
Diagnostic Performance of Point Shear Wave Elastography (pSWE) Using Acoustic Radiation Force Impulse (ARFI) Technology in Mesenteric Masses: A Feasibility Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ultrasound Examinations
2.2. Acoustic Radiation Force Impulse Examinations
2.3. Statistical Analysis
3. Results
3.1. Demographic and Clinical Data
3.2. B-Mode Ultrasound Data
3.3. Acoustic Radiation Force Impulse Examinations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Coffey, J.C.; O’Leary, D.P. The mesentery: Structure, function, and role in disease. Lancet Gastroenterol. Hepatol. 2016, 1, 238–247. [Google Scholar] [CrossRef]
- Dufay, C.; Abdelli, A.; Le Pennec, V.; Chiche, L. Mesenteric tumors: Diagnosis and treatment. J. Visc. Surg. 2012, 149, e239–e251. [Google Scholar] [CrossRef] [PubMed]
- Danford, C.J.; Lin, S.C.; Wolf, J.L. Sclerosing Mesenteritis. Am. J. Gastroenterol. 2019, 114, 867–873. [Google Scholar] [CrossRef]
- Diab, R.; Virarkar, M.; Saleh, M.; Elsheif, S.; Javadi, S.; Bhosale, P.; Faria, S. Imaging spectrum of mesenteric masses. Abdom. Radiol. 2020, 45, 3618–3636. [Google Scholar] [CrossRef]
- Aslan, S.; Nural, M.S. CT features of asymptomatic heterotopic pancreas in jejunal mesentery. Turk. J. Gastroenterol. 2019, 30, 208–210. [Google Scholar] [CrossRef] [PubMed]
- Winant, A.J.; Vora, A.; Ginter, P.S.; Levine, M.S.; Brylka, D.A. More than just metastases: A practical approach to solid mesenteric masses. Abdom. Imaging 2014, 39, 605–621. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.P.; Arnoletti, J.P.; Varadarajulu, S.; Morgan, D.E. Post-pancreatitis Fat Necrosis Mimicking Carcinomatosis. Radiol. Case Rep. 2008, 3, 192. [Google Scholar] [CrossRef] [Green Version]
- Gottschalk, U.; Nitzsche, C.; Felber, J.; Dietrich, C.F. Enteroscopy and imaging in sclerosing mesenteritis. Z. Gastroenterol. 2012, 50, 1013–1017. [Google Scholar] [CrossRef]
- Zissin, R.; Metser, U.; Hain, D.; Even-Sapir, E. Mesenteric panniculitis in oncologic patients: PET-CT findings. Br. J. Radiol. 2006, 79, 37–43. [Google Scholar] [CrossRef]
- Nakatani, K.; Nakamoto, Y.; Togashi, K. FDG-PET/CT assessment of misty mesentery: Feasibility for distinguishing viable mesenteric malignancy from stable conditions. Eur. J. Radiol. 2013, 82, e380–e385. [Google Scholar] [CrossRef] [Green Version]
- Trenker, C.; Safai Zadeh, E.; Petzold, G.; Görg, C.; Neesse, A. Mesenteric Masses on 2D Mode and Contrast-Enhanced Ultrasound: A Retrospective Study in 69 Patients. Ultraschall Med.-Eur. J. Ultrasound 2017, 38, 655–660. [Google Scholar] [CrossRef] [PubMed]
