
Dorsal Root Ganglia Volume—Normative Values, Correlation with Demographic Determinants and Reliability of Three Different Methods of Volumetry

 , ,
, ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Clinical and Demographic Patient Data
2.2. Imaging Protocol
2.3. Imaging Analysis
2.4. Statistical Analysis
3. Results
3.1. Demographic Characteristics of Subjects
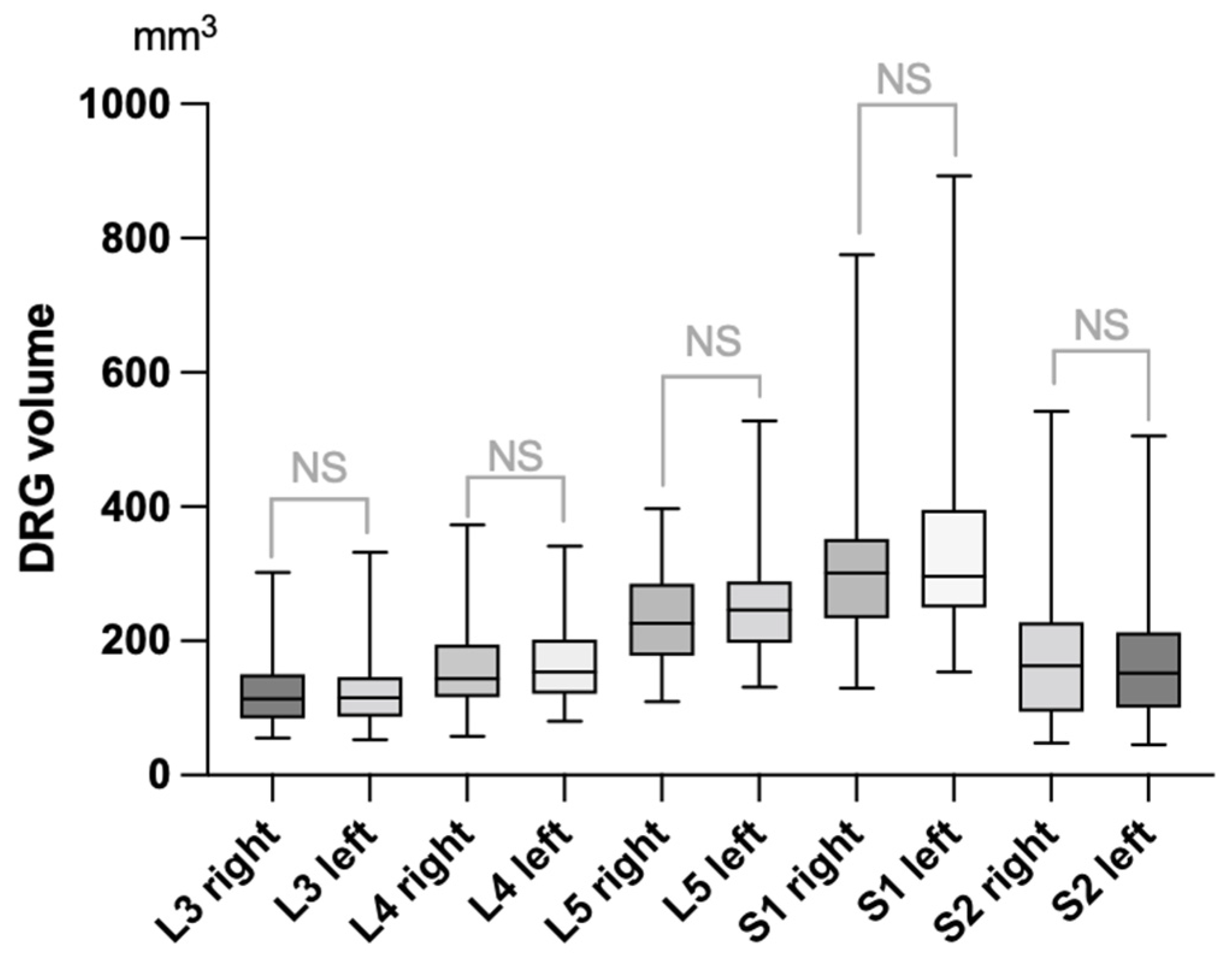
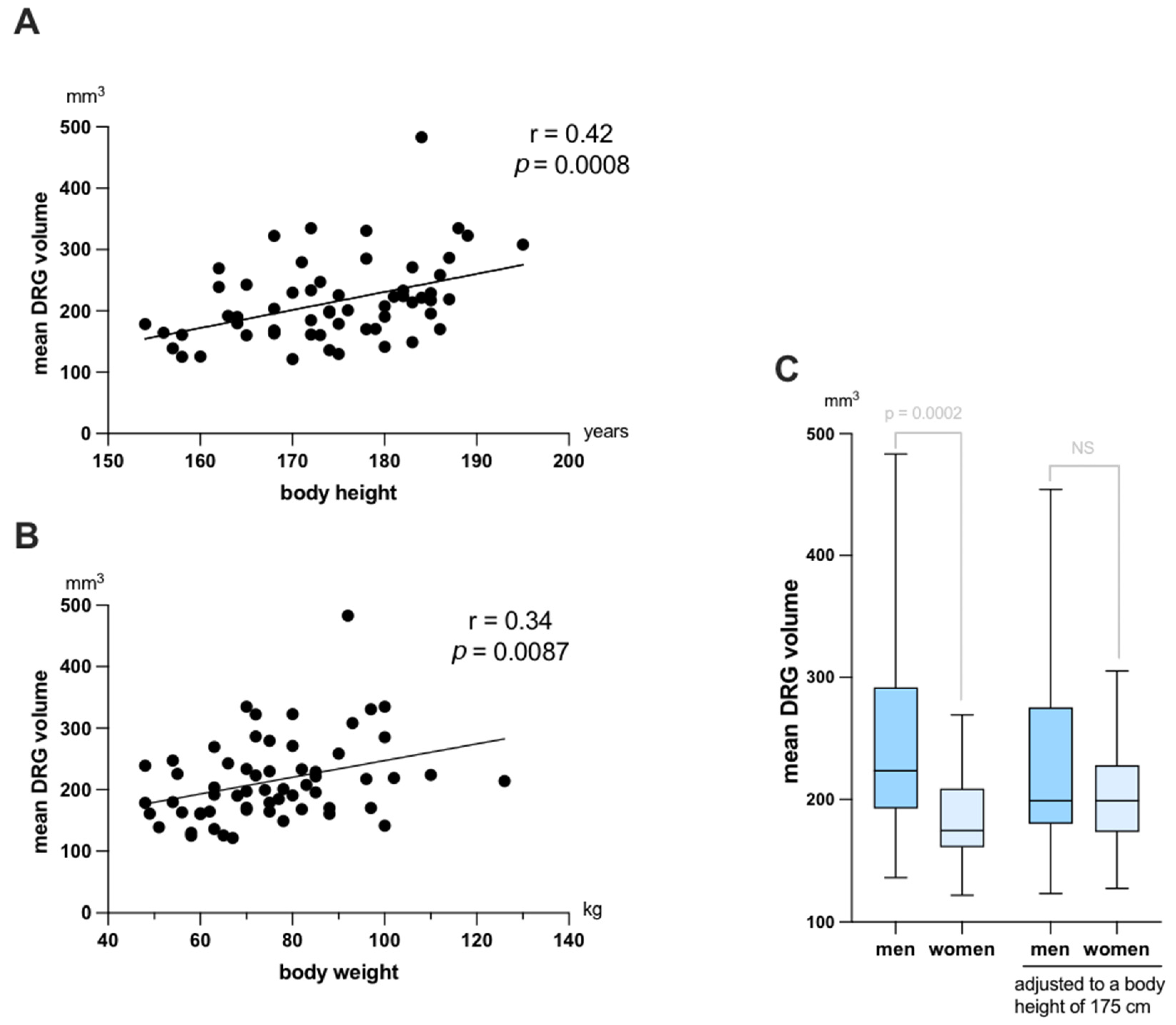
3.2. Normal Values of DRG Volumes and Correlations with Demographic Variables
3.3. Inter-Reader Reliability as Assessed for Each Method
3.4. Inter-Method Reliability
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Pham, M.; Oikonomou, D.; Hornung, B.; Weiler, M.; Heiland, S.; Baumer, P.; Kollmer, J.; Nawroth, P.P.; Bendszus, M. Magnetic resonance neurography detects diabetic neuropathy early and with Proximal Predominance. Ann. Neurol. 2015, 78, 939–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chhabra, A.; Madhuranthakam, A.J.; Andreisek, G. Magnetic resonance neurography: Current perspectives and literature review. Eur. Radiol. 2018, 28, 698–707. [Google Scholar] [CrossRef] [PubMed]
- Baumer, P.; Dombert, T.; Staub, F.; Kaestel, T.; Bartsch, A.J.; Heiland, S.; Bendszus, M.; Pham, M. Ulnar neuropathy at the elbow: MR neurography--nerve T2 signal increase and caliber. Radiology 2011, 260, 199–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Godel, T.; Baumer, P.; Farschtschi, S.; Gugel, I.; Kronlage, M.; Hofstadler, B.; Heiland, S.; Gelderblom, M.; Bendszus, M.; Mautner, V.F. Peripheral nervous system alterations in infant and adult neurofibromatosis type 2. Neurology 2019, 93, e590–e598. [Google Scholar] [CrossRef]
- Godel, T.; Baumer, P.; Pham, M.; Kohn, A.; Muschol, N.; Kronlage, M.; Kollmer, J.; Heiland, S.; Bendszus, M.; Mautner, V.F. Human dorsal root ganglion in vivo morphometry and perfusion in Fabry painful neuropathy. Neurology 2017, 89, 1274–1282. [Google Scholar] [CrossRef]
- Godel, T.; Baumer, P.; Stumpfe, K.; Muschol, N.; Kronlage, M.; Brunnee, M.; Kollmer, J.; Heiland, S.; Bendszus, M.; Mautner, V.F. Dorsal root ganglia volume is increased in patients with the Fabry-related GLA variant p.D313Y. J. Neurol. 2019, 266, 1332–1339. [Google Scholar] [CrossRef]
