
Upfront Screening by Quantitative Real-Time PCR Assay Identifies NUP98::NSD1 Fusion Transcript in Indian AML Patients

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Collection
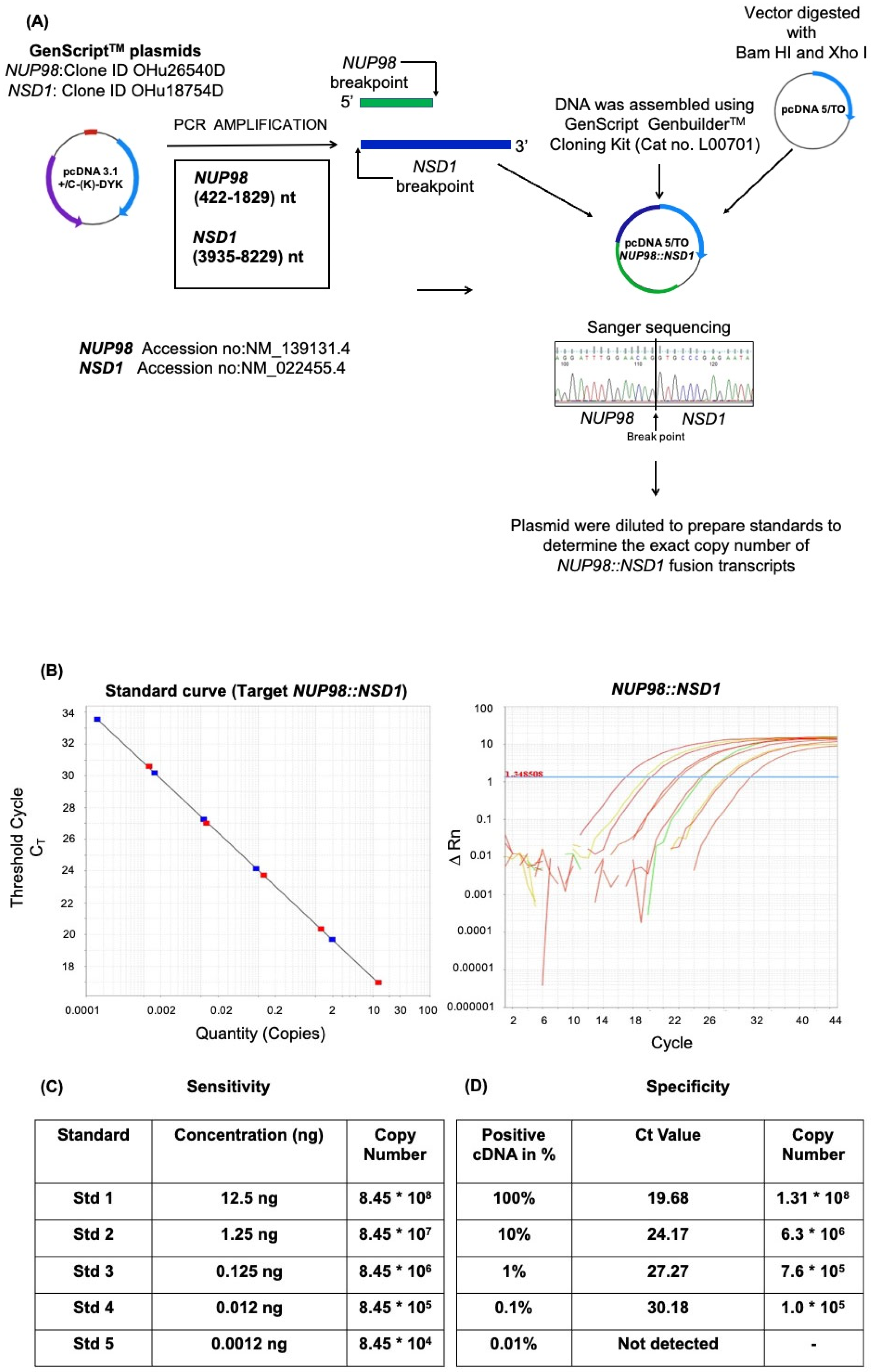
2.2. Plasmid Construction
2.3. Designing of Primers and Probes
2.4. Sensitivity of Assay
2.5. Specificity of the Assay
2.6. RNA Extraction and cDNA Preparation
2.7. Quantitative qRT-PCR
2.8. Statistical Data Analysis
2.9. Sanger’s Sequencing for Validation of NUP98-NSD1 Fusion
2.10. FLT3-ITD Fragment Analysis
3. Results
3.1. Development of a qRT-PCR Assay to Determine NUP98::NSD1 Fusion Transcript
3.2. Screening of Patients for the Presence of NUP98::NSD1 Fusion in the Indian Cohort
3.3. Sanger Sequencing Confirmation of NUP98::NSD1 Breakpoint Fusion
3.4. FLT3-ITD Status in NUP98::NSD1 Fusion Positive Patients
3.5. NUP98::NSD1 Fusion Patients Have Altered the Expression of Genes Associated with Self-Renewal and Differentiation
3.6. NUP98::NSD1 Patients Show Poor Responses to Induction Therapy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Morishita, M.; Mevius, D.; Di Luccio, E. In vitro histone lysine methylation by NSD1, NSD2/MMSET/WHSC1 and NSD3/WHSC1L. BMC Struct. Biol. 2014, 14, 25. [Google Scholar] [CrossRef] [Green Version]
- Faravelli, F. NSD1 mutations in Sotos syndrome. Am. J. Med. Genet. Part C Semin. Med. Genet. 2005, 137C, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Berdasco, M.; Ropero, S.; Setien, F.; Fraga, M.F.; Lapunzina, P.; Losson, R.; Alaminos, M.; Cheung, N.-K.; Rahman, N.; Esteller, M. Epigenetic inactivation of the Sotos overgrowth syndrome gene histone methyltransferase NSD1 in human neuroblastoma and glioma. Proc. Natl. Acad. Sci. USA 2009, 106, 21830–21835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farhangdoost, N.; Horth, C.; Hu, B.; Bareke, E.; Chen, X.; Li, Y.; Coradin, M.; Garcia, B.A.; Lu, C.; Majewski, J. Chromatin dysregulation associated with NSD1 mutation in head and neck squamous cell carcinoma. Cell Rep. 2021, 34, 108769. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Wang, K.; Liang, Q.; Tian, T.-T.; Zhong, Z. Role of NSD1 as potential therapeutic target in tumor. Pharmacol. Res. 2021, 173, 105888. [Google Scholar] [CrossRef]
