
Visualization of Ray Propagation through Extended Depth-of-Focus Intraocular Lenses



Abstract
:1. Introduction
2. Material & Methods
2.1. Intraocular Lenses
2.2. Ray Propagation Setup
2.3. Unwanted Visual Effects Testing
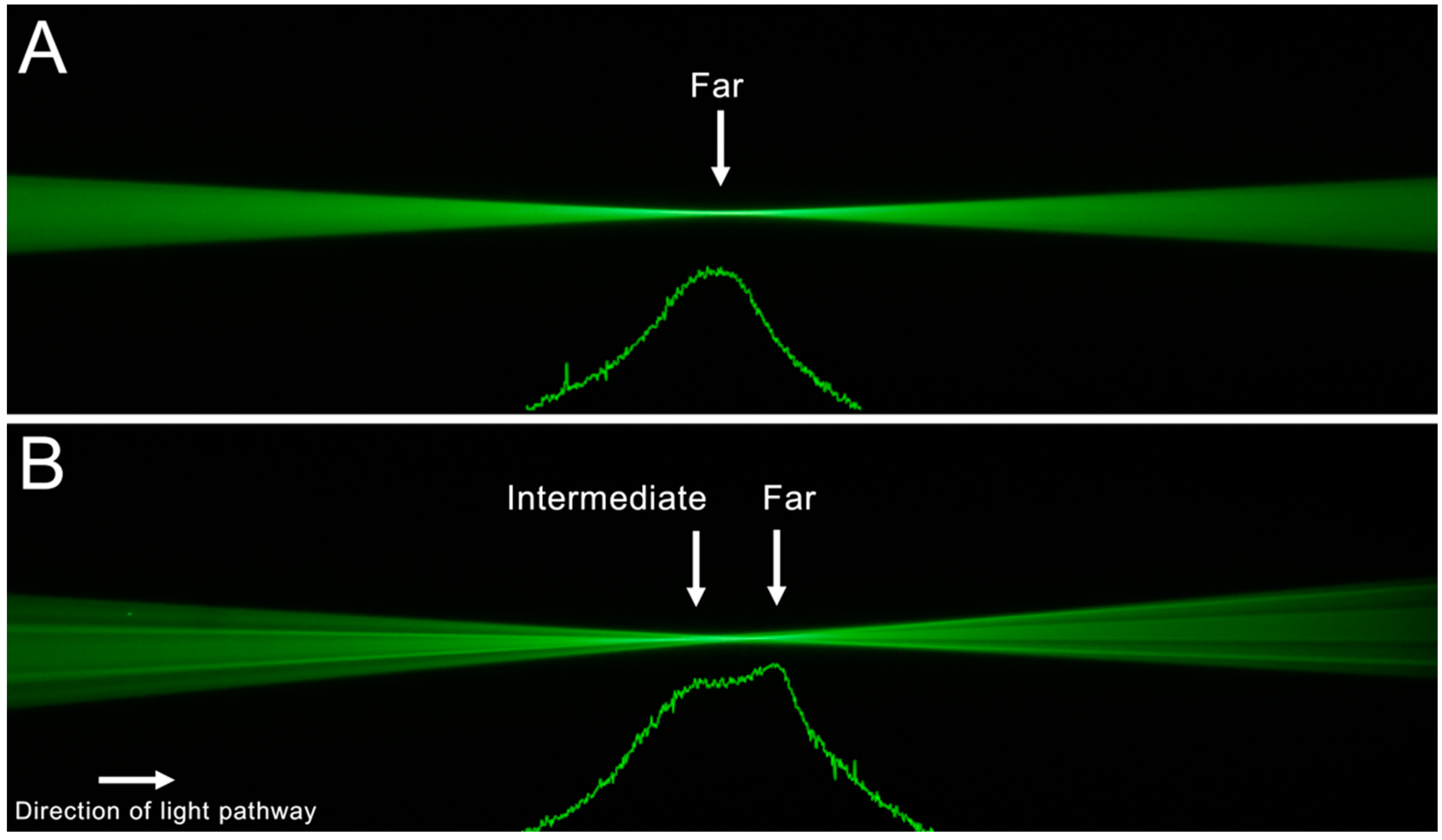
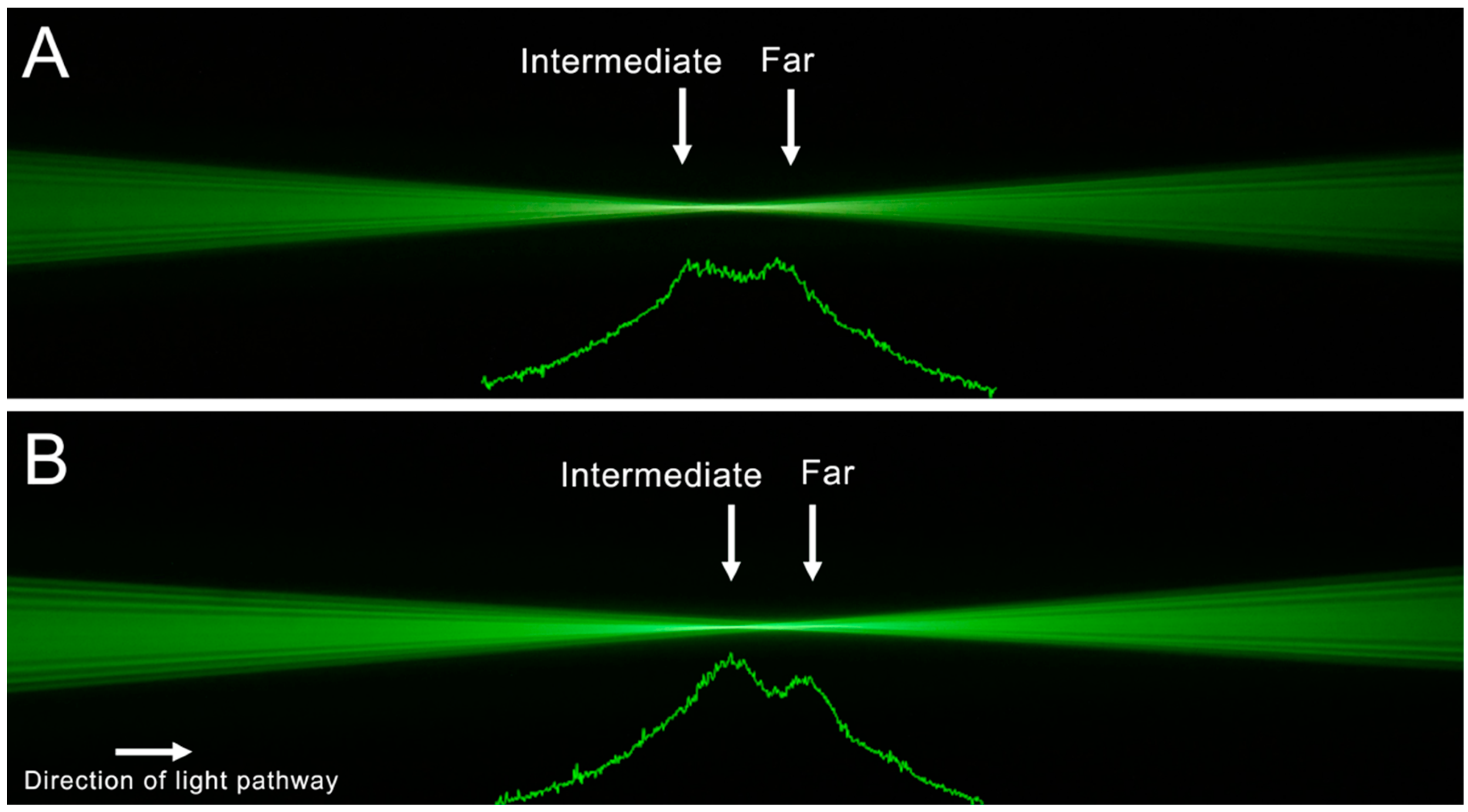
3. Results
Unwanted Visual Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kohnen, T.; Suryakumar, R. Extended depth-of-focus technology in intraocular lenses. J. Cataract. Refract. Surg. 2020, 46, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Baur, I.D.; Khoramnia, R.; Weindler, J.; Naujokaitis, T.; Poompokawat, P.; Auffarth, G.U. Clinical Outcomes of a New Hybrid Monofocal IOL with Extended Depth of Focus. J. Refract. Surg. 2021, 37, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Kohnen, T.; Petermann, K.; Böhm, M.; Hemkeppler, E.; Ahmad, W.; Hinzelmann, L.; Pawlowicz, K.; Jandewerth, T.; Lwowski, C. Non-diffractive wavefront shaping extended depth of focus (EDoF) intraocular lens: Visual performance and patient-reported outcome. J. Cataract. Refract. Surg. 2021, 48, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Bala, C.; Poyales, F.; Guarro, M.; Mesa, R.R.; Mearza, A.; Varma, D.K.; Jasti, S.; Lemp-Hull, J. Multicountry clinical outcomes of a new nondiffractive presbyopia-correcting IOL. J. Cataract Refract. Surg. 2021, 48, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Łabuz, G.; Son, H.