- Safai Zadeh, E.; Kindermann, J.; Dietrich, C.F.; Görg, C.; Bleyl, T.; Alhyari, A.; Trenker, C. Clinical Awareness and Acceptance of Sonographically Diagnosed Epiploic Appendagitis (EA): A Retrospective Analysis of EA in a Single Tertiary Academic Referral Center. Ultrasound Int. Open 2020, 6, E87–E93. [Google Scholar] [CrossRef] [PubMed]
- Safai Zadeh, E.; Beutel, B.; Dietrich, C.F.; Keber, C.U.; Huber, K.P.; Görg, C.; Trenker, C. Perfusion Patterns of Peripheral Pulmonary Lesions in COVID-19 Patients Using Contrast-Enhanced Ultrasound (CEUS). J. Ultrasound Med. 2021, 40, 2403–2411. [Google Scholar] [CrossRef] [PubMed]
- Safai Zadeh, E.; Dietrich, C.F.; Amjad, A.; Trenker, C.; Görg, C. Transcutaneous B-Mode Ultrasound (TUS) and contrast-enhanced ultrasound (CEUS) pattern of mediastinal tumors: A Pictorial Essay. J. Ultrason. 2021, 21, e340–e347. [Google Scholar] [CrossRef]
- Safai Zadeh, E.; Görg, C.; Dietrich, C.F.; Görlach, J.; Alhyari, A.; Trenker, C. Contrast-Enhanced Ultrasound for Evaluation of Pleural Effusion: A Pictorial Essay. J. Ultrasound Med. 2021, 41, 485–503. [Google Scholar] [CrossRef]
- Safai Zadeh, E.; Keber, C.U.; Dietrich, C.F.; Westhoff, C.C.; Günter, C.; Beutel, B.; Alhyari, A.; Trenker, C.; Görg, C. Perfusion Patterns of Peripheral Pulmonary Granulomatous Lesions Using Contrast-Enhanced Ultrasound (CEUS) and Their Correlation with Immunohistochemically Detected Vascularization Patterns. J. Ultrasound Med. 2021, 41, 565–574. [Google Scholar] [CrossRef]
- Safai Zadeh, E.; Weide, J.; Dietrich, C.F.; Trenker, C.; Koczulla, A.R.; Görg, C. Diagnostic Accuracy of B-Mode- and Contrast-Enhanced Ultrasound in Differentiating Malignant from Benign Pleural Effusions. Diagnostics 2021, 11, 1293. [Google Scholar] [CrossRef]
- Safai Zadeh, E.; Westhoff, C.C.; Keber, C.U.; Trenker, C.; Dietrich, C.F.; Alhyari, A.; Mohr, C.G.L.; Görg, C. Perfusion Patterns of Peripheral Organizing Pneumonia (POP) Using Contrast-Enhanced Ultrasound (CEUS) and Their Correlation with Immunohistochemically Detected Vascularization Patterns. Diagnostics 2021, 11, 1601. [Google Scholar] [CrossRef]
- Safai Zadeh, E.; Dietrich, C.F.; Kmoth, L.; Trenker, C.; Alhyari, A.; Ludwig, M.; Görg, C. Peripheral Pulmonary Lesions in Confirmed Pulmonary Arterial Embolism: Follow-up Study of B-Mode Ultrasound and of Perfusion Patterns Using Contrast-Enhanced Ultrasound (CEUS). J. Ultrasound Med. 2021. [Google Scholar] [CrossRef]
