
The Predicting Role of the Neutrophil-to-Lymphocyte Ratio for the Tumor Grade and Prognosis in Pancreatic Neuroendocrine Tumors


Abstract
:1. Introduction
2. Materials and Methods
2.1. Published Studies Search and Selection Criteria
2.2. Data Extraction
2.3. Statistical Analyses
3. Results
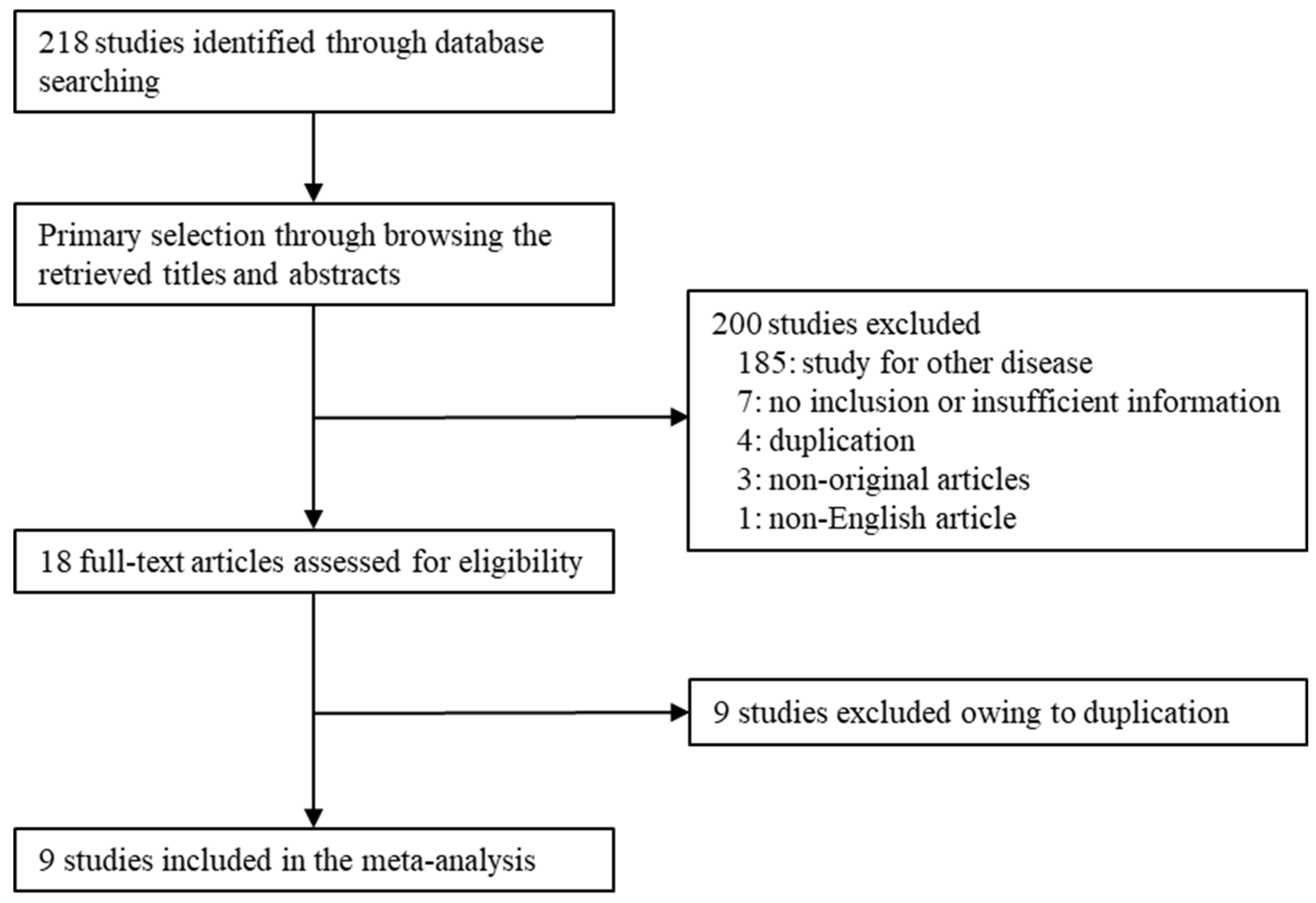
3.1. Selection and Characteristics of the Studies
3.2. The Higher Neutrophil-to-Lymphocyte Ratio in Pancreatic Neuroendocrine Tumors
3.3. Prognostic Implications of the Neutrophil-to-Lymphocyte Ratio in Pancreatic Neuroendocrine Tumors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lawrence, B.; Gustafsson, B.I.; Chan, A.; Svejda, B.; Kidd, M.; Modlin, I.M. The epidemiology of gastroenteropancreatic neuroendocrine tumors. Endocrinol. Metab. Clin. N. Am. 2011, 40, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Metz, D.C.; Jensen, R.T. Gastrointestinal neuroendocrine tumors: Pancreatic endocrine tumors. Gastroenterology 2008, 135, 1469–1492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, J.C.; Hassan, M.; Phan, A.; Dagohoy, C.; Leary, C.; Mares, J.E.; Abdalla, E.K.; Fleming, J.B.; Vauthey, J.N.; Rashid, A.; et al. One hundred years after “carcinoid”: Epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J. Clin. Oncol. 2008, 26, 3063–3072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fesinmeyer, M.D.; Austin, M.A.; Li, C.I.; De Roos, A.J.; Bowen, D.J. Differences in survival by histologic type of pancreatic cancer. Cancer Epidemiol. Biomark. Prev. 2005, 14, 1766–1773. [Google Scholar] [CrossRef] [Green Version]
- Bilimoria, K.Y.; Bentrem, D.J.; Merkow, R.P.; Tomlinson, J.S.; Stewart, A.K.; Ko, C.Y.; Talamonti, M.S. Application of the pancreatic adenocarcinoma staging system to pancreatic neuroendocrine tumors. J. Am. Coll. Surg. 2007, 205, 558–563. [Google Scholar] [CrossRef] [PubMed]
- WHO Classification of Tumours Editorial Board. WHO Classification of Tumours of the Digestive System, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2018. [Google Scholar]
- Grivennikov, S.I.; Greten, F.R.; Karin, M. Immunity, inflammation, and cancer. Cell 2010, 140, 883–899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diakos, C.I.; Charles, K.A.; McMillan, D.C.; Clarke, S.J. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014, 15, e493–e503. [Google Scholar] [CrossRef]
