
Dedicated CCTA Followed by High-Pitch Scanning versus TRO-CT for Contrast Media and Radiation Dose Reduction: A Retrospective Study

 and
and
Abstract
1. Introduction
2. Methods
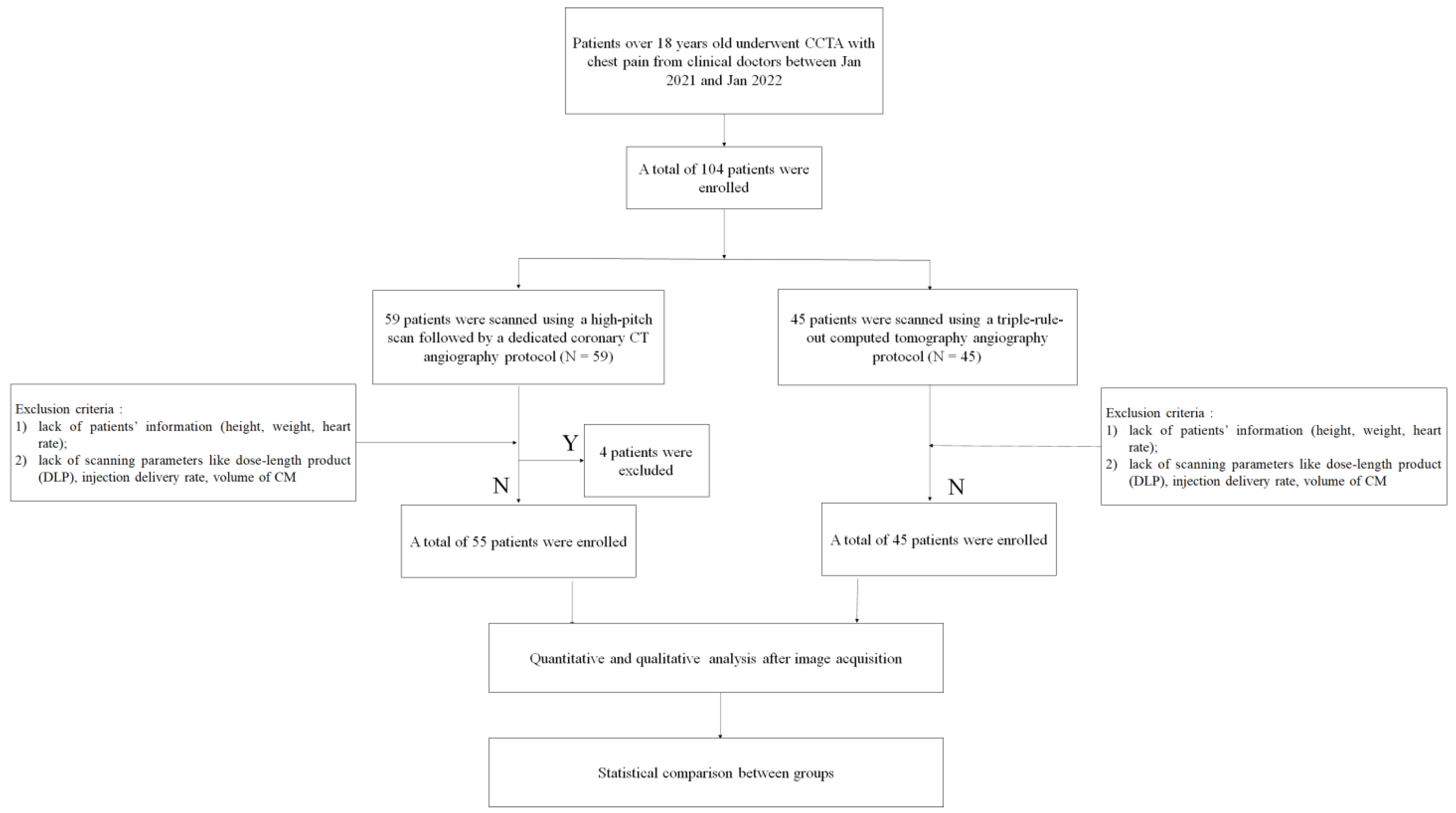
2.1. Patient Population
2.2. Image Acquisition
2.3. Image Reconstruction and Evaluation
2.4. Radiation Dose
2.5. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Abbreviation | Meaning |
| TRO-CTA | Triple-Rule-Out Computed Tomography Angiography |
| CM | Contrast Media |
| CCTA | Coronary Computed Tomography Angiography |
| PA | Pulmonary Artery |
| TA | Thoracic Aorta |
| CA | Coronary Artery |
| PE | Pulmonary Embolism |
| AD | Aortic Dissection |
| ACS | Acute Coronary Syndrome |
| DLP | Dose-Length Product |
| CS | Calcium Score |
| ATVS | Automatic tube voltage selection |
| SD | Standard Deviation |
| PT | Pulmonary Trunk |
| LPA | Left Pulmonary Artery |
| RPA | Right Pulmonary Artery |
| AO | Aortic Root |
| AA | Aortic Arch |
| DA | Descending Aorta |
| LMCA-P | Proximal Left Main Coronary Artery |
| LAD-M | Middle Left Anterior Descending |
| LAD-D | Distal Left Anterior Descending |
| LCX-M | Middle Left Circumflex |
| LCX-D | Distal Left Circumflex |
| RCA-P | Proximal Right Coronary Artery |
| RCA-M | Middle Right Coronary Artery |
| RCA-D | Distal Coronary Right Artery |
| ESM | Erector Spinae Muscle |
| PVAT | Perivascular Adipose Tissue |
| SNR | Signal-to-Noise Ratio |
| CNR | Contrast-to-Noise Ratio |
| CTDIvol | CT dose index |
| ED | Effective Dose |
References
- Raff, G.L.; Hoffmann, U.; Udelson, J.E. Trials of imaging use in the emergency Department for Acute Chest Pain. JACC Cardiovasc. Imaging 2017, 10, 338–349. [Google Scholar] [CrossRef]
- Russo, V.; Sportoletti, C.; Scalas, G.; Attinà, D.; Buia, F.; Niro, F.; Modolon, C.; De Luca, C.; Monteduro, F.; Lovato, L. The triple rule out CT in acute chest pain: A challenge for emergency radiologists? Emerg. Radiol. 2021, 28, 735–742. [Google Scholar] [CrossRef]
- Chae, M.K.; Kim, E.K.; Jung, K.Y.; Shin, T.G.; Sim, M.S.; Jo, I.J.; Song, K.J.; Chang, S.A.; Song, Y.B.; Hahn, J.Y.; et al. Triple rule-out computed tomography for risk stratification of patients with acute chest pain. J. Cardiovasc. Comput. Tomogr. 2016, 10, 291–300. [Google Scholar] [CrossRef]
