
Prevalence of Occult Hepatitis C Virus Infection in Egyptian Patients with Lymphoma: A New Vision

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Sampling
2.2.1. Serum Separation
2.2.2. Isolation of PBMCs
2.2.3. Plasma Separation
2.3. RNA Extraction from Plasma and PBMCs
2.4. Detection of HCV RNA in Plasma and PBMCs
2.5. Biochemical Measurements
2.6. Statistical Analysis
3. Results
3.1. Demographic and Biochemical Parameters of the Studied Groups
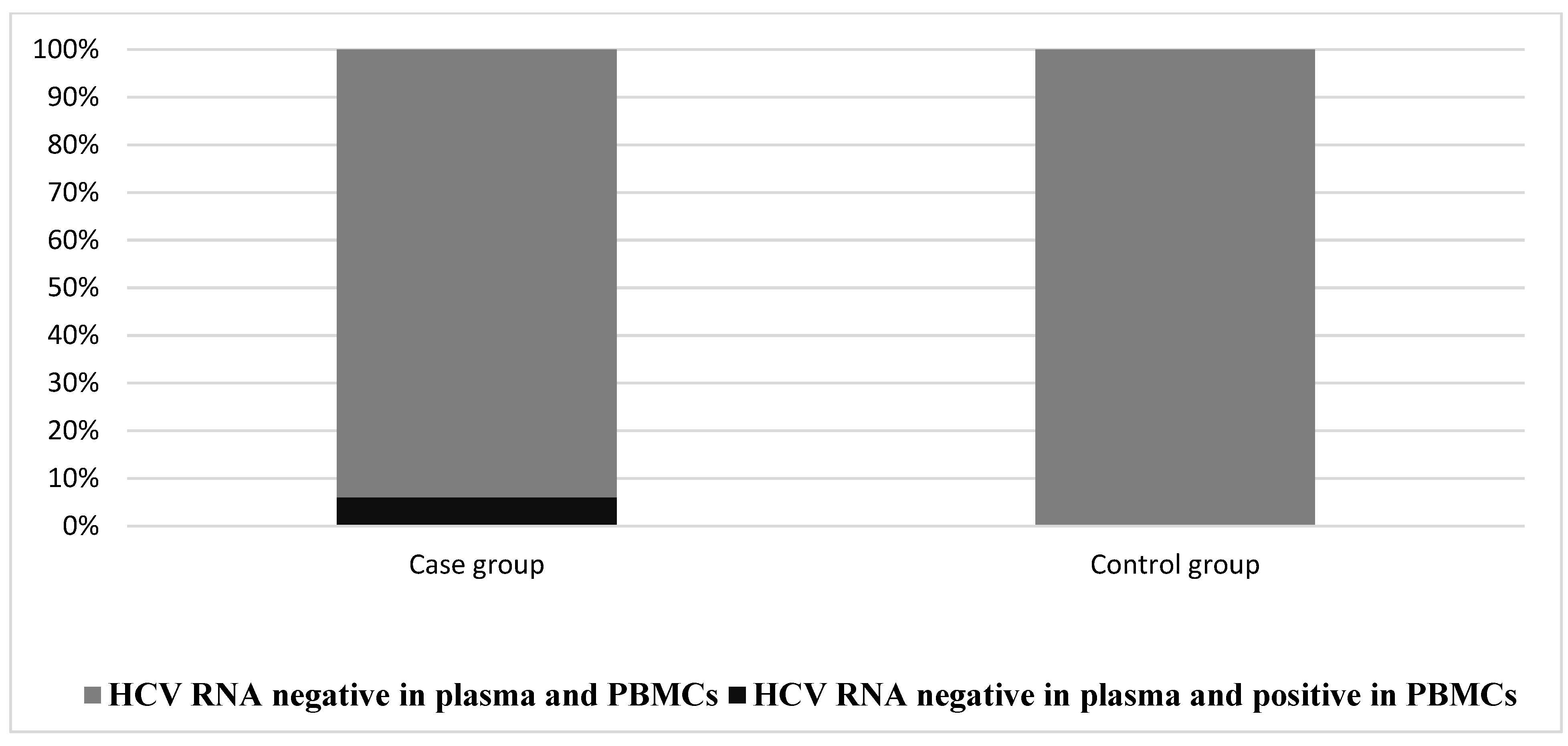
3.2. The Prevalence of OCI in the Studied Groups
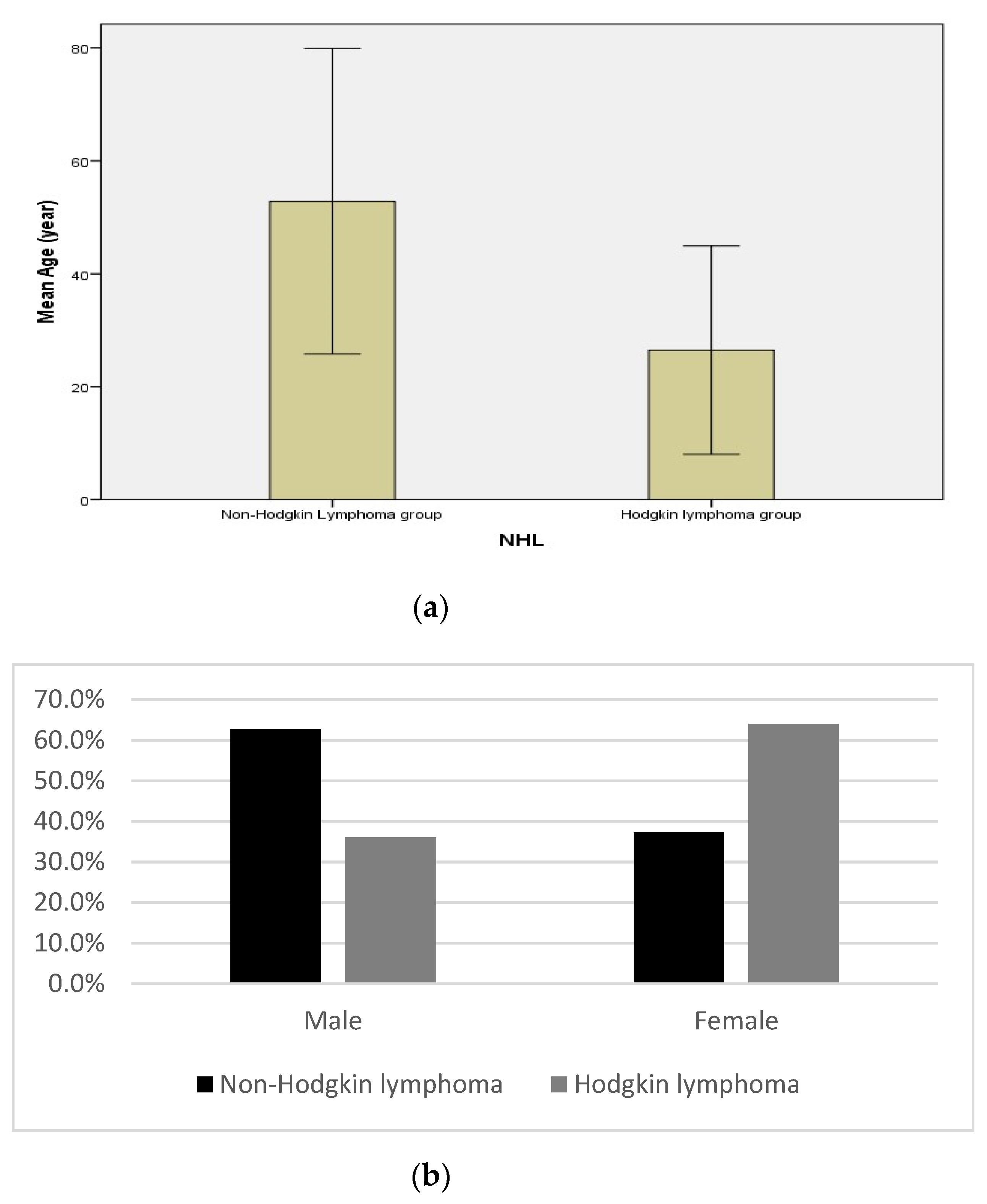
3.3. Demographic and Biochemical Measurements in Non-Hodgkin’s and Hodgkin’s Lymphoma in the Case Group
3.4. The Prevalence of OCI in Patients with Different Types of Lymphoma
3.5. Demographic and Biochemical Parameters in the Case Group According to the Presence or Absence of OCI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Helaly, G.F.; Elsheredy, A.G.; El Basset Mousa, A.A.; Ahmed, H.K.F.; Oluyemi, A.E.G.S. Seronegative and occult hepatitis C virus infections in patients with hematological disorders. Arch. Virol. 2017, 162, 63–69. [Google Scholar] [CrossRef] [PubMed]
- El-Ghitany, E.M. Hepatitis C Virus Infection in Egypt: Current Situation and Future Perspective. J. High Inst. Public Health 2019, 49, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Farahani, M.; Bokharaei-Salim, F.; Ghane, M.; Basi, A.; Meysami, P.; Keyvani, H. Prevalence of occult hepatitis C virus infection in Iranian patients with lymphoproliferative disorders. J. Med. Virol. 2013, 85, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Niepmann, M.; Shalamova, L.A.; Gerresheim, G.K.; Rossbach, O. Signals involved in regulation of hepatitis C virus RNA genome translation and replication. Front. Microbiol. 2018, 9, 395. [Google Scholar] [CrossRef] [PubMed]
- Zignego, A.L.; Giannini, C.; Gragnani, L. HCV and lymphoproliferation. Clin. Dev. Immunol. 2012, 2012, 980942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attar, B.M.; Van Thiel, D. A New Twist to a Chronic HCV Infection: Occult Hepatitis C. Gastroenterol. Res. Pract. 2015, 2015, 579147. [Google Scholar] [CrossRef]
- Veerapu, N.S.; Park, S.H.; Tully, D.C.; Allen, T.M.; Rehermann, B. Trace amounts of sporadically reappearing HCV RNA can cause infection. J. Clin. Investig. 2014, 124, 3469–3478. [Google Scholar] [CrossRef] [Green Version]
