
Comparability between Computed Tomography Morphological Vascular Parameters and Echocardiography for the Assessment of Pulmonary Hypertension in Patients with Severe Aortic Valve Stenosis—Results of a Multi-Center Study
 , , , ,
, , , , 
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population
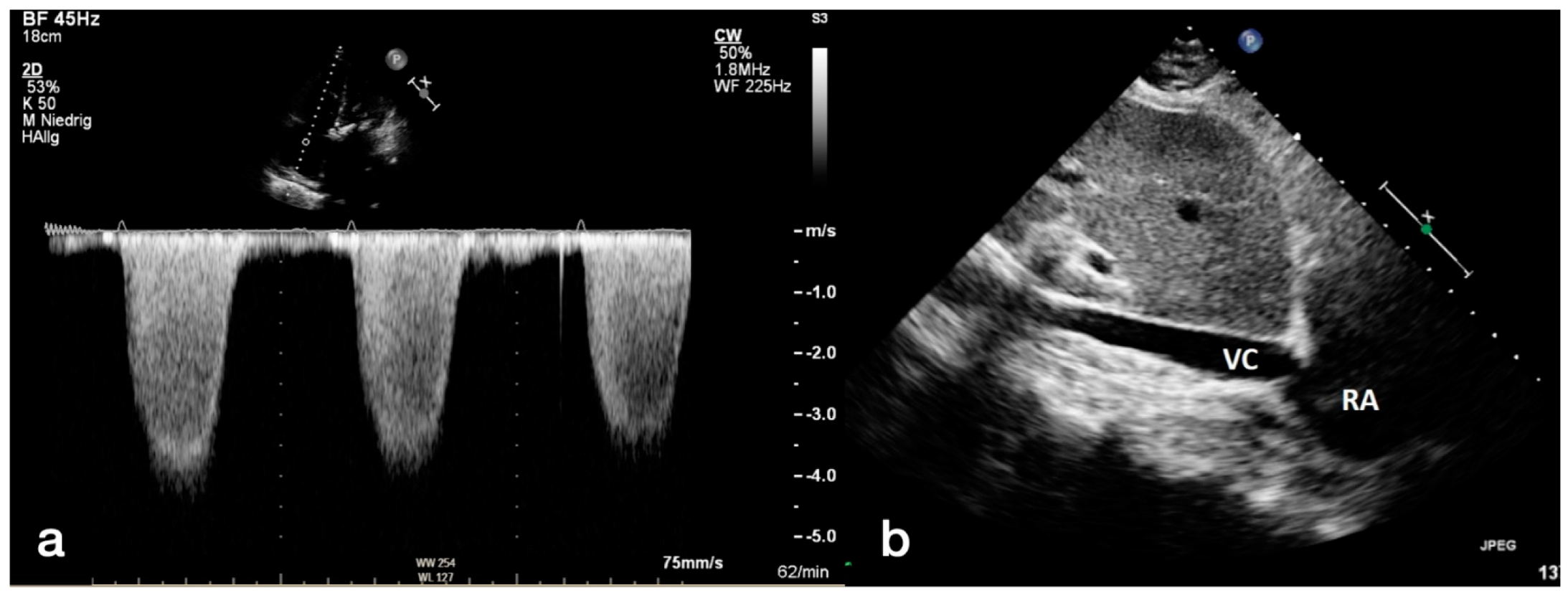
2.2. Transthoracic Echocardiography
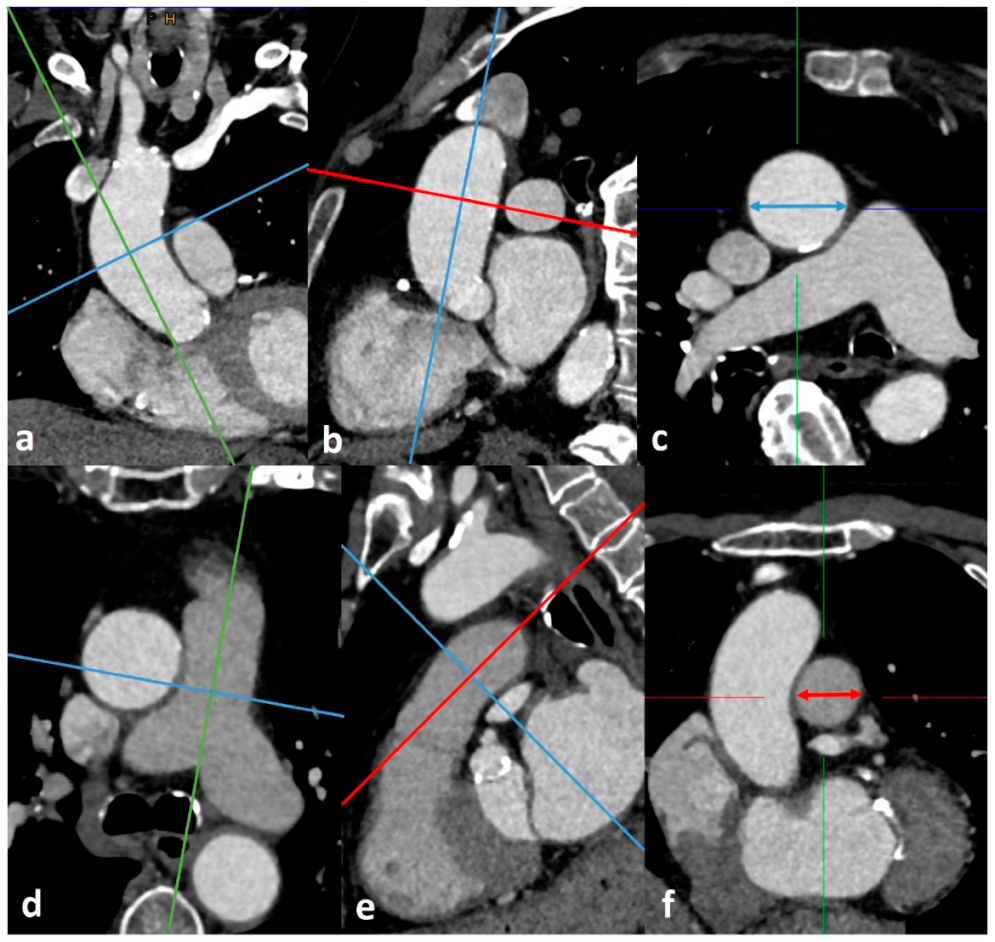
2.3. CTA Protocol and Measurement of Diameters for PH Assessment
- The widest short-axis diameter of the main pulmonary artery (PA) within 3 cm of the bifurcation of the pulmonary trunk.