- Zhao, Z.; Zhao, X.; Lu, J.; Xue, J.; Liu, P.; Mao, H. Prognostic roles of neutrophil to lymphocyte ratio and platelet to lymphocyte ratio in ovarian cancer: A meta-analysis of retrospective studies. Arch. Gynecol. Obstet. 2018, 297, 849–857. [Google Scholar] [CrossRef]
- Yodying, H.; Matsuda, A.; Miyashita, M.; Matsumoto, S.; Sakurazawa, N.; Yamada, M.; Uchida, E. Prognostic significance of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in oncologic outcomes of esophageal cancer: A systematic review and meta-analysis. Ann. Surg. Oncol. 2016, 23, 646–654. [Google Scholar] [CrossRef]
- Zheng, J.; Cai, J.; Li, H.; Zeng, K.; He, L.; Fu, H.; Zhang, J.; Chen, L.; Yao, J.; Zhang, Y.; et al. Neutrophil to lymphocyte ratio and platelet to lymphocyte ratio as prognostic predictors for hepatocellular carcinoma patients with various treatments: A meta-analysis and systematic review. Cell. Physiol. Biochem. 2017, 44, 967–981. [Google Scholar] [CrossRef]
- Wang, L.; Liang, D.; Xu, X.; Jin, J.; Li, S.; Tian, G.; Gao, Z.; Liu, C.; He, Y. The prognostic value of neutrophil to lymphocyte and platelet to lymphocyte ratios for patients with lung cancer. Oncol. Lett. 2017, 14, 6449–6456. [Google Scholar] [CrossRef] [Green Version]
- Arima, K.; Okabe, H.; Hashimoto, D.; Chikamoto, A.; Nitta, H.; Higashi, T.; Kaida, T.; Yamamura, K.; Kitano, Y.; Komohara, Y.; et al. Neutrophil-to-lymphocyte ratio predicts metachronous liver metastasis of pancreatic neuroendocrine tumors. Int. J. Clin. Oncol. 2017, 22, 734–739. [Google Scholar] [CrossRef] [PubMed]
- Debien, V.; Davidson, G.; Baltzinger, P.; Kurtz, J.E.; Séverac, F.; Imperiale, A.; Pessaux, P.; Addeo, P.; Bachellier, P.; Su, X.; et al. Involvement of Neutrophils in Metastatic Evolution of Pancreatic Neuroendocrine Tumors. Cancers 2021, 13, 2771. [Google Scholar] [CrossRef] [PubMed]
- Gaitanidis, A.; Patel, D.; Nilubol, N.; Tirosh, A.; Sadowski, S.; Kebebew, E. Markers of systemic inflammatory response are prognostic factors in patients with pancreatic neuroendocrine tumors (PNETs): A prospective analysis. Ann. Surg. Oncol. 2018, 25, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Harimoto, N.; Hoshino, K.; Muranushi, R.; Hagiwara, K.; Yamanaka, T.; Ishii, N.; Tsukagoshi, M.; Igarashi, T.; Tanaka, H.; Watanabe, A.; et al. Prognostic significance of neutrophil-lymphocyte ratio in resectable pancreatic neuroendocrine tumors with special reference to tumor-associated macrophages. Pancreatology 2019, 19, 897–902. [Google Scholar] [CrossRef]
