
Evaluation of Shoulder Microcirculation Abnormality Using Laser Doppler Flowmetry


Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
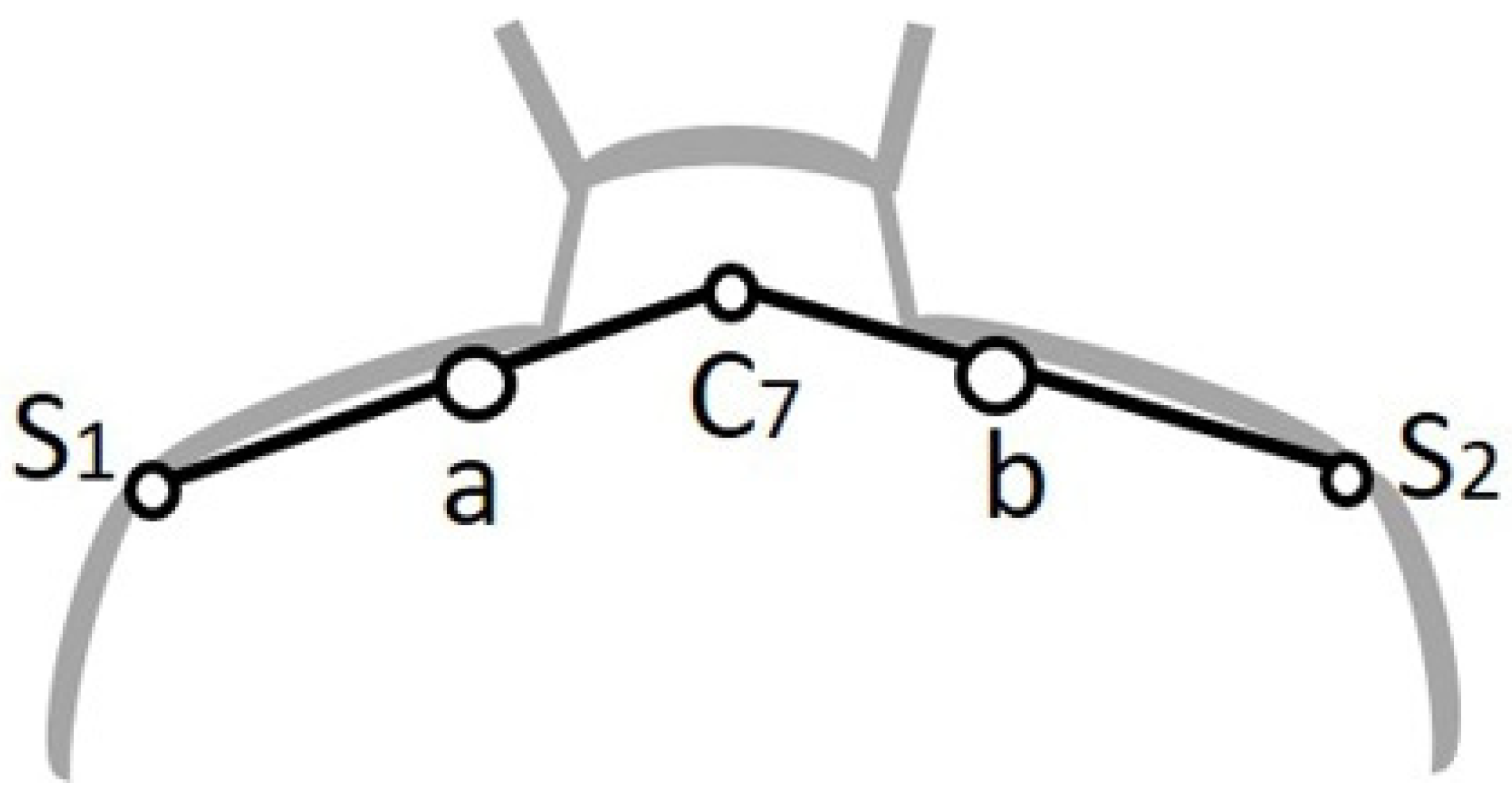
2.2. Measurements
2.3. Data Analysis
2.4. Statistical Analysis
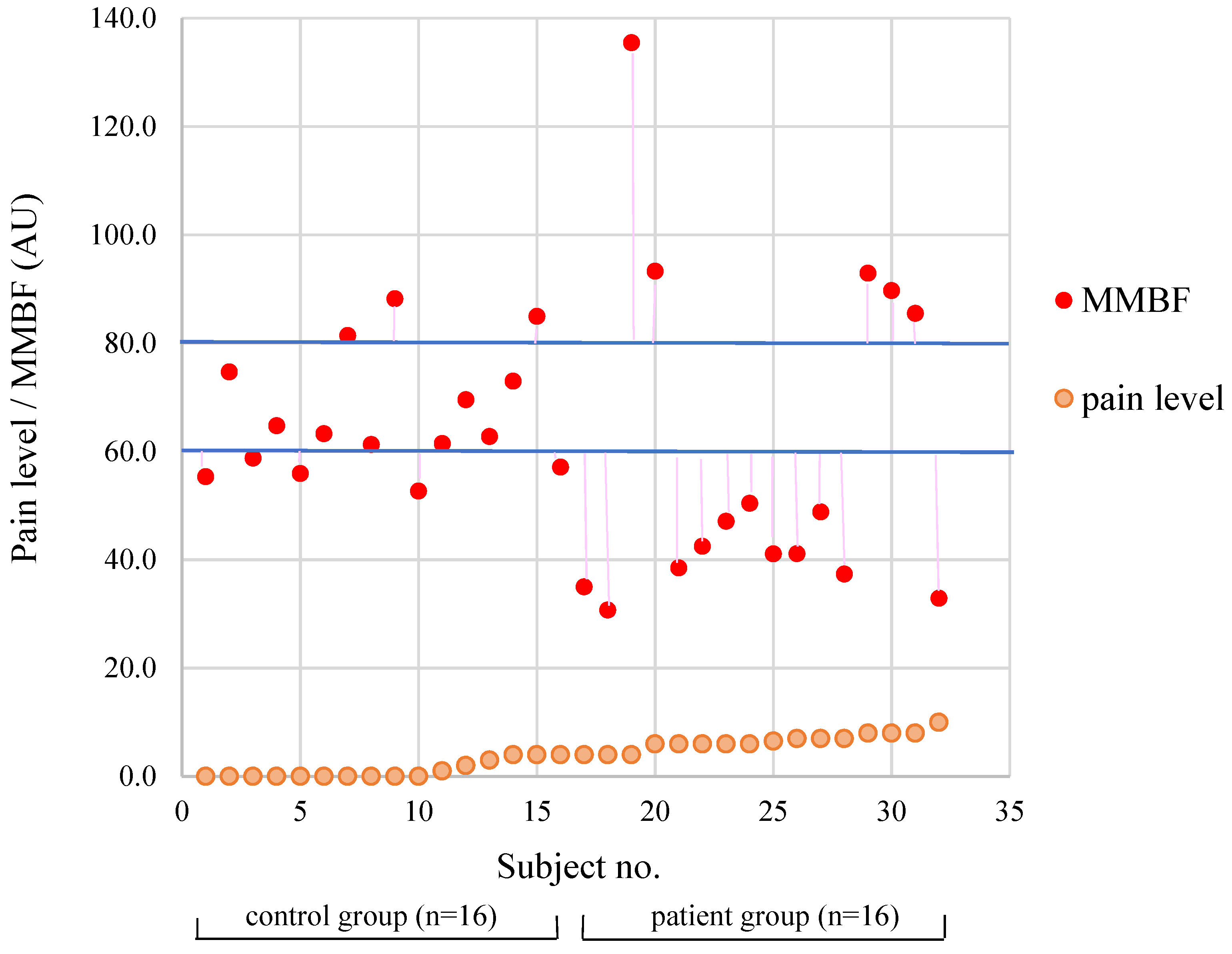
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| 3C | Computer, Communication and Consumer electronics |
| LDF | Laser Doppler Flowmetry |
| MBF | microcirculatory blood flow |
| MMBF | mean microcirculatory blood flow |
| MTrPs | myofascial trigger points |
| NSP | neck-shoulder pain |
| SPP | skin perfusion pressure |
References
- Tersa-Miralles, C.; Pastells-Peiró, R.; Rubí-Carnacea, F.; Bellon, F.; Arnaldo, E.R. Effectiveness of workplace exercise interventions in the treatment of musculoskeletal disorders in office workers: A protocol of a systematic review. BMJ Open 2020, 10, e038854. [Google Scholar] [CrossRef] [PubMed]
- Jun, D.; Zoe, M.; Johnston, V.; O’Leary, S. Physical risk factors for developing non-specific neck pain in office workers: A systematic review and meta-analysis. Int. Arch. Occup. Environ. Health 2017, 90, 373–410. [Google Scholar] [CrossRef]
- Bodin, J.; Garlantézec, R.; Costet, N.; Descatha, A.; Viel, J.F.; Roquelaure, Y. Shoulder pain among male industrial workers: Validation of a conceptual model in two independent French working populations. Appl. Ergon. 2020, 85, 103075. [Google Scholar] [CrossRef]
- Chen, R.Y.; Yu, L.H. Following the trend for a comprehensive healthy workplace in Taiwan. Global Health Promot. 2016, 23, 35–45. [Google Scholar] [CrossRef]
- Hwang, U.J.; Kwon, O.Y.; Yi, C.H.; Jeon, H.S.; Weon, J.H.; Ha, S.M. Predictors of upper trapezius pain with myofascial trigger points in food service workers: The STROBE study. Medicine 2017, 96, e7252. [Google Scholar] [CrossRef]
- Cagnie, B.; Dewitte, V.; Coppieters, I.; Oosterwijck, J.V.; Cools, A.; Danneels, L. Effect of Ischemic Compression on Trigger Points in the Neck and Shoulder Muscles in Office Workers: A Cohort Study. J. Manipul. Physiol. Therap. 2013, 36, 482–489. [Google Scholar] [CrossRef]