- DeLaney, M.C.; Neth, M.; Thomas, J.J. Chest pain triage: Current trends in the emergency departments in the United States. J. Nucl. Cardiol. 2017, 24, 2004–2011. [Google Scholar] [CrossRef]
- Hollander, J.E.; Chang, A.M. Triple rule out CTA scans or the right test for the right patient. JACC Cardiovasc. Imaging 2015, 8, 826–827. [Google Scholar] [CrossRef]
- Burris, A.C., 2nd; Boura, J.A.; Raff, G.L.; Chinnaiyan, K.M. Triple rule out versus coronary CT angiography in patients with acute chest pain: Results from the ACIC consortium. JACC Cardiovasc. Imaging 2015, 8, 817–825. [Google Scholar] [CrossRef]
- Ketelsen, D.; Luetkhoff, M.H.; Thomas, C.; Werner, M.; Buchgeister, M.; Tsiflikas, I.; Reimann, A.; Burgstahler, C.; Kopp, A.F.; Claussen, C.D.; et al. Estimation of the radiation exposure of a chest pain protocol with ECG-gating in dual-source computed tomography. Eur. Radiol. 2009, 19, 37–41. [Google Scholar] [CrossRef]
- Nguyen, P.K.; Lee, W.H.; Li, Y.F.; Hong, W.X.; Hu, S.; Chan, C.; Liang, G.; Nguyen, I.; Ong, S.G.; Churko, J.; et al. Assessment of the radiation effects of cardiac CT angiography using protein and genetic biomarkers. JACC Cardiovasc. Imaging 2015, 8, 873–884. [Google Scholar] [CrossRef]
- Si-Mohamed, S.; Greffier, J.; Bobbia, X.; Larbi, A.; Delicque, J.; Khasanova, E.; Beregi, J.P.; Macri, F. Diagnostic performance of a low dose triple rule-out CT angiography using SAFIRE in emergency department. Diagn. Interv. Imaging 2017, 98, 881–891. [Google Scholar] [CrossRef]
- Takx, R.A.P.; Krissak, R.; Fink, C.; Bachmann, V.; Henzler, T.; Meyer, M.; Nance, J.W.; Schoenberg, S.O.; Apfaltrer, P. Low-tube-voltage selection for triple-rule-out CTA: Relation to patient size. Eur. Radiol. 2017, 27, 2292–2297. [Google Scholar] [CrossRef]
- Gruettner, J.; Fink, C.; Walter, T.; Meyer, M.; Apfaltrer, P.; Schoepf, U.J.; Saur, J.; Sueselbeck, T.; Traunwieser, D.; Takx, R.; et al. Coronary computed tomography and triple rule out CT in patients with acute chest pain and an intermediate cardiac risk profile. Part 1: Impact on patient management. Eur. J. Radiol. 2013, 82, 100–105. [Google Scholar] [CrossRef]
- Wong, D.T.; Soh, S.Y.; Ko, B.S.; Cameron, J.D.; Crossett, M.; Nasis, A.; Troupis, J.; Meredith, I.T.; Seneviratne, S.K. Superior CT coronary angiography image quality at lower radiation exposure with second generation 320-detector row CT in patients with elevated heart rate: A comparison with first generation 320-detector row CT. Cardiovasc. Diagn. Ther. 2014, 4, 299–306. [Google Scholar] [CrossRef]