- Luo, G.; Liu, C.; Cheng, H.; Jin, K.; Guo, M.; Lu, Y.; Long, J.; Xu, J.; Ni, Q.; Chen, J.; et al. Neutrophil-lymphocyte ratio predicts survival in pancreatic neuroendocrine tumors. Oncol. Lett. 2017, 13, 2454–2458. [Google Scholar] [CrossRef] [Green Version]
- Miura, T.; Ohtsuka, H.; Aoki, T.; Aoki, S.; Hata, T.; Takadate, T.; Maeda, S.; Ariake, K.; Kawaguchi, K.; Masuda, K.; et al. Increased neutrophil-lymphocyte ratio predicts recurrence in patients with well-differentiated pancreatic neuroendocrine neoplasm based on the 2017 World Health Organization classification. BMC Surg. 2021, 21, 176. [Google Scholar] [CrossRef]
- Panni, R.Z.; Lopez-Aguiar, A.G.; Liu, J.; Poultsides, G.A.; Rocha, F.G.; Hawkins, W.G.; Strasberg, S.M.; Trikalinos, N.A.; Maithel, S.; Fields, R.C.; et al. Association of preoperative monocyte-to-lymphocyte and neutrophil-to-lymphocyte ratio with recurrence-free and overall survival after resection of pancreatic neuroendocrine tumors (US-NETSG). J. Surg. Oncol. 2019, 120, 632–638. [Google Scholar] [CrossRef]
- Tong, Z.; Liu, L.; Zheng, Y.; Jiang, W.; Zhao, P.; Fang, W.; Wang, W. Predictive value of preoperative peripheral blood neutrophil/lymphocyte ratio for lymph node metastasis in patients of resectable pancreatic neuroendocrine tumors: A nomogram-based study. World J. Surg. Oncol. 2017, 15, 108. [Google Scholar] [CrossRef]
- Zhou, B.; Zhan, C.; Wu, J.; Liu, J.; Zhou, J.; Zheng, S. Prognostic significance of preoperative neutrophil-to-lymphocyte ratio in surgically resectable pancreatic neuroendocrine tumors. Med. Sci. Monit. 2017, 23, 5574–5588. [Google Scholar] [CrossRef] [Green Version]
- Jeong, J.H.; Kim, N.Y.; Pyo, J.S. Prognostic roles of lymph node micrometastasis in non-small cell lung cancer. Pathol. Res. Pract. 2018, 214, 240–244. [Google Scholar] [CrossRef] [PubMed]
- Parmar, M.K.; Torri, V.; Stewart, L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat. Med. 1998, 17, 2815–2834. [Google Scholar] [CrossRef]
- Peto, R. Experimental survival curves for interval-censored data. J. R. Stat. Soc. Ser. C Appl. Stat. 1973, 22, 86–91. [Google Scholar] [CrossRef]
- Franko, J.; Feng, W.; Yip, L.; Genovese, E.; Moser, A.J. Non-functional neuroendocrine carcinoma of the pancreas: Incidence, tumor biology, and outcomes in 2158 patients. J. Gastrointest. Surg. 2010, 14, 541–548. [Google Scholar] [CrossRef]
