidemiol. 2016, 26, 611–612. [Google Scholar] [CrossRef]
- Agréus, L.; Kuipers, E.J.; Kupcinskas, L.; Malfertheiner, P.; Di Mario, F.; Leja, M.; Mahachai, V.; Yaron, N.; van Oijen, M.; Perez Perez, G.; et al. Rationale in diagnosis and screening of atrophic gastritis with stomach-specific plasma biomarkers. Scand. J. Gastroenterol. 2012, 47, 136–157. [Google Scholar] [CrossRef]
- Fischbach, W.; Malfertheiner, P. Helicobacter pylori Infection. Dtsch. Arztebl. Int. 2018, 115, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Pichon, M.; Tran, C.T.; Motillon, G.; Debiais, C.; Gautier, S.; Aballea, M.; Cremniter, J.; Vasseur, P.; Tougeron, D.; Garcia, M.; et al. Where to Biopsy to Detect Helicobacter pylori and How Many Biopsies Are Needed to Detect Antibiotic Resistance in a Human Stomach. J. Clin. Med. 2020, 9, 2812. [Google Scholar] [CrossRef]
- Osaki, T.; Mabe, K.; Hanawa, T.; Kamiya, S. Urease-positive bacteria in the stomach induce a false-positive reaction in a urea breath test for diagnosis of Helicobacter pylori infection. J. Med. Microbiol. 2008, 57, 814–819. [Google Scholar] [CrossRef] [PubMed]
- Benoit, A.; Hoyeau, N.; Fléjou, J.F. Diagnosis of Helicobacter pylori infection on gastric biopsies: Standard stain, special stain or immunohistochemistry? Ann. Pathol. 2018, 38, 363–369. [Google Scholar] [CrossRef]
- Mégraud, F.; Lehours, P. Helicobacter pylori detection and antimicrobial susceptibility testing. Clin. Microbiol. Rev. 2007, 20, 280–322. [Google Scholar] [CrossRef] [PubMed]
- Pichon, M.; Pichard, B.; Barrioz, T.; Plouzeau, C.; Croquet, V.; Fotsing, G.; Chéron, A.; Vuillemin, É.; Wangermez, M.; Haineaux, P.A.; et al. Diagnostic Accuracy of a Noninvasive Test for Detection of Helicobacter pylori and Resistance to Clarithromycin in Stool by the Amplidiag H. pylori+ClariR Real-Time PCR Assay. J. Clin. Microbiol. 2020, 58, e01719–e01787. [Google Scholar] [CrossRef]
- Leja, M.; Park, J.Y.; Murillo, R.; Liepniece-Karele, I.; Isajevs, S.; Kikuste, I.; Rudzite, D.; Krike, P.; Parshutin, S.; Polaka, I.; et al. Multicentric randomised study of Helicobacter pylori eradication and pepsinogen testing for prevention of gastric cancer mortality: The GISTAR study. BMJ Open 2017, 7, e016999. [Google Scholar] [CrossRef]
- Skrebinska, S.; Daugule, I.; Santare, D.; Isajevs, S.; Liepniece-Karele, I.; Rudzite, D.; Kikuste, I.; Vanags, A.; Tolmanis, I.; Atstupens, J.; et al. Accuracy of two plasma antibody tests and faecal antigen test for non-invasive detection of H. pylori in middle-aged Caucasian general population sample. Scand. J. Gastroenterol. 2018, 53, 777–783. [Google Scholar] [CrossRef]
- Burucoa, C.; Delchier, J.C.; Courillon-Mallet, A.; de Korwin, J.D.; Megraud, F.; Zerbib, F.; Raymond, J.; Fauchere, J.L. Comparative evaluation of 29 commercial Helicobacter pylori serological kits. Helicobacter 2013, 18, 169–179. [Google Scholar] [CrossRef]
- Dixon, M.F.; Genta, R.M.; Yardley, J.H.; Correa, P. Classification and grading of gastritis. The updated Sydney System. International Workshop on the Histopathology of Gastritis, Houston 1994. Am. J. Surg. Pathol. 1996, 20, 1161–1181. [Google Scholar] [CrossRef]
- Rugge, M.; Fassan, M.; Pizzi, M.; Farinati, F.; Sturniolo, G.C.; Plebani, M.; Graham, D.Y. Operative link for gastritis assessment vs operative link on intestinal metaplasia assessment. World J. Gastroenterol. WJG 2011, 17, 4596–4601. [Google Scholar] [CrossRef] [PubMed]
- Oleastro, M.; Ménard, A.; Santos, A.; Lamouliatte, H.; Monteiro, L.; Barthélémy, P.; Mégraud, F. Real-time PCR assay for rapid and accurate detection of point mutations conferring resistance to clarithromycin in Helicobacter pylori. J. Clin. Microbiol. 2003, 41, 397–402. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Lee, S.Y.; Lee, S.P.; Kim, J.H.; Sung, I.K.; Park, H.S.; Shim, C.S.; Han, H.S. The histologic detection of Helicobacter pylori in seropositive subjects is affected by pathology and secretory ability of the stomach. Helicobacter 2018, 23, e12480. [Google Scholar] [CrossRef] [PubMed]
- Seo, T.H.; Lee, S.; Uchida, T.; Fujioka, T.; Fujioka, T.; Jin, C.J.; Hwang, T.S.; Han, H.S. The origin of non-H. pylori-related positive Giemsa staining in human gastric biopsy specimens: A prospective study. Dig. Liver Dis. 2011, 43, 23–27. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).