- Su, X.; Zhang, J.; Mouawad, R.; Compérat, E.; Rouprêt, M.; Allanic, F.; Parra, J.; Bitker, M.-O.; Thompson, E.J.; Gowrishankar, B.; et al. NSD1 Inactivation and SETD2 Mutation Drive a Convergence toward Loss of Function of H3K36 Writers in Clear Cell Renal Cell Carcinomas. Cancer Res. 2017, 77, 4835–4845. [Google Scholar] [CrossRef] [Green Version]
- Taketani, T.; Taki, T.; Nakamura, H.; Taniwaki, M.; Masuda, J.; Hayashi, Y. NUP98–NSD3 fusion gene in radiation-associated myelodysplastic syndrome with t(8;11)(p11;p15) and expression pattern of NSD family genes. Cancer Genet. Cytogenet. 2009, 190, 108–112. [Google Scholar] [CrossRef]
- Tauchmann, S.; Schwaller, J. NSD1: A Lysine Methyltransferase between Developmental Disorders and Cancer. Life 2021, 11, 877. [Google Scholar] [CrossRef]
- Hollink, I.H.I.M.; Heuvel-Eibrink, M.M.V.D.; Arentsen-Peters, S.T.C.J.M.; Pratcorona, M.; Abbas, S.; Kuipers, J.E.; Van Galen, J.F.; Beverloo, H.B.; Sonneveld, E.; Kaspers, G.-J.J.L.; et al. NUP98/NSD1 characterizes a novel poor prognostic group in acute myeloid leukemia with a distinct HOX gene expression pattern. Blood 2011, 118, 3645–3656. [Google Scholar] [CrossRef] [Green Version]
- Ostronoff, F.; Othus, M.; Gerbing, R.B.; Loken, M.R.; Raimondi, S.C.; Hirsch, B.A.; Lange, B.J.; Petersdorf, S.; Radich, J.; Appelbaum, F.R.; et al. NUP98/NSD1 and FLT3/ITD coexpression is more prevalent in younger AML patients and leads to induction failure: A COG and SWOG report. Blood J. Am. Soc. Hematol. 2014, 124, 2400–2407. [Google Scholar] [CrossRef]