- Godel, T.; Kohn, A.; Muschol, N.; Kronlage, M.; Schwarz, D.; Kollmer, J.; Heiland, S.; Bendszus, M.; Mautner, V.F.; Baumer, P. Dorsal root ganglia in vivo morphometry and perfusion in female patients with Fabry disease. J. Neurol. 2018, 265, 2723–2729. [Google Scholar] [CrossRef]
- Godel, T.; Mautner, V.F.; Farschtschi, S.; Pham, M.; Schwarz, D.; Kronlage, M.; Gugel, I.; Heiland, S.; Bendszus, M.; Baumer, P. Dorsal root ganglia volume differentiates schwannomatosis and neurofibromatosis 2. Ann. Neurol. 2018, 83, 854–857. [Google Scholar] [CrossRef]
- Haberberger, R.V.; Barry, C.; Dominguez, N.; Matusica, D. Human Dorsal Root Ganglia. Front. Cell. Neurosci. 2019, 13, 271. [Google Scholar] [CrossRef]
- Kronlage, M.; Schwehr, V.; Schwarz, D.; Godel, T.; Uhlmann, L.; Heiland, S.; Bendszus, M.; Baumer, P. Peripheral nerve diffusion tensor imaging (DTI): Normal values and demographic determinants in a cohort of 60 healthy individuals. Eur. Radiol. 2018, 28, 1801–1808. [Google Scholar] [CrossRef]
- Kronlage, M.; Schwehr, V.; Schwarz, D.; Godel, T.; Heiland, S.; Bendszus, M.; Baumer, P. Magnetic Resonance Neurography: Normal Values and Demographic Determinants of Nerve Caliber and T2 Relaxometry in 60 healthy individuals. Clin. Neuroradiol. 2019, 29, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Fosleitner, O.; Schwehr, V.; Godel, T.; Preisner, F.; Baumer, P.; Heiland, S.; Bendszus, M.; Kronlage, M. Magnetization Transfer Ratio of Peripheral Nerve and Skeletal Muscle: Correlation with Demographic Variables in Healthy Volunteers. Clin. Neuroradiol. 2022, 32, 557–564. [Google Scholar] [CrossRef]
- Weiner, S.; Strinitz, M.; Herfurth, J.; Hessenauer, F.; Nauroth-Kress, C.; Kampf, T.; Homola, G.A.; Uceyler, N.; Sommer, C.; Pham, M.; et al. Dorsal Root Ganglion Volumetry by MR Gangliography. AJNR Am. J. Neuroradiol. 2022, 43, 769–775. [Google Scholar] [CrossRef] [PubMed]
- Kollmann, P.; Mautner, V.F.; Koeppen, J.; Wenzel, R.; Friedman, J.M.; Salamon, J.; Farschtschi, S. MRI based volumetric measurements of vestibular schwannomas in patients with neurofibromatosis type 2: Comparison of three different software tools. Sci. Rep. 2020, 10, 11541. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Li, K.; Wang, Q.; Liu, X.; Zhao, X.; Zhong, Z.; Gu, C.; Li, R. Magnetic Resonance Neurography for Evaluation of Dorsal Root Ganglion Morphology. World Neurosurg. 2021, 154, e54–e60. [Google Scholar] [CrossRef] [PubMed]