- The widest short-axis diameter of the ascending aorta (AA) at the level of the bifurcation of the pulmonary trunk.
- The widest short-axis diameter of the right pulmonary artery (RPA).
- The widest short-axis diameter of the left pulmonary artery (LPA).
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
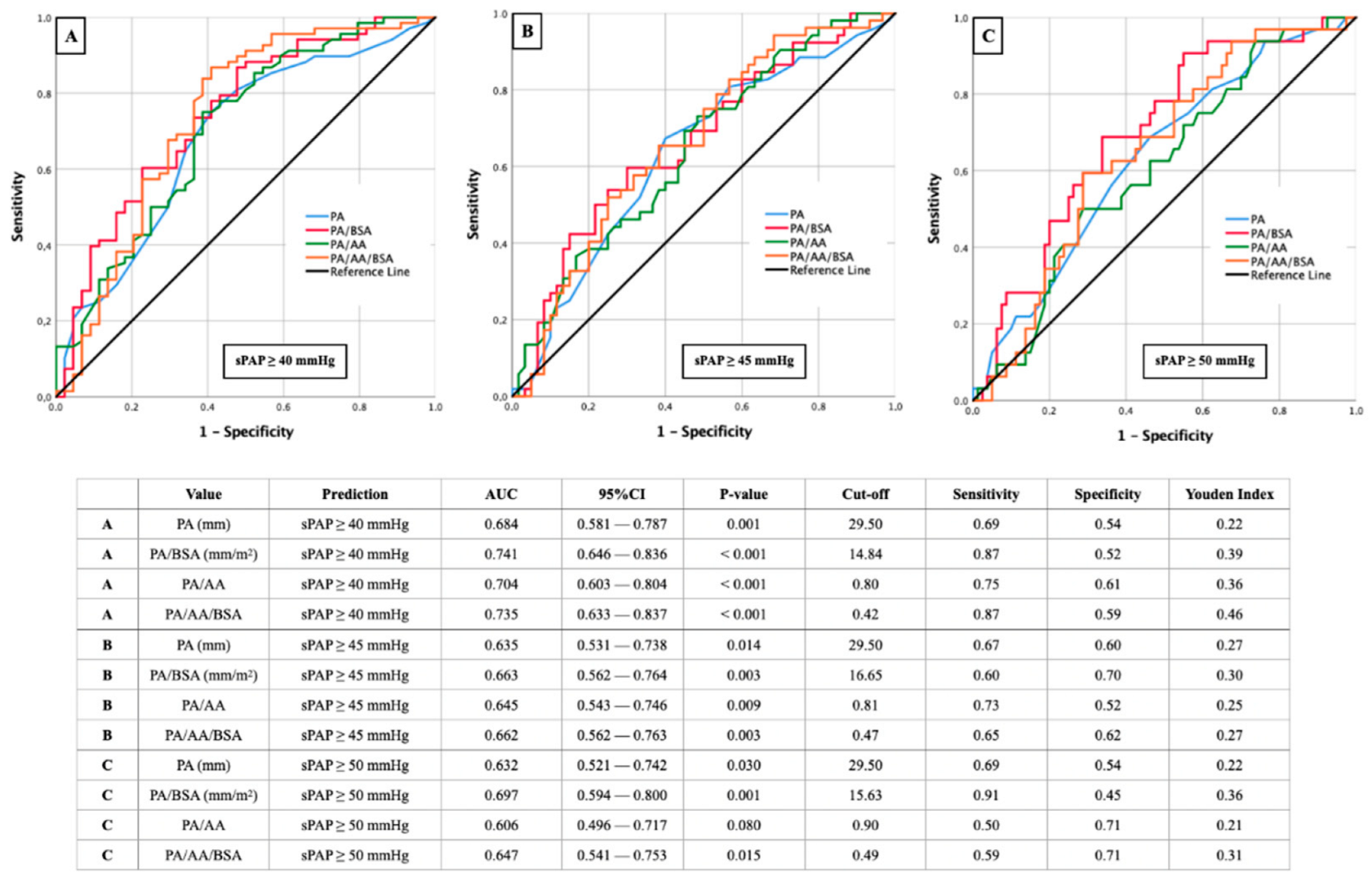
3.2. AUROC Results—sPAP and PA (±Ratios)
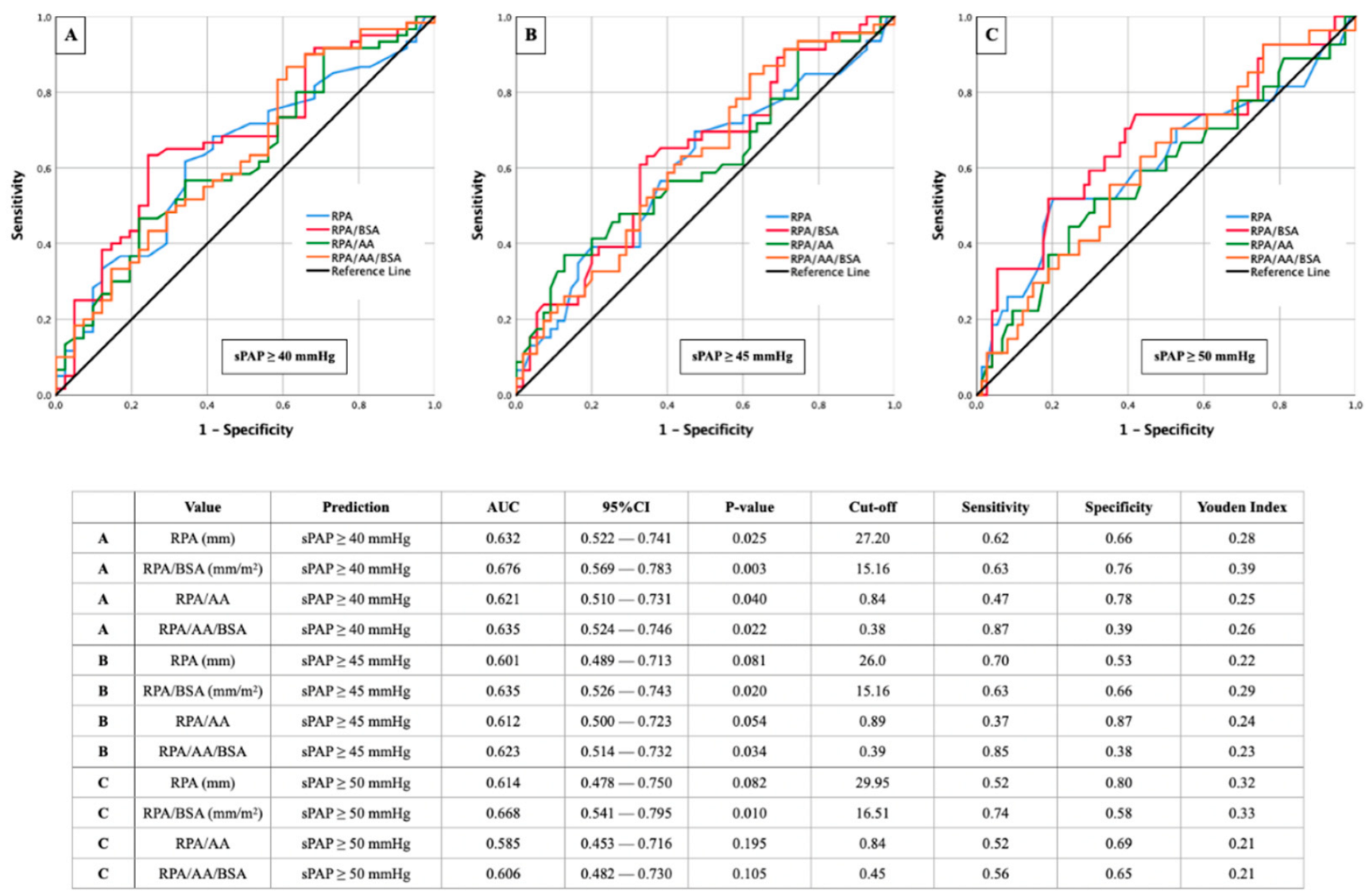
3.3. AUROC Results—sPAP and RPA (±Ratios)
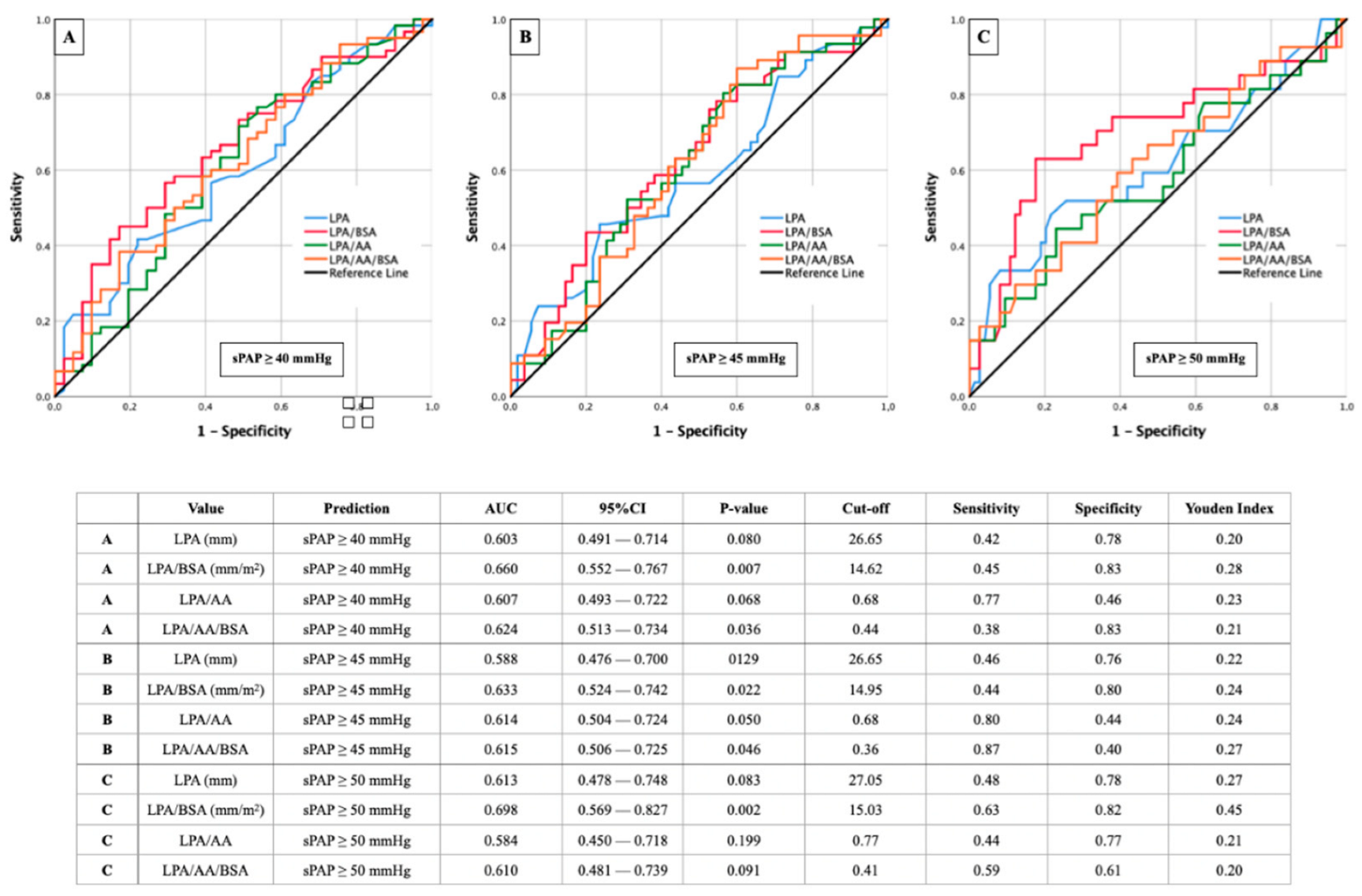
3.4. AUROC Results—sPAP and LPA (±Ratios)
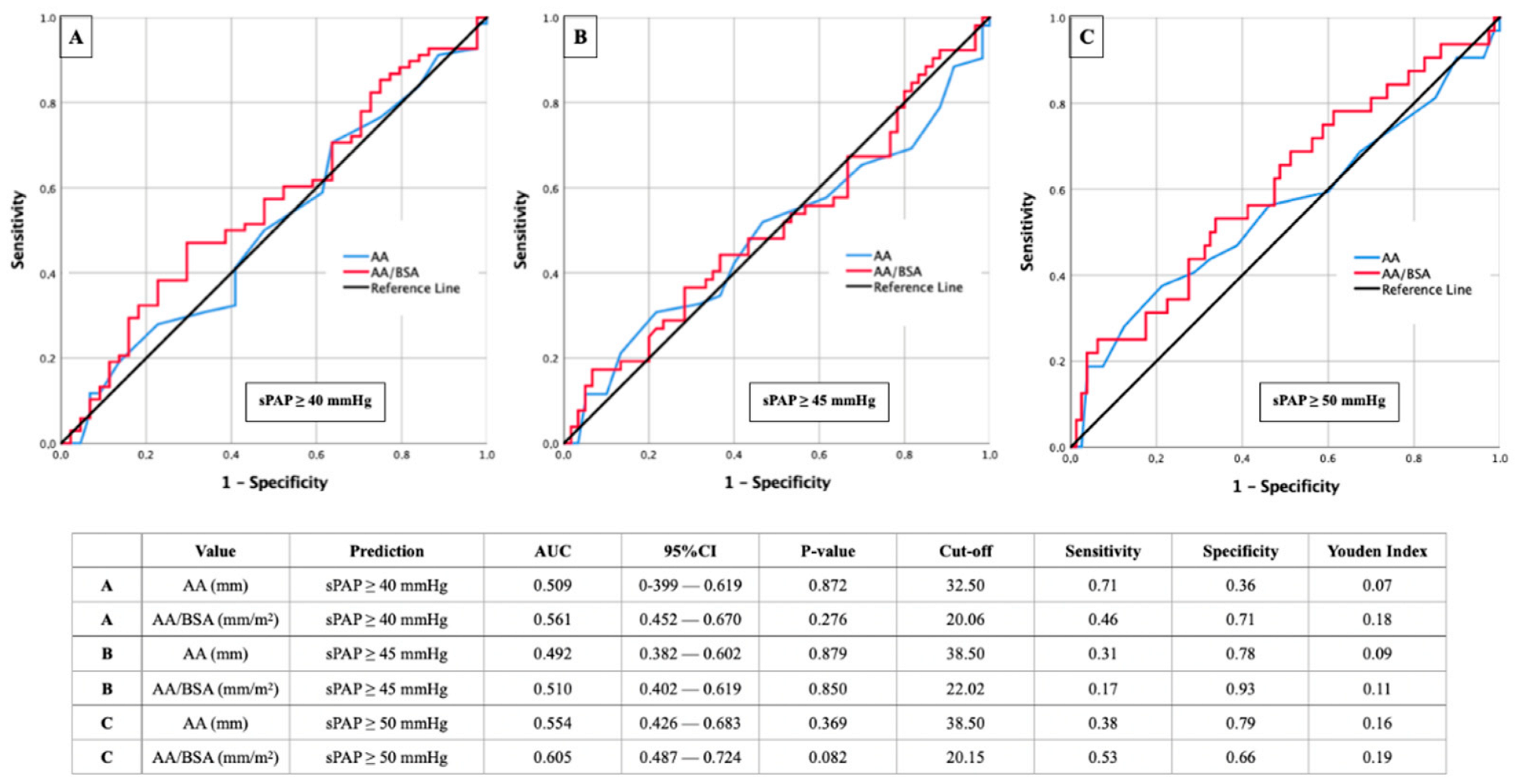
3.5. AUROC Results—sPAP and AA (±Ratios)
3.6. Correlation Analysis
4. Discussion
4.1. sPAP 40 mmHg with the Best Results—Pathophysiological Attempt of Explanations
4.2. PA vs. LPA and RPA—Why Do the Pulmonary Arteries Perform Worse Compared to the Pulmonary Trunk?
4.3. Body Surface Area—Significantly Improved Informative Value through Indexing
5. Conclusions
6. Limitation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wake, N.; Kumamaru, K.; Prior, R.; Rybicki, F.J.; Steigner, M.L. Computed tomography angiography for transcatheter aortic valve replacement. Radiol. Technol. 2013, 84, 326–340. [Google Scholar] [PubMed]
- Schwarz, F.; Lange, P.; Zinsser, D.; Greif, M.; Boekstegers, P.; Schmitz, C.; Reiser, M.F.; Kupatt, C.; Becker, H.C. CT-angiography-based evaluation of the aortic annulus for prosthesis sizing in transcatheter aortic valve implantation (TAVI)-predictive value and optimal thresholds for major anatomic parameters. PLoS ONE 2014, 9, e103481. [Google Scholar] [CrossRef] [PubMed]
- Alushi, B.; Beckhoff, F.; Leistner, D.; Franz, M.; Reinthaler, M.; Stähli, B.E.; Morguet, A.; Figulla, H.R.; Doenst, T.; Maisano, F.; et al. Pulmonary Hypertension in Patients with Severe Aortic Stenosis: Prognostic Impact After Transcatheter Aortic Valve Replacement: Pulmonary Hypertension in Patients Undergoing TAVR. JACC Cardiovasc. Imaging 2019, 12, 591–601. [Google Scholar] [CrossRef] [PubMed]
