
Energy, Waves, and Forces in Bilateral Fracture of the Femoral Necks: Two Case Presentations and Updated Critical Review

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Presentation
3. Discussion
4. Conclusions
- (a)
- a clinical and paraclinical examination; history of the fracture as told and remembered by the patient; history of comorbidities and their respective treatments; and continuity of medication in cases such as diabetes, dialysis, heart disease, and others of the chronic kind.
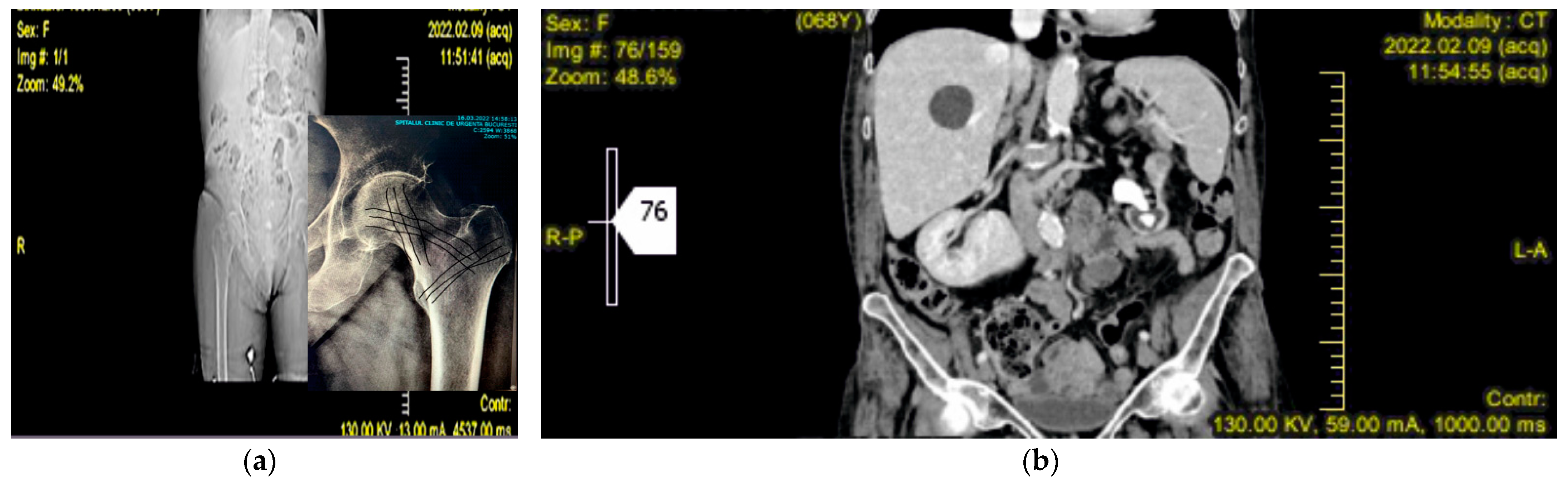
- (b)
- imaging and spectral techniques in support of primary X-ray radiographs, to get a more precise picture of the case and diagnostic.
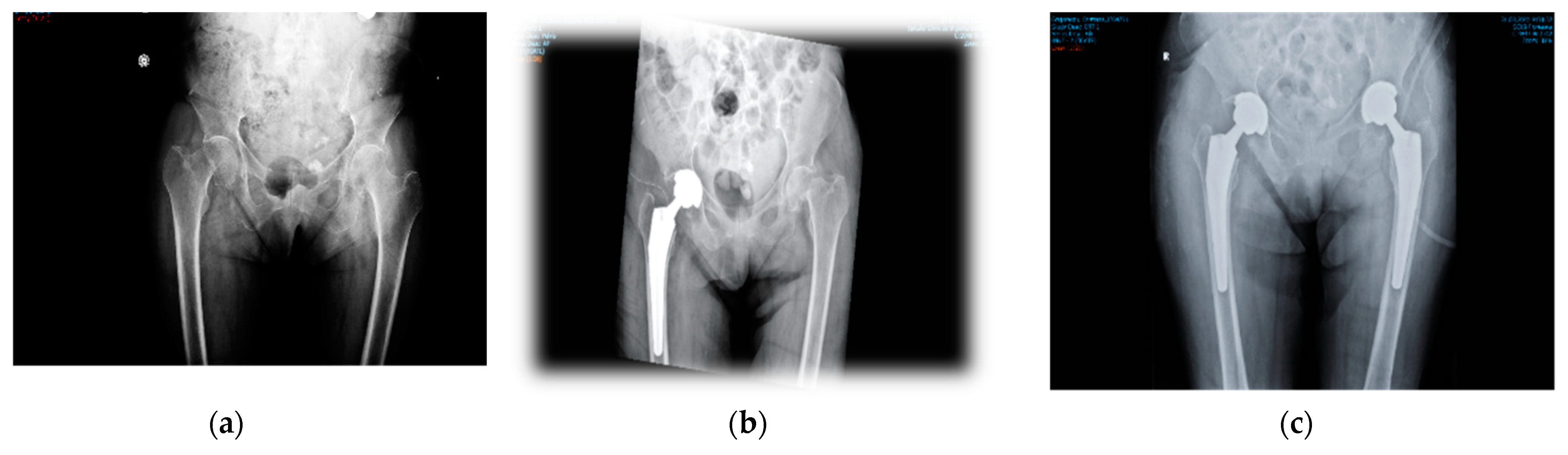
- (c)
- surgery and appropriate manipulation and fixation of the bones, using the most suitable devices (screws, cables, cement/non-cement prostheses, etc.).