- Findeisen, H.; Görg, C.; Hartbrich, R.; Dietrich, C.F.; Görg, K.; Trenker, C.; Safai Zadeh, E. Contrast-enhanced ultrasound is helpful for differentiating benign from malignant parietal pleural lesions. J. Clin. Ultrasound 2021, 50, 90–98. [Google Scholar] [CrossRef]
- Săftoiu, A.; Gilja, O.H.; Sidhu, P.S.; Dietrich, C.F.; Cantisani, V.; Amy, D.; Bachmann-Nielsen, M.; Bob, F.; Bojunga, J.; Brock, M.; et al. The EFSUMB Guidelines and Recommendations for the Clinical Practice of Elastography in Non-Hepatic Applications: Update 2018. Ultraschall Med. 2019, 40, 425–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dietrich, C.F.; Bamber, J.; Berzigotti, A.; Bota, S.; Cantisani, V.; Castera, L.; Cosgrove, D.; Ferraioli, G.; Friedrich-Rust, M.; Gilja, O.H.; et al. EFSUMB Guidelines and Recommendations on the Clinical Use of Liver Ultrasound Elastography, Update 2017 (Long Version). Ultraschall Med. 2017, 38, e16–e47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferraioli, G.; Barr, R.G.; Farrokh, A.; Radzina, M.; Cui, X.W.; Dong, Y.; Rocher, L.; Cantisani, V.; Polito, E.; D’Onofrio, M.; et al. How to perform shear wave elastography. Part I. Med. Ultrason. 2022, 24, 95–106. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, C.F.; Burmeister, S.; Hollerbach, S.; Arcidiacono, P.G.; Braden, B.; Fusaroli, P.; Hocke, M.; Iglesias-Garcia, J.; Kitano, M.; Larghi, A.; et al. Do we need elastography for EUS? Endosc. Ultrasound 2020, 9, 284–290. [Google Scholar] [CrossRef]
- Dietrich, C.F.; Ferraioli, G.; Sirli, R.; Popescu, A.; Sporea, I.; Pienar, C.; Kunze, C.; Taut, H.; Schrading, S.; Bota, S.; et al. General advice in ultrasound based elastography of pediatric patients. Med. Ultrason. 2019, 21, 315–326. [Google Scholar] [CrossRef] [Green Version]
- Dietrich, C.F.; Hocke, M. Elastography of the Pancreas, Current View. Clin. Endosc. 2019, 52, 533–540. [Google Scholar] [CrossRef] [Green Version]
- D’Onofrio, M.; Crosara, S.; De Robertis, R.; Canestrini, S.; Demozzi, E.; Gallotti, A.; Pozzi Mucelli, R. Acoustic radiation force impulse of the liver. World J. Gastroenterol. 2013, 19, 4841–4849. [Google Scholar] [CrossRef]
- Heese, F.; Görg, C. The value of highest quality ultrasound as a reference for ultrasound diagnosis. Ultraschall Med. 2006, 27, 220–224. [Google Scholar] [CrossRef]