- Meulemeester, K.E.D.; Castelein, B.; Coppieters, I.; Barbe, T.; Cools, A.; Cagnie, B. Comparing Trigger Point Dry Needling and Manual Pressure Technique for the Management of Myofascial Neck/Shoulder Pain: A Randomized Clinical Trial. J. Manipul. Physiol. Therap. 2017, 40, 11–20. [Google Scholar] [CrossRef]
- Chia, T.; Bau, J.G.; Li, Y.H.; Wei, S.H.; Hsiu, H.; Pao, L. Microcirculatory Characteristics in Neck/Shoulder of the Adults with Sedentary and Exercise Lifestyles. J. Med. Biol. Eng. 2017, 37, 912–919. [Google Scholar] [CrossRef]
- Bau, J.G.; Chia, T.; Chung, Y.F.; Chen, K.H.; Wu, S.K. A Novel Assessment of Flexibility by Microcirculatory Signals. Sensors 2014, 14, 478–491. [Google Scholar] [CrossRef]
- Gold, J.E.; Hallman, D.M.; Hellström, F.; Björklund, M.; Crenshaw, A.G.; Mathiassen, S.E.; Barbe, M.F.; Ali, S. Systematic review of quantitative imaging biomarkers for neck and shoulder musculoskeletal disorders. BMC Musculoskelet. Disord. 2017, 18, 395. [Google Scholar] [CrossRef] [PubMed]
- Salgado, D.R.; Favory, R.; Backer, D.D. Microcirculatory assessment in daily clinical practice—Not yet ready but not too far! Einstein 2010, 8, 107–116. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Valeanu, L.; Bubenek-Turconi, S.I.; Ginghina, C.; Balan, C. Hemodynamic Monitoring in Sepsis-A Conceptual Framework of Macro- and Microcirculatory Alterations. Diagnostics 2021, 11, 1559. [Google Scholar] [CrossRef]
- Pan, X.; Chen, G.; Wu, P.; Han, C.; Ho, J.K. Skin perfusion pressure as a predictor of ischemic wound healing potential. Biomed. Rep. 2018, 8, 330–334. [Google Scholar] [CrossRef]
- Bau, J.G.; Chia, T.; Wei, S.H.; Li, Y.H.; Kuo, F.C. Correlations of Neck/Shoulder Perfusion Characteristics and Pain Symptoms of the Female Office Workers with Sedentary Lifestyle. PLoS ONE 2017, 12, e0169318. [Google Scholar] [CrossRef] [PubMed]
- Lin, F.C.; Hsiu, H.; Chiu, H.S.; Chen, C.T.; Hsu, C.H. Characteristics of pulse-waveform and laser-Doppler indices in frozen-shoulder patients. Biomed. Sign. Process. Control 2020, 56, 101718. [Google Scholar] [CrossRef]
- Jacob, M.; Chappell, D.; Becker, B.F. Regulation of blood flow and volume exchange across the microcirculation. Crit. Care 2016, 20, 319. [Google Scholar] [CrossRef]
