
Endoscopic Ultrasound Guided Fine Needle Aspiration versus Endoscopic Ultrasound Guided Fine Needle Biopsy for Pancreatic Cancer Diagnosis: A Systematic Review and Meta-Analysis

 and
and
Abstract
1. Introduction
2. Methods
2.1. Information Source and Search Strategy
2.2. Keywords—Search Equation
2.3. Eligibility Criteria, Articles Selection
2.4. Data Extraction and Quality Analysis of the Retained Studies
2.5. Data Synthesis
3. Results
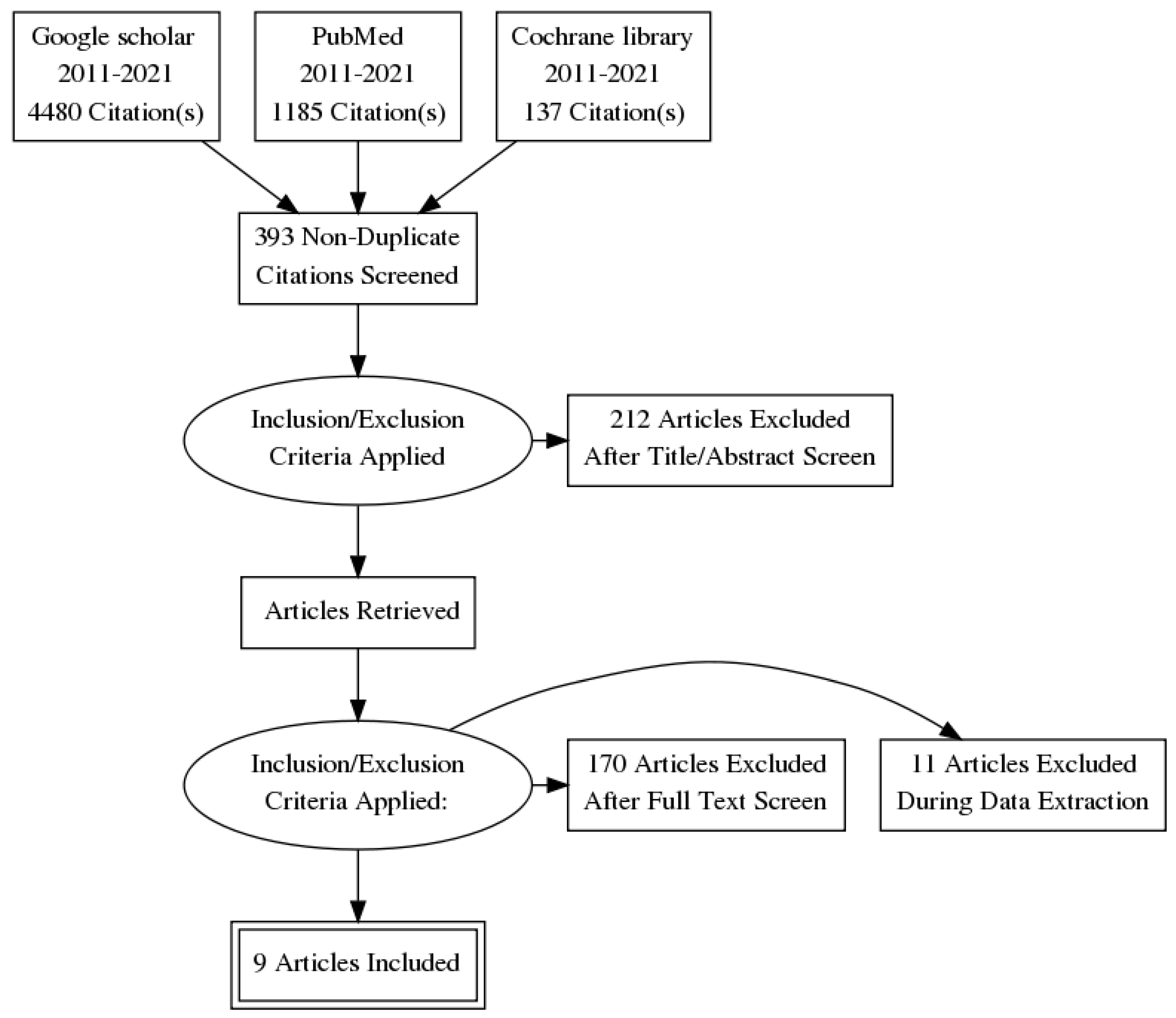
3.1. Selected Articles
3.2. Study Characteristics
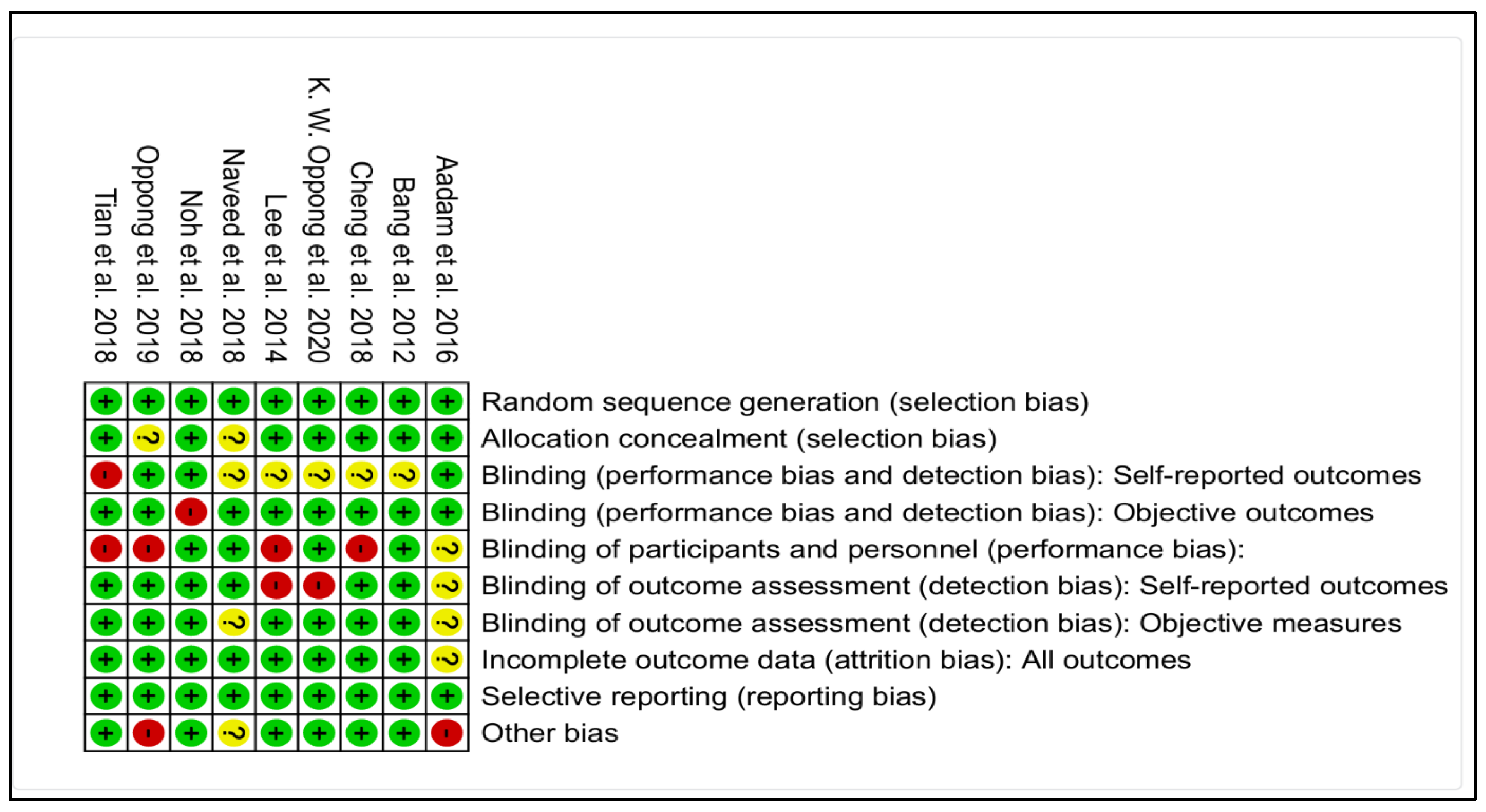
3.3. Study Quality Analysis
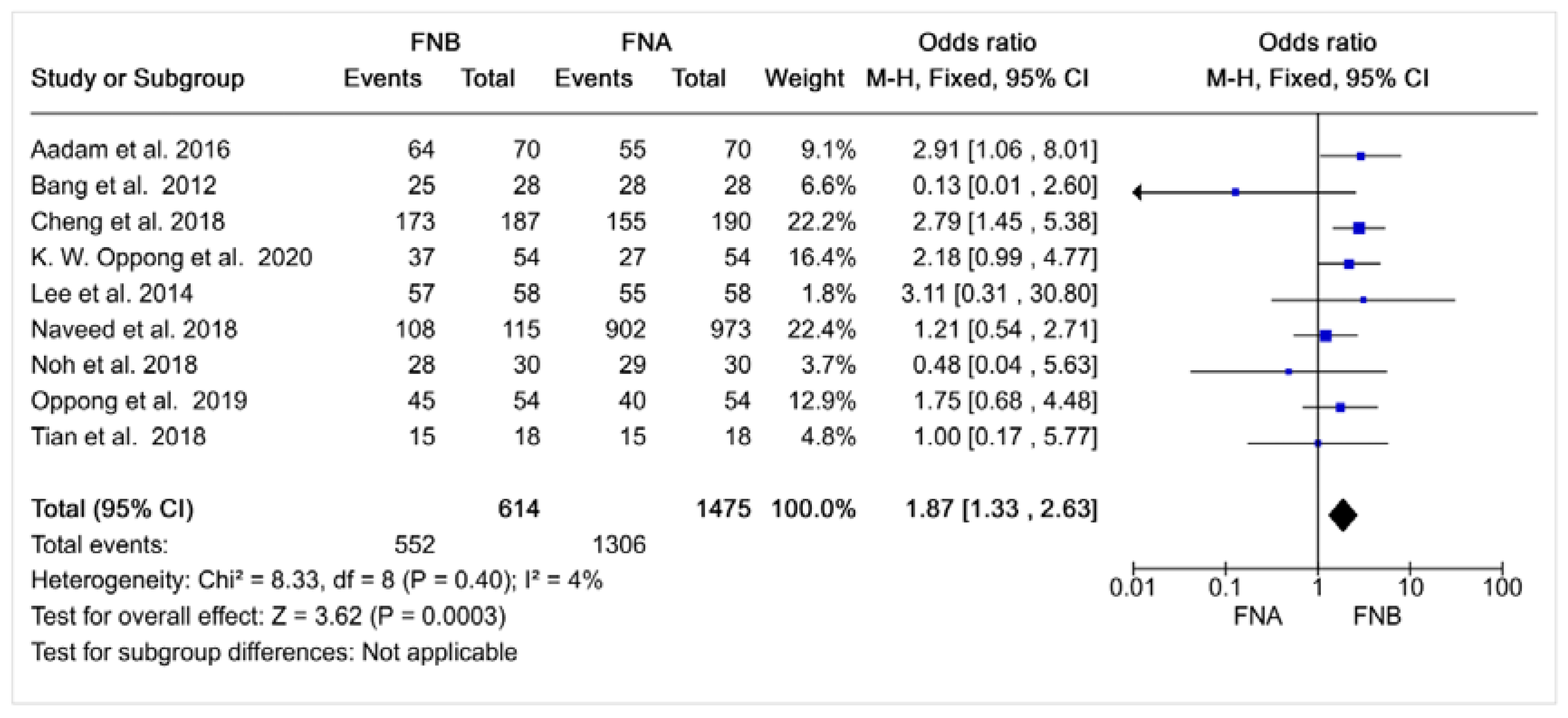
3.4. Quantitative Synthesis of the Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Partensky, C. Cancer is a burden in global scale. Médecine Mal. Métaboliques 2019, 13, 288–292. Available online: https://www.sciencedirect.com/science/article/pii/S1957255719300768 (accessed on 3 July 2021). [CrossRef]
- McGuigan, A.; Kelly, P.; Turkington, R.C.; Jones, C.; Coleman, H.G.; McCain, R.S. Pancreatic cancer: A review of clinical diagnosis, epidemiology, treatment and outcomes. World J. Gastroenterol. 2018, 24, 4846–4861. [Google Scholar] [CrossRef] [PubMed]
- Feng, R.-M.; Zong, Y.-N.; Cao, S.-M.; Xu, R.-H. Current cancer situation in China: Good or bad news from the 2018 Global Cancer Statistics? Cancer Commun. 2019, 39, 22. Available online: http://doi.wiley.com/10.1186/s40880-019-0368-6 (accessed on 3 July 2021). [CrossRef] [PubMed]