- Petruzziello, A.; Marigliano, S.; Loquercio, G.; Cozzolino, A.; Cacciapuoti, C. Global epidemiology of hepatitis C virus infection: An up-date of the distribution and circulation of hepatitis C virus genotypes. World J. Gastroenterol. 2016, 22, 7824–7840. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2016. CA. Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef] [Green Version]
- Youssef, S.S.; Nasr, A.S.; El Zanaty, T.; El Rawi, R.S.; Mattar, M.M. Prevalence of occult hepatitis C virus in egyptian patients with chronic lymphoproliferative disorders. Hepat. Res. Treat. 2012, 2012, 429784. [Google Scholar] [CrossRef] [Green Version]
- Tasleem, S.; Sood, G.K. Hepatitis C Associated B-cell Non-Hodgkin Lymphoma: Clinical Features and the Role of Antiviral Therapy. J. Clin. Transl. Hepatol. 2015, 3, 134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Marco, L.; Manzini, P.; Trevisan, M.; Gillio-Tos, A.; Danielle, F.; Balloco, C.; Pizzi, A.; de Filippo, E.; D’Antico, S.; Violante, B.; et al. Prevalence and follow-up of Occult HCV infection in an Italian population free of clinically detectable infectious liver disease. PLoS ONE 2012, 7, e43541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boom, R.; Sol, C.J.A.; Salimans, M.M.M.; Jansen, C.L.; Wertheim-Van Dillen, P.M.E.; Van Der Noordaa, J. Rapid and simple method for purification of nucleic acids. J. Clin. Microbiol. 1990, 28, 495–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sy, T.; Jamal, M.M. Epidemiology of Hepatitis C Virus (HCV) Infection. Int. J. Med. Sci. 2006, 3, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- REITMAN, S.; FRANKEL, S. A colorimetric method for the determination of serum glutamic oxalacetic and glutamic pyruvic transaminases. Am. J. Clin. Pathol. 1957, 28, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Walters, M.I.; Gerarde, H.W. An ultramicromethod for the determination of conjugated and total bilirubin in serum or plasma. Microchem. J. 1970, 15, 231–243. [Google Scholar] [CrossRef]
- Gregor, A.; Kostrzewska, E.; Godorowska, W. Determination of serum proteins in the presence of dextran by means of the Biuret reaction. Infusionstherapie 1977, 4, 48–50. [Google Scholar] [CrossRef]
