
Influence of Medial Osteotomy Height and Hinge Position in Open Wedge High Tibial Osteotomy: A Simulation Study
 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
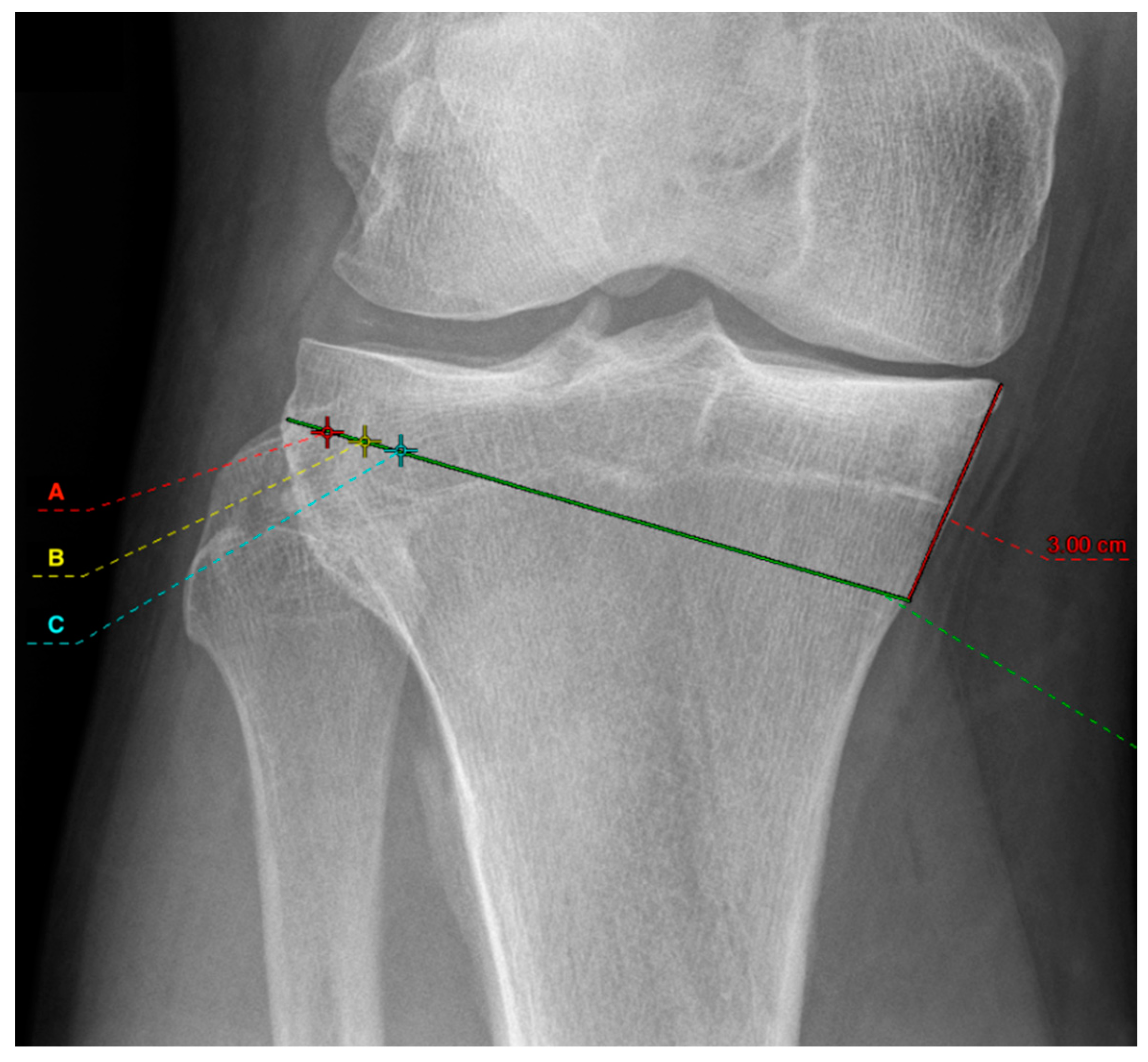
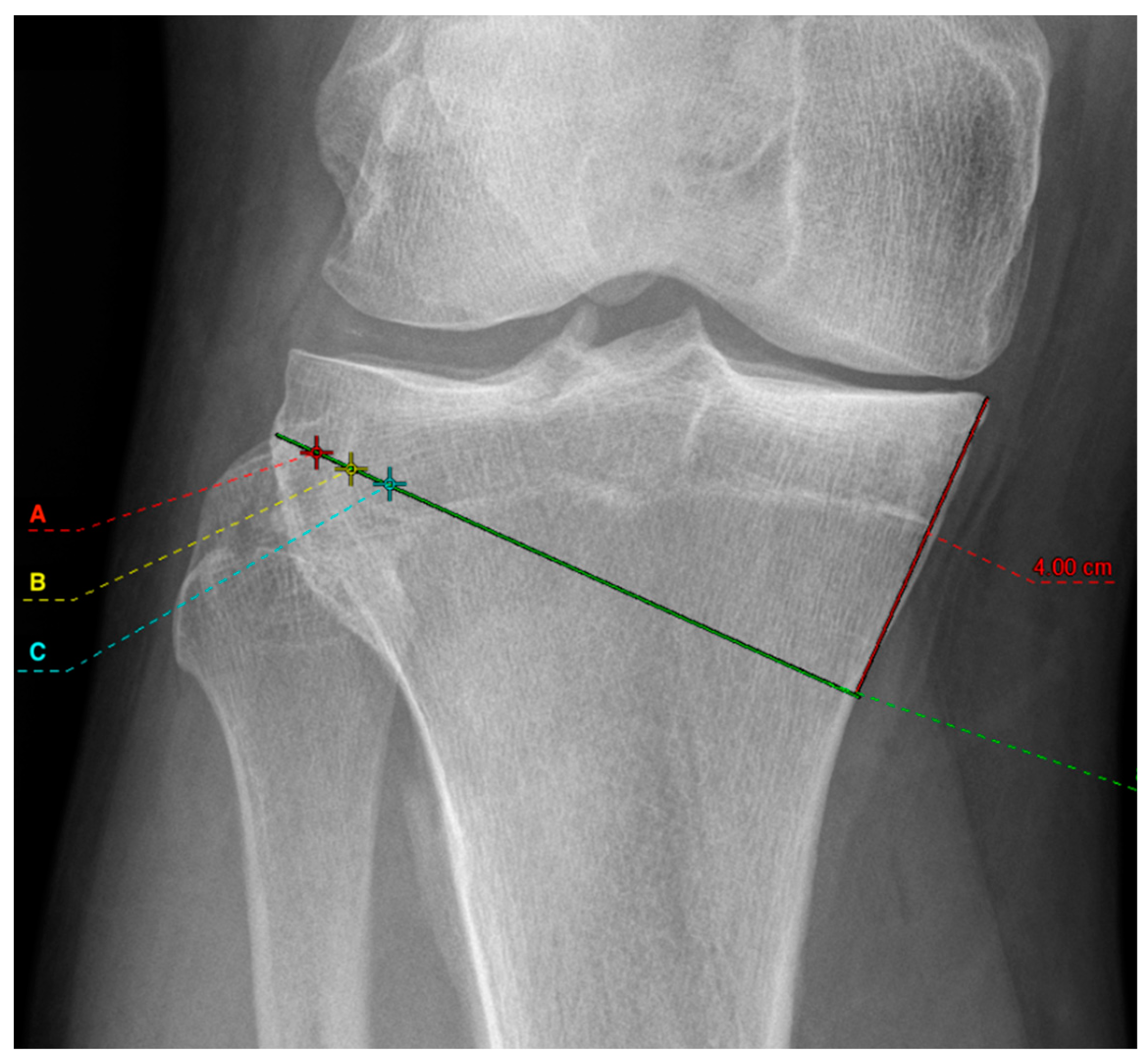
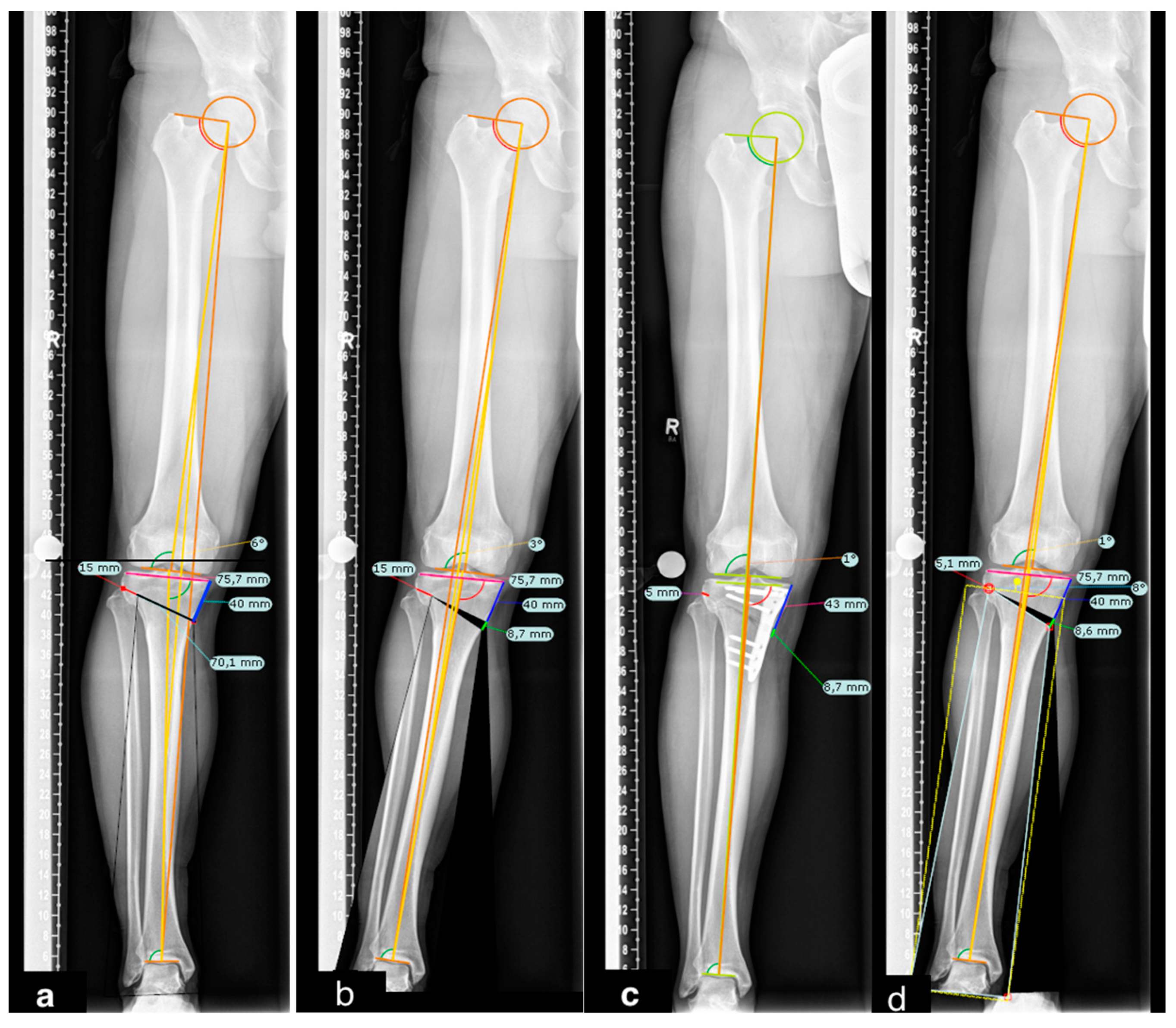
2.1. Radiographic Assessment
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Amendola, A.; Bonasia, D.E. Results of High Tibial Osteotomy: Review of the Literature. Int. Orthop. 2010, 34, 155–160. [Google Scholar] [CrossRef]
- Ollivier, B.; Berger, P.; Depuydt, C.; Vandenneucker, H. Good Long-Term Survival and Patient-Reported Outcomes after High Tibial Osteotomy for Medial Compartment Osteoarthritis. Knee Surgery Sport. Traumatol. Arthrosc. 2021, 29, 3569–3584. [Google Scholar] [CrossRef]
- Liu, J.N.; Agarwalla, A.; Garcia, G.H.; Christian, D.R.; Redondo, M.L.; Yanke, A.B.; Cole, B.J. Return to Sport Following Isolated Opening Wedge High Tibial Osteotomy. Knee 2019, 26, 1306–1312. [Google Scholar] [CrossRef]
- Hui, C.; Salmon, L.J.; Kok, A.; Williams, H.A.; Hockers, N.; Van Der Tempel, W.M.; Chana, R.; Pinczewski, L.A. Long-Term Survival of High Tibial Osteotomy for Medial Compartment Osteoarthritis of the Knee. Am. J. Sports Med. 2011, 39, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Jin, C.; Song, E.K.; Santoso, A.; Ingale, P.S.; Choi, I.S.; Seon, J.K. Survival and Risk Factor Analysis of Medial Open Wedge High Tibial Osteotomy for Unicompartment Knee Osteoarthritis. Arthrosc. J. Arthrosc. Relat. Surg. 2020, 36, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Keenan, O.J.F.; Clement, N.D.; Nutton, R.; Keating, J.F. Older Age and Female Gender Are Independent Predictors of Early Conversion to Total Knee Arthroplasty after High Tibial Osteotomy. Knee 2019, 26, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Kumagai, K.; Yamada, S.; Akamatsu, T.; Nejima, S.; Ogino, T.; Sotozawa, M.; Inaba, Y. Intraoperatively Accurate Limb Alignment after Opening Wedge High Tibial Osteotomy Can Be Lost by Large Knee Joint Line Convergence Angle during Surgery. Arch. Orthop. Trauma Surg. 2021, 141, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Krause, M.; Drenck, T.C.; Korthaus, A.; Preiss, A.; Frosch, K.H.; Akoto, R. Patella Height Is Not Altered by Descending Medial Open-Wedge High Tibial Osteotomy (HTO) Compared to Ascending HTO. Knee Surgery Sport. Traumatol. Arthrosc. 2018, 26, 1859–1866. [Google Scholar] [CrossRef]
- Song, S.J.; Bae, D.K.; Kim, K., II; Lee, C.H. Conversion Total Knee Arthroplasty after Failed High Tibial Osteotomy. Knee Surg. Relat. Res. 2016, 28, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.W.; Park, S.H.; Lee, B.H.; Oh, M.; Chang, M.; Ahn, J.H.; Wang, J.H. The Effect of Hinge Position on Posterior Tibial Slope in Medial Open-Wedge High Tibial Osteotomy. Arthrosc. J. Arthrosc. Relat. Surg. 2015, 31, 1128–1133. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.H.; Bae, J.H.; Lim, H.C.; Shon, W.Y.; Kim, C.W.; Cho, J.W. Medial Open Wedge High Tibial Osteotomy. Am. J. Sports Med. 2009, 37, 2411–2418. [Google Scholar] [CrossRef]
- Jo, H.S.; Park, J.S.; Byun, J.H.; Lee, Y.B.; Choi, Y.L.; Cho, S.H.; Moon, D.K.; Lee, S.H.; Hwang, S.C. The Effects of Different Hinge Positions on Posterior Tibial Slope in Medial Open-Wedge High Tibial Osteotomy. Knee Surgery Sport. Traumatol. Arthrosc. 2018, 26, 1851–1858. [Google Scholar] [CrossRef]
- Chen, P.; Zhan, Y.; Zhan, S.; Li, R.; Luo, C.; Xie, X. Biomechanical Evaluation of Different Types of Lateral Hinge Fractures in Medial Opening Wedge High Tibial Osteotomy. Clin. Biomech. 2021, 83, 105295. [Google Scholar] [CrossRef]