- Drouillard, A.; Manfredi, S.; Lepage, C.; Bouvier, A.-M. Epidemiology of pancreatic cancer. Bull. Cancer 2018, 105, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Sanagapalli, S.; Stoita, A. Challenges in diagnosis of pancreatic cancer. World J. Gastroenterol. 2018, 24, 2047–2060. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5960811/ (accessed on 6 June 2021). [CrossRef]
- Cosgrove, N.D.; Yan, L.; Siddiqui, A. Preoperative endoscopic ultrasound-guided fine needle aspiration for diagnosis of pancreatic cancer in potentially resectable patients: Is this safe? Endosc. Ultrasound. 2015, 4, 81–84. [Google Scholar]
- Renelus, B.D.; Jamorabo, D.S.; Boston, I.; Briggs, W.M.; Poneros, J.M. Endoscopic Ultrasound-Guided Fine Needle Biopsy Needles Provide Higher Diagnostic Yield Compared to Endoscopic Ultrasound-Guided Fine Needle Aspiration Needles When Sampling Solid Pancreatic Lesions: A Meta-Analysis. Clin. Endosc. 2021, 54, 261–268. [Google Scholar] [CrossRef]
- Van Riet, P.A.; Erler, N.S.; Bruno, M.J.; Cahen, D.L. Comparison of fine-needle aspiration and fine-needle biopsy devices for endoscopic ultrasound-guided sampling of solid lesions: A systemic review and meta-analysis. Endoscopy 2021, 53, 411–423. [Google Scholar] [CrossRef]
- Han, S.; Bhullar, F.; Alaber, O.; Kamal, A.; Hopson, P.; Kanthasamy, K.; Coughlin, S.; Archibugi, L.; Thiruvengadam, N.; Moreau, C.; et al. Comparative diagnostic accuracy of EUS needles in solid pancreatic masses: A network meta-analysis. Endosc. Int. Open 2021, 9, E853–E862. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8159621/ (accessed on 8 June 2021).