-S.; Yildirim, T.M.; Khoramnia, R.; Auffarth, G.U. Assessment of the image quality of extended depth-of-focus intraocular lens models in polychromatic light. J. Cataract Refract. Surg. 2020, 46, 108–115. [Google Scholar] [CrossRef]
- Son, H.-S.; Łabuz, G.; Khoramnia, R.; Yildirim, T.M.; Auffarth, G.U. Laboratory analysis and ray visualization of diffractive optics with enhanced intermediate vision. BMC Ophthalmol. 2021, 21, 1–7. [Google Scholar] [CrossRef]
- Vega, F.M.M.S.; Garzón, N.; Gil, M.A.; Rigato, F. Features of the optical surface of an extended depth of focus intraocular lens. In Proceedings of the 37th Congress of the ESCRS, Paris, France, 14–18 September 2019. [Google Scholar]
- Millán, M.S.; Vega, F. Extended depth of focus intraocular lens. Chromatic performance. Biomed. Opt. Express 2017, 8, 4294–4309. [Google Scholar] [CrossRef] [Green Version]
- Łabuz, G.; Papadatou, E.; Khoramnia, R.; Auffarth, G.U. Longitudinal chromatic aberration and polychromatic image quality metrics of intraocular lenses. J. Refract. Surg. 2018, 34, 832–838. [Google Scholar] [CrossRef] [Green Version]
- Weeber, H.A.; Meijer, S.T.; Piers, P.A. Extending the range of vision using diffractive intraocular lens technology. J. Cataract. Refract. Surg. 2015, 41, 2746–2754. [Google Scholar] [CrossRef]