- Cerveira, N.; Correia, C.; Doria, S.; Bizarro, S.; Rocha, P.; Gomes, P.; Torres, L.; Norton, L.; Borges, B.S.; Castedo, S.; et al. Frequency of NUP98-NSD1 fusion transcript in childhood acute myeloid leukaemia. Leukemia 2003, 17, 2244–2247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimada, A.; Iijima-Yamashita, Y.; Tawa, A.; Tomizawa, D.; Yamada, M.; Norio, S.; Watanabe, T.; Taga, T.; Iwamoto, S.; Terui, K.; et al. Risk-stratified therapy for children with FLT3-ITD-positive acute myeloid leukemia: Results from the JPLSG AML-05 study. Int. J. Hematol. 2018, 107, 586–595. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.; Jawad, M.; Twigg, S.R.F.; Saracoglu, K.; Sauerbrey, A.; Thomas, A.E.; Eils, R.; Harbott, J.; Kearney, L. A cryptic t(5;11)(q35;p15.5) in 2 children with acute myeloid leukemia with apparently normal karyotypes, identified by a multiplex fluorescence in situ hybridization telomere assay. Blood 2002, 99, 2526–2531. [Google Scholar] [CrossRef] [Green Version]
- Jaju, R.J. A novel gene, NSD1, is fused to NUP98 in the t(5;11)(q35;p15.5) in de novo childhood acute myeloid leukemia. Blood 2001, 98, 1264–1267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, H.J.; Lee, J.H.; Lee, Y.E.; Baek, H.J.; Kook, H.; Park, J.H.; Lee, S.Y.; Choi, H.W.; Choi, H.J.; Kee, S.J.; et al. The First Korean Case of NUP98-NSD1 and a Novel SNRK-ETV6 Fusion in a Pediatric Therapy-related Acute Myeloid Leukemia Patient Detected by Targeted RNA Sequencing. Ann. Lab. Med. 2021, 41, 443–446. [Google Scholar] [CrossRef] [PubMed]
- Kitamura, H.; Tabe, Y.; Ai, T.; Tsuchiya, K.; Yuri, M.; Misawa, S.; Horii, T.; Kawaguchi, A.; Ohsaka, A.; Kimura, S. A new highly sensitive real-time quantitative-PCR method for detection of BCR-ABL1 to monitor minimal residual disease in chronic myeloid leukemia after discontinuation of imatinib. PLoS ONE 2019, 14, e0207170. [Google Scholar] [CrossRef] [Green Version]
- Test Details—BCR-ABL RNA PCR Quantitation for Leukemia. Available online: https://knightdxlabs.ohsu.edu/home/test-details?id=BCR-ABL+RNA+PCR+Quantitation+for+Leukemia (accessed on 10 September 2022).