- Barr, R.G.; Ferraioli, G.; Palmeri, M.L.; Goodman, Z.D.; Garcia-Tsao, G.; Rubin, J.; Garra, B.; Myers, R.P.; Wilson, S.R.; Rubens, D.; et al. Elastography Assessment of Liver Fibrosis: Society of Radiologists in Ultrasound Consensus Conference Statement. Radiology 2015, 276, 845–861. [Google Scholar] [CrossRef] [Green Version]
- Alhyari, A.; Görg, C.; Dietrich, C.F.; Trenker, C.; Ludwig, M.; Safai Zadeh, E. Diagnostic Performance of Point Shear Wave Elastography Using Acoustic Radiation Force Impulse Technology in Peripheral Pulmonary Consolidations: A Feasibility Study. Ultrasound Med. Biol. 2022, S0301-5629(22)00003-5. [Google Scholar] [CrossRef]
- Dalla Pria, H.R.F.; Torres, U.S.; Velloni, F.; Santiago, R.A.; Zacarias, M.S.; Silva, L.F.D.; Tamamoto, F.; Walsh, D.; von Atzingen, A.C.; Coffey, J.C.; et al. The Mesenteric Organ: New Anatomical Concepts and an Imaging-based Review on Its Diseases. Semin. Ultrasound CT MR 2019, 40, 515–532. [Google Scholar] [CrossRef] [PubMed]
- Ozturk, A.; Grajo, J.R.; Dhyani, M.; Anthony, B.W.; Samir, A.E. Principles of ultrasound elastography. Abdom. Radiol. 2018, 43, 773–785. [Google Scholar] [CrossRef] [PubMed]
- Șirli, R.; Popescu, A.; Sporea, I. Liver Fibrosis Assessment by Point Shear-Wave Elastography Techniques. In Ultrasound Elastography; IntechOpen: London, UK, 2019. [Google Scholar] [CrossRef] [Green Version]
- Petzold, G.; Hofer, J.; Ellenrieder, V.; Neesse, A.; Kunsch, S. Liver Stiffness Measured by 2-Dimensional Shear Wave Elastography: Prospective Evaluation of Healthy Volunteers and Patients With Liver Cirrhosis. J. Ultrasound Med. 2019, 38, 1769–1777. [Google Scholar] [CrossRef] [PubMed]
- Kiani, A.; Brun, V.; Lainé, F.; Turlin, B.; Morcet, J.; Michalak, S.; Le Gruyer, A.; Legros, L.; Bardou-Jacquet, E.; Gandon, Y.; et al. Acoustic radiation force impulse imaging for assessing liver fibrosis in alcoholic liver disease. World J. Gastroenterol. 2016, 22, 4926–4935. [Google Scholar] [CrossRef] [PubMed]
- Tachi, Y.; Hirai, T.; Kojima, Y.; Miyata, A.; Ohara, K.; Ishizu, Y.; Honda, T.; Kuzuya, T.; Hayashi, K.; Ishigami, M.; et al. Liver stiffness measurement using acoustic radiation force impulse elastography in hepatitis C virus-infected patients with a sustained virological response. Aliment Pharm. Ther. 2016, 44, 346–355. [Google Scholar] [CrossRef] [PubMed]
- Bob, F.; Bota, S.; Sporea, I.; Sirli, R.; Petrica, L.; Schiller, A. Kidney shear wave speed values in subjects with and without renal pathology and inter-operator reproducibility of acoustic radiation force impulse elastography (ARFI)—Preliminary results. PLoS ONE 2014, 9, e113761. [Google Scholar] [CrossRef] [Green Version]