- (d)
- post-surgery care, according to the evolution of the patient.
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gupta, A.K.; Narang, A.; Gupta, S.; Rajesh, K. Bilateral Neck of Femur Fracture in a Child With Underlying Vitamin D Deficiency: A Case Report on Management and 10-Year Follow-Up. Cureus 2022, 14, e22953. [Google Scholar] [CrossRef] [PubMed]
- Upadhyay, A.; Maini, L.; Batra, S.; Mishra, P.; Jain, P. Simultaneous bilateral fractures of femoral neck in children: Mechanism of injury. Injury 2004, 35, 1073–1075. [Google Scholar] [CrossRef]
- Palocaren, T. Femoral neck fractures in children: A review. Indian J. Orthop. 2018, 52, 501–506. [Google Scholar] [CrossRef] [PubMed]
- Yoon, B.H.; Kwon, M.S. Atraumatic bilateral fracture of the femoral neck in young male patient with suspected osteomalacia. J. Bone Metab. 2017, 24, 197–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadiq, M.; Kulkarni, V.; Hussain, S.A.; Ismail, M.; Nayak, M. Low-velocity simultaneous bilateral femoral neck fracture following long-term antiepileptic therapy: A case report. World J. Orthop. 2019, 10, 371–377. [Google Scholar] [CrossRef]
- Alkaramani, E.; Salameh, M.; Adam, M.; George, B.; Alser, Y.; Ahmed, G. Simultaneous bilateral neck of femur fracture in a young adult with underlying metabolic disturbances. Case Rep. Orthop. 2020, 2020, 8972542. [Google Scholar] [CrossRef] [Green Version]
- Cohen, I.; Melamed, E.; Lipkin, A.; Robinson, D. Transient osteoporosis of pregnancy complicated by a pathologic subcapital hip fracture. J. Trauma 2007, 62, 1281–1283. [Google Scholar] [CrossRef]
- Chowdhury, F.U.; Robinson, P.; Grainger, A.J.; Harris, N. Transient regional osteoporosis: A rare cause of foot and ankle pain. Foot Ankle Surg. 2006, 12, 79–83. [Google Scholar] [CrossRef]
- Debnath, U.K.; Kishore, R.; Black, R.J. Isolated acetabular osteoporosis in TOH in pregnancy: A case report. South Med. J. 2005, 98, 1146–1148. [Google Scholar] [CrossRef]
- Ofluoglu, O.; Ofluoglu, D. A case report: Pregnancy-induced severe osteoporosis with eight vertebral fractures. Rheumatol. Int. 2008, 29, 197–201. [Google Scholar] [CrossRef]
- Lloyd, J.M.; Lewis, M.; Jones, A. Transient osteoporosis of the knee in pregnancy. J. Knee Surg. 2006, 19, 121–123. [Google Scholar] [CrossRef] [PubMed]
- Ma, F.Y.; Falkenberg, M. Case reports: Transient osteoporosis of the hip: An atypical case. Clin. Orthop. Relat. Res. 2006, 445, 245–249. [Google Scholar] [CrossRef] [PubMed]
- Pai, W.C.; Lin, C.Y.; Kao, M.J.; Lin, F.C. Transient osteoporosis of the hip during pregnancy: A case report. Taiwan J. Phys. Med. Rehabil. 2009, 37, 131–137. [Google Scholar]
- Sahan, I.; de Deken, J.; Anagnostakos, K. Bilateral Femoral Neck Fracture in a Postpartum Woman: Beware of the Risk Factors. Hindawi Case Rep. Orthop. 2019, 2019, 4134351. [Google Scholar] [CrossRef] [Green Version]
- Tan, X.-Y.; Lei, T.; Wu, G.B.; Luo, H.E.; Huang, G.; He, C.Y.; Lu, M.; Lei, P.F. Successful treatment for bilateral femoral neck insufficiency fractures: A rare lesion case report and an updated review of the literature. BMC Musculoskelet. Disord. 2020, 21, 102. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, T.J.; Cole, P.A. Pelvic, Insufficiency fractures. Geriatr. Orthop. Surg. Rehabil. 2014, 5, 178–190. [Google Scholar] [CrossRef]