- Chen, Y.; Wang, Q.; Li, J.; Jia, Y.; Yang, Q.; He, T. Triple-rule-out CT angiography using two axial scans with 16 cm wide-detector for radiation dose reduction. Eur. Radiol. 2018, 28, 4654–4661. [Google Scholar] [CrossRef]
- Ripley, D.P.; Uddin, A.; Greenwood, J.P. Greenwood, CT triple rule-out examination: Higher radiation dose without clinical benefit. BMJ 2013, 347, f5118. [Google Scholar] [CrossRef]
- Jin, L.; Gao, Y.; Shan, Y.; Sun, Y.; Li, M.; Wang, Z. Qualitative and quantitative image analysis of 16 cm wide-coverage computed tomography compared to new-generation dual-source CT. J. Xray Sci. Technol. 2020, 28, 527–539. [Google Scholar] [CrossRef]
- Jin, L.; Jie, B.; Gao, Y.; Jiang, A.; Weng, T.; Li, M. Low dose contrast media in step-and-shoot coronary angiography with third-generation dual-source computed tomography: Feasibility of using 30 mL of contrast media in patients with body surface area <1.7 m2. Quant. Imaging Med. Surg. 2021, 11, 2598–2609. [Google Scholar] [CrossRef]
- Jin, L.; Gao, Y.; Sun, Y.; Li, C.; Gao, P.; Zhao, W.; Li, M. Contrast medium administration with a body surface area protocol in step-and-shoot coronary computed tomography angiography with dual-source scanners. Sci. Rep. 2020, 10, 16690. [Google Scholar] [CrossRef]
- Hou, D.J.; Tso, D.K.; Davison, C.; Inacio, J.; Louis, L.J.; Nicolaou, S.; Reimann, A.J. Clinical utility of ultra high pitch dual source thoracic CT imaging of acute pulmonary embolism in the emergency department: Are we one step closer towards a non-gated triple rule out? Eur. J. Radiol. 2013, 82, 1793–1798. [Google Scholar] [CrossRef]
- Lu, G.M.; Luo, S.; Meinel, F.G.; McQuiston, A.D.; Zhou, C.S.; Kong, X.; Zhao, Y.E.; Zheng, L.; Schoepf, U.J.; Zhang, L.J. High-pitch computed tomography pulmonary angiography with iterative reconstruction at 80 kVp and 20 mL contrast agent volume. Eur. Radiol. 2014, 24, 3260–3268. [Google Scholar] [CrossRef]
- Spearman, J.V.; Schoepf, U.J.; Rottenkolber, M.; Driesser, I.; Canstein, C.; Thierfelder, K.M.; Krazinski, A.W.; De Cecco, C.N.; Meinel, F.G. Effect of automated attenuation-based tube voltage selection on radiation dose at CT: An observational study on a global scale. Radiology 2016, 279, 167–174. [Google Scholar] [CrossRef]