- Kumagai, K.; Yamada, S.; Nejima, S.; Muramatsu, S.; Akamatsu, Y.; Inaba, Y. Lateral Hinge Fracture Delays Healing of the Osteotomy Gap in Opening Wedge High Tibial Osteotomy with a Beta-Tricalcium Phosphate Block. Knee 2020, 27, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Pape, D.; Dueck, K.; Haag, M.; Lorbach, O.; Seil, R.; Madry, H. Wedge Volume and Osteotomy Surface Depend on Surgical Technique for High Tibial Osteotomy. Knee Surgery Sport. Traumatol. Arthrosc. 2013, 21, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Paley, D.; Herzenberg, J.E.; Tetsworth, K.; McKie, J.; Bhave, A. Deformity Planning for Frontal and Sagittal Plane Corrective Osteotomies. Orthop. Clin. N. Am. 1994, 25, 425–465. [Google Scholar] [CrossRef]
- Nakamura, R.; Komatsu, N.; Fujita, K.; Kuroda, K.; Takahashi, M.; Omi, R.; Katsuki, Y.; Tsuchiya, H. Appropriate Hinge Position for Prevention of Unstable Lateral Hinge Fracture in Open Wedge High Tibial Osteotomy. Bone Jt. J. 2017, 99B, 1313–1318. [Google Scholar] [CrossRef] [PubMed]
- Vieira, S.M.; Kaymak, U.; Sousa, J.M.C. Cohen’s Kappa Coefficient as a Performance Measure for Feature Selection. In Proceedings of the International Conference on Fuzzy Systems 2010, Barcelona, Spain, 18–23 July 2010. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159. [Google Scholar] [CrossRef] [PubMed]
- Mina, C.; Garrett, W.E.; Pietrobon, R.; Glisson, R.; Higgins, L. High Tibial Osteotomy for Unloading Osteochondral Defects in the Medial Compartment of the Knee. Am. J. Sports Med. 2008, 36, 949–955. [Google Scholar] [CrossRef] [PubMed]
- Hankemeier, S.; Mommsen, P.; Krettek, C.; Jagodzinski, M.; Brand, J.; Meyer, C.; Meller, R. Accuracy of High Tibial Osteotomy: Comparison between Open- and Closed-Wedge Technique. Knee Surgery Sport. Traumatol. Arthrosc. 2010, 18, 1328–1333. [Google Scholar] [CrossRef] [PubMed]
