

Spontaneous Uterine Rupture and Adenomyosis, a Rare but Possible Correlation: Case Report and Literature Review

 , ,
, ,  ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
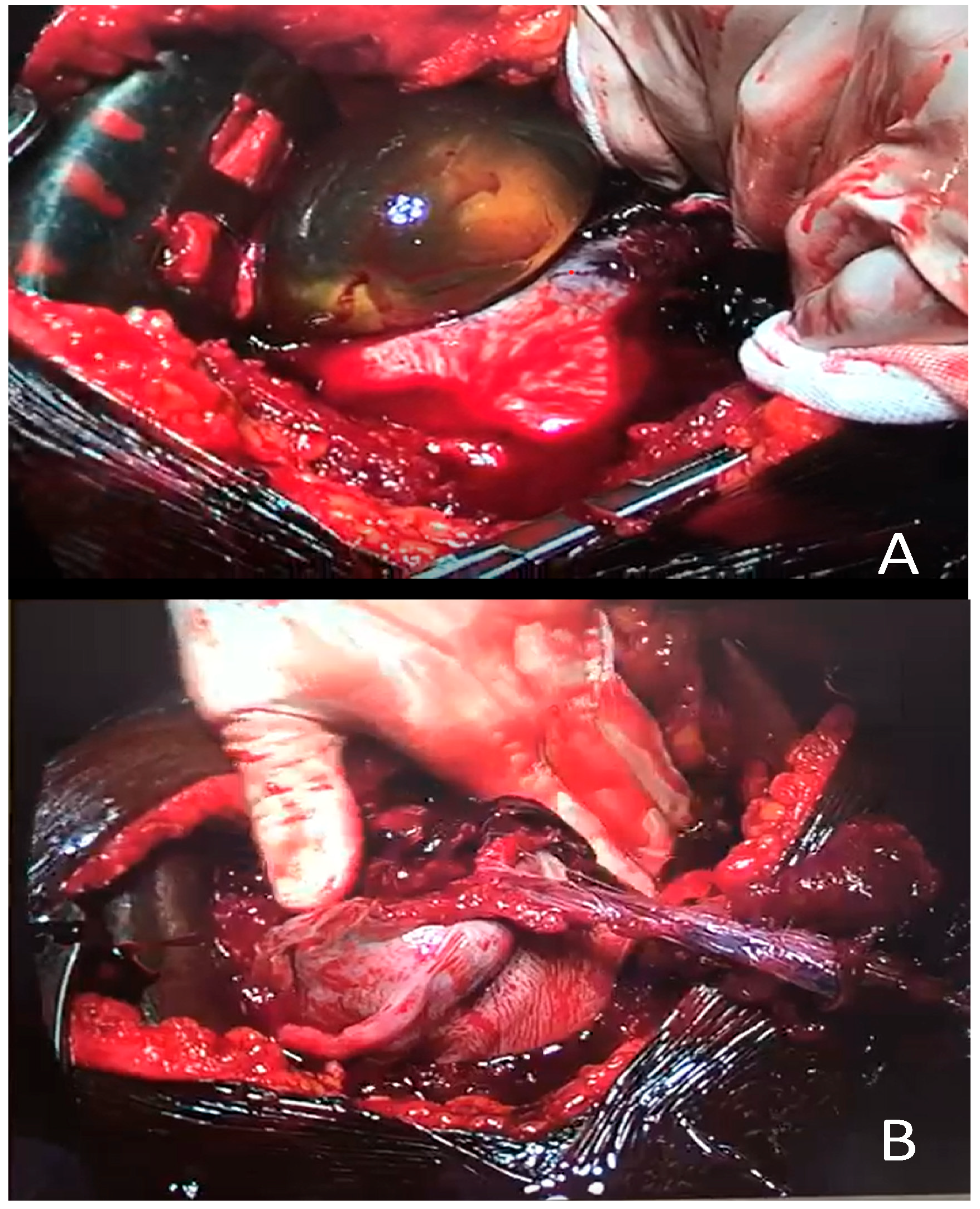
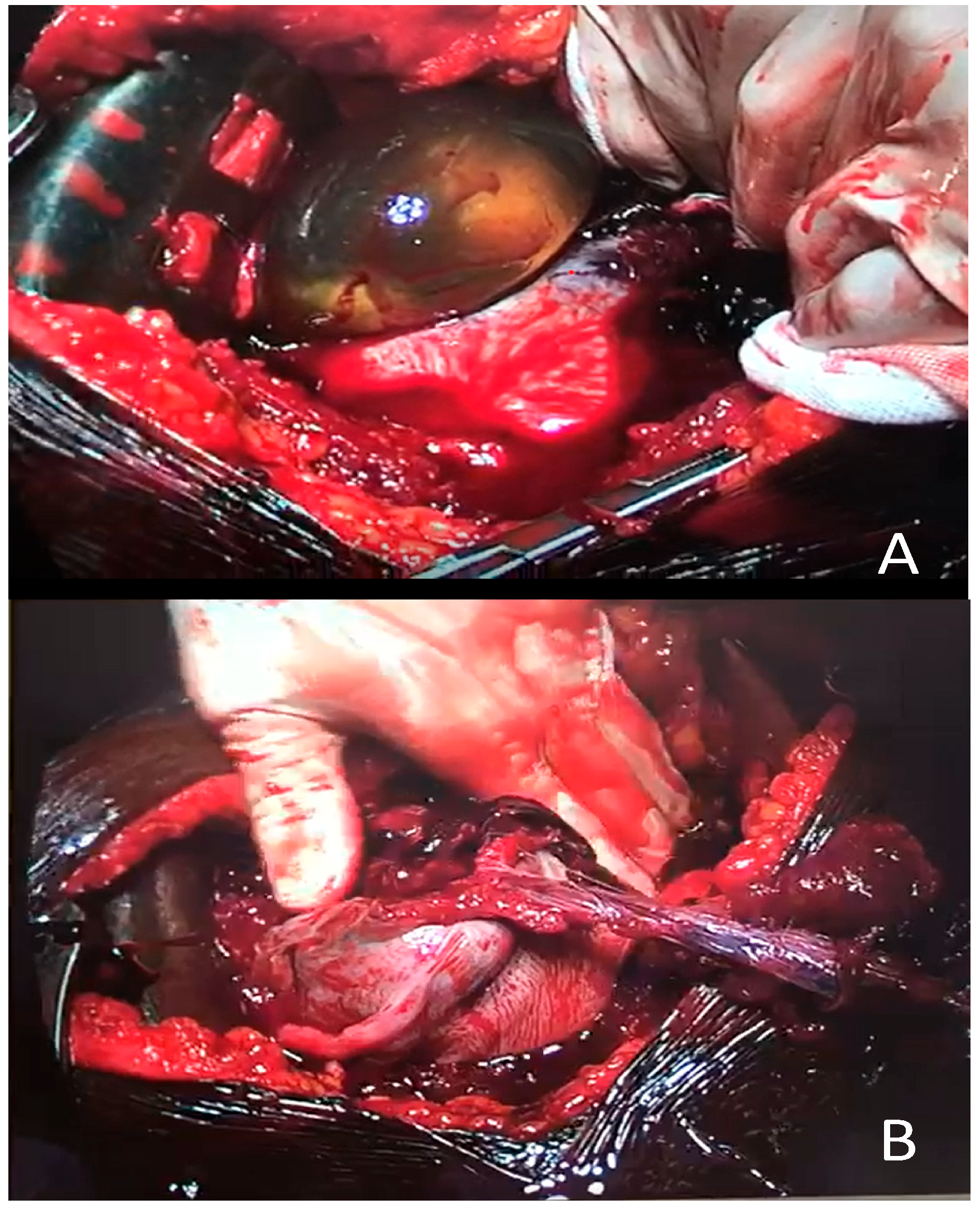
Case Report
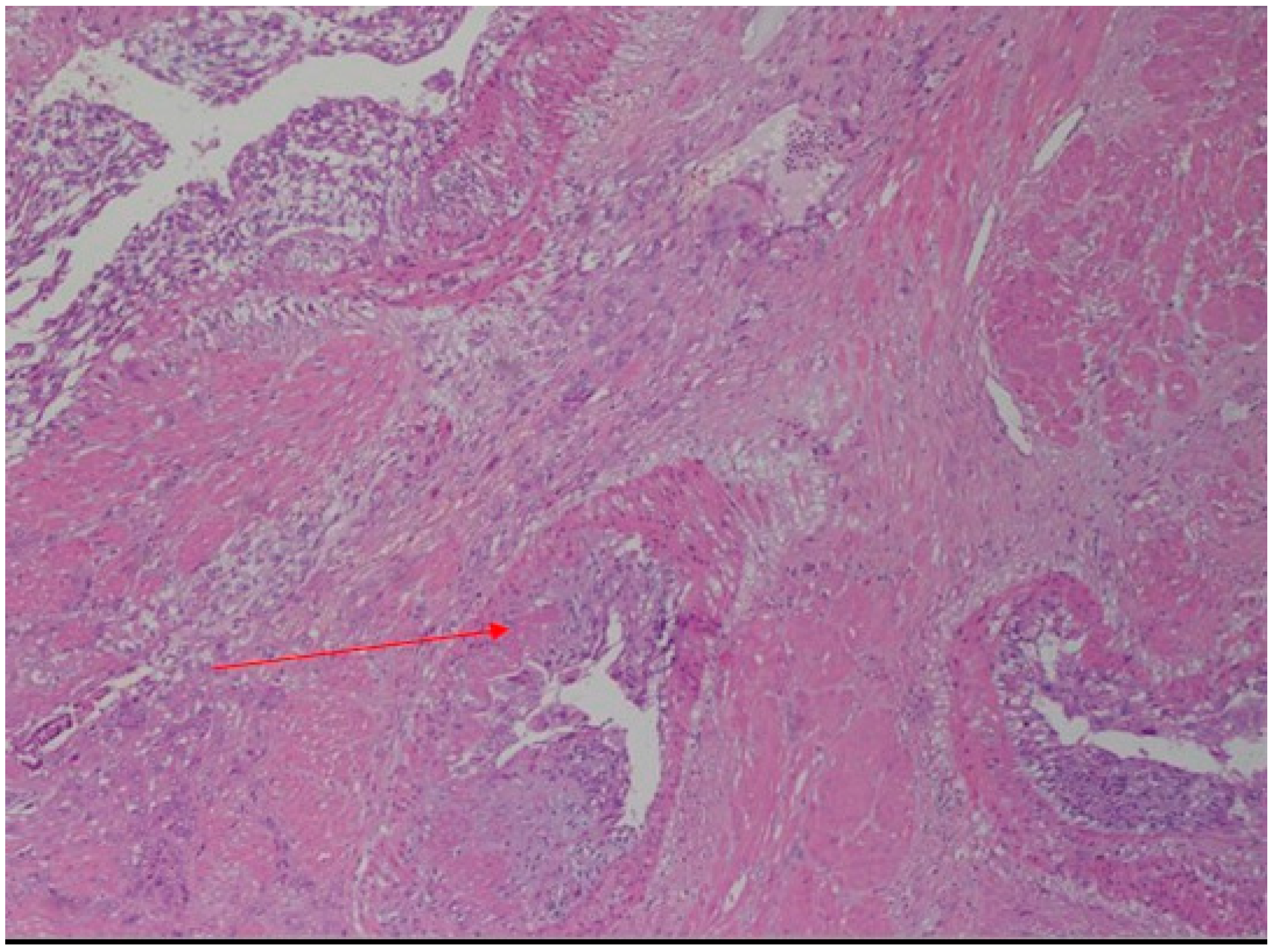
2. Discussion
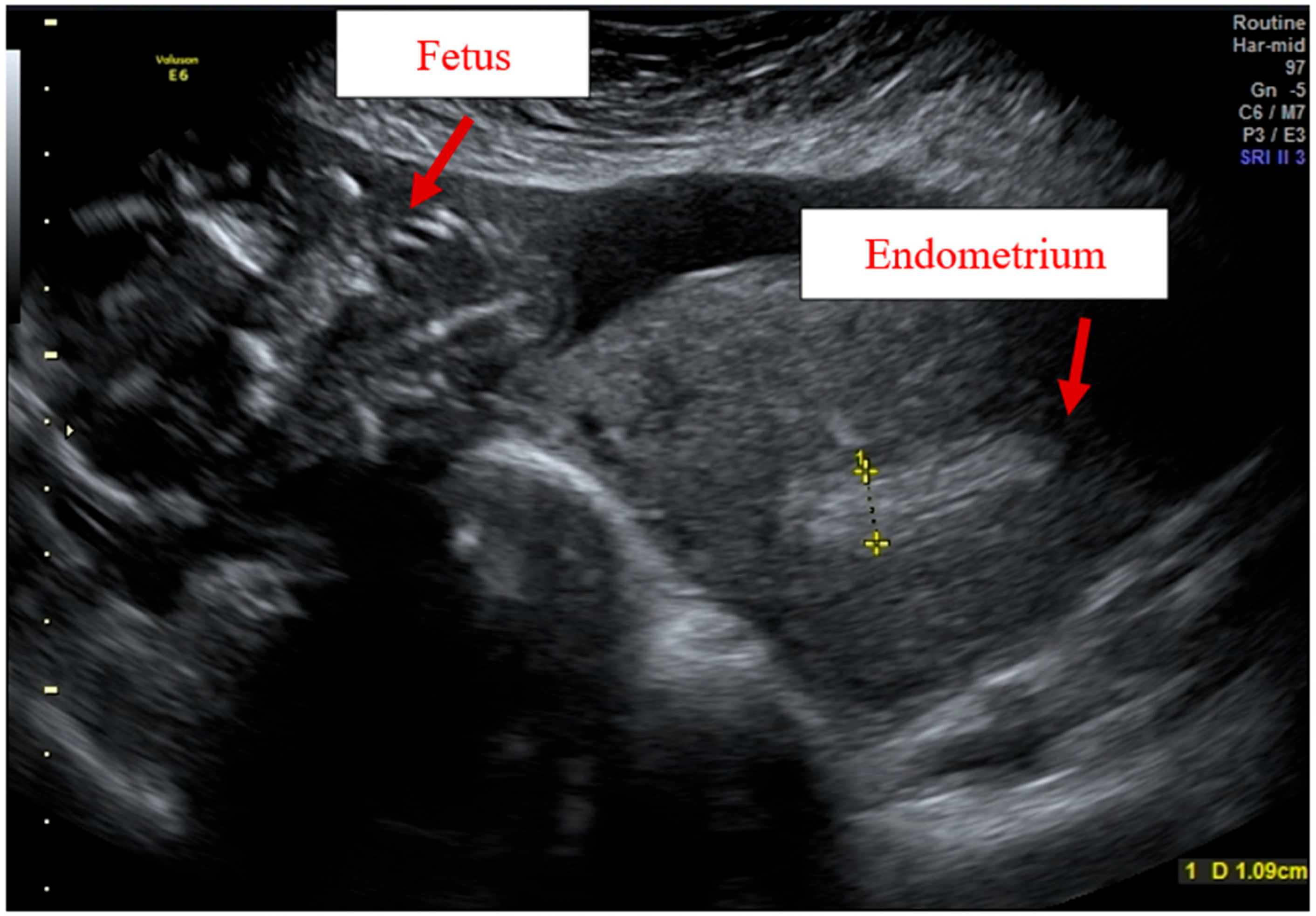
Adenomyosis Ultrasound Diagnosis and Classification
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Agostinho, L.; Cruz, R.; Osório, F.; Alves, J.; Setúbal, A.; Guerra, A. MRI for adenomyosis: A pictorial review. Insights Imaging 2017, 8, 549–556. [Google Scholar] [CrossRef] [Green Version]