- Wang, J.; Zhao, S.; Chen, Y.; Jia, R.; Zhang, X. Endoscopic ultrasound guided fine needle aspiration versus endoscopic ultrasound guided fine needle biopsy in sampling pancreatic masses: A meta-analysis. Medicine 2017, 96, e7452. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. Available online: https://www.bmj.com/content/343/bmj.d5928 (accessed on 19 June 2021). [CrossRef]
- Quality-Assessment-Tool-Dictionary-En.pdf. Available online: https://www.healthevidence.org/documents/our-appraisal-tools/quality-assessment-tool-dictionary-en.pdf (accessed on 8 July 2021).
- Tian, L.; Tang, A.L.; Zhang, L.; Liu, X.W.; Li, J.B.; Wang, F.; Shen, S.R.; Wang, X.Y. Evaluation of 22G fine-needle aspiration (FNA) versus fine-needle biopsy (FNB) for endoscopic ultrasound-guided sampling of pancreatic lesions: A prospective comparison study. Surg. Endosc. 2018, 32, 3533–3539. Available online: http://link.springer.com/10.1007/s00464-018-6075-6 (accessed on 7 June 2021). [CrossRef] [PubMed]
- Aadam, A.A.; Wani, S.; Amick, A.; Shah, J.N.; Bhat, Y.M.; Hamerski, C.M.; Klapman, J.B.; Muthusamy, V.R.; Watson, R.R.; Rademaker, A.W.; et al. A randomized controlled cross-over trial and cost analysis comparing endoscopic ultrasound fine needle aspiration and fine needle biopsy. Endosc. Int. Open 2016, 4, E497–E505. [Google Scholar] [CrossRef] [PubMed]