- Vijayvargiya, M.; Shetty, V.; Makwana, K.; Agarwal, N. Bilateral simultaneous neck femur fracture following domestic fall in an elderly patient: A rare case report. Rev. Bras. Ortop. 2017, 52, 363–365. [Google Scholar] [CrossRef]
- Powell, H.D.W. Dw Powell Simultaneous Bilateral Fractures of the Neck of the Femur. J. Bone Jt. Surg. 1960, 42B, 2. [Google Scholar]
- Gao, Y.-S.; Zhu, Z.-H.; Zhang, C.-Q. Simultaneous bilateral fractures of the femoral neck caused by high energy: A case report and literature review. Chin. J. Traumatol. 2015, 18, 304–306. [Google Scholar] [CrossRef]
- Farouk, O.; Mahran, D.G.; Said, H.G.; Alaa, M.M.; Eisa, A.A.; Said, G.Z.; Rashed, H.; Ez-Eldeen, A. Hypovitaminosis D Among Patients Admitted With Hip Fracture to a Level-1 Trauma Center in the Sunny Upper Egypt: Prevalence and Associated Correlates. Geriatr. Orthop. Surg. Rehabil. 2016, 7, 148–152. [Google Scholar] [CrossRef] [Green Version]
- Fujita, S.; Morihara, T.; Arai, Y.; Chatani, K.; Takahashi, K.A.; Fujiwara, H.; Mikihiro, F.; Toshikazu, K. Absence of osteonecrosis of the femoral head following, the high degree of bilateral femoral neck fracture with displacement. J. Orthop. Sci. 2006, 11, 628–631. [Google Scholar] [CrossRef] [PubMed]
- Madho, R.; Rand, J.A. Ten-year follow-up study of missed, simultaneous, bilateral femoral-neck fractures treated by bipolar arthroplasties in a patient with chronic renal failure. Clin. Orthop. Relat. Res. 1993, 291, 185–187. [Google Scholar]
- Gur, S.; Yilmaz, H.; Tüzüner, S.; Aydin, A.T.; Süleymanlar, G. Fractures due to hypocalcemic convulsion. Int. Orthop. 1999, 23, 308–309. [Google Scholar]
- Haddad, F.S.; Bann, S.; Hill, R.A.; Jones, D.H.A. Displaced stress fracture of the femoral neck in an active amenorrhoeic adolescent. Brit. J. Sports Med. 1997, 31, 70–75. [Google Scholar] [CrossRef]
- Taylor, L.J.; Grant, S.C. Hipocalcemic bilateral fracture of the femoral neck during a convulsion. J. Bone Jt. Surg. Br. 1985, 67B, 536–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devas, M.B. Stress fracture of the femoral neck. J. Bone Jt. Surg. Br. 1965, 47B, 728–738. [Google Scholar] [CrossRef]
- Rengman, E. Fatigue fractures of the lower extremities: One of bilateral cases of bilateral fatigue fracture of the collum femoris. Acta Orthop. 1959, 29, 43–48. [Google Scholar] [CrossRef]
- Alison, S.-I. An Investigation of Shock Wave Propagation and Attenuation in the Lower Extremity Using Finite Element Analysis. Master’s Thesis, University of Windsor, Windsor, ON, Canada, 2010. ISBN: 978-0-494-70588-9. Available online: https://scholar.uwindsor.ca/etd/7173 (accessed on 23 June 2022).
- Wildstein, M.S. Femoral Neck Stress and Insufficiency Fractures. Available online: http://emedicine.medscape.com/article/1246691-overview#a4 (accessed on 10 July 2022).
- Web, M.D. Understanding Bone Fractures—The Basics. 2014. Available online: http://www.webmd.com/a-to-z-guides/understanding-fractures-basic-information (accessed on 12 August 2022).