- Ruopp, N.F.; Cockrill, B.A. Diagnosis and Treatment of Pulmonary Arterial Hypertension: A Review. JAMA 2022, 327, 1379–1391. [Google Scholar] [CrossRef]
- Ruaro, B.; Confalonieri, P.; Caforio, G.; Baratella, E.; Pozzan, R.; Tavano, S.; Bozzi, C.; Lerda, S.; Geri, P.; Biolo, M.; et al. Chronic Thromboembolic Pulmonary Hypertension: An Observational Study. Medicina 2022, 58, 1094. [Google Scholar] [CrossRef]
- Galiè, N.; Humbert, M.; Vachiery, J.L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Vonk Noordegraaf, A.; Beghetti, M.; et al. ESC Scientific Document Group 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur. Heart J. 2016, 37, 67–119. [Google Scholar] [CrossRef]
- Humbert, M.; Kovacs, G.; Hoeper, M.M.; Badagliacca, R.; Berger, R.; Brida, M.; Carlsen, J.; Coats, A.; Escribano-Subias, P.; Ferrari, P.; et al. ESC/ERS Scientific Document Group 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Heart J. 2022; Epub ahead of printing. [Google Scholar] [CrossRef]
- Boxhammer, E.; Berezin, A.E.; Paar, V.; Bacher, N.; Topf, A.; Pavlov, S.; Hoppe, U.C.; Lichtenauer, M. Severe Aortic Valve Stenosis and Pulmonary Hypertension: A Systematic Review of Non-Invasive Ways of Risk Stratification, Especially in Patients Undergoing Transcatheter Aortic Valve Replacement. J. Pers. Med. 2022, 12, 603. [Google Scholar] [CrossRef]
- Kapoor, N.; Varadarajan, P.; Pai, R.G. Echocardiographic predictors of pulmonary hypertension in patients with severe aortic stenosis. Eur. J. Echocardiogr. 2008, 9, 31–33. [Google Scholar] [CrossRef]
- Masri, A.; Abdelkarim, I.; Sharbaugh, M.S.; Althouse, A.D.; Xu, J.; Han, W.; Chan, S.Y.; Katz, W.E.; Crock, F.W.; Harinstein, M.E.; et al. Outcomes of persistent pulmonary hypertension following transcatheter aortic valve replacement. Heart 2018, 104, 821–827. [Google Scholar] [CrossRef]