- Bang, J.Y.; Hebert-Magee, S.; Trevino, J.; Ramesh, J.; Varadarajulu, S. Randomized trial comparing the 22-gauge aspiration and 22-gauge biopsy needles for EUS-guided sampling of solid pancreatic mass lesions. Gastrointest Endosc. 2012, 76, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Cheng, B.; Zhang, Y.; Chen, Q.; Sun, B.; Deng, Z.; Shan, H.; Dou, L.; Wang, J.; Li, Y.; Yang, X.; et al. Analysis of Fine-Needle Biopsy vs. Fine-Needle Aspiration in Diagnosis of Pancreatic and Abdominal Masses: A Prospective, Multicenter, Randomized Controlled Trial. Clin. Gastroenterol. Hepatol. 2018, 16, 1314–1321. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.N.; Moon, J.H.; Kim, H.K.; Choi, H.J.; Choi, M.H.; Kim, D.C.; Lee, T.H.; Cha, S.W.; Cho, Y.D.; Park, S.H. Core biopsy needle versus standard aspiration needle for endoscopic ultrasound-guided sampling of solid pancreatic masses: A randomized parallel-group study. Endoscopy 2014, 46, 1056–1062. [Google Scholar] [CrossRef] [PubMed]
- Oh, D.H.; Choi, K.; Gu, S.; Cho, J.; Jang, K.T.; Woo, Y.S.; Lee, K.T.; Lee, J.K.; Lee, K.H. Comparison of 22-gauge standard fine needle versus core biopsy needle for endoscopic ultrasound-guided sampling of suspected pancreatic cancer: A randomized crossover trial. Scand. J. Gastroenterol. 2018, 53, 94–99. [Google Scholar]
- Naveed, M.; Siddiqui, A.A.; Kowalski, T.E.; Loren, D.E.; Khalid, A.; Soomro, A.; Mazhar, S.M.; Yoo, J.; Hasan, R.; Yalamanchili, S.; et al. A Multicenter comparative trial of a novel EUS-guided core biopsy needle (SharkCore™) with the 22-gauge needle in patients with solid pancreatic mass lesions. Endosc. Ultrasound 2018, 7, 34–40. Available online: https://jdc.jefferson.edu/gastro_hepfp/48 (accessed on 1 January 2018).