- Doumas, B.T.; Ard Watson, W.; Biggs, H.G. Albumin standards and the measurement of serum albumin with bromcresol green. Clin. Chim. Acta 1971, 31, 87–96. [Google Scholar] [CrossRef]
- Castillo, I.; Pardo, M.; Bartolomé, J.; Ortiz-Movilla, N.; Rodríguez-Iñigo, E.; De Lucas, S.; Salas, C.; Jiménez-Heffernan, J.A.; Pérez-Mota, A.; Graus, J.; et al. Occult Hepatitis C Virus Infection in Patients in Whom the Etiology of Persistently Abnormal Results of Liver-Function Tests Is Unknown. J. Infect. Dis. 2004, 189, 7–14. [Google Scholar] [CrossRef] [Green Version]
- Abdel-Moneim, A.S. Occult hepatitis C infections: Time to change the defined groups. Microbiol. Immunol. 2019, 63, 474–475. [Google Scholar] [CrossRef]
- Castillo, I.; Bartolomé, J.; Quiroga, J.A.; Barril, G.; Carreño, V. Diagnosis of occult hepatitis C without the need for a liver biopsy. J. Med. Virol. 2010, 82, 1554–1559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacParland, S.A.; Pham, T.N.Q.; Guy, C.S.; Michalak, T.I. Hepatitis C virus persisting after clinically apparent sustained virological response to antiviral therapy retains infectivity in vitro. Hepatology 2009, 49, 1431–1441. [Google Scholar] [CrossRef] [PubMed]
- Roque Cuéllar, M.; García Lozano, J.; Sánchez, B.; Carrillo Cruz, E.; De la Cruz Vicente, F. Occult Hepatitis C Virus Infection in Spanish Patients with Lymphoproliferative Disorders. J. Emerg. Dis. Virol. 2017, 3, 2473. [Google Scholar] [CrossRef]
- Rezaee-Zavareh, M.S.; Hadi, R.; Karimi-Sari, H.; Khosravi, M.H.M.H.; Ajudani, R.; Dolatimehr, F.; Ramezani-Binabaj, M.; Miri, S.M.; Alavian, S.M. Occult HCV Infection: The Current State of Knowledge. Iran. Red Crescent Med. J. 2015, 17, e34181. [Google Scholar] [CrossRef] [Green Version]
- Planinc-Peraica, A.; Ostojić Kolonić, S.; Radić-Krišto, D.; Dominis, M.; Jakšić, B. Serum Immunoglobulins in non-Hodgkin’s Lymphoma Patients. Coll. Antropol. 2010, 34, 407–411. [Google Scholar]
- Waked, I.; Esmat, G.; Elsharkawy, A.; El-Serafy, M.; Abdel-Razek, W.; Ghalab, R.; Elshishiney, G.; Salah, A.; Abdel Megid, S.; Kabil, K.; et al. Screening and Treatment Program to Eliminate Hepatitis C in Egypt. N. Engl. J. Med. 2020, 382, 1166–1174. [Google Scholar] [CrossRef]