- Lo, W.N.; Cheung, K.W.; Yung, S.H.; Chiu, K.H. Arthroscopy-Assisted Computer Navigation in High Tibial Osteotomy for Varus Knee Deformity. J. Orthop. Surg. (Hong Kong) 2009, 17, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.H.; Park, S.C.; Park, H.J.; Han, S.B. Effect of Soft Tissue Laxity of the Knee Joint on Limb Alignment Correction in Open-Wedge High Tibial Osteotomy. Knee Surgery Sport. Traumatol. Arthrosc. 2016, 24, 3704–3712. [Google Scholar] [CrossRef]
- Marti, C.B.; Gautier, E.; Wachtl, S.W.; Jakob, R.P. Accuracy of Frontal and Sagittal Plane Correction in Open-Wedge High Tibial Osteotomy. Arthrosc. J. Arthrosc. Relat. Surg. 2004, 20, 366–372. [Google Scholar] [CrossRef] [PubMed]
- Kyung, B.S.; Kim, J.G.; Jang, K.M.; Chang, M.; Moon, Y.W.; Ahn, J.H.; Wang, J.H. Are Navigation Systems Accurate Enough to Predict the Correction Angle during High Tibial Osteotomy?: Comparison of Navigation Systems with 3-Dimensional Computed Tomography and Standing Radiographs. Am. J. Sports Med. 2013, 41, 2368–2374. [Google Scholar] [CrossRef] [PubMed]
- Schröter, S.; Ihle, C.; Mueller, J.; Lobenhoffer, P.; Stöckle, U.; van Heerwaarden, R. Digital Planning of High Tibial Osteotomy. Interrater Reliability by Using Two Different Software. Knee Surgery Sport. Traumatol. Arthrosc. 2013, 21, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.S.; Kim, M.G.; Byun, H.W.; Kim, S.B.; Kim, J.G. Reliability of the Imaging Software in the Preoperative Planning of the Open-Wedge High Tibial Osteotomy. Knee Surgery Sport. Traumatol. Arthrosc. 2015, 23, 846–851. [Google Scholar] [CrossRef]