- Chaturvedi, C.-P.; Hosey, A.M.; Palii, C.; Perez-Iratxeta, C.; Nakatani, Y.; Ranish, J.A.; Dilworth, F.J.; Brand, M. Dual role for the methyltransferase G9a in the maintenance of β-globin gene transcription in adult erythroid cells. Proc. Natl. Acad. Sci. USA 2009, 106, 18303–18308. [Google Scholar] [CrossRef] [Green Version]
- Niktoreh, N.; Walter, C.; Zimmermann, M.; von Neuhoff, C.; von Neuhoff, N.; Rasche, M.; Waack, K.; Creutzig, U.; Hanenberg, H.; Reinhardt, D. Mutated WT1, FLT3-ITD, and NUP98-NSD1 Fusion in Various Combinations Define a Poor Prognostic Group in Pediatric Acute Myeloid Leukemia. J. Oncol. 2019, 2019, 1609128. [Google Scholar] [CrossRef] [Green Version]
- Petit, A.; Radford, I.; Waill, M.-C.; Romana, S.P.; Berger, R. NUP98–NSD1 fusion by insertion in acute myeloblastic leukemia. Cancer Genet. Cytogenet. 2008, 180, 43–46. [Google Scholar] [CrossRef]
- Struski, S.; Lagarde, S.; Bories, P.; Puiseux, C.; Prade, N.; Cuccuini, W.; Pages, M.-P.; Bidet, A.; Gervais, C.; Lafage-Pochitaloff, M.; et al. NUP98 is rearranged in 3.8% of pediatric AML forming a clinical and molecular homogenous group with a poor prognosis. Leukemia 2016, 31, 565–572. [Google Scholar] [CrossRef]
- Wang, G.G.; Cai, L.; Pasillas, M.P.; Kamps, M.P. NUP98–NSD1 links H3K36 methylation to Hox-A gene activation and leukaemogenesis. Nat. Cell Biol. 2007, 9, 804–812. [Google Scholar] [CrossRef] [PubMed]
- Shiba, N.; Ichikawa, H.; Taki, T.; Park, M.-J.; Jo, A.; Mitani, S.; Kobayashi, T.; Shimada, A.; Sotomatsu, M.; Arakawa, H.; et al. NUP98-NSD1gene fusion and its related gene expression signature are strongly associated with a poor prognosis in pediatric acute myeloid leukemia. Genes Chromosomes Cancer 2013, 52, 683–693. [Google Scholar] [CrossRef] [PubMed]
- Döhner, H.; Estey, E.; Grimwade, D.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Larson, R.A.; et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kivioja, J.L.; Martí, J.M.L.; Kumar, A.; Kontro, M.; Edgren, H.; Parsons, A.; Lundán, T.; Wolf, M.; Porkka, K.; Heckman, C.A. Chimeric NUP98–NSD1 transcripts from the cryptic t(5;11)(q35.2;p15.4) in adult de novo acute myeloid leukemia. Leuk. Lymphoma 2017, 59, 725–732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akiki, S.; Dyer, S.A.; Grimwade, D.; Ivey, A.; Abou-Zeid, N.; Borrow, J.; Jeffries, S.; Caddick, J.; Newell, H.; Begum, S.; et al. NUP98-NSD1 fusion in association withFLT3-ITD mutation identifies a prognostically relevant subgroup of pediatric acute myeloid leukemia patients suitable for monitoring by real time quantitative PCR. Genes Chromosomes Cancer 2013, 52, 1053–1064. [Google Scholar] [CrossRef]
- Thanasopoulou, A.; Tzankov, A.; Schwaller, J. Potent co-operation between the NUP98-NSD1 fusion and the FLT3-ITD mutation in acute myeloid leukemia induction. Haematologica 2014, 99, 1465–1471. [Google Scholar] [CrossRef] [Green Version]