- Kretz, T.; Tarib, I.; Kaiser, I.; Herbers, C.; Hagen, P.; Breyer, D. Postoperative results in patients implanted with a novel enhanced depth of focus intraocular lens. EC Ophthalmol. 2018, 4, 192–202. [Google Scholar]
- Carl Zeiss Meditec AG. AT LARA® 829MP IOL. Available online: https://www.zeiss.com/meditec/int/products/iols/edof-iols/at-lara-family.html (accessed on 5 July 2022).
- Son, H.S.; Labuz, G.; Khoramnia, R.; Merz, P.; Yildirim, T.M.; Auffarth, G.U. Ray propagation imaging and optical quality evaluation of different intraocular lens models. PLoS ONE 2020, 15, e0228342. [Google Scholar] [CrossRef] [PubMed]
- Alba-Bueno, F.; Garzón, N.; Vega, F.; Poyales, F.; Millán, M.S. Patient-perceived and laboratory-measured halos associated with diffractive bifocal and trifocal intraocular lenses. Curr. Eye Res. 2018, 43, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Schallhorn, J.M. Multifocal and extended depth of focus intraocular lenses: A comparison of data from the United States food and drug administration premarket approval trials. J. Refract. Surg. 2021, 37, 98–104. [Google Scholar] [CrossRef] [PubMed]
- ISO 11979-2; Ophthalmic Implants—Intraocular Lenses—Part 2: Optical Properties and Test Methods. Standardization TIOf: Geneva, Switzerland, 2014.