- Simons, D.G.; Travell, J.G.; Simons, L.S. Travell & Simons’s Myofascial Pain and Dysfunction: The Trigger Point Manual, 2nd ed.; Williams & Wilkins: Baltimore, MD, USA, 1999; Volume 1. [Google Scholar]
- Hong, C.Z. Treatment of myofascial pain syndrome. Curr. Pain Headache Rep. 2006, 10, 345–349. [Google Scholar] [CrossRef]
- Bau, J.G.; Yang, C.B.; Huang, B.W.; Lin, Y.S.; Wu, W.F. Warming effect of blankets with high far-infrared emissivity on skin microcirculation in type 2 diabetic patients. Biomed. Eng. Applicat. Basis Commun. 2020, 32, 2150003. [Google Scholar] [CrossRef]
- Castronuovo, J.J.; Adera, H.M.; Smiell, J.M.; Price, R.M. Skin per fusion pressure measurement is valuable in the diagnosis of critical limb ischemia. J. Vasc. Surg. 1997, 26, 629–637. [Google Scholar] [CrossRef]
- Pitts, J. Skin Perfusion Pressure: A Case Study Demonstrating Microcirculatory Blood Flow. J. Diagn. Med. Sonogr. 2014, 30, 213–216. [Google Scholar] [CrossRef]
- Hong, C.Z. Pathophysiology of myofascial trigger point. J. Formos. Med. Assoc. 1996, 95, 93–104. [Google Scholar]
- Hong, C.Z. Muscle Pain, 1st ed.; Ho-chi: New Taipei City, Taiwan, 2015; p. 70. (In Chinese) [Google Scholar]
- Larsson, B.; Rosendal, L.; Kristiansen, J.; Sjogaard, G.; Sogaard, K.; Ghafouri, B.; Abdiu, A.; Kjaer, M.; Gerdle, B. Responses of algesic and metabolic substances to 8 h of repetitive manual work in myalgic human trapezius muscle. Pain 2008, 140, 479–490. [Google Scholar] [CrossRef]
- Takiguchi, S.; Maekawa, K.; Ono, T.; Sasai, N.; Kaji, M.; Clark, G.T.; Kuboki, T. Relationship between a chronically painful trapezius muscle and its metabolic state analyzed with PET/CT. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 110, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Shah, J.P.; Danoff, J.V.; Desai, M.J.; Parikh, S.; Nakamura, L.Y.; Phillips, T.M.; Gerber, L.H. Biochemicals associated with pain and inflammation are elevated in sites near to and remote from active myofascial trigger points. Arch. Phys. Med. Rehabil. 2008, 89, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Pober, J.S.; Sessa, W.C. Inflammation and the Blood Microvascular System. Cold Spring Harb. Perspect. Biol. 2015, 7, a016345. [Google Scholar] [CrossRef]