- Yamato, G.; Yamaguchi, H.; Handa, H.; Shiba, N.; Kawamura, M.; Wakita, S.; Inokuchi, K.; Hara, Y.; Ohki, K.; Okubo, J.; et al. Clinical features and prognostic impact of PRDM16 expression in adult acute myeloid leukemia. Genes Chromosomes Cancer 2017, 56, 800–809. [Google Scholar] [CrossRef]
- Shiba, N.; Ohki, K.; Kobayashi, T.; Hara, Y.; Yamato, G.; Tanoshima, R.; Ichikawa, H.; Tomizawa, D.; Park, M.-J.; Shimada, A.; et al. High PRDM16 expression identifies a prognostic subgroup of pediatric acute myeloid leukaemia correlated to FLT3-ITD, KMT2A-PTD, and NUP98-NSD1: The results of the Japanese Paediatric Leukaemia/Lymphoma Study Group AML-05 trial. Br. J. Haematol. 2015, 172, 581–591. [Google Scholar] [CrossRef]
- Lavallée, V.P.; Lemieux, S.; Boucher, G.; Gendron, P.; Boivin, I.; Girard, S.; Hebert, J.; Sauvageau, G. Identification of MYC mutations in acute myeloid leukemias with NUP98-NSD1 translocations. Leukemia 2016, 30, 1621–1624. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Cloning Primers | |
|---|---|
| NUP98::NSD1 fusion forward | 5′AAAGATCATGACATAGATTACAAGGATGACGATGA CAAGGCCATGTTTAACAAATCATTTGGAACACC-3′ |
| NUP98::NSD1 fusion reverse | 5′AGTCGAGGCTGATCAGCGGGTTTAAACGGGCC CTCTAGACCTACTTCTGTTCTGATTCTGCACACTT-3′ |
| Sequencing Primers | |
| NUP98-Seq F | 5′-ACTCTTGGAACTGGGCTTGG-3′ |
| NSD1-Seq R | 5′-GGCTAGAAGGCTTTCCTCTTC-3′ |
| qRT-PCR primers | |
| NUP98 t(5,11) F | 5′-GGCCCCTGGATTTAATACTACGA-3′ |
| NSD1 t(5,11)R | 5′-CTTCCTAAGGCGTTTCTTCTCTGA-3′ |
| NUP98-NSD1 t(5,11) probe | 5′-FAM-TTTGGAGCCCCCCAGGCC-MGB NFQ-3′ |
| ABL1-F | 5′-CCCAGAGAAGGTCTATGAACTCATG-3′ |
| ABL1-R | 5′-AGGAGGGCCGGTCAGA-3′ |
| ABL1 probe | 5′-VIC-TCCACTGCCAACATGC-MGB NFQ-3′ |
| HOXA1 F | 5′-CCCTCGGACCATAGGATTACAA-3′ |
| HOXA1 R | 5′-GCCGCCGCAACTGTTG-3′ |
| HOXA3 F | 5′-CGACAGCTCGGCGATCTAC-3′ |
| HOXA3 R | 5′-CGGGTACGGCTGCTGATT-3′ |
| HOXA4 F | 5′-GGTGGTGTACCCCTGGATGA-3′ |
| HOXA4 R | 5′-GACTTGCTGCCGGGTATAGG-3′ |
| HOXA5 F | 5′-GGAGTTCCACTTCAACCGTTACC-3′ |
| HOXA5 R | 5′-CGGAGAGGCAAAGAGCATGT-3′ |
| HOXA6 F | 5′-GTCTGGTAGCGCGTGTAGGT-3′ |
| HOXA6 R | 5′-CCCTGTTTACCCCTGGATG-3′ |
| HOXA7 F | 5′-CTTCTCCAGTTCCAGCGTCT-3′ |
| HOXA7 R | 5′-AAGCCAGTTTCCGCATCTAC-3′ |
| HOXA9 F | 5′-CCACGCTTGACACTCACACT-3′ |
| HOXA9 R | 5′-GCTCTCATTCTCGGCATTGT-3′ |
| HOXA10 F | 5′-TCTTTGCTGTGAGCCAGTTG-3′ |
| HOXA10 R | 5′-CTCCAGCCCCTTCAGAAAAC-3′ |
| HOXA11 F | 5′-CGGCCACACTGAGGACAAG-3′ |
| HOXA11 R | 5′-AACTCTCGCTCCAGCTCTCG-3′ |
| HOXB6 F | 5′-TCCCCTCCCAATGAGTTCCT-3′ |
| HOXB6 R | 5′-ACTCCTGCCCGCTGGC-3′ |
| PRDM16 F | 5′-TGCCGCACGCAGATCA-3′ |
| PRDM16 R | 5′-GGGAGGAGGTAGTGCTGAACAT-3′ |
| MECOM F | 5′-CGGAGTGTGGCAAAACGTT-3′ |
| MECOM R | 5′-GCTGTGGATGTGCTTGTGTTGT-3′ |
| NKX2-3 F | 5′-GGTTCCAGAATCGCAGGTACAA-3′ |
| NKX2-3 R | 5′-GCGCCAAGCTCCAGAGACT-3′ |
| VENTX F | 5′-GGCTGGCCAGGGAGATG-3′ |