- Oppong, K.; Bekkali, N.; Leeds, J.; Johnson, S.; Nayar, M.; Darne, A.; Egan, M.; Bassett, P.; Haugk, B. PWE-072 EUS Fork-tip biopsy versus EUS FNA in the diagnosis of solid pancreatic masses. Gut1 2019, 68 (Suppl. 2), A160–A161. Available online: https://gut.bmj.com/content/68/Suppl_2/A160.2 (accessed on 7 June 2021).
- Oppong, K.W.; Bekkali, N.L.; Leeds, J.S.; Johnson, S.J.; Nayar, M.K.; Darné, A.; Egan, M.; Bassett, P.; Haugk, B. Fork-tip needle biopsy versus fine-needle aspiration in endoscopic ultrasound-guided sampling of solid pancreatic masses: A randomized crossover study. Endoscopy 2020, 52, 454–461. [Google Scholar] [CrossRef]
- Kandel, P.; Wallace, M.B. Recent advancement in EUS-guided fine needle sampling. J. Gastroenterol. 2019, 54, 377–387. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6470116/ (accessed on 4 July 2021). [CrossRef] [PubMed]
- Jani, B.S.; Rzouq, F.; Saligram, S.; Lim, D.; Rastogi, A.; Bonino, J.; Olyaee, M. Endoscopic Ultrasound-Guided Fine-Needle Aspiration of Pancreatic Lesions: A Systematic Review of Technical and Procedural Variables. N. Am. J. Med. Sci. 2016, 8, 1–11. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4784176/ (accessed on 8 July 2021). [PubMed]
- Colby, S. EUS-FNB without ROSE Not Inferior to EUS-FNB with ROSE for Detecting Solid Pancreatic Lesions—Gastroenterology Advisor 2021. Available online: https://www.gastroenterologyadvisor.com/pancreatic-disorders/rapid-on-site-evaluation-no-longer-routinely-recommended-for-evaluation-of-solid-pancreatic-lesions/ (accessed on 20 November 2022).
