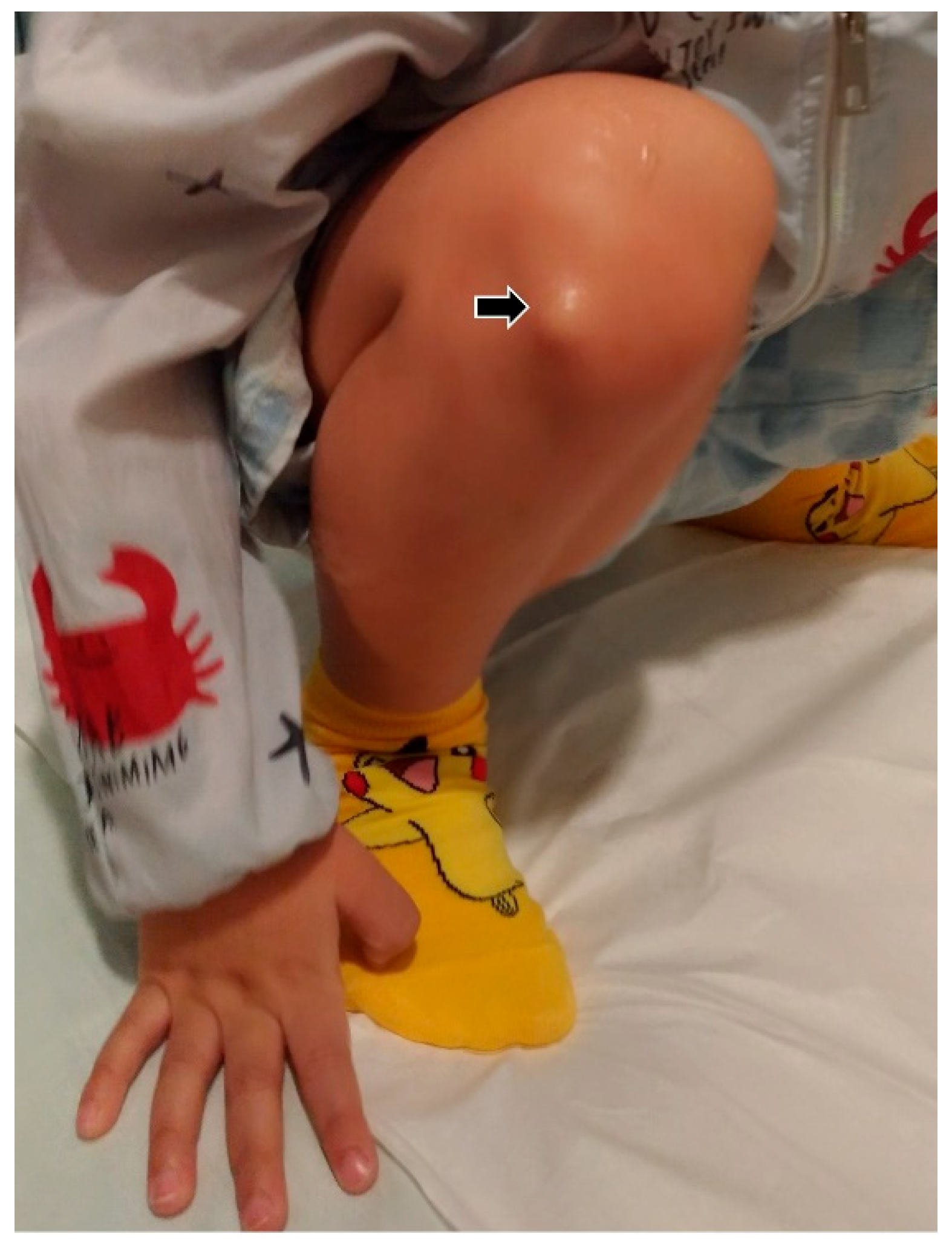
A 3-year-old boy was found to have a painless mass over his right anterior lateral knee. The onset of the mass was about 6 months prior to examination. Besides the mass, there was no obvious swelling at other compartments of his right knee. His mother did not recall any trauma in the affected knee. The mass was hardly identified during knee extension and became visible upon squatting. The mass was soft and elastic. No associated skin-color change was visualized. He was brought to the pediatric orthopedic clinic, where physical examination revealed normal bony alignment of his knees. Based on the initial impression of a ganglion cyst, he was referred for an ultrasound check-up. All of the sonographic images presented in this case report were obtained using a 13–18 MHz high-frequency linear transducer (Aplio 500, Canon Medical Systems Europe B.V., Zoetermeer, The Netherlands). The scanning depth was set between 2 and 3 cm, with the focus fixed at 1 cm deep.