- Mutlak, D.; Aronson, D.; Carasso, S.; Lessick, J.; Reisner, S.A.; Agmon, Y. Frequency, determinants and outcome of pulmonary hypertension in patients with aortic valve stenosis. Am. J. Med. Sci. 2012, 343, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Barbash, I.M.; Escarcega, R.O.; Minha, S.; Ben-Dor, I.; Torguson, R.; Goldstein, S.A.; Wang, Z.; Okubagzi, P.; Satler, L.F.; Pichard, A.D.; et al. Prevalence and impact of pulmonary hypertension on patients with aortic stenosis who underwent transcatheter aortic valve replacement. Am. J. Cardiol. 2015, 115, 1435–1442. [Google Scholar] [CrossRef] [PubMed]
- Boxhammer, E.; Paar, V.; Jirak, P.; Köller, C.; Demirel, O.; Eder, S.; Reiter, C.; Kammler, J.; Kellermair, J.; Hammerer, M.; et al. Main pulmonary artery diameter in combination with cardiovascular biomarkers. New possibilities to identify pulmonary hypertension in patients with severe aortic valve stenosis? Minerva Med. 2022; Epub ahead of printing. [Google Scholar] [CrossRef] [PubMed]
- Schewel, J.; Schlüter, M.; Schmidt, T.; Kuck, K.H.; Frerker, C.; Schewel, D. Correlation between Doppler echocardiography and right heart catheterization assessment of systolic pulmonary artery pressure in patients with severe aortic stenosis. Echocardiography 2020, 37, 380–387. [Google Scholar] [CrossRef]
- Freeman, L.A.; Young, P.M.; Foley, T.A.; Williamson, E.E.; Bruce, C.J.; Greason, K.L. CT and MRI assessment of the aortic root and ascending aorta. AJR. Am. J. Roentgenol. 2013, 200, W581–W592. [Google Scholar] [CrossRef] [PubMed]
- Hossain, R.; Chelala, L.; Sleilaty, G.; Amin, S.; Vairavamurthy, J.; Chen, R.; Gupta, A.; Jeudy, J.; White, C. Preprocedure CT Findings of Right Heart Failure as a Predictor of Mortality After Transcatheter Aortic Valve Replacement. AJR. Am. J. Roentgenol. 2021, 216, 57–65. [Google Scholar] [CrossRef]
- Thenappan, T.; Chan, S.Y.; Weir, E.K. Role of extracellular matrix in the pathogenesis of pulmonary arterial hypertension. Am. J. Physiol. Heart Circ. Physiol. 2018, 315, H1322–H1331. [Google Scholar] [CrossRef]