- Falconi, M.; Bartsch, D.K.; Eriksson, B.; Klöppel, G.; Lopes, J.M.; O’Connor, J.M.; Salazar, R.; Taal, B.G.; Vullierme, M.P.; O’Toole, D.; et al. ENETS Consensus Guidelines for the management of patients with digestive neuroendocrine neoplasms of the digestive system: Well-differentiated pancreatic non-functioning tumors. Neuroendocrinology 2012, 95, 120–134. [Google Scholar] [CrossRef] [PubMed]
- Falconi, M.; Eriksson, B.; Kaltsas, G.; Bartsch, D.K.; Capdevila, J.; Caplin, M.; Kos-Kudla, B.; Kwekkeboom, D.; Rindi, G.; Klöppel, G.; et al. ENETS Consensus Guidelines Update for the Management of Patients with Functional Pancreatic Neuroendocrine Tumors and Non-Functional Pancreatic Neuroendocrine Tumors. Neuroendocrinology 2016, 103, 153–171. [Google Scholar] [CrossRef] [Green Version]
- Strosberg, J.R.; Cheema, A.; Weber, J.M.; Ghayouri, M.; Han, G.; Hodul, P.J.; Kvols, L.K. Relapse-free survival in patients with nonmetastatic, surgically resected pancreatic neuroendocrine tumors: An analysis of the AJCC and ENETS staging classifications. Ann. Surg. 2012, 256, 321–325. [Google Scholar] [CrossRef]
- Strosberg, J.R.; Cheema, A.; Weber, J.; Han, G.; Coppola, D.; Kvols, L.K. Prognostic validity of a novel American Joint Committee on Cancer Staging Classification for pancreatic neuroendocrine tumors. J. Clin. Oncol. 2011, 29, 3044–3049. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Author, Year | Location | Tx Option | Tumor Grade | Criteria | Number of Patients | ||||
|---|---|---|---|---|---|---|---|---|---|
| G1 | G2 | G3 | Total | High | Low | ||||
| Arima, 2017 | Japan | Surgery | 46 | 9 | 3 | 2.40 | 58 | 12 | 46 |
| Debien, 2021 | France | Mixed | 75 | 69 | 0 | 4.00 | 144 | 27 | 117 |
| Gaitanidis, 2017 | U.S.A. | Mixed | ND | ND | ND | 2.30 | 97 | ND | ND |
| Harimoto, 2019 | Japan | Surgery | 34 | 17 | 4 | 3.41 | 55 | 14 | 41 |
| Luo, 2017 | China | Mixed | ND | ND | ND | 2.40 | 89 | 28 | 61 |
| Miura, 2021 | Japan | Surgery | 73 | 45 | 2 | 2.62 | 120 | 18 | 102 |
| Panni, 2019 | U.S.A. | Surgery | 305 | 152 | 20 | 3.70 | 620 | 171 | 449 |
| Tong, 2017 | China | Surgery | 52 | 32 | 11 | 1.40 | 95 | ND | ND |
| Zhou, 2017 | China | Surgery | 73 | 76 | 23 | 2.31 | 172 | 67 | 105 |
| Number of Subset | Fixed Effect [95% CI] | Heterogeneity Test [p-Value] | Random Effect [95% CI] | Egger’s Test [p-Value] | |
|---|---|---|---|---|---|
| Overall | 7 | 0.273 [0.249, 0.299] | <0.001 | 0.253 [0.198, 0.317] | 0.404 |
| G1 | 5 | 0.168 [0.128, 0.218] | 0.098 | 0.155 [0.103, 0.227] | 0.077 |