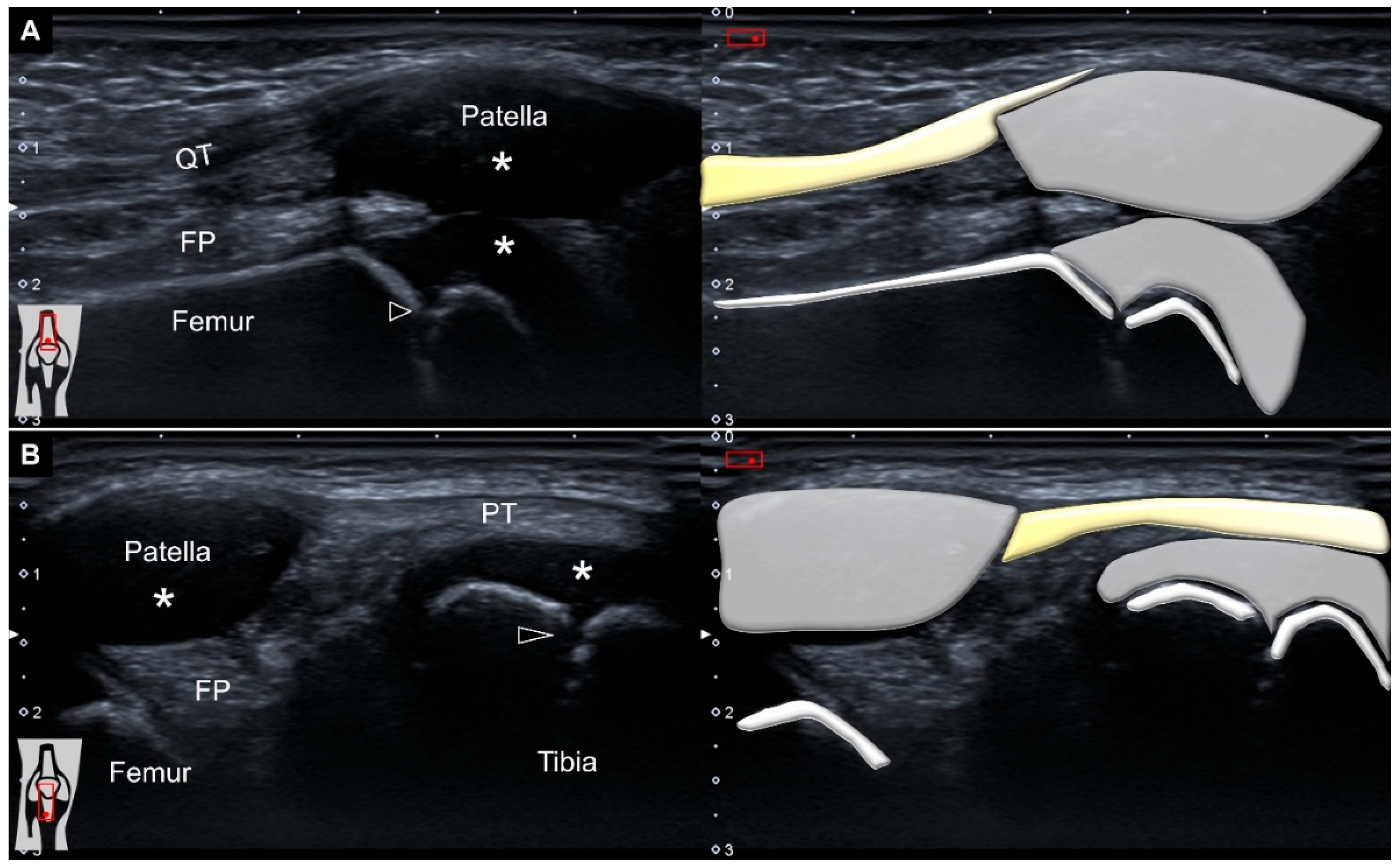
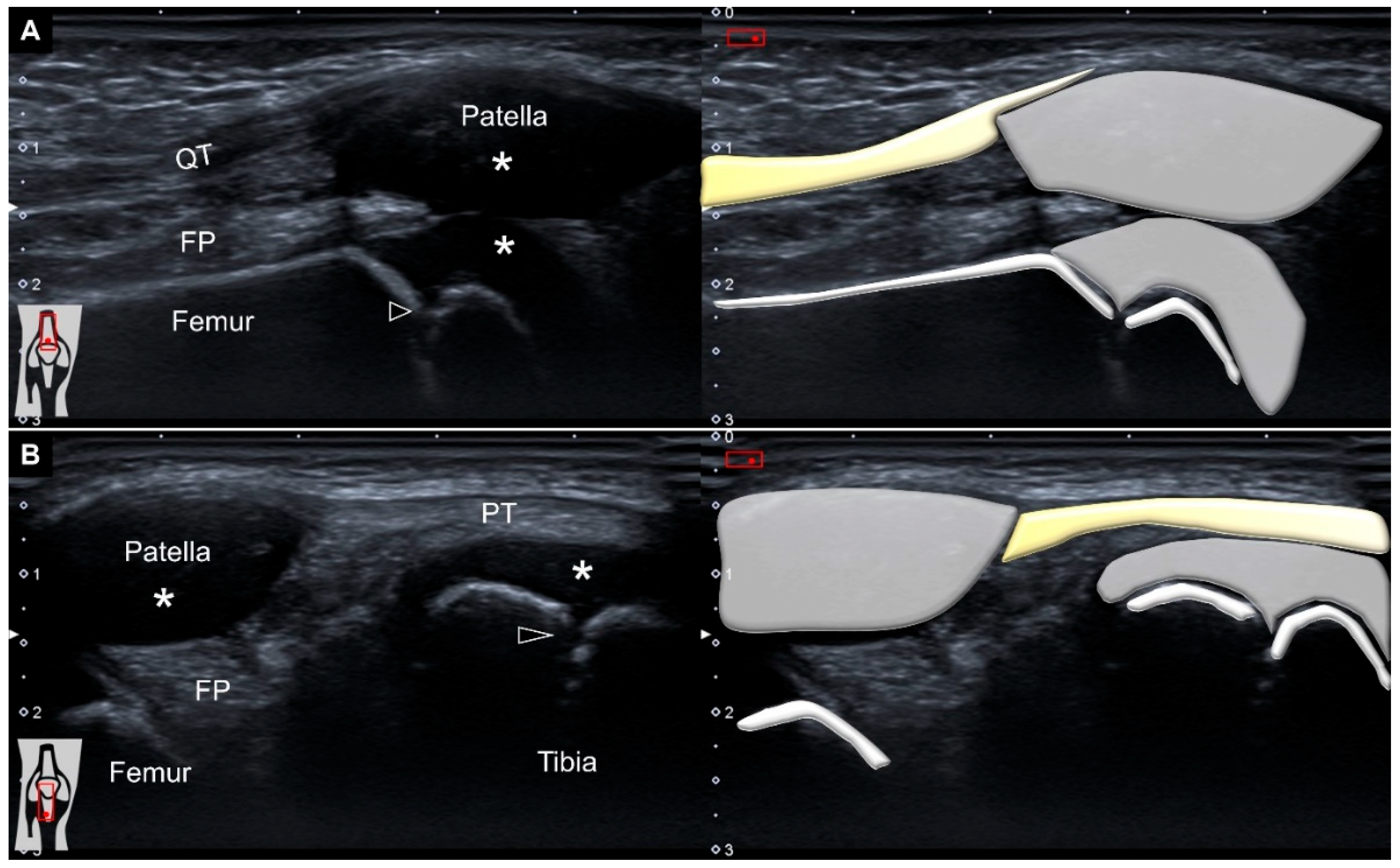
With his right knee extended in the supine position, ultrasound imaging over the suprapatellar region demonstrated no effusion, an intact quadriceps tendon, a non-ossified patella, prominent femoral cartilage, and a clear epiphyseal growth plate (
Figure 1A). The transducer was relocated distally to scan the infrapatellar area. Likewise, the fibrillar appearance of the patellar tendon remained without any remarkable pathologies (
Figure 1B).