- Huttner, H.B.; Steiner, T.; Hartmann, M.; Kohrmann, M.; Juettler, E.; Mueller, S.; Wikner, J.; Meyding-Lamade, U.; Schramm, P.; Schwab, S.; et al. Comparison of ABC/2 estimation technique to computer-assisted planimetric analysis in warfarin-related intracerebral parenchymal hemorrhage. Stroke 2006, 37, 404–408. [Google Scholar] [CrossRef] [Green Version]
- Divani, A.A.; Majidi, S.; Luo, X.; Souslian, F.G.; Zhang, J.; Abosch, A.; Tummala, R.P. The ABCs of accurate volumetric measurement of cerebral hematoma. Stroke 2011, 42, 1569–1574. [Google Scholar] [CrossRef] [Green Version]
- Opalak, C.F.; Parry, M.; Rock, A.K.; Sima, A.P.; Carr, M.T.; Chandra, V.; Workman, K.G.; Somasundaram, A.; Broaddus, W.C. Comparison of ABC/2 estimation and a volumetric computerized method for measurement of meningiomas using magnetic resonance imaging. J. Neurooncol. 2019, 144, 275–282. [Google Scholar] [CrossRef]
- Apostolidis, L.; Schwarz, D.; Xia, A.; Weiler, M.; Heckel, A.; Godel, T.; Heiland, S.; Schlemmer, H.P.; Jager, D.; Bendszus, M.; et al. Dorsal root ganglia hypertrophy as in vivo correlate of oxaliplatin-induced polyneuropathy. PLoS ONE 2017, 12, e0183845. [Google Scholar] [CrossRef] [Green Version]
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apostolidis, L.; Kowalscheck, L.; Weber, T.F.; Godel, T.; Bendszus, M.; Kauczor, H.U.; Jager, D.; Schlemmer, H.P.; Baumer, P. Dorsal Root Ganglion Morphometric Changes Under Oxaliplatin Treatment: Longitudinal Assessment by Computed Tomography. Clin. Neuroradiol. 2022, 32, 547–556. [Google Scholar] [CrossRef] [PubMed]
- Godel, T.; Baumer, P.; Farschtschi, S.; Puschel, K.; Hofstadler, B.; Heiland, S.; Gelderblom, M.; Bendszus, M.; Hagel, C.; Mautner, V.F. Long-term Follow-up and Histological Correlation of Peripheral Nervous System Alterations in Neurofibromatosis Type 2. Clin. Neuroradiol. 2021, 32, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Seok, H.Y.; Jang, J.H.; Won, S.J.; Yoon, J.S.; Park, K.S.; Kim, B.J. Cross-sectional area reference values of nerves in the lower extremities using ultrasonography. Muscle Nerve 2014, 50, 564–570. [Google Scholar] [CrossRef] [PubMed]