- Mangold, S.; Wichmann, J.L.; Schoepf, U.J.; Poole, Z.B.; Canstein, C.; Varga-Szemes, A.; Caruso, D.; Bamberg, F.; Nikolaou, K.; De Cecco, C.N. Automated tube voltage selection for radiation dose and contrast medium reduction at coronary CT angiography using 3(rd) generation dual-source CT. Eur. Radiol. 2016, 26, 3608–3616. [Google Scholar] [CrossRef] [PubMed]
- Vonder, M.; Pelgrim, G.J.; Huijsse, S.E.; Meyer, M.; Greuter, M.J.; Henzler, T.; Flohr, T.G.; Oudkerk, M.; Vliegenthart, R. Feasibility of spectral shaping for detection and quantification of coronary calcifications in ultra-low dose CT. Eur. Radiol. 2017, 27, 2047–2054. [Google Scholar] [CrossRef] [PubMed]
- Tesche, C.; De Cecco, C.N.; Schoepf, U.J.; Duguay, T.M.; Albrecht, M.H.; Caruso, D.; Varga-Szemes, A.; Lesslie, V.W.; Ebersberger, U.; Canstein, C.; et al. Iterative beam-hardening correction with advanced modeled iterative reconstruction in low voltage CT coronary calcium scoring with tin filtration: Impact on coronary artery calcium quantification and image quality. J. Cardiovasc. Comput. Tomogr. 2017, 11, 354–359. [Google Scholar] [CrossRef]
- Wichmann, J.L.; Katzberg, R.W.; Litwin, S.E.; Zwerner, P.L.; De Cecco, C.N.; Vogl, T.J.; Costello, P.; Schoepf, U.J. Contrast-induced nephropathy. Circulation 2015, 132, 1931–1936. [Google Scholar] [CrossRef] [PubMed]
- Halpern, E.J. Triple-rule-out CT angiography for evaluation of acute chest pain and possible acute coronary syndrome. Radiology 2009, 252, 332–345. [Google Scholar] [CrossRef]
- Abbara, S.; Blanke, P.; Maroules, C.D.; Cheezum, M.; Choi, A.D.; Han, B.K.; Marwan, M.; Naoum, C.; Norgaard, B.L.; Rubinshtein, R.; et al. SCCT guidelines for the performance and acquisition of coronary computed tomographic angiography: A report of the society of cardiovascular Computed Tomography Guidelines Committee: Endorsed by the North American Society for Cardiovascular Imaging (NASCI). J. Cardiovasc. Comput. Tomogr. 2016, 10, 435–449. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Group A | Group B | ||||
|---|---|---|---|---|---|
| CS | CCTA | High-Pitch1 | High-Pitch2 | ||
| Sn100 kV | 55 | 0 | 0 | 0 | 0 |
| 120 kV | 0 | 2 | 3 | 1 | 1 |
