
The Importance of Cardiac Computed Tomography in the Diagnosis of Caseous Calcification of the Mitral Annulus—Case Reports



{kind=link}
{kind=link}
Abstract
:1. Introduction
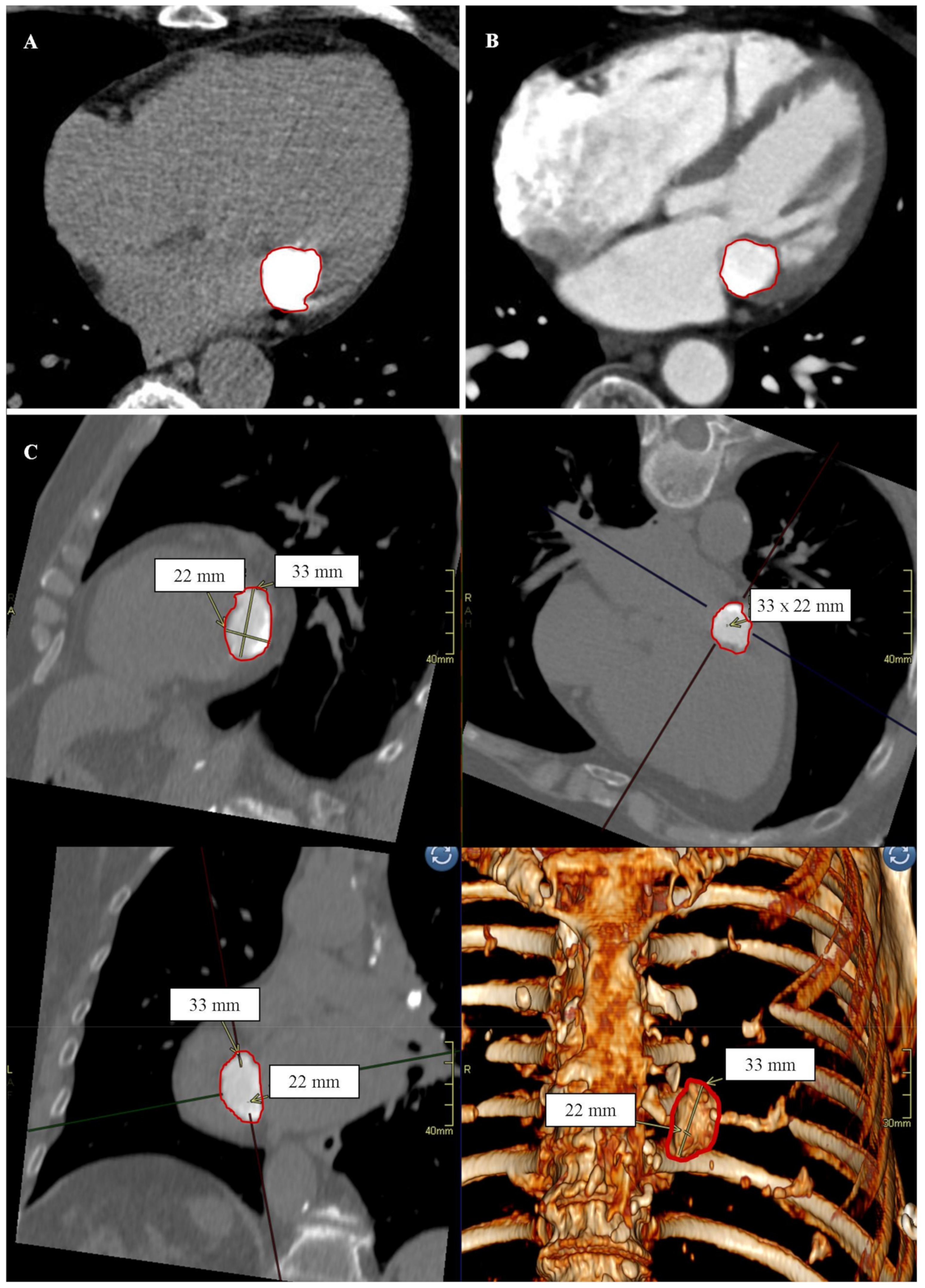
2. Case Reports
2.1. Patient No. 1
2.2. Patient No. 2
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Curl, E.; Riemer, E. Caseous calcification of the mitral annulus: Case report and brief review. Eur. Hear. J. Case Rep. 2018, 2, yty124. [Google Scholar] [CrossRef] [PubMed]
- Pomerance, A. Pathological and clinical study of calcification of the mitral valve ring. J. Clin. Pathol. 1970, 23, 354–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-De-Alegria, A.; Rubio-Alvarez, J.; Baleato-González, S. Caseous Calcification of the Mitral Annulus: A Rare Cause of Intracardiac Mass. Case Rep. Radiol. 2012, 2012, 596962. [Google Scholar] [CrossRef] [PubMed]
- Carpentier, A.F.; Pellerin, M.; Fuzellier, J.-F.; Relland, J.Y. Extensive calcification of the mitral valve anulus: Pathology and surgical management. J. Thorac. Cardiovasc. Surg. 1996, 111, 718–730. [Google Scholar] [CrossRef] [Green Version]
- Goodman, H.B.; Dorney, E.R. Marfan’s syndrome with massive calcification of the mitral annulus at age twenty-six. Am. J. Cardiol. 1969, 24, 426–431. [Google Scholar] [CrossRef]
- Michałowska, I.; Szymański, P.; Kwiatek, P.; Spałek, M.; Furmanek, M.; Zieliński, P.; Kochańska, S.; Lipczyńska, M. Caseous calcification of the mitral annulus—The complementary role of computed tomography and transthoracic echocardiogram. Pol. J. Radiol. 2018, 83, e621–e626. [Google Scholar] [CrossRef] [PubMed]
- García-Ibarrondo, N.; Lang, R.M. Calcificación caseosa del anillo mitral, un raro hallazgo ecocardiográfico [Caseous calcification of the mitral annulus, a rare echocardiographic finding]. Rev. Española Cardiol. 2011, 64, 828–831. [Google Scholar] [CrossRef] [PubMed]
- Elgendy, I.Y.; Conti, C.R. Caseous Calcification of the Mitral Annulus: A Review. Clin. Cardiol. 2013, 36, E27–E31. [Google Scholar] [CrossRef] [PubMed]
- Toia, P.; La Grutta, L.; Sollami, G.; Clemente, A.; Gagliardo, C.; Galia, M.; Maffei, E.; Midiri, M.; Cademartiri, F. Technical development in cardiac CT: Current standards and future improvements—A narrative review. Cardiovasc. Diagn. Ther. 2020, 10, 2018–2035. [Google Scholar] [CrossRef] [PubMed]
- Strzelczyk, J.; Styczyński, G.; Szmigielski, C.; Bidiuk, J. Very rare location of the mitral valve abscess. Pol. Arch. Intern. Med. 2021, 131, 742–743. [Google Scholar] [CrossRef] [PubMed]
- Gao, H.; Yao, L.; Cheng, Y.; Wu, C.; Mei, X.; Mou, Y.; Jiang, L.; Zheng, Z. Caseous calcification of the mitral annulus mimicking benign cardiac tumour of the mitral valve. Cardiovasc. J. Afr. 2021, 32, 52–55. [Google Scholar] [CrossRef] [PubMed]