- Lammers, S.R.; Kao, P.H.; Qi, H.J.; Hunter, K.; Lanning, C.; Albietz, J.; Hofmeister, S.; Mecham, R.; Stenmark, K.R.; Shandas, R. Changes in the structure-function relationship of elastin and its impact on the proximal pulmonary arterial mechanics of hypertensive calves. Am. J. Physiol. Heart Circ. Physiol. 2008, 295, H1451–H1459. [Google Scholar] [CrossRef]
- Bertero, T.; Oldham, W.M.; Cottrill, K.A.; Pisano, S.; Vanderpool, R.R.; Yu, Q.; Zhao, J.; Tai, Y.; Tang, Y.; Zhang, Y.Y.; et al. Vascular stiffness mechanoactivates YAP/TAZ-dependent glutaminolysis to drive pulmonary hypertension. J. Clin. Investig. 2016, 126, 3313–3335. [Google Scholar] [CrossRef]
- Rehman, A.; Darira, J.; Ahmed, M.S.; Hamid, K.; Shazlee, M.K.; Hyder, S. Evaluating Signs of Pulmonary Hypertension on Computed Tomography and Correlating with Echocardiography: A Study at a Tertiary Care Hospital. Cureus 2022, 14, e25319. [Google Scholar] [CrossRef]
- Ussavarungsi, K.; Whitlock, J.; Lundy, T.; Carabenciov, I.; Burger, C.; Lee, A. The Significance of Pulmonary Artery Size in Pulmonary Hypertension. Diseases 2014, 2, 243–259. [Google Scholar] [CrossRef]
- Zhu, Y.; Tang, X.; Wang, Z.; Wei, Y.; Zhu, X.; Liu, W.; Xu, Y.; Tang, L.; Shi, H. Pulmonary Hypertension Parameters Assessment by Electrocardiographically Gated Computed Tomography: Normal Limits by Age, Sex, and Body Surface Area in a Chinese Population. J. Thorac. Imaging 2019, 34, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Mahammedi, A.; Oshmyansky, A.; Hassoun, P.M.; Thiemann, D.R.; Siegelman, S.S. Pulmonary artery measurements in pulmonary hypertension: The role of computed tomography. J. Thorac. Imaging 2013, 28, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Sudo, M.; Sugiura, A.; Treiling, L.; Al-Kassou, B.; Shamekhi, J.; Kütting, D.; Wilde, N.; Weber, M.; Zimmer, S.; Nickenig, G.; et al. Baseline PA/BSA ratio in patients undergoing transcatheter aortic valve replacement—A novel CT-based marker for the prediction of pulmonary hypertension and outcome. Int. J. Cardiol. 2022, 348, 26–32. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall Cohort n = 138 | |