- Deprez, P.H.; Moons, L.M.; O’Toole, D.; Gincul, R.; Seicean, A.; Pimentel-Nunes, P.; Fernández-Esparrach, G.; Polkowski, M.; Vieth, M.; Borbath, I.; et al. Endoscopic management of subepithelial lesions including neuroendocrine neoplasms: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2022, 54, 412–429. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.; Pattarapuntakul, T.; Netinatsunton, N.; Ovartlarnporn, B.; Sottisuporn, J.; Chamroonkul, N.; Sripongpun, P.; Jandee, S.; Kaewdech, A.; Attasaranya, S.; et al. Diagnostic performance of endoscopic ultrasound-guided tissue acquisition by EUS-FNA versus EUS-FNB for solid pancreatic mass without ROSE: A retrospective study. World J. Surg. Oncol. 2022, 20, 215. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.I.; Chatterjee, A.; Berger, R.; Kanber, Y.; Wyse, J.; Lam, E.; Gan, I.; Auger, M.; Kenshil, S.; Telford, J.; et al. Endoscopic ultrasound (EUS)-guided fine needle biopsy alone vs. EUS-guided fine needle aspiration with rapid onsite evaluation in pancreatic lesions: A multicenter randomized trial. Endoscopy 2022, 54, 4–12. [Google Scholar] [CrossRef]
- Pausawasdi, N.; Cheirsilpa, K.; Chalermwai, W.; Asokan, I.; Sriprayoon, T.; Charatcharoenwitthaya, P. Endoscopic Ultrasound-Guided Fine-Needle Biopsy Using 22G Franseen Needles without Rapid On-Site Evaluation for Diagnosis of Intraabdominal Masses. J. Clin. Med. 2022, 11, 1051. [Google Scholar] [CrossRef]
- Ishikawa, T.; Ohno, E.; Mizutani, Y.; Iida, T.; Uetsuki, K.; Yashika, J.; Yamada, K.; Gibo, N.; Aoki, T.; Kataoka, K.; et al. Usefulness of Macroscopic On-Site Evaluation Using a Stereomicroscope during EUS-FNB for Diagnosing Solid Pancreatic Lesions. Can. J. Gastroenterol. Hepatol. 2022, 2022, 2737578. [Google Scholar] [CrossRef]
- Lai, J.H.; Lin, C.C.; Lin, H.H.; Chen, M.J. Is contrast-enhanced endoscopic ultrasound-guided fine needle biopsy better than conventional fine needle biopsy? A retrospective study in a medical center. Surg. Endosc. 2022, 36, 6138–6143. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Authors | Title | Type | Country, Patients and Lesions Type | Method and Needle Type | Diagnostic Precision | Other Results | Conclusion |
|---|---|---|---|---|---|---|---|
| Tian et al. (2018) [13] | «Evaluation of 22G fine-needle aspiration (FNA) versus 22G fine-needle biopsy (FNB) for endoscopic ultrasound-guided sampling of pancreatic lesions: a prospective comparison study» | Prospective comparative studies | Studies realized in China on 23 men and 13 women at average age of 59.5 ± 19.5 years old (45–75 years old) with solid pancreatic masses. Total number of included patients: 46. | Patients were randomly allocated in two groups: EUS-FNA (n = 18) and EUS-FNB (n = 18) Using 22G EUS-FNB needles (EchoTipProCore, Cook Medical) and 22G EUS-FNA (Olympus, GF UCT 160). | The precision of the diagnostic was about 83.3% for both techniques (p > 0.05). | The negative predictive value, the sensitivity and the specificity were, respectively, 50%, 80% and 100% for EUS-FNB and 82%, 78% and 100% for EUS-FNA. The positive predictive value was about 100% for both of the techniques. The EUS-FNB needed less punctures than the EUS-FNA (1.11 vs. 1.83 p < 0.05). | 22G EUS-FNB is a sure and effective way to diagnose the solid pancreatic masses and the EUS-FNB needs a lower number of needle pass to establish a diagnostic compared with EUS-FNA |
| Oppong et al. (2019) [20] | «PWE-072 EUS Fork-tip biopsy versus EUS FNA in the diagnosis of solid pancreatic masses» | Randomized controlled trial | Studies performed in the United Kingdom on 108 patients with 57 men at an average age of 66.9 ± 10.9 years old with solid pancreatic masses. Total number of included patients: 108. | Each patient went through three passes with a EUS-FNA needle (Beacon 25G and 22G) and three passes with a cored EUS-FNA (SharkCore 25G and 22G) randomly made. 25G needles were used for trans-duodenal sampling and 22G for trans-gastric. | The diagnostic precision of the EUS-FNB was significantly superior to that of the FNB (84.2% vs. 75% p = 0.041). | The notification time of the pathology (191 s vs. 332 s p < 0.0001) was significantly shorter with the EUS-FNB than with the EUS-FNA EUS-FNB had a diagnostic tool more abundant (59.2% vs. 44.4% p = 0.017) and an easier diagnostic (68.9 % vs. 51.9% p = 0.03) than EUS-FNA | SharkCore Needle were significantly better than the EUS-FNA standard needle in diagnosing the solid pancreatic masses and associated to a better quality of sample, a facility of time notification of sampling and a shorter pathology notification |