| 110 kV | 0 | 3 | 2 | 1 | 4 |
| 100 kV | 0 | 9 | 4 | 0 | 9 |
| 90 kV | 0 | 41 | 15 | 2 | 31 |
| 80 kV | 0 | 0 | 31 | 8 | 0 |
| Parameters | Group A | Group B | p |
|---|---|---|---|
| CTDIvol (mGy) | 0.70 ± 0.38 (for CA) 18.75 ± 12.95 (for CCTA) 2.54 ± 1.56 (for high-pitch scan) | 20.42 ± 9.60 | 0.516 |
| DLP (mGy-cm) | 8.81 ± 4.15 (for CA) 179.50 ± 94.48 (for CCTA) 79.86 ± 51.70 (for high-pitch scan) | 525.28 ± 240.12 | <0.001 |
| ED (mSv) | 0.23 ± 0.11 (for CA ∗ 0.026) 4.67 ± 2.46 (for CCTA ∗ 0.026) 1.36 ± 0.88 (for high-pitch scan ∗ 0.017) | 8.93 ± 4.08 (∗0.017) | |
| Total ED (mSv) | 6.25 ± 2.94 | 8.93 ± 4.08 | <0.001 |
| Delivery rate CM | 3.90 ± 0.67 (for CCTA) | 4.50 ± 0 (for first phase) | NA |
| 4.00 ± 0 (for high-pitch scan) | 4.00 ± 0 (for second phase) | NA | |
| Delivery rate Sa | 3.90 ± 0.67 (for CCTA) | 3.50 ± 0 | NA |
| 4.00 ± 0 (for high-pitch scan) | |||
| Contrast media (mL) | 75.7 ± 8.9 | 95.0 ± 0 | <0.001 |
| Saline (mL) | 79.0 ± 6.7 | 30.0 ± 0 | <0.001 |
| Criteria | Group A (n = 55) | Group B (n = 45) | p |
|---|---|---|---|
| Baseline characteristics | |||
| Female (%) | 30 (54.5%) | 21 (46.7%) | 0.433 |
| Age (years) | 66.6 ± 13.1 (23–91) | 62.3 ± 10.6 (30–83) | 0.076 |
| Body mass index (kg/m2) | 23.61 ± 3.18 (16.26–30.70) | 24.35 ± 3.43 (17.29–31.85) | 0.268 |
| Heart rate (bpm) | 73 ± 10 (51–92) | 70 ± 10 (50–100) | 0.173 |
| Clinical outcomes | |||
| Pulmonary embolism | 0 | 0 | |
| Aortic enlargement | 0 | 3 | |
| Pneumonia | 5 | 3 | |
| Aortic dissection | 0 | 0 | |
| Atherosclerotic ulcer | 34 | 28 | |
| Coronary artery stenosis | 24 | 20 | |
| Myocardial bridge | 18 | 21 | |
| Anomalous coronary artery | 3 | 0 | |
| PCI | 3 | 2 | |
| Criteria | Group A (n = 55) | Group B (n = 45) | p |
|---|---|---|---|
| Attenuation values (HU) | |||
| PT | 346.95 (263.61, 476.55) | 497.10 (391.98, 581.58) | <0.001 |
| LPA | 337.95 (256.95, 470.63) | 470.84 (368.34, 535.67) | <0.001 |
| RPA | 357.14 (260.91, 471.70) | 457.31 (359.58, 580.03) | <0.001 |
| AO | 321.67 (251.66, 385.13) | 499.37 (418.23, 553.13) | <0.001 |
| AA | 300.62 (238.69, 375.24) | 532.42 (456.91, 572.67) | <0.001 |
| DA | 262.38 (220.86, 359.63) | 504.71 (440.26, 564.55) | <0.001 |
| LMCA-P | 441.50 (391.40, 501.11) | 504.75 (443.31, 568.06) | 0.001 |
| LAD-M | 376.92 (320.38, 434.67) | 358.86 (288.77, 439.29) | 0.201 |