- Wang, L.; Dai, E.; Koch, D.D.; Nathoo, A. Optical aberrations of the human anterior cornea. J. Cataract. Refract. Surg. 2003, 29, 1514–1521. [Google Scholar] [CrossRef]
- Łabuz, G.; Son, H.-S.; Naujokaitis, T.; Yildirim, T.M.; Khoramnia, R.; Auffarth, G.U. Laboratory Investigation of Preclinical Visual-Quality Metrics and Halo-Size in Enhanced Monofocal Intraocular Lenses. Ophthalmol. Ther. 2021, 10, 1093–1104. [Google Scholar] [CrossRef]
- Pedrotti, E.; Bruni, E.; Bonacci, E.; Badalamenti, R.; Mastropasqua, R.; Marchini, G. Comparative analysis of the clinical outcomes with a monofocal and an extended range of vision intraocular lens. J. Refract. Surg. 2016, 32, 436–442. [Google Scholar] [CrossRef]
- Cochener, B.; Boutillier, G.; Lamard, M.; Auberger-Zagnoli, C. A comparative evaluation of a new generation of diffractive trifocal and extended depth of focus intraocular lenses. J. Refract. Surg. 2018, 34, 507–514. [Google Scholar] [CrossRef]
- Breyer, D.R.; Kaymak, H.; Ax, T.; Kretz, F.T.; Auffarth, G.U.; Hagen, P.R. Multifocal intraocular lenses and extended depth of focus intraocular lenses. Asia-Pac. J. Ophthalmol. 2017, 6, 339–349. [Google Scholar]
- Chae, S.H.; Son, H.S.; Khoramnia, R.; Lee, K.H.; Choi, C.Y. Laboratory evaluation of the optical properties of two extended-depth-of-focus intraocular lenses. BMC Ophthalmol. 2020, 20, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Auffarth, G.U.; Moraru, O.; Munteanu, M.; Tognetto, D.; Bordin, P.; Belucci, R.; Khoramnia, R.; Son, H.-S. European, Multicenter, Prospective, Non-comparative Clinical Evaluation of an Extended Depth of Focus Intraocular Lens. J. Refract. Surg. 2020, 36, 426–434. [Google Scholar] [CrossRef]
- Giers, B.C.; Khoramnia, R.; Varadi, D.; Wallek, H.; Son, H.S.; Attia, M.S.; Auffarth, G.U. Functional results and photic phenomena with new extended-depth-of-focus intraocular Lens. BMC Ophthalmol. 2019, 19, 197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attia, M.S.A.; Auffarth, G.U.; Kretz, F.T.A.; Tandogan, T.; Rabsilber, T.M.; Holzer, M.P.; Khoramnia, R. Clinical evaluation of an extended depth of focus intraocular lens with the Salzburg reading desk. J. Refract. Surg. 2017, 33, 664–669. [Google Scholar] [CrossRef] [PubMed]
- Rocha, K.M. Extended Depth of Focus IOLs: The Next Chapter in Refractive Technology? J. Refract. Surg. 2017, 33, 146–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacRae, S.; Holladay, J.T.; Glasser, A.; Calogero, D.; Hilmantel, G.; Masket, S.; Stark, W.; Tarver, M.E.; Nguyen, T.; Eydelman, M. Special Report: American Academy of Ophthalmology Task Force Consensus Statement for Extended Depth of Focus Intraocular Lenses. Ophthalmology 2016, 124, 139–141. [Google Scholar] [CrossRef] [Green Version]
- Doughty, M.J. pH dependent spectral properties of sodium fluorescein ophthalmic solutions revisited. Ophthalmic Physiol. Opt. 2010, 30, 167–174. [Google Scholar] [CrossRef]
- Eppig, T.; Rubly, K.; Rawer, A.; Langenbucher, A. Visualization of light propagation with multifocal intraocular lenses using the ouzo effect. BioMed Res. Int. 2019, 2019, 6425040. [Google Scholar] [CrossRef] [Green Version]
- Millán, M.S.; Vega, F. Through-focus energy efficiency and longitudinal chromatic aberration of three presbyopia-correcting intraocular lenses. Transl. Vis. Sci. Technol. 2020, 9, 13. [Google Scholar] [CrossRef]
- Łabuz, G.; Auffarth, G.U.; Özen, A.; Van den Berg, T.J.; Yildirim, T.M.; Son, H.S.; Khoramnia, R. The effect of a spectral filter on visual quality in patients with an extended-depth-of-focus intraocular lens. Am. J. Ophthalmol. 2019, 208, 56–63. [Google Scholar] [CrossRef]
- Reiß, S.; Forbrig, J.; Guthoff, R.F.; Terwee, T.; Stolz, H.; Siewert, S.; El-Tamer, A.; Hinze, U.; Chichkov, B.N.; Stachs, O. Optimierung der Visualisierungstechnik für Strahlenverläufe durch Intraokularlinsen zur Charakterisierung multifokaler Abbildungseigenschaften von Fresnel-Zonenplatten. Klin. Mon. Für Augenheilkd. 2014, 231, 1183–1186. [Google Scholar] [CrossRef]