As no obvious mass was identified in the supine position, we then asked him to squat so as to make the mass more visible (
Figure 2).
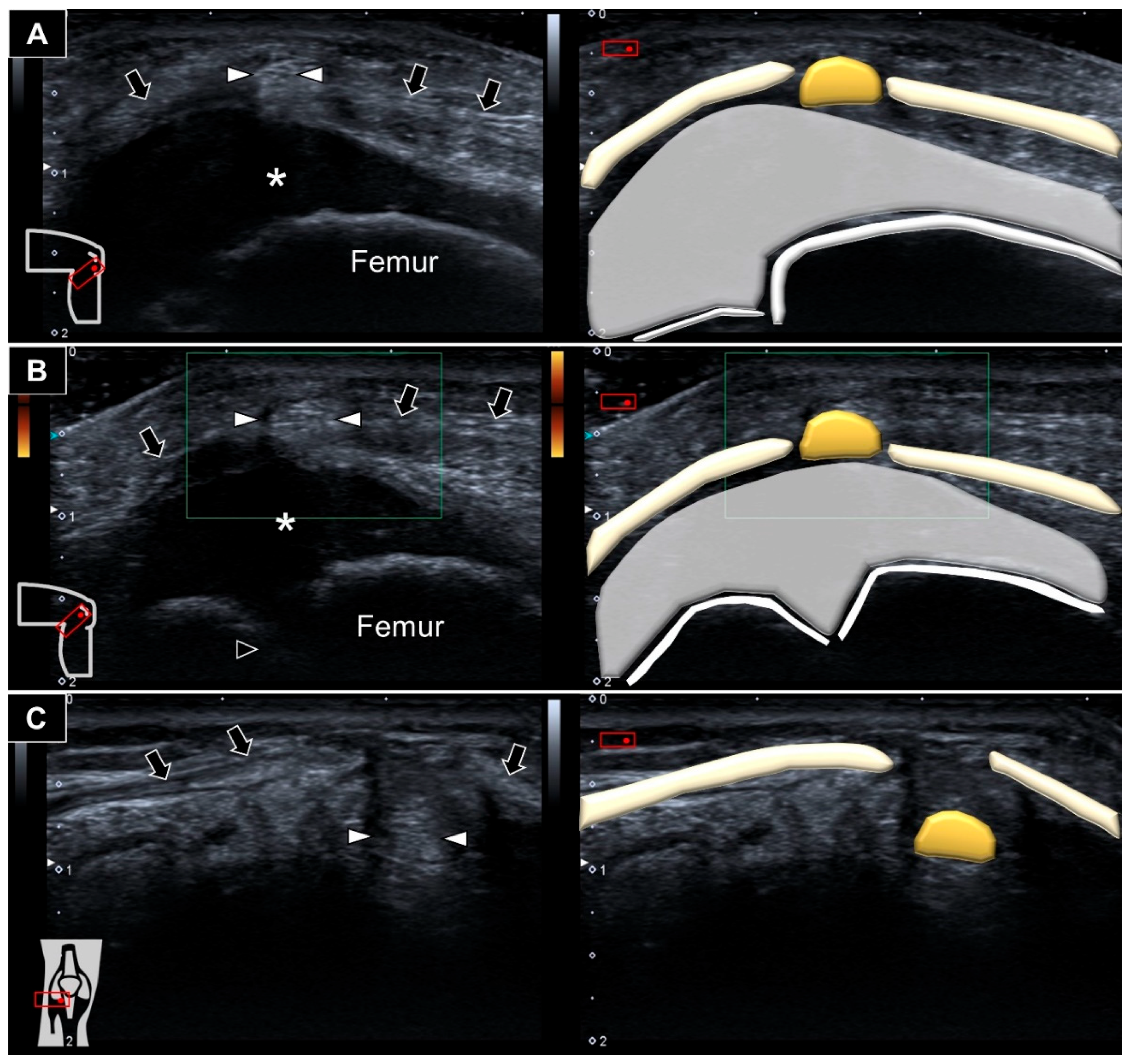
Ultrasound imaging showed an ill-demarcated hyperechoic mass protruding next to the cartilage overlying the distal femur towards the subcutaneous layer through a slit over the lateral patellar retinaculum (
Figure 3A and
Video S1). No increased vascularity was visualized inside or surrounding the lesion (
Figure 3B). Repositioning the knee back to extension while lying supine, the mass was seen sinking to the space underneath the lateral patellar retinaculum (
Figure 3C). Accordingly, herniation of the fat pad through a defect in the lateral patellar retinaculum was diagnosed.
Concerning musculoskeletal sonography, substantial differences might exist between children and adults [
1,
2]. Compared with those of adults, children’s bones harbor growth plates, profound cartilage, and visible juxta-articular vascularity [
3]. At the knee region in a 3-year-old child, the non-ossified patella appeared anechoic, mimicking effusion or a ganglion cyst. Furthermore, the growth plates manifest as discontinuity over the end of long bones, which can be misrecognized as fractures [
4]. All of the aforementioned factors might lead to difficulty in interpreting pediatric knee ultrasound examinations. In children with unilateral signs/symptoms, comparison with the asymptomatic side would be helpful in determining whether the finding is normal or pathological.
The anterior lateral knee component is a multilayer structure, whereas a two-layered or a three-layered model has been proposed by previous studies [
5,