| Naveed et al. (2018) [19] | «A multicenter comparative trial of a novel EUS-guided core biopsy needle (SharkCore™) with the 22-gauge needle in patients with solid pancreatic mass lesions» | Multicenter retrospective comparative studies | Studies made in the United States of 1088 patients where 533 were women. The average age of the patients was 66 years old with solid pancreatic masses. Total number of included patients: 1088. | 115 sustained a EUS-FNB with a 22G SharkCore needle and 973 sustained standard EUS-FNA of 22G (EchoTip Ultra 3 needle; Wilson-Cook Medical, Winston-Salem, North Carolina) | The diagnostic precision was about 94.1% for the EUS-FNB and 92.7% for EUS-FNA p = 0.85 | The difference was not statistically significant for the sensitivity and the specificity in the two groups. The median number of passes to obtain a tissue diagnostic by using EUS-FNB was significantly inferior to that of the standard needle (1 vs. 3 p < 0.001). | The EUS-FNB has a diagnostic yield similar to the EUS-FNA standard needle and greatly reduces the amount of necessary needle passes to get the tissues diagnostic. |
| Cheng et al. (2018) [16] | «Analysis of Fine-Needle Biopsy vs. Fine-Needle Aspiration in Diagnosis of Pancreatic and Abdominal Masses: A Prospective, Multicenter, Randomized Controlled Trial» | Prospective trial, multicenter, controlled and randomized | Studies made in China with 377 patients with solid pancreatic masses with 232 men. The average age was 58 years old (249 pancreatic masses). Total number of included patients: 377. | Patients were randomly allocated into groups for an evaluation 22G EUS-FNA (n = 190 and 22G EUS-FNB (n = 187). Group A, using commercially available FNA needles (22G EchoTip Ultra needle, Cook Medical); Group B, using the EUS-FNB needles (22G EchoTip ProCore needle, Cook Medical). | The diagnostic precision was about 92.68% for EUS-FNB vs. 81.75% for EUS-FNA (p = 0.0099) while the cytological precision was about 88.62% (EUS-FNB) vs. 79.37% (EUS-FNA) (p = 0.00468). | The sampling for the EUS-FNB was about 91.44% vs. 80% for the EUS-FNA (p = 0.0015). | The samples obtained through EUS-FNB needles produced a more accurate diagnostic than the samples collected with EUS-FNA needles for the pancreatic masses. |
| Bang et al. (2012) [15] | «Randomized trial comparing the 22-gauge aspiration and 22-gauge biopsy needles for EUS-guided sampling of solid pancreatic mass lesions» | Randomized controlled trial | Studies made in the United-States with 31 men and 25 women in the age between 57–77 with solid pancreatic masses. Total number of included patients: 56. | In total, 28 patients were randomly selected in the group of 22G EUS-FNB (Echotip ProCore; Cook Endoscopy, Bloomington, IN) and 28 in the group of 22G EUS-FNA (Expect; Boston Scientific, Natick, Mass). | The diagnostic precision was about 100% for the EUS-FNA and 89.3% for the EUS-FNB (p = 0.24). | No significant difference in the median number of needle passes for diagnosing pancreatic lesions. Noted 3.6% of complications for the two methods. Samples quality was about 80% for EUS-FNB vs. 66.7% for the EUS-FNA p = 0.66. | Lack of significant difference between the two needles for the diagnostic precision. |
| Aadam et al. (2016) [14] | «A randomized controlled cross-over trial and cost analysis comparing endoscopic ultrasound fine needle aspiration and fine needle biopsy» | Multicenter randomized crossed trial | Studies realized in the United States on 74 men and 66 women with an average age of 64 years old with solid pancreatic masses. Total number of included patients: 140 | 140 patients were involved and 70 of them were randomly divided in the group 22G and 25G EUS-FNA (EchotipTM, Cook Medical, Winston-Salem, NC; ExpectTM, Boston Scientific, Natick MA) and the other 70 for 19G, 22G and 25G EUS-FNB (Echotip ProcoreTM, Cook Medical, Winston-Salem, NC). | The diagnostic precision was about 91.7% for the EUS-FNB vs. 78.4% for the EUS-FNA (p = 0.19). | The quality of the sample was better with the EUS-FNB (90%) vs. 67.1% for the EUS-FNA p = 0.002. | There is no statistical difference concerning the diagnostic performance between the 2 needles. |