| LAD-D | 305.88 (255.40, 363.30) | 188.64 (147.35, 268.69) | <0.001 |
| LCX-M | 383.33 (329.55, 448.17) | 399.47 (309.85, 485.99) | 0.577 |
| LCX-D | 329.21 (255.27, 372.67) | 260.50 (199.00, 305.05) | 0.001 |
| RCA-P | 451.86 (395.00,510.20) | 506.67 (417.81, 555.14) | 0.040 |
| RCA-M | 469.92 (385.50,535.30) | 471.45 (379.58, 529.00) | 0.898 |
| RCA-D | 430.67 (350.15, 492.70) | 454.19 (377.26, 526.09) | 0.194 |
| ESM | 67.25 (57.33, 74.89) | 50.83 (35.62, 57.98) | <0.001 |
| PVAT | −107.30 (−116.45, −97.60) | −104.54 (−106.66, −100.60) | 0.091 |
| Image noise | |||
| PT | 26.46 (24.12, 30.42) | 13.20 (11.49, 15.68) | <0.001 |
| LPA | 28.24 (24.50, 32.30) | 14.18 (11.20, 16.34) | <0.001 |
| RPA | 27.12 (23.66, 31.90) | 17.71 (14.59, 22.30) | <0.001 |
| AO | 30.08 (25.49, 33.58) | 16.30 (12.81, 17.80) | <0.001 |
| AA | 22.36 (19.71, 24.66) | 11.50 (10.33, 13.84) | <0.001 |
| DA | 28.74 (25.43, 31.16) | 12.97 (11.31, 17.09) | <0.001 |
| LMCA-P | 10.59 (7.63, 13.51) | 13.76 (9.65, 18.02) | 0.007 |
| LAD-M | 17.28 (13.23, 21.13) | 30.41 (19.41, 35.24) | <0.001 |
| LAD-D | 21.72 (16.27, 29.28) | 30.42 (23.80, 42.19) | 0.001 |
| LCX-M | 19.34 (12.35, 23.18) | 21.58 (15.87, 33.36) | 0.047 |
| LCX-D | 23.25 (15.87, 27.95) | 30.28 (22.20, 37.79) | <0.001 |
| RCA-P | 12.44 (10.24, 14.04) | 15.53 (11.79, 22.50) | 0.001 |
| RCA-M | 15.49 (10.34, 20.49) | 22.20 (15.10, 27.38) | 0.002 |
| RCA-D | 20.27 (14.78, 26.23) | 23.99 (18.29, 28.66) | 0.043 |
| SNR values | |||
| PT | 12.95 (10.57, 17.06) | 37.95 (30.10, 44.15) | <0.001 |
| LPA | 13.07 (9.92, 15.26) | 31.98 (26.61, 37.79) | <0.001 |
| RPA | 13. 80 (9.76, 15.91) | 25.12 (20.66, 35.77) | <0.001 |
| AO | 10.67 (9.50, 12.96) | 30.32 (25.28, 35.28) | <0.001 |
| AA | 13.28 (11.73, 17.26) | 42.75 (35.39, 51.21) | <0.001 |
| DA | 9.64 (7.76, 13.14) | 34.09 (27.31, 42.93) | <0.001 |
| LMCA-P | 39.83 (34.78, 54.37) | 36.46 (27.44, 47.05) | 0.128 |
| LAD-M | 21.87 (16.14, 29.90) | 12.71 (8.86, 19.83) | <0.001 |
| LAD-D | 13.50 (10.69, 18.33) | 6.18 (4.54, 9.27) | <0.001 |
| LCX-M | 20.70 (15.35, 29.37) | 18.14 (9.41, 28.39) | 0.167 |
| LCX-D | 14.14 (9.94, 21.53) | 8.59 (5.77, 12.39) | <0.001 |
| RCA-P | 34.29 (25.59, 41.68) | 28.83 (19.02, 44.13) | 0.388 |
| RCA-M | 28.76 (21.23, 43.95) | 21.97 (14.92, 32.56) | 0.005 |