| VENTX R | 5′-TGCGGCGATTCTGAAACC-3′ |
| UTF F | 5′-GACCAGCTGCTGACCTTGAA-3′ |
| UTF R | 5′-CTGCCCAGAATGAAGCCCA-3′ |
| ASL F | 5′-CAGCATGGATGCCACTAGTGA-3′ |
| ASL R | 5′-CACAGCGAAGCCCAGAACA-3′ |
| GAPDH F | 5′-AATCCCATCACCATCTTCCA-3′ |
| GAPDH R | 5′-TGGACTCCACGACGTACTCA-3′ |
| Fragment analysis primers | |
| FLT3 exon14 F | 5′-FAM-AGCAATTTAGGTATGAAAGCCAGCTA-3′ |
| FLT3 exon14 R | 5′-CTTTCAGCATTTTGACGGCAACC-3′ |
| Patient No. | Age (in Years) | Sex | FAB | WBC Count at Diagnosis (WBC Count /L) | BM Blast (%) | FLT3-ITD Status | Treatment Protocol | Induction Chemo Response | HSCT | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|
| Adult #1 | 57 | M | M4 | 19.2 * 109 | 70% | FLT3-ITD Positive (AR 0.35) | 3 + 7 f/b HAM | Induction failure | No | Expired due to severe sepsis & respiratory failure |
| Adult #2 | 64 | F | M2 | 12.8 * 109 | 95% | FLT3-ITD Positive (AR 0.35) | Azacitidine + Venetoclax f/b HAM | Induction failure | No | Died due to disease progression |
| Adult #3 | 33 | M | M3 | 20 * 109 | 95% | FLT3-ITD Positive (AR 0.31) | 3 + 7 + Midostaurin | Induction failure | No | Died due to intracranial bleed. |
| Pediatric #1 | 15 | M | M2 | 19.9 * 109 | 55% | FLT3-ITD Positive (AR 0.36) | 3 + 7 + Midostaurin | Achieved remission | Yes | Disease relapsed 7 months after allogenic stem cell transplant |
| Pediatric #2 | 15 | F | M2 | 18.6 * 109 | 71% | FLT3-ITD Positive (AR 0.21) | 3 + 7 + Midostaurin | Induction failure | No | Expired due to MDR sepsis (kliebsella pneumoniae) |
| Pediatric #3 | 12 | F | M1 | 17.9 * 109 | 90% | FLT3-ITD Positive (AR 0.37) | 3 + 7 + Midostaurin f/b HAM+ Midostaurin | Induction failure | Yes | Disease relapsed 4 months after allogenic stem cell transplant |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shah, A.; Sharma, A.; Katiyar, S.; Gupta, A.; Chaturvedi, C.P. Upfront Screening by Quantitative Real-Time PCR Assay Identifies NUP98::NSD1 Fusion Transcript in Indian AML Patients. Diagnostics 2022, 12, 3001. https://doi.org/10.3390/diagnostics12123001
Shah A, Sharma A, Katiyar S, Gupta A, Chaturvedi CP. Upfront Screening by Quantitative Real-Time PCR Assay Identifies NUP98::NSD1 Fusion Transcript in Indian AML Patients. Diagnostics. 2022; 12(12):3001. https://doi.org/10.3390/diagnostics12123001
Chicago/Turabian StyleShah, Arunim, Akhilesh Sharma, Shobhita Katiyar, Anshul Gupta, and Chandra Prakash Chaturvedi. 2022. "Upfront Screening by Quantitative Real-Time PCR Assay Identifies NUP98::NSD1 Fusion Transcript in Indian AML Patients" Diagnostics 12, no. 12: 3001. https://doi.org/10.3390/diagnostics12123001
APA StyleShah, A., Sharma, A., Katiyar, S., Gupta, A., & Chaturvedi, C. P. (2022). Upfront Screening by Quantitative Real-Time PCR Assay Identifies NUP98::NSD1 Fusion Transcript in Indian AML Patients. Diagnostics, 12(12), 3001. https://doi.org/10.3390/diagnostics12123001