| Oppong et al. (2020) [21] | «Fork-tip needle biopsy versus fine-needle aspiration in endoscopic ultrasound-guided sampling of solid pancreatic masses: a randomized crossover study» | Randomized crossed studies | Studies done in United Kingdom of 57 men and 51 women with an average age of 69 years old (30–87 years old) with solid pancreatic masses. Total number of included patients: 108 | 108 patients were recruited. 54 patients were divided in the 22G SharkCore needle group (EUS-FNB) and 54 in the 25G Beacon needle group (EUS-FNA) | The diagnostic precision was about 69% [IC 95% 60–78%] for the EUS-FNB and 51% [IC 95% 41–61%] for the EUS-FNA p < 0.001. | The median time of diagnostic observation was 188 s for the FNB vs. 332 s for the FNA (p < 0.001). There was a significant difference in the sensitivity: 82% [IC: 95% 72–89%] for the EUS-FNB and 71% [IC 95% 60–80%] pour l’EUS-FNA. | The diagnostic yields of FNB needle with forked tip were significantly better than that of FNA with a reduced time of pathology observation. |
| Lee et al. (2014) [17] | «Core biopsy needle versus standard aspiration needle for endoscopic ultrasound-guided sampling of solid pancreatic masses: a randomized parallel-group study» | Randomized controlled studies in parallel groups | Studies realized in South Korea of 116 patients with an average age of 63.1 years old for the FNA group and 66.7 years old for the FNB group, with a solid pancreatic masses. 61 men and 55 women. Total number of included patients: 116. | The patients with pancreatic masses were included in a prospective way and randomized, with 58 for the 22G EUS-FNB group (Echotip ProcoreTM, Cook Medical). and 58 for the 22G EUS-FNA (EchotipTM, Cook Medical) | The diagnostic precision was about 98.3% for the EUS-FNB and 94.8% for the EUS-FNA (p = 0.671). | The EUS-FNB needed a fewer number of median passes in comparison with the EUS-FNA (1 vs. 2; p < 0.001). | The diagnostic precision was the same for the 2 types of needles. However, there was less passes needed to establish the malignity diagnosis with the FNB. |
| Noh et al. (2017) [18] | «Comparison of 22-gauge standard fine needle versus core biopsy needle for endoscopic ultrasound-guided sampling of suspected pancreatic cancer: a randomized crossover trial» | Randomized crossed trial | Studies realized in South Korea of 60 patients aged between 18 and 80 years old with pancreatic masses. We can count 35 men and 25 women with an average age of 61.6 years old. Total number of included patients: 60. | A total of 60 patients with pancreatic cancers suspicion not resectable selected for a sampling guided by EUS were randomly allocated in two groups. 30 patients for 22G EUS-FNA (Olympus, Japan) and 30 patients for 22G EUS-FNB needles (EchotipProcoreTM, Cook Medical, Ireland) realized in random order. | FNA and FNB needles reported respectively a level of diagnostic precision of 95% and 93.3% (p = 0.564). | The EUS-FNB showed a better quality of sample than the EUS-FNA. | The diagnostic precision of the sampling guided by EUS for pancreatic cancer by using 22G FNA was comparable to that of FNB needles. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hassan, G.M.; Laporte, L.; Paquin, S.C.; Menard, C.; Sahai, A.V.; Mâsse, B.; Trottier, H. Endoscopic Ultrasound Guided Fine Needle Aspiration versus Endoscopic Ultrasound Guided Fine Needle Biopsy for Pancreatic Cancer Diagnosis: A Systematic Review and Meta-Analysis. Diagnostics 2022, 12, 2951. https://doi.org/10.3390/diagnostics12122951
Hassan GM, Laporte L, Paquin SC, Menard C, Sahai AV, Mâsse B, Trottier H. Endoscopic Ultrasound Guided Fine Needle Aspiration versus Endoscopic Ultrasound Guided Fine Needle Biopsy for Pancreatic Cancer Diagnosis: A Systematic Review and Meta-Analysis. Diagnostics. 2022; 12(12):2951. https://doi.org/10.3390/diagnostics12122951
Chicago/Turabian StyleHassan, Galab M., Louise Laporte, Sarto C. Paquin, Charles Menard, Anand V. Sahai, Benoît Mâsse, and Helen Trottier. 2022. "Endoscopic Ultrasound Guided Fine Needle Aspiration versus Endoscopic Ultrasound Guided Fine Needle Biopsy for Pancreatic Cancer Diagnosis: A Systematic Review and Meta-Analysis" Diagnostics 12, no. 12: 2951. https://doi.org/10.3390/diagnostics12122951
APA StyleHassan, G. M., Laporte, L., Paquin, S. C., Menard, C., Sahai, A. V., Mâsse, B., & Trottier, H. (2022). Endoscopic Ultrasound Guided Fine Needle Aspiration versus Endoscopic Ultrasound Guided Fine Needle Biopsy for Pancreatic Cancer Diagnosis: A Systematic Review and Meta-Analysis. Diagnostics, 12(12), 2951. https://doi.org/10.3390/diagnostics12122951