- De Re, V.; De Vita, S.; Marzotto, A.; Rupolo, M.; Gloghini, A.; Pivetta, B.; Gasparotto, D.; Carbone, A.; Boiocchi, M. Sequence analysis of the immunoglobulin antigen receptor of hepatitis C virus-Associated non-Hodgkin lymphomas suggests that the malignant cells are derived from the rheumatoid factorn-Producing cells that occur mainly in type II cryoglobulinemia. Blood 2000, 96, 3578–3584. [Google Scholar] [CrossRef]
- Defrancesco, I.; Zerbi, C.; Rattotti, S.; Merli, M.; Bruno, R.; Paulli, M.; Arcaini, L. HCV infection and non-Hodgkin lymphomas: An evolving story. Clin. Exp. Med. 2020, 20, 321–328. [Google Scholar] [CrossRef]
- Machida, K.; Cheng, K.T.-H.; Pavio, N.; Sung, V.M.-H.; Lai, M.M.C. Hepatitis C Virus E2-CD81 Interaction Induces Hypermutation of the Immunoglobulin Gene in B Cells. J. Virol. 2005, 79, 8079–8089. [Google Scholar] [CrossRef] [Green Version]
- Saad, Y.; Zakaria, S.; Ramzy, I.; El Raziky, M.; Shaker, O.; Elakel, W.; Said, M.; Noseir, M.; El-Daly, M.; Hamid, M.A.; et al. Prevalence of occult hepatitis C in Egyptian patients with non alcoholic fatty liver disease. Open J. Intern. Med. 2011, 1, 33–37. [Google Scholar] [CrossRef] [Green Version]
- Eldaly, O.M.; Elbehedy, E.M.; Fakhr, A.E.; Lotfy, A. Prevalence of Occult Hepatitis C Virus in Blood Donors in Zagazig City Blood Banks. Egypt. J. Med. Microbiol. 2016, 25, 1–8. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter | Groups | p-Value | |
|---|---|---|---|
| Case Group | Control Group | ||
| N = 100 (%) | N = 100 (%) | ||
| Age (year): | |||
| Mean ± SD | 46.24 ± 17.0 | 44.72 ± 12.65 | 0.474 |
| Gender: | |||
| Male | 56 (56%) | 51 (51%) | 0.478 |
| Female | 44 (44%) | 49 (49%) | |
| T. protein (g/dL) | |||
| Mean ± SD | 7.17 ± 0.49 | 7.46 ± 0.45 | <0.001 ** |
| S. albumin (g/dL) | |||
| Mean ± SD | 4.26 ± 0.52 | 4.31 ± 0.4 | 0.476 |
| ALT: | |||
| Median | 22 | 21.5 | 0.487 |
| Range | 10–90.5 | 14–27 | |
| AST: | |||
| Median | 24 | 23.5 | 0.247 |
| Range | 12.2–100.2 | 15–33 | |
| T. bilirubin: | |||
| Median | 0.6 | 0.6 | 0.11 |
| Range | 0.21–2.19 | 0.21–0.65 | |
| D. bilirubin: | |||
| Median | 0.17 | 0.15 | 0.164 |
| Range | 0.08–0.63 | 0.14–0.4 | |
| Parameter | Lymphoma | p-Value | |
|---|---|---|---|
| Non-Hodgkin’s | Hodgkin’s | ||
| N = 75 | N = 25 | ||
| T. protein (g/dL) | |||
| Mean ± SD | 7.13 ± 0.53 | 7.28 ± 0.34 | 0.195 |
| S. albumin (g/dL) | |||
| Mean ± SD | 4.2 ± 0.55 | 4.46 ± 0.33 | 0.006 * |
| ALT: | |||
| Median | 22 | 20 | 0.695 |
| Range | 10–90.5 | 10–47 | |