- Li, G.; Li, D.-W.; Fang, Y.-X.; Song, Y.-J.; Deng, Z.-J.; Gao, J.; Xie, Y.; Yin, T.-S.; Ying, L.; Tang, K.-F. Performance of Shear Wave Elastography for Differentiation of Benign and Malignant Solid Breast Masses. PLoS ONE 2013, 8, e76322. [Google Scholar] [CrossRef]
- Liu, B.; Liang, J.; Zheng, Y.; Xie, X.; Huang, G.; Zhou, L.; Wang, W.; Lu, M. Two-dimensional shear wave elastography as promising diagnostic tool for predicting malignant thyroid nodules: A prospective single-centre experience. Eur. Radiol. 2015, 25, 624–634. [Google Scholar] [CrossRef]
- Zhan, J.; Jin, J.-M.; Diao, X.-H.; Chen, Y. Acoustic radiation force impulse imaging (ARFI) for differentiation of benign and malignant thyroid nodules—A meta-analysis. Eur. J. Radiol. 2015, 84, 2181–2186. [Google Scholar] [CrossRef]
- Horton, K.M.; Lawler, L.P.; Fishman, E.K. CT findings in sclerosing mesenteritis (panniculitis): Spectrum of disease. Radiographics 2003, 23, 1561–1567. [Google Scholar] [CrossRef]
- Green, M.S.; Chhabra, R.; Goyal, H. Sclerosing mesenteritis: A comprehensive clinical review. Ann. Transl. Med. 2018, 6, 336. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.J.; Ding, H.; Mao, F.; Sun, H.C.; Xu, C.; Wang, W.P. Assessment of liver fibrosis with elastography point quantification technique in chronic hepatitis B virus patients: A comparison with liver pathological results. J. Gastroenterol. Hepatol. 2014, 29, 814–819. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MM Subgroup |
Malignant Hematological MM |
Malignant Non-Hematological MM |
Benign Inflammatory MM (Mesenteritis) | Mesenteric Lipomatosis |
Other Benign Masses |
|---|---|---|---|---|---|
| No. of lesions | (n = 15) | (n = 17) | (n = 26) | (n = 8) | (n = 3) |
| Etiology | - Lymphoma (14) - Chloroma (1) | - Desmoid fibromatosis (2) - GIST (3) - CRC (2) - NET (3) - PDAC (1) - Liposarcoma (2) - Merkel cell carcinoma (1) - Gastric carcinoma (1) - Follicular thyroid carcinoma (1) - Ovarian carcinoma (1) | - Sclerosing mesenteritis (15) - Mesenteric involvement in Crohn’s disease (4) - Fat necrosis in necrotizing pancreatitis (2) - Mesenteritis in acute edematous pancreatitis (1) - Mesenteritis due to perforated bowel (2) - Non-specific (2) | - Mesenteric fat bulk (8) | - Heterotopic pancreas (2) - Lipoma (1) |
| Subgroup | Number of Lesions (n) | ARFI Velocity (m/s) | Average Depth of Measurement (Mean ± SD in cm) | ||
|---|---|---|---|---|---|
| Mean ± SD | Minimum | Maximum | |||