- Elson, D.W.; Petheram, T.G.; Dawson, M.J. High Reliability in Digital Planning of Medial Opening Wedge High Tibial Osteotomy, Using Miniaci’s Method. Knee Surgery Sport. Traumatol. Arthrosc. 2015, 23, 2041–2048. [Google Scholar] [CrossRef] [PubMed]
- Miniaci, A.; Ballmer, F.T.; Ballmer, P.M.; Jakob, R.P. Proximal Tibial Osteotomy. A New Fixation Device. Clin. Orthop. Relat. Res. 1989, 246, 250–259. [Google Scholar]
- Dugdale, T.W.; Noyes, F.R.; Styer, D. Preoperative Planning for High Tibial Osteotomy: The Effect of Lateral Tibiofemoral Separation and Tibiofemoral Length. Clin. Orthop. Relat. Res. 1992, 248–264. [Google Scholar] [CrossRef]
- Blackburn, J.; Ansari, A.; Porteous, A.; Murray, J. Reliability of Two Techniques and Training Level of the Observer in Measuring the Correction Angle When Planning a High Tibial Osteotomy. Knee 2018, 25, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Sivertsen, E.A.; Vik, J.; Meland, A.S.V.; Nerhus, T.K. The Dugdale Planning Method for High Tibial Osteotomies Underestimates the Correction Angle Compared to the Miniaci Method. Knee Surgery Sport. Traumatol. Arthrosc. 2021. [Google Scholar] [CrossRef] [PubMed]
- Staubli, A.E.; De Simoni, C.; Babst, R.; Lobenhoffer, P. TomoFix: A New LCP-Concept for Open Wedge Osteotomy of the Medial Proximal Tibia—Early Results in 92 Cases. Injury 2003, 34, 3–10. [Google Scholar] [CrossRef]
- Staubli, A.E.; Jacob, H.A.C. Evolution of Open-Wedge High-Tibial Osteotomy: Experience with a Special Angular Stable Device for Internal Fixation without Interposition Material. Int. Orthop. 2010, 34, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Lobenhoffer, P.; Agneskirchner, J.D. Improvements in Surgical Technique of Valgus High Tibial Osteotomy. Knee Surgery Sport. Traumatol. Arthrosc. 2003, 11, 132–138. [Google Scholar] [CrossRef]