- Sagnier, S.; Poli, M.; Oysel-Mestre, M.; Corneloup, O.; Debruxelles, S.; Renou, P.; Rouanet, F.; Sibon, I. Caseous calcification of the mitral annulus associated with stroke: Report of two cases. Rev. Neurol. 2015, 171, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Higashi, H.; Ohara, T.; Nakatani, S.; Hashimoto, S.; Torii, T.; Miyashita, K.; Naritomi, H.; Kitakaze, M. A case of caseous calcification of the mitral annulus: A potential source of embolic stroke. J. Cardiol. Cases 2010, 2, e141–e143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ono, M.; Mizuno, A.; Masuda, K.; Suzuki, K.; Abe, K.; Kawazoe, K.; Komiyama, N. Infective Endocarditis on Caseous Calcification of the Mitral Annulus Involving Both the Anterior and Posterior Annulus: A Rare Case Report. Intern. Med. 2018, 57, 965–969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farrag, A.; Bakhoum, S.; Salem, M.; El-Faramawy, A.; Gergis, E. The association between extracoronary calcification and coronary artery disease in patients with type 2 diabetes mellitus. Hear. Vessel. 2011, 28, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Hamasaki, A.; Uchida, T.; Sadahiro, M. Spontaneous rupture of a caseous calcification of the mitral annulus in a hemodialysis patient. J. Card. Surg. 2017, 32, 85–87. [Google Scholar] [CrossRef] [PubMed]
- Dietl, C.A.; Hawthorn, C.M.; Raizada, V. Risk of Cerebral Embolization with Caseous Calcification of the Mitral Annulus: Review Article. Open Cardiovasc. Med. J. 2016, 10, 221–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wehman, B.; Dawood, M.; Ghoreishi, M.; Cheema, F.; Jones, J.; Kane, M.A.; Ward, C.W.; Gammie, J.S. Surgical Management of Caseous Calcification of the Mitral Annulus. Ann. Thorac. Surg. 2015, 99, 2231–2233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deluca, G.; Correale, M.; Ieva, R.; Del Salvatore, B.; Gramenzi, S.; Di Biase, M. The Incidence and Clinical Course of Caseous Calcification of the Mitral Annulus: A Prospective Echocardiographic Study. J. Am. Soc. Echocardiogr. 2008, 21, 828–833. [Google Scholar] [CrossRef] [PubMed]
- Correale, M.; DeLuca, G.; Ieva, R.; Di Biase, M. Spontaneous resolution of a caseous calcification of the mitral annulus. Clinics 2009, 64, 1130–1132. [Google Scholar] [CrossRef] [PubMed] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gać, P.; Cheładze, P.; Poręba, R. The Importance of Cardiac Computed Tomography in the Diagnosis of Caseous Calcification of the Mitral Annulus—Case Reports. Diagnostics 2022, 12, 667. https://doi.org/10.3390/diagnostics12030667
Gać P, Cheładze P, Poręba R. The Importance of Cardiac Computed Tomography in the Diagnosis of Caseous Calcification of the Mitral Annulus—Case Reports. Diagnostics. 2022; 12(3):667. https://doi.org/10.3390/diagnostics12030667
Chicago/Turabian StyleGać, Paweł, Przemysław Cheładze, and Rafał Poręba. 2022. "The Importance of Cardiac Computed Tomography in the Diagnosis of Caseous Calcification of the Mitral Annulus—Case Reports" Diagnostics 12, no. 3: 667. https://doi.org/10.3390/diagnostics12030667
APA StyleGać, P., Cheładze, P., & Poręba, R. (2022). The Importance of Cardiac Computed Tomography in the Diagnosis of Caseous Calcification of the Mitral Annulus—Case Reports. Diagnostics, 12(3), 667. https://doi.org/10.3390/diagnostics12030667