6]. A recent study investigating the anatomical, histological, and radiological aspects of the anterior lateral knee compartment revealed that the lateral patellar retinaculum could actually be differentiated from the lateral patellar femoral ligament [
7]. A focal defect over the lateral patellar femoral retinaculum is not rare and is mostly asymptomatic. One magnetic resonance imaging study on adult patients revealed that the defect was associated with a decrease in the infrapatellar fat pad thickness, but not a lower Kellgren–Lawrence radiological grade of the knee joint [
8]. The authors also found that the correlation of the defect size with age, body weight, height, subcutaneous fat thickness, or the infrapatellar fat pad area was not statistically significant. Another ultrasound study on 48 healthy adult volunteers demonstrated that vessels could be consistently identified lateral to the patellar tendon, penetrating the defect to reach to the subcutaneous layer [
9]. The aforementioned research also revealed that the mean transverse diameter of the defect was 2.75 mm. Compared with magnetic resonance imaging, dynamic examination is more easily conducted under ultrasound [
10]. A case report of a 45-year-old man demonstrated that herniation of the fat pad through a slit of the lateral patellar retinaculum could be provoked after knee flexion and readily identified with ultrasound imaging [
11]. The defect in the above-discussed case might be derived from the anterolateral portal during the antecedent arthroscopic surgery. Similarly, the herniated fat pad in our patient could only be seen during squatting. To this end, our case highlighted the usefulness of ultrasound examination as regards pediatric knee problems, as well as its capability for dynamic scanning to capture the exact “pathological moment”.