- Takeuchi, R.; Ishikawa, H.; Kumagai, K.; Yamaguchi, Y.; Chiba, N.; Akamatsu, Y.; Saito, T. Fractures around the Lateral Cortical Hinge after a Medial Opening-Wedge High Tibial Osteotomy: A New Classification of Lateral Hinge Fracture. Arthrosc. J. Arthrosc. Relat. Surg. 2012, 28, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Jacobi, M.; Wahl, P.; Jakob, R.P. Avoiding Intraoperative Complications in Open-Wedge High Tibial Valgus Osteotomy: Technical Advancement. Knee Surgery Sport. Traumatol. Arthrosc. 2010, 18, 200–203. [Google Scholar] [CrossRef] [PubMed]
- Vanadurongwan, B.; Siripisitsak, T.; Sudjai, N.; Harnroongroj, T. The Anatomical Safe Zone for Medial Opening Oblique Wedge High Tibial Osteotomy. Singap. Med. J. 2013, 54, 102–104. [Google Scholar] [CrossRef] [PubMed]
- Kessler, O.C.; Jacob, H.A.C.; Romero, J. Avoidance of Medial Cortical Fracture in High Tibial Osteotomy: Improved Technique. Clin. Orthop. Relat. Res. 2002, 395, 180–185. [Google Scholar] [CrossRef]
- Han, S.B.; Lee, D.H.; Shetty, G.M.; Chae, D.J.; Song, J.G.; Nha, K.W. A “Safe Zone” in Medial Open-Wedge High Tibia Osteotomy to Prevent Lateral Cortex Fracture. Knee Surgery Sport. Traumatol. Arthrosc. 2013, 21, 90–95. [Google Scholar] [CrossRef]
- Mihalko, W.M.; Krackow, K.A. Preoperative Planning for Lower Extremity Osteotomies: An Analysis Using 4 Different Methods and 3 Different Osteotomy Techniques. J. Arthroplasty 2001, 16, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Hernigou, P. Open Wedge Tibial Osteotomy: Combined Coronal and Sagittal Correction. Knee 2002, 9, 15–20. [Google Scholar] [CrossRef]
- Nelissen, E.M.; Van Langelaan, E.J.; Nelissen, R.G.H.H. Stability of Medial Opening Wedge High Tibial Osteotomy: A Failure Analysis. Int. Orthop. 2010, 34, 217–223. [Google Scholar] [CrossRef] [PubMed]