- Hofstadler, B.; Baumer, P.; Schwarz, D.; Kronlage, M.; Heiland, S.; Bendszus, M.; Godel, T. MR Neurography: Normative Values in Correlation to Demographic Determinants in Children and Adolescents. Clin. Neuroradiol. 2020, 30, 671–677. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Popovic, Z.B.; Thomas, J.D. Assessing observer variability: A user’s guide. Cardiovasc. Diagn. Ther. 2017, 7, 317–324. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| L3 | L4 | L5 | S1 | S2 | |
|---|---|---|---|---|---|
| Number of values (right + left) | 120 | 120 | 120 | 120 | 111 |
| Mean DRG volume (mm3) | 124.8 | 163.4 | 244.0 | 323.3 | 179.4 |
| Std. Deviation (mm3) | 51.1 | 58.5 | 76.9 | 124.5 | 107.1 |
| 3% Percentile–97% Percentile (mm3) | 58.1–251.9 | 86.7–308.5 | 130.3–410.3 | 164.7–633.2 | 55.8–458.2 |
| Range (mm3) | 52.9–331.7 | 57.8–373.3 | 109.5–527.6 | 129.7–893.3 | 45.4–542.3 |
| Reader 1 | Reader 2 | |
|---|---|---|
| Axis-corrected estimation vs. exact volumetry | 0.91 (0.89–0.93) | 0.88 (0.85–0.91) |
| Non-axis-corrected estimation vs. exact volumetry | 0.90 (0.84–0.93) | 0.88 (0.81–0.92) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kronlage, M.; Fischer, T.D.; Behnisch, R.; Schwarz, D.; Bäumer, P.; Schwehr, V.; Heiland, S.; Bendszus, M.; Godel, T. Dorsal Root Ganglia Volume—Normative Values, Correlation with Demographic Determinants and Reliability of Three Different Methods of Volumetry. Diagnostics 2022, 12, 1570. https://doi.org/10.3390/diagnostics12071570
Kronlage M, Fischer TD, Behnisch R, Schwarz D, Bäumer P, Schwehr V, Heiland S, Bendszus M, Godel T. Dorsal Root Ganglia Volume—Normative Values, Correlation with Demographic Determinants and Reliability of Three Different Methods of Volumetry. Diagnostics. 2022; 12(7):1570. https://doi.org/10.3390/diagnostics12071570
Chicago/Turabian StyleKronlage, Moritz, Thomas David Fischer, Rouven Behnisch, Daniel Schwarz, Philipp Bäumer, Veronique Schwehr, Sabine Heiland, Martin Bendszus, and Tim Godel. 2022. "Dorsal Root Ganglia Volume—Normative Values, Correlation with Demographic Determinants and Reliability of Three Different Methods of Volumetry" Diagnostics 12, no. 7: 1570. https://doi.org/10.3390/diagnostics12071570