| RCA-D | 21.91 (15.17, 29.80) | 18.76 (13.42, 26.92) | 0.297 |
| CNR values | |||
| PT | 41.47 (28.68, 60.64) | 56.12 (44.90, 91.06) | 0.001 |
| LPA | 40.93 (27.34, 59.47) | 52.39 (39.65, 80.95) | 0.004 |
| RPA | 40.85 (27.13, 60.76) | 54.58 (39.57, 92.67) | 0.004 |
| AO | 40.06 (26.77, 52.51) | 56.47 (44.33, 90.85) | <0.001 |
| AA | 34.43 (24.68, 52.15) | 60.57 (46.94, 95.05) | <0.001 |
| DA | 31.24 (21.58, 47.73) | 59.94 (44.57, 93.00) | <0.001 |
| LMCA-P | 91.47 (74.58, 102.94) | 99.20 (83.16, 114.09) | 0.041 |
| LAD-M | 76.65 (67.14, 95.76) | 73.75 (58.72, 89.71) | 0.257 |
| LAD-D | 61.33 (54.40, 80.98) | 48.23 (39.22, 59.04) | <0.001 |
| LCX-M | 79.11 (64.75, 96.09) | 78.97 (67.42, 96.11) | 0.790 |
| LCX-D | 70.57 (53.01, 84.02) | 60.34 (46.78, 70.85) | 0.020 |
| RCA-P | 89.32 (76.14, 106.14) | 100.79 (82.20, 110.16) | 0.187 |
| RCA-M | 88.51 (76.75, 107.25) | 92.33 (73.68, 109.60) | 0.893 |
| RCA-D | 83.21 (73.87, 99.20) | 90.28 (71.59, 112.59) | 0.456 |
| Qualitative image score (4-point scale) | |||
| Pulmonary arteries | 2 (2, 2) | 2 (1, 3) | 0.199 |
| Coronary arteries | 2 (2, 2) | 2 (2, 2.5) | 0.101 |
| Thoracic aorta | 2 (2, 3) | 2 (1, 2) | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, K.; Wang, X.; Zheng, S.; Li, C.; Jin, L.; Li, M. Dedicated CCTA Followed by High-Pitch Scanning versus TRO-CT for Contrast Media and Radiation Dose Reduction: A Retrospective Study. Diagnostics 2022, 12, 2647. https://doi.org/10.3390/diagnostics12112647
Wang K, Wang X, Zheng S, Li C, Jin L, Li M. Dedicated CCTA Followed by High-Pitch Scanning versus TRO-CT for Contrast Media and Radiation Dose Reduction: A Retrospective Study. Diagnostics. 2022; 12(11):2647. https://doi.org/10.3390/diagnostics12112647
Chicago/Turabian StyleWang, Kun, Xiaodong Wang, Shaoqiang Zheng, Cheng Li, Liang Jin, and Ming Li. 2022. "Dedicated CCTA Followed by High-Pitch Scanning versus TRO-CT for Contrast Media and Radiation Dose Reduction: A Retrospective Study" Diagnostics 12, no. 11: 2647. https://doi.org/10.3390/diagnostics12112647
APA StyleWang, K., Wang, X., Zheng, S., Li, C., Jin, L., & Li, M. (2022). Dedicated CCTA Followed by High-Pitch Scanning versus TRO-CT for Contrast Media and Radiation Dose Reduction: A Retrospective Study. Diagnostics, 12(11), 2647. https://doi.org/10.3390/diagnostics12112647