| bMMs | 37 | 1.59 ± 0.93 | 0.59 | 3.62 | 4.75 ± 1.20 |
| Mesenteritis | 26 | 1.75 ± 1.02 | 0.59 | 3.62 | 4.53 ± 0.99 |
| Mesenteric fat bulk | 8 | 0.90 ± 0.24 | 0.67 | 1.35 | 5.43 ± 1.65 |
| Other benign masses | 3 | 1.99 ± 0.13 | 1.86 | 2.12 | 4.83 ± 1.26 |
| mMMs | 32 | 2.76 ± 1.01 | 0.77 | 4.22 | 4.25 ± 0.80 |
| Non-hematological | 17 | 2.79 ± 1.03 | 1.18 | 4.22 | 4.07 ± 0.80 |
| Hematological | 15 | 2.73 ± 1.03 | 0.77 | 4.18 | 4.47 ± 0.78 |
| Author | Number of Patients | Imaging Modality | Parameter Predictive of Malignancy | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | p-Value |
|---|---|---|---|---|---|---|---|---|
| Trenker et al., (2017) [11] * | 69 | B-mode US | Hypoechoic or complex echogenicity | 94 | 50 | 80 | 79 | <0.001 |
| Regular borders | 81 | 68 | 84 | 63 | <0.05 | |||
| Trenker et al., (2017) [11] * | 69 | CEUS | Parenchymal phase washout | 75 | 59 | 80 | 52 | <0.05 |
| Nakatani et al., (2013) [12] ** | 71 | PET-CT | Diammax > 10 mm | 69 | 98 | 90 | 93 | <0.001 |
| SUVmax ≥ 3.0 | 85 | 98 | 92 | 96 | <0.001 | |||
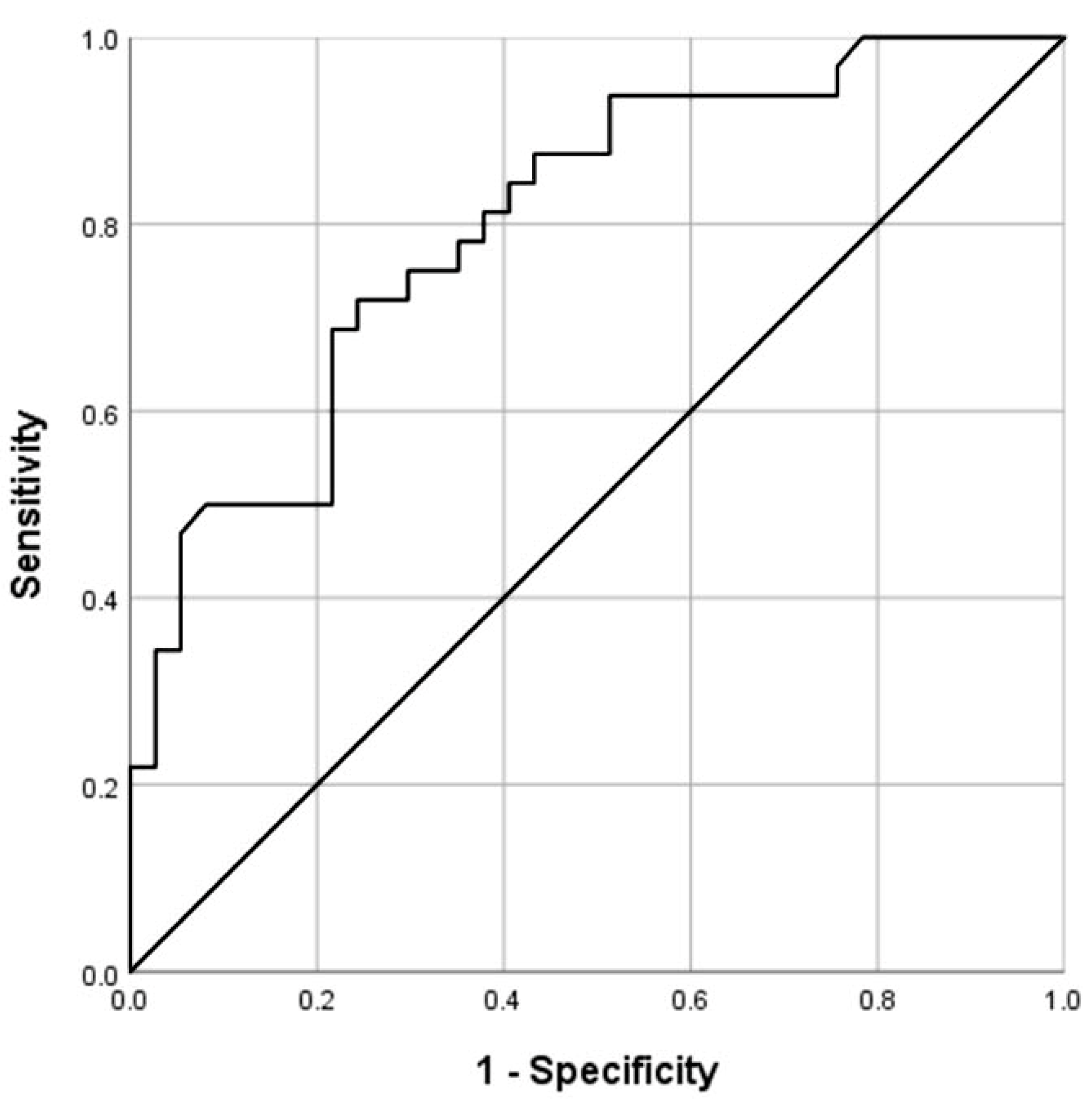
| Present study | 69 | ARFI elastography | Mean velocity > 2.05 m/s | 75 | 70 | 69 | 77 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhyari, A.; Görg, C.; Dietrich, C.F.; Kawohl, S.; Safai Zadeh, E. Diagnostic Performance of Point Shear Wave Elastography (pSWE) Using Acoustic Radiation Force Impulse (ARFI) Technology in Mesenteric Masses: A Feasibility Study. Diagnostics 2022, 12, 523. https://doi.org/10.3390/diagnostics12020523
Alhyari A, Görg C, Dietrich CF, Kawohl S, Safai Zadeh E. Diagnostic Performance of Point Shear Wave Elastography (pSWE) Using Acoustic Radiation Force Impulse (ARFI) Technology in Mesenteric Masses: A Feasibility Study. Diagnostics. 2022; 12(2):523. https://doi.org/10.3390/diagnostics12020523
Chicago/Turabian StyleAlhyari, Amjad, Christian Görg, Christoph Frank Dietrich, Svenja Kawohl, and Ehsan Safai Zadeh. 2022. "Diagnostic Performance of Point Shear Wave Elastography (pSWE) Using Acoustic Radiation Force Impulse (ARFI) Technology in Mesenteric Masses: A Feasibility Study" Diagnostics 12, no. 2: 523. https://doi.org/10.3390/diagnostics12020523
APA StyleAlhyari, A., Görg, C., Dietrich, C. F., Kawohl, S., & Safai Zadeh, E. (2022). Diagnostic Performance of Point Shear Wave Elastography (pSWE) Using Acoustic Radiation Force Impulse (ARFI) Technology in Mesenteric Masses: A Feasibility Study. Diagnostics, 12(2), 523. https://doi.org/10.3390/diagnostics12020523