| G2/3 | 9 | 0.408 [0.347, 0.473] | 0.031 | 0.419 [0.313, 0.534] | 0.392 |
| G2 * | 4 | 0.392 [0.312, 0.477] | 0.011 | 0.367 [0.210, 0.559] | 0.735 |
| G3 # | 4 | 0.573 [0.395, 0.733] | 0.579 | 0.573 [0.395, 0.733] | 0.263 |
| NLR criteria | |||||
| High (≥2.40) | 6 | 0.253 [0.227, 0.280] | 0.017 | 0.232 [0.184, 0.287] | 0.253 |
| Low (<2.40) | 1 | 0.390 [0.320, 0.464] | 1.000 | 0.390 [0.320, 0.464] | - |
| Number of Subset | Fixed Effect [95% CI] | Heterogeneity Test [p-Value] | Random Effect [95% CI] | Egger’s Test [p-Value] | |
|---|---|---|---|---|---|
| Pancreatic neuroendocrine tumor | |||||
| G1 | 3 | 1.835 [1.719, 1.952] | 0.041 | 1.912 [1.670, 2.155] | 0.010 |
| G2/3 | 5 | 2.547 [2.318, 2.777] | 0.041 | 2.629 [2.229, 3.028] | 0.328 |
| G2 * | 2 | 2.258 [1.918, 2.598] | 0.834 | 2.258 [1.918, 2.598] | - |
| G3 #,† | 2 | 3.363 [2.738, 3.988] | 0.474 | 3.363 [2.738, 3.988] | - |
| Number of Subset | Fixed Effect [95% CI] | Heterogeneity Test [p-Value] | Random Effect [95% CI] | Egger’s Test [p-Value] | |
|---|---|---|---|---|---|
| Overall survival | 6 | 2.141 [1.533, 2.990] | 0.325 | 2.180 [1.499, 3.169] | 0.472 |
| NLR criteria | |||||
| High (≥2.40) | 5 | 1.978 [1.392, 2.811] | 0.433 | 1.978 [1.392, 2.811] | 0.731 |
| Low (<2.40) | 1 | 4.471 [1.531, 13.055] | 1.000 | 4.471 [1.531, 13.055] | - |
| Recurrence-free survival | 6 | 2.351 [1.701, 3.249] | 0.274 | 2.462 [1.677, 3.615] | 0.055 |
| NLR criteria | |||||
| High (≥2.40) | 4 | 2.213 [1.528, 3.206] | 0.142 | 2.449 [1.416, 4.237] | 0.213 |
| Low (<2.40) | 2 | 2.852 [1.469, 5.537] | 0.489 | 2.852 [1.469, 5.537] | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, D.; Pyo, J.-S.; Chung, K.H.; Son, B.K. The Predicting Role of the Neutrophil-to-Lymphocyte Ratio for the Tumor Grade and Prognosis in Pancreatic Neuroendocrine Tumors. Diagnostics 2022, 12, 737. https://doi.org/10.3390/diagnostics12030737
Oh D, Pyo J-S, Chung KH, Son BK. The Predicting Role of the Neutrophil-to-Lymphocyte Ratio for the Tumor Grade and Prognosis in Pancreatic Neuroendocrine Tumors. Diagnostics. 2022; 12(3):737. https://doi.org/10.3390/diagnostics12030737
Chicago/Turabian StyleOh, Dongwook, Jung-Soo Pyo, Kwang Hyun Chung, and Byoung Kwan Son. 2022. "The Predicting Role of the Neutrophil-to-Lymphocyte Ratio for the Tumor Grade and Prognosis in Pancreatic Neuroendocrine Tumors" Diagnostics 12, no. 3: 737. https://doi.org/10.3390/diagnostics12030737