| AST: | |||
| Median | 24 | 22 | 0.031 * |
| Range | 1–100.2 | 12.2–38 | |
| T. bilirubin: | |||
| Median | 0.65 | 0.45 | 0.221 |
| Range | 0.21–1.39 | 0.29–2.19 | |
| D. bilirubin: | |||
| Median | 0.17 | 0.16 | 0.814 |
| Range | 0.08–0.63 | 0.10–0.26 | |
| Occult C | Lymphoma | p-Value | |
|---|---|---|---|
| Non-Hodgkin’s | Hodgkin’s | ||
| N = 75 (%) | N = 25 (%) | ||
| Positive | 6 (8%) | 0 (0%) | |
| Negative | 69 (92%) | 25 (100%) | 0.322 |
| Parameter | Occult C | p-Value | |
|---|---|---|---|
| Absent | Present | ||
| N = 94 (%) | N = 6 (%) | ||
| Age (year): | |||
| Mean ± SD | 46.89 ± 17.11 | 36.0 ± 12.03 | 0.129 |
| Gender: | |||
| Male | 42 (60.9%) | 5 (83.3%) | 0.401 |
| Female | 27 (39.1%) | 1 (16.7%) | |
| T. protein (g/dL) | |||
| Mean ± SD | 7.2 ± 0.47 | 6.65 ± 0.61 | 0.007 * |
| S. albumin (g/dL) | |||
| Mean ± SD | 4.29 ± 0.5 | 3.82 ± 0.68 | 0.03 * |
| ALT: | 0.021 * | ||
| Median | 21.5 | 42.5 | |
| Range | 10–47 | 15.4–90.5 | |
| AST: | |||
| Median | 23 | 26.2 | 0.006 * |
| Range | 12.2–38 | 23–100 | |
| T. bilirubin: | |||
| Median | 0.6 | 0.6 | 0.977 |
| Range | 0.21–2.19 | 0.22–1.39 | |
| D. bilirubin: | |||
| Median | 0.17 | 0.17 | 0.556 |
| Range | 0.08–0.63 | 0.13–0.63 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elkashef, K.A.; Emam, W.A.; Mesbah, N.M.; Abo-Elmatty, D.M.; Abdel-Hamed, A.R. Prevalence of Occult Hepatitis C Virus Infection in Egyptian Patients with Lymphoma: A New Vision. Diagnostics 2022, 12, 1015. https://doi.org/10.3390/diagnostics12041015
Elkashef KA, Emam WA, Mesbah NM, Abo-Elmatty DM, Abdel-Hamed AR. Prevalence of Occult Hepatitis C Virus Infection in Egyptian Patients with Lymphoma: A New Vision. Diagnostics. 2022; 12(4):1015. https://doi.org/10.3390/diagnostics12041015
Chicago/Turabian StyleElkashef, Kholoud A., Wafaa A. Emam, Noha M. Mesbah, Dina M. Abo-Elmatty, and Asmaa R. Abdel-Hamed. 2022. "Prevalence of Occult Hepatitis C Virus Infection in Egyptian Patients with Lymphoma: A New Vision" Diagnostics 12, no. 4: 1015. https://doi.org/10.3390/diagnostics12041015
APA StyleElkashef, K. A., Emam, W. A., Mesbah, N. M., Abo-Elmatty, D. M., & Abdel-Hamed, A. R. (2022). Prevalence of Occult Hepatitis C Virus Infection in Egyptian Patients with Lymphoma: A New Vision. Diagnostics, 12(4), 1015. https://doi.org/10.3390/diagnostics12041015