Author Contributions
Conceptualization, W.-T.W. and K.-V.C.; methodology, K.-V.C.; software, K.-W.W.; validation, K.M., V.R., and L.Ö.; writing—original draft preparation, W.-T.W.; writing—review and editing, K.-V.C.; funding acquisition, K.-V.C. All authors have read and agreed to the published version of the manuscript.
Funding
This study was made possible by (1) research funding from the Community and Geriatric Medicine Research Center, National Taiwan University Hospital, Bei-Hu Branch, Taipei, Taiwan; (2) Ministry of Science and Technology (MOST 106-2314-B-002-180-MY3, 109-2314-B-002-114-MY3, and 109-2314-B-002-127), and (3) the Taiwan Society of Ultrasound in Medicine.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Patient consent was obtained.
Data Availability Statement
Data are contained within the main text of the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chang, K.V.; Sahin Onat, S.; Lee, C.W.; Kara, M.; Hung, C.Y.; Ozcakar, L. EURO-MUSCULUS/USPRM basic scanning protocols revisited in children. Eur. J. Phys. Rehabil. Med. 2016, 52, 887–901. [Google Scholar] [PubMed]
- Ozcakar, L.; Kara, M.; Chang, K.V.; Tok, F.; Hung, C.Y.; Akkaya, N.; Wu, C.H.; Carli, A.B.; Hsiao, M.Y.; Tekin, L.; et al. EURO-MUSCULUS/USPRM. Basic scanning protocols for knee. Eur. J. Phys. Rehabil. Med. 2015, 51, 641–646. [Google Scholar] [PubMed]
- Tok, F.; Demirkaya, E.; Özçakar, L. Musculoskeletal ultrasound in pediatric rheumatology. Pediatr. Rheumatol. 2011, 9, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Borja, C.; Watkins, R.; Woolridge, T. Common Ultrasound Applications for Pediatric Musculoskeletal Conditions. Curr. Rev. Musculoskelet. Med. 2022, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Fulkerson, J.P.; Gossling, H.R. Anatomy of the knee joint lateral retinaculum. Clin. Orthop. Relat. Res. 1980, 90, 183–188. [Google Scholar] [CrossRef]
- Merican, A.M.; Amis, A.A. Anatomy of the lateral retinaculum of the knee. J. Bone Joint Surg. Br. 2008, 90, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Biz, C.; Stecco, C.; Crimì, A.; Pirri, C.; Fosser, M.; Fede, C.; Fan, C.; Ruggieri, P.; De Caro, R. Are Patellofemoral Ligaments and Retinacula Distinct Structures of the Knee Joint? An Anatomic, Histological and Magnetic Resonance Imaging Study. Int. J. Environ. Res. Public Health 2022, 19, 1110. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.S.; Yun, S.J.; Jin, W.; Kim, G.Y.; Park, S.Y.; Park, J.S.; Ryu, K.N. A Focal Defect at the Lateral Patellar Retinaculum on Clinical Knee MRI and Cadaveric Study: A Normal Variant or Pathologic Lesion? AJR Am. J. Roentgenol. 2017, 208, 1103–1109. [Google Scholar] [CrossRef] [PubMed]
- Moraux, A.; Bianchi, S.; Tassery, F.; Le Corroller, T. The lateral patellar retinaculum defect: Anatomical study using ultrasound. Skelet. Radiol. 2019, 48, 1753–1758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, W.T.; Lin, C.Y.; Shu, Y.C.; Chen, L.R.; Ozcakar, L.; Chang, K.V. Subacromial Motion Metrics in Painful Shoulder Impingement: A Dynamic Quantitative Ultrasound Analysis. Arch. Phys. Med. Rehabil. 2022, in press. [Google Scholar] [CrossRef] [PubMed]
- Mezian, K.; Chang, K.V.; Zamecnik, D.; Mezian, H.; Ozcakar, L. Herniation of Hoffa’s Fat Pad Through the Lateral Retinaculum: Usefulness of Dynamic Ultrasonography to Diagnose a Lateral Knee Mass. Am. J. Phys. Med. Rehabil. 2018, 97, e113. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 
{kind=link}
{kind=link}
{kind=link}