|---|---|
| Clinical Data | |
| Age (years)–mean ± SD | 82.98 ± 5.05 |
| Gender (male)–% | 52.2 |
| Weight (kg)–mean ± SD | 73.55 ± 12.90 |
| Height (cm)–mean ± SD | 167.44 ± 8.67 |
| BMI (kg/m2)–mean ± SD | 26.21 ± 4.07 |
| BSA (m2)–mean ± SD | 1.82 ± 0.17 |
| NYHA–median ± IQR | 3.00 ± 0.50 |
| STSScore–mean ± SD | 3.01 ± 1.50 |
| Concomitant Disease | |
| Diabetes mellitus–% | 22.5 |
| Arterial Hypertension–% | 81.9 |
| CVD–% | 69.6 |
| CVD–1 vessel–% | 19.6 |
| CVD–2 vessels–% | 13.8 |
| CVD–3 vessels–% | 14.5 |
| Myocardial infarction–% | 3.6 |
| Atrial fibrillation–% | 34.1 |
| Pacemaker–% | 5.1 |
| Malignancy–% | 20.3 |
| Stroke–% | 7.2 |
| PAD–% | 6.5 |
| COPD–% | 8.0 |
| Echocardiography | |
| LVEF (%)–mean ± SD | 53.92 ± 10.32 |
| LVEDD (mm)–mean ± SD | 46.76 ± 6.18 |
| AV Vmax (m/s)–mean ± SD | 4.41 ± 0.52 |
| AV dPmean (mmHg)–mean ± SD | 49.76 ± 11.80 |
| AV dPmax (mmHg)–mean ± SD | 80.71 ± 18.80 |
| sPAP (mmHg)–mean ± SD | 44.94 ± 16.65 |
| sPAP ≥ 40 mmHg–% | 63.0 |
| sPAP ≥ 45 mmHg–% | 50.0 |
| sPAP ≥ 50 mmHg–% | 33.3 |
| TAPSE (mm)–mean ± SD | 22.01 ± 3.72 |
| AVI ≥ II°–% | 16.7 |
| MVI ≥ II°–% | 31.2 |
| TVI ≥ II°–% | 21.7 |
| Computed Tomography | |
| PA ≥ 29 mm–% | 60.9 |
| PA/AA ≥ 0.80–% | 62.9 |
| PA/AA ≥ 0.90–% | 35.7 |
| Laboratory Data | |
| Crea (mg/dL)–median ± IQR | 1.00 ± 0.40 |
| BNP (pg/mL)–median ± IQR | 1797.00 ± 2978.60 |
| cTnI (pg/mL)–median ± IQR | 22.00 ± 30.00 |
| Hkt (%)–median ± IQR | 39.00 ± 7.35 |
| Hb (g/dL)–median ± IQR | 12.90 ± 2.30 |
| CK (U/L)–median ± IQR | 74.00 ± 82.50 |
| Overall Cohort n = 138 | sPAP ≥ 40 mmHg n = 87 | sPAP ≥ 45 mmHg n = 69 | sPAP ≥ 50 mmHg n = 46 | |
|---|---|---|---|---|
| Clinical Data | ||||
| PA (mm)–mean ± SD | 29.89 ± 5.45 | 31.19 ± 5.41 | 30.98 ± 5.22 | 31.56 ± 5.35 |
| AA (mm)–mean ± SD | 35.10 ± 4.61 | 35.12 ± 4.58 | 35.04 ± 4.94 | 35.84 ± 5.39 |