- Son, H.-S.; Łabuz, G.; Khoramnia, R.; Yildirim, T.M.; Choi, C.Y.; Knorz, M.C.; Auffarth, G.U. Visualization of Forward Light Scatter in Opacified Intraocular Lenses and Straylight Assessment. Diagnostics 2021, 11, 1512. [Google Scholar] [CrossRef]
- Fernández-Vega-Cueto, L.; Madrid-Costa, D.; Alfonso-Bartolozzi, B.; Vega, F.; Millán, M.S.; Alfonso, J.F. Optical and Clinical Outcomes of an Extended Range of Vision Intraocular Lens. J. Refract. Surg. 2022, 38, 168–176. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Dong, Y.; Wang, Y. Efficacy and safety of extended depth of focus intraocular lenses in cataract surgery: A systematic review and meta-analysis. BMC Ophthalmol. 2019, 19, 198. [Google Scholar] [CrossRef] [PubMed]
- Ganesh, S.; Brar, S.; Nikhil, R.; Rathod, D. Clinical Outcomes, Contrast Sensitivity, Reading Performance and Patient Satisfaction Following Bilateral Implantation of AT LARA 829MP EDoF IOLs. Clin. Ophthalmol. 2021, 15, 4247. [Google Scholar] [CrossRef] [PubMed]
- Reinhard, T.; Maier, P.; Böhringer, D.; Bertelmann, E.; Brockmann, T.; Kiraly, L.; Salom, D.; Piovella, M.; Colonval, S.; Mendicute, J. Comparison of two extended depth of focus intraocular lenses with a monofocal lens: A multi-centre randomised trial. Graefe Arch. Clin. Exp. Ophthalmol. 2021, 259, 431–442. [Google Scholar] [CrossRef]
- Arrigo, A.; Gambaro, G.; Fasce, F.; Aragona, E.; Figini, I.; Bandello, F. Extended depth-of-focus (EDOF) AcrySof® IQ Vivity® intraocular lens implant: A real-life experience. Graefe Arch. Clin. Exp. Ophthalmol. 2021, 259, 2717–2722. [Google Scholar] [CrossRef]
- Johannsdottir, K.R.; Stelmach, L.B. Monovision: A review of the scientific literature. Optom. Vis. Sci. 2001, 78, 646–651. [Google Scholar] [CrossRef]
- Zhang, F.; Sugar, A.; Jacobsen, G.; Collins, M. Visual function and patient satisfaction: Comparison between bilateral diffractive multifocal intraocular lenses and monovision pseudophakia. J. Cataract. Refract. Surg. 2011, 37, 446–453. [Google Scholar] [CrossRef]
- Terwee, T.; Weeber, H.; van der Mooren, M.; Piers, P. Visualization of the retinal image in an eye model with spherical and aspheric, diffractive, and refractive multifocal intraocular lenses. J. Refract. Surg. 2008, 24, 223–232. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AcrySof IQ SN60WF | AcrySof IQ Vivity DFT015 | Symfony ZXR00 | AT Lara 829 MP | |
|---|---|---|---|---|
| Optic design | One-piece | One-piece/wavefront shaping-optic | One-piece/combined diffractive-refractive extended-depth-of-focus | One-piece/combined diffractive-refractive extended-depth-of-focus |
| Lens diameter | 13.0 mm | 13.0 mm | 13.0 mm | 11.0 mm |
| Optic diameter | 6.0 mm | 6.0 mm | 6.0 mm | 6.0 mm |
| Dioptric power | 20.0 D | 20.0 D | 20.0 D | 20.0 D |
| Lens material | Hydrophobic Acrylate | Hydrophobic Acrylate | Hydrophobic Acrylate | Hydrophilic Acrylate (25% water content), hydrophobic surface |
| Refractive index | 1.55 | 1.55 | 1.47 | 1.46 |
| Spherical Aberration | −0.20 μm | −0.20 μm | −0.27 μm | Aberration neutral |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baur, I.D.; Auffarth, G.U.; Yan, W.; Łabuz, G.; Khoramnia, R. Visualization of Ray Propagation through Extended Depth-of-Focus Intraocular Lenses. Diagnostics 2022, 12, 2667. https://doi.org/10.3390/diagnostics12112667
Baur ID, Auffarth GU, Yan W, Łabuz G, Khoramnia R. Visualization of Ray Propagation through Extended Depth-of-Focus Intraocular Lenses. Diagnostics. 2022; 12(11):2667. https://doi.org/10.3390/diagnostics12112667
Chicago/Turabian StyleBaur, Isabella D., Gerd U. Auffarth, Weijia Yan, Grzegorz Łabuz, and Ramin Khoramnia. 2022. "Visualization of Ray Propagation through Extended Depth-of-Focus Intraocular Lenses" Diagnostics 12, no. 11: 2667. https://doi.org/10.3390/diagnostics12112667