- Bohiltea, R.; Ducu, I.; Mihai, B.; Iordache, A.-M.; Dorobat, B.; Vladareanu, E.M.; Iordache, S.-M.; Bohiltea, A.-T.; Bacalbasa, N.; Grigorescu, C.E.A.; et al. Uterine Artery Embolization Combined with Subsequent Suction Evacuation as Low-Risk Treatment for Cesarean Scar Pregnancy. Diagnostics 2021, 11, 2350. [Google Scholar] [CrossRef]
- Bohîltea, R.E.; Dima, V.; Ducu, I.; Iordache, A.M.; Mihai, B.M.; Munteanu, O.; Grigoriu, C.; Veduta, A.; Pelinescu-Onciul, D.; Vladareanu, R. Clinically Relevant Prenatal Ultra-sound Diagnosis of Umbilical Cord Pathology. Diagnostics 2022, 12, 236. [Google Scholar] [CrossRef]
- Bohiltea, R.E.; Varlas, V.-N.; Dima, V.; Iordache, A.-M.; Salmen, T.; Mihai, B.-M.; Bohiltea, A.T.; Vladareanu, E.M.; Ducu, I.; Grigoriu, C. The Strategy against Iatrogenic Prematurity Due to True Umbilical Knot: From Prenatal Diagnosis Challenges to the Favorable Fetal Outcome. J. Clin. Med. 2022, 11, 818. [Google Scholar] [CrossRef]
- Zhu, Y.; Hu, J.; Han, W.; Lu, J.; Zeng, Y. Simultaneous bilateral femoral neck fractures in a dialysis-dependent patient: Case report and literature review. BMC Musculoskelet. Disord. 2020, 21, 242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karapinar, H.; Ozdemir, M.; Akyol, S.; Ulku, O. Spontaneous bilateral femoral neck fractures in a young adult with chronic renal failure. Acta Orthop. Belg. 2003, 69, 82–85. [Google Scholar]
- Alem, A.M.; Sherrard, D.J.; Gillen, D.L.; Weiss, N.S.; Beresford, S.A.; Heckbert, S.R.; Wong, C.; Stehman-Breen, C. Increased risk of hip fracture among patients with end-stage renal disease. Kidney Int. 2000, 58, 396–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nair, S.S.; Mitani, A.A.; Goldstein, B.A.; Chertow, G.M.; Lowenberg, D.W.; Winkelmayer, W.C. Temporal Trends in the Incidence, Treatment, and Outcomes of Hip Fracture in Older Patients Initiating Dialysis in the United States. Clin. J. Am. Soc. Nephrol. 2013, 8, 1336–1342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarvi, M.N.; Luo, Y. Sideways fall-induced impact force and its effect on hip fracture risk: A review. Osteoporos. Int. 2017, 28, 2759–2780. [Google Scholar] [CrossRef]
- Shahabpoor, E.; Pavic, A. Human-Structure Dynamic Interaction during Short-Distance Free Falls. Shock. Vib. 2016, 2016, 2108676. [Google Scholar] [CrossRef] [Green Version]
- Nam, J.; Chee, W.; Kim, K. Identification of Falling Human Body Dynamics. In Proceedings of the 2003 American Control Conference, Denver, CO, USA, 4–6 June 2003. [Google Scholar]
- Yassin, A.; Jawad, I.; Coomber, R.; Gonzalez-Castro, A. Non-traumatic, bilateral subcapital femoral fractures postpartum. BMJ Case Rep. 2014, 2014, bcr2013201625. [Google Scholar] [CrossRef] [Green Version]
- Arisumi, S.; Mawatari, T.; Ikemura, S.; Matsui, G.; Iguchi, T.; Mitsuyasu, H. Spontaneous bilateral femoral neck fractures in a young male adult: A case report and literature review. BMC Musculoskelet. Disord. 2019, 20, 449. [Google Scholar] [CrossRef] [Green Version]
- Sood, A.; Rao, C.; Holloway, I. Bilateral femoral neck fractures in an adult male following minimal trauma after a simple mechanical fall: A case report. Cases J. 2009, 2, 92. [Google Scholar] [CrossRef] [Green Version]
- Park, J.H.; Jeong, H.-J.; Shin, H.-K.; Kim, E.; Ko, T.S.; Choi, Y.M. Bilateral Fracture of Femoral Neck in Korea: A Case Report. Hip Pelvis 2015, 27, 53–56. [Google Scholar] [CrossRef] [Green Version]
- Boog, P.; Keizer, S.B.; Bregje, J.W. Thomassen, An unexpected cause of bilateral femoral neck fractures. Curr. Orthop. Pract. 2012, 23, 634–636. [Google Scholar] [CrossRef]
- Khosla, S.; Amin, S.; Orwoll, E. Osteoporosis in men. Endocr. Rev. 2008, 29, 441–464. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baciu, C.C. Energy, Waves, and Forces in Bilateral Fracture of the Femoral Necks: Two Case Presentations and Updated Critical Review. Diagnostics 2022, 12, 2592. https://doi.org/10.3390/diagnostics12112592
Baciu CC. Energy, Waves, and Forces in Bilateral Fracture of the Femoral Necks: Two Case Presentations and Updated Critical Review. Diagnostics. 2022; 12(11):2592. https://doi.org/10.3390/diagnostics12112592
Chicago/Turabian StyleBaciu, Cosmin Constantin. 2022. "Energy, Waves, and Forces in Bilateral Fracture of the Femoral Necks: Two Case Presentations and Updated Critical Review" Diagnostics 12, no. 11: 2592. https://doi.org/10.3390/diagnostics12112592