| PA/BSA (mm/m2)–mean ± SD | 16.51 ± 3.00 | 17.33 ± 2.52 | 17.22 ± 2.53 | 17.72 ± 2.36 |
| PA/AA–mean ± SD | 0.86 ± 0.13 | 0.89 ± 0.13 | 0.89 ± 0.13 | 0.89 ± 0.12 |
| PA/AA/BSA–mean ± SD | 0.47 ± 0.08 | 0.50 ± 0.07 | 0.50 ± 0.08 | 0.50 ± 0.07 |
| RPA (mm)–mean ± SD | 27.55 ± 4.59 | 28.40 ± 4.80 | 28.53 ± 5.06 | 28.98 ± 5.33 |
| RPA/BSA (mm/m2)–mean ± SD | 15.15 ± 2.45 | 15.68 ± 2.41 | 15.71 ± 2.46 | 16.06+ 2.56 |
| RPA/AA–mean ± SD | 0.79 ± 0.13 | 0.81 ± 0.13 | 0.82 ± 0.14 | 0.81 ± 0.13 |
| RPA/AA/BSA–mean ± SD | 0.44 ± 0.08 | 0.45 ± 0.08 | 0.46 ± 0.08 | 0.46 ± 0.08 |
| LPA (mm)–mean ± SD | 25.45 ± 3.43 | 26.00 ± 3.58 | 26.12 ± 3.73 | 26.66 ± 3.97 |
| LPA/BSA (mm/m2)–mean ± SD | 14.01 ± 1.93 | 14.39 ± 2.00 | 14.42 ± 2.00 | 14.84 ± 2.27 |
| LPA/AA–mean ± SD | 0.73 ± 0.10 | 0.75 ± 0.10 | 0.75 ± 0.10 | 0.75 ± 0.12 |
| LPA/AA/BSA–mean ± SD | 0.40 ± 0.07 | 0.42 ± 0.07 | 0.42 ± 0.07 | 0.43 ± 0.08 |
| AA/BSA (mm/m2)–mean ± SD | 19.43 ± 2.64 | 19.59 ± 2.48 | 19.52 ± 2.68 | 20.19 ± 2.85 |
| Spearman Correlation | sPAP ≥ 40 mmHg | sPAP ≥ 45 mmHg | sPAP ≥ 50 mmHg | |||
|---|---|---|---|---|---|---|
| rs | p | rs | p | rs | p | |
| PA | 0.305 | 0.001 | 0.229 | 0.014 | 0.203 | 0.029 |
| PA/BSA | 0.408 | <0.001 | 0.282 | 0.003 | 0.309 | 0.001 |
| PA/AA | 0.324 | <0.001 | 0.236 | 0.011 | 0.156 | 0.096 |
| PA/AA/BSA | 0.398 | <0.001 | 0.281 | 0.003 | 0.230 | 0.014 |
| RPA | 0.239 | 0.015 | 0.191 | 0.052 | 0.193 | 0.050 |
| RPA/BSA | 0.291 | 0.003 | 0.220 | 0.025 | 0.239 | 0.015 |
| RPA/AA | 0.208 | 0.036 | 0.194 | 0.051 | 0.132 | 0.187 |
| RPA/AA/BSA | 0.230 | 0.021 | 0.212 | 0.033 | 0.162 | 0.106 |
| LPA | 0.184 | 0.062 | 0.160 | 0.106 | 0.178 | 0.070 |
| LPA/BSA | 0.246 | 0.012 | 0.200 | 0.043 | 0.252 | 0.010 |
| LPA/AA | 0.189 | 0.057 | 0.202 | 0.041 | 0.132 | 0.186 |
| LPA/AA/BSA | 0.210 | 0.035 | 0.199 | 0.046 | 0.169 | 0.091 |
| AA | 0.023 | 0.807 | −0.008 | 0.933 | 0.087 | 0.353 |