- van de Pol, G.J.; Verdonschot, N.; van Kampen, A. The Value of the Intra-Operative Clinical Mechanical Axis Measurement in Open-Wedge Valgus High Tibial Osteotomies. Knee 2012, 19, 933–938. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Mean Wedge Width (mm) | SD | |
|---|---|---|
| 3 cm-A | 8.9 | ±3.9 |
| 3 cm-B | 10.3 | ±4.2 |
| 3 cm-C | 11.6 | ±4.4 |
| 4 cm-A | 9 | ±3.8 |
| 4 cm-B | 10.2 | ±4.1 |
| 4 cm-C | 11.4 | ±4.2 |
| plateau width (mm) | 79.5 | ±6.9 |
| femoral length (mm) | 475.0 | ±34.5 |
| tibial length (mm) | 372.6 | ±30.2 |
| Varus (°) | Frequency (n = 55) | Percent (%) |
|---|---|---|
| 3.00 | 15 | 27.3 |
| 4.00 | 10 | 18.2 |
| 5.00 | 4 | 7.3 |
| 6.00 | 8 | 14.5 |
| 7.00 | 2 | 3.6 |
| 8.00 | 5 | 9.1 |
| 9.00 | 6 | 10.9 |
| 12.00 | 3 | 5.5 |
| 13.00 | 1 | 1.8 |
| 17.00 | 1 | 1.8 |
| Observers | Rater 1 ICC (95% CI) | Rater 2 ICC (95% CI) | R1 vs R2 ICC (95% CI) |
|---|---|---|---|
| mFTA | 0.988 (0.972–0.995) | 0.988 (0.972–0.995) | 0.988 (0.972–0.995) |
| 3 cm-A | 0.990 (0.975–0.996) | 0.990 (0.977–0.996) | 0.979 (0.954–0.991) |
| 3 cm-B | 0.995 (0.990–0.998) | 0.994 (0.986–0.997) | 0.990 (0.976–0.995) |
| 3 cm-C | 0.996 (0.991–0.998) | 0.992 (0.982–0.997) | 0.988 (0.972–0.995) |
| 4 cm-A | 0.993 (0.983–0.997) | 0.994 (0.968–0.998) | 0.988 (0.864–0.997) |
| 4 cm-B | 0.996 (0.990–0.998) | 0.995 (0.983–0.998) | 0.991 (0.943–0.997) |
| 4 cm-C | 0.994 (0.984–0.997) | 0.992 (0.979–0.997) | 0.985 (0.942–0.995) |
| plateau width | 0.994 (0.979–0.998) | 0.955 (0.894–0.980) | 0.949 (0.843–0.981) |
| femoral length | 0.998 (0.996–0.999) | 0.998 (0.993–0.999) | 0.997 (0.981–0.999) |
| tibial length | 0.996 (0.991–0.998) | 0.830 (0.651–0.922) | 0.827 (0.644–0.921) |
| Compared Groups | Difference of Mean (mm) | p | Rate ≥ 2 m (%) |
|---|---|---|---|
| 3 cm-A vs. 3 cm-B | 1.325 | 0.534 | 9% |