- Nelsen, L.M.; Lenderking, W.R.; Pokrzywinski, R.; Balantzc, Z.; Black, L.; Pokras, S.; Enslin, M.B.; Cooper, M.; Lukes, A.S. Experi- ence of symptoms and disease impact in patients with adenomyosis. Patient 2018, 11, 319–328. [Google Scholar] [CrossRef] [Green Version]
- Aleksandrovych, V.; Basta, P.; Gil, K. Current facts constituting an understanding of the nature of adenomyosis. Adv. Clin. Exp. Med. 2018, 28, 839–846. [Google Scholar] [CrossRef]
- Kishi, Y.; Suginami, H.; Kuramori, R.; Yabuta, M.; Suginami, R.; Taniguchi, F. Four subtypes of adenomyosis assessed by magnetic resonance imaging and their specification. Am. J. Obstet. Gynecol. 2012, 207, 114.e1–114.e7. [Google Scholar] [CrossRef]
- Azziz, R. Adenomyosis in pregnancy. A review. J. Reprod. Med. 1986, 31, 224–227. [Google Scholar]
- Bensaid, F.; Kettani, F.; el Fehri, S.; Chraibi, C.; Alaoui, M.T. Les complications obstétricales de l’adénomyose. Revue de la littérature, à propos de 2 observations [Obstetrical complications of adenomyosis. Literature review and two case reports. J. Gynecol. Obstet. Biol. Reprod. 1996, 25, 416–418. [Google Scholar]
- Mueller, M.D.; Saile, G.; Brühwiler, H. Spontane Uterusruptur in der 18. Schwangerschaftswoche bei einer Primigravida mit einer ausgedehnten Adenomyose [Spontaneous uterine rupture in the 18th week of pregnancy in a primigravida patient with adenomyosis]. Zentralbl. Gynakol. 1996, 118, 42–44. [Google Scholar]
- Pafumi, C.; Farina, M.; Pernicone, G.; Russo, A.; Bandiera, S.; Giardina, P.; Cianci, A. Adenomyosis and uterus rupture during labor. Chin. Med. J. 2001, 64, 244–246. [Google Scholar]
- Villa, G.; Mabrouk, M.; Guerrini, M.; Mignemi, G.; Colleoni, G.G.; Venturoli, S.; Seracchioli, R. Uterine Rupture in a Primigravida with Adenomyosis Recently Subjected to Laparoscopic Resection of Rectovaginal Endometriosis: Case Report. J. Minim. Invasive Gynecol. 2008, 15, 360–361. [Google Scholar] [CrossRef]
- Miller, D.A.; Goodwin, T.M.; Gherman, R.B.; Paul, R.H. Intrapartum rupture of the unscarred uterus. Obstet. Gynecol. 1997, 89, 671. [Google Scholar] [CrossRef]
- Jovanovic, B.; Petrovic, A.; Petrovic, B. Decidual transformation in adenomyosis during pregnancy as an indication for hysterectomy. Med. Pregl. 2009, 62, 