| AA/BSA | 0.103 | 0.278 | 0.018 | 0.851 | 0.165 | 0.082 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boxhammer, E.; Scharinger, B.; Kaufmann, R.; Brandtner, H.; Schmidbauer, L.; Kammler, J.; Kellermair, J.; Reiter, C.; Akbari, K.; Hammerer, M.; et al. Comparability between Computed Tomography Morphological Vascular Parameters and Echocardiography for the Assessment of Pulmonary Hypertension in Patients with Severe Aortic Valve Stenosis—Results of a Multi-Center Study. Diagnostics 2022, 12, 2363. https://doi.org/10.3390/diagnostics12102363
Boxhammer E, Scharinger B, Kaufmann R, Brandtner H, Schmidbauer L, Kammler J, Kellermair J, Reiter C, Akbari K, Hammerer M, et al. Comparability between Computed Tomography Morphological Vascular Parameters and Echocardiography for the Assessment of Pulmonary Hypertension in Patients with Severe Aortic Valve Stenosis—Results of a Multi-Center Study. Diagnostics. 2022; 12(10):2363. https://doi.org/10.3390/diagnostics12102363
Chicago/Turabian StyleBoxhammer, Elke, Bernhard Scharinger, Reinhard Kaufmann, Herwig Brandtner, Lukas Schmidbauer, Jürgen Kammler, Jörg Kellermair, Christian Reiter, Kaveh Akbari, Matthias Hammerer, and et al. 2022. "Comparability between Computed Tomography Morphological Vascular Parameters and Echocardiography for the Assessment of Pulmonary Hypertension in Patients with Severe Aortic Valve Stenosis—Results of a Multi-Center Study" Diagnostics 12, no. 10: 2363. https://doi.org/10.3390/diagnostics12102363
APA StyleBoxhammer, E., Scharinger, B., Kaufmann, R., Brandtner, H., Schmidbauer, L., Kammler, J., Kellermair, J., Reiter, C., Akbari, K., Hammerer, M., Blessberger, H., Steinwender, C., Hergan, K., Hoppe, U. C., Lichtenauer, M., & Hecht, S. (2022). Comparability between Computed Tomography Morphological Vascular Parameters and Echocardiography for the Assessment of Pulmonary Hypertension in Patients with Severe Aortic Valve Stenosis—Results of a Multi-Center Study. Diagnostics, 12(10), 2363. https://doi.org/10.3390/diagnostics12102363