| 3 cm-B vs. 3 cm-C | 1.285 | 0.568 | 7% |
| 3 cm-A vs. 3 cm-C | 2.611 | 0.012 * | 91% |
| 4 cm-A vs. 4 cm-B | 1.216 | 0.626 | 4% |
| 4 cm-B vs. 4 cm-C | 1.198 | 0.641 | 2% |
| 4 cm-A vs. 4 cm-C | 2.415 | 0.026 * | 82% |
| 3 cm-A vs. 4 cm-A | 0.009 | 1.000 | 0% |
| 3 cm-A vs. 4 cm-B | 1.225 | 0.619 | 7% |
| 3 cm-A vs. 4 cm-C | 2.424 | 0.025 * | 78% |
| 3 cm-B vs. 4 cm-A | 1.316 | 0.541 | 7% |
| 3 cm-B vs. 4 cm-B | 0.100 | 1.000 | 0% |
| 3 cm-B vs. 4 cm-C | 1.098 | 0.722 | 0% |
| 3 cm-C vs. 4 cm-A | 2.601 | 0.012 * | 80% |
| 3 cm-C vs. 4 cm-B | 1.385 | 0.483 | 16% |
| 3 cm-C vs. 4 cm-C | 0.187 | 1.000 | 0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thürig, G.; Korthaus, A.; Frings, J.; Berninger, M.T.; Frosch, K.-H.; Krause, M. Influence of Medial Osteotomy Height and Hinge Position in Open Wedge High Tibial Osteotomy: A Simulation Study. Diagnostics 2022, 12, 2546. https://doi.org/10.3390/diagnostics12102546
Thürig G, Korthaus A, Frings J, Berninger MT, Frosch K-H, Krause M. Influence of Medial Osteotomy Height and Hinge Position in Open Wedge High Tibial Osteotomy: A Simulation Study. Diagnostics. 2022; 12(10):2546. https://doi.org/10.3390/diagnostics12102546
Chicago/Turabian StyleThürig, Grégoire, Alexander Korthaus, Jannik Frings, Markus Thomas Berninger, Karl-Heinz Frosch, and Matthias Krause. 2022. "Influence of Medial Osteotomy Height and Hinge Position in Open Wedge High Tibial Osteotomy: A Simulation Study" Diagnostics 12, no. 10: 2546. https://doi.org/10.3390/diagnostics12102546
APA StyleThürig, G., Korthaus, A., Frings, J., Berninger, M. T., Frosch, K.-H., & Krause, M. (2022). Influence of Medial Osteotomy Height and Hinge Position in Open Wedge High Tibial Osteotomy: A Simulation Study. Diagnostics, 12(10), 2546. https://doi.org/10.3390/diagnostics12102546