- Bunker, T.D.; Reilly, J.; Baird, K.S.; Hamblen, D.L. Expression of growth factors, c-ytokines and matrix metalloproteinases in frozen shoulder. J. Bone Jt. Surg. 2000, 82, 768–773. [Google Scholar] [CrossRef]
- Itoi, E.; Arce, G.; Bain, G.I.; Diercks, R.L.; Guttmann, D.; Imhoff, A.B.; Mazzocca, A.D.; Sugaya, H.; Yoo, Y.S. Shoulder Stiffness: Current Concepts and Concerns. J. Arthroscop. Relat. Surg. 2016, 32, 1402–1414. [Google Scholar] [CrossRef] [PubMed]
- Backer, D.D.; Creteur, J.; Preiser, J.C.; Dubois, M.J.; Vincent, J.L. Microvascular blood flow is altered in patients with sepsis. Am. J. Respir. Crit. Care Med. 2002, 166, 98–104. [Google Scholar] [CrossRef]
- Trzeciak, S.; Dellinger, R.P.; Parrillo, J.E.; Guglielmi, M.; Bajaj, J.; Abate, N.L. Early microcirculatory perfusion derangements in patients with severe sepsis and septic shock: Relationship to hemodynamics, oxygen transport, and survival. Ann. Emerg. Med. 2007, 49, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.Y.; Chang, S.L.; Wu, Y.E.; Hsu, T.L.; Wang, W.K. Resonance. The Missing Phenomenon in Hemodynamics. Circ. Res. 1991, 69, 246–249. [Google Scholar] [CrossRef] [PubMed]
- Hallman, D.M.; Gupta, N.; Mathiassen, S.E.; Holtermann, A. Association between objectively measured sitting time and neck–shoulder pain among blue-collar workers. Int. Arch. Occupat. Environ. Health 2015, 88, 1031–1042. [Google Scholar] [CrossRef]
- Djade, C.D.; Porgo, T.V.; Zomahoun, H.T.V.; Perrault-Sullivan, G.; Dionne, C.E. Incidence of shoulder pain in 40 years old and over and associated factors: A systematic review. Eur. J. Pain 2019, 24, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Bayattork, M.; Skovlund, S.V.; Sundstrup, E.; Andersen, L.L. Work limitations due to neck-shoulder pain and physical work demands in older workers: Cross-sectional study. Int. Arch. Occupat. Environ. Health 2021, 94, 433–440. [Google Scholar] [CrossRef]
- Stock, S.R.; Nicolakakis, N.; Vézina, N.; Vézina, M.; Gilbert, L.; Turcot, A.; Taïeb, H.S.; Sinden, K. Are work organization interventions effective in preventing or reducing work-related musculoskeletal disorders? A systematic review of the literature. Scandinav. J. Work Environ. Health 2018, 44, 113–133. [Google Scholar] [CrossRef] [PubMed]
- Bau, J.-G.; Wu, S.-K.; Huang, B.-W.; Lin, T.T.-L.; Huang, S.-C. Myofascial Treatment for Microcirculation in Patients with Postural Neck and Shoulder Pain. Diagnostics 2021, 11, 2226. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Control Group (n = 16) | Patient Group (n = 16) | p Value | |
|---|---|---|---|
| Age (years) | 35.3 ± 4.3 | 40.6 ± 6.5 | 0.016 * |
| BMI (kg/m2) | 22.2 ± 2.8 | 24.4 ± 3.7 | 0.09 |
| SBP (mmHg) | 117.6 ± 11.9 | 122.7 ± 16.3 | 0.25 |
| DBP (mmHg) | 73.5 ± 9.8 | 74.3 ± 10.5 | 0.925 |
| Exercise/week (hours) | 2.4 ± 3.1 | 0.9 ± 1.7 | 0.119 |
| Sitting/day (hours) | 6.4 ± 1.7 | 6.3 ± 3.2 | 0.499 |
| Time using 3C products/day (hours) | 7.5 ± 2.9 | 4.8 ± 3.3 | 0.048 * |
| Shoulder pain level | 1.1 ± 1.6 | 6.5 ± 1.6 | <0.001 ** |
| MMBF | 66.6 ± 10.6 | 58.9 ± 29.6 | 0.065 |
| Absolute-deviationMMBF | 9.0 ± 5.6 | 9.9 ± 15.3 | <0.001 ** |
| Age | MMBF | MMBF deviation | Shoulder Pain Level | Pain Duration | Symptom Effect | |
|---|---|---|---|---|---|---|
| Age (years) | 1 | |||||
| MMBF | −0.066 | 1 | ||||
| MMBF deviation | 0.350 * | −0.432 * | 1 | |||
| Shoulder pain level | 0.408 * | −0.202 | 0.650 ** | 1 | ||
| Pain duration | 0.392 * | −0.230 | 0.641 ** | 0.819 ** | 1 | |
| Symptom effect | 0.262 | −0.227 | 0.450 ** | 0.792 ** | 0.662 ** | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chia, T.; Bau, J.-G.; Hung, G.-D.; Tsai, S.-H.; Hu, C.-M. Evaluation of Shoulder Microcirculation Abnormality Using Laser Doppler Flowmetry. Diagnostics 2022, 12, 143. https://doi.org/10.3390/diagnostics12010143
Chia T, Bau J-G, Hung G-D, Tsai S-H, Hu C-M. Evaluation of Shoulder Microcirculation Abnormality Using Laser Doppler Flowmetry. Diagnostics. 2022; 12(1):143. https://doi.org/10.3390/diagnostics12010143
Chicago/Turabian StyleChia, Taipau, Jian-Guo Bau, Guo-Dung Hung, Sz-Huan Tsai, and Che-Ming Hu. 2022. "Evaluation of Shoulder Microcirculation Abnormality Using Laser Doppler Flowmetry" Diagnostics 12, no. 1: 143. https://doi.org/10.3390/diagnostics12010143
APA StyleChia, T., Bau, J.-G., Hung, G.-D., Tsai, S.-H., & Hu, C.-M. (2022). Evaluation of Shoulder Microcirculation Abnormality Using Laser Doppler Flowmetry. Diagnostics, 12(1), 143. https://doi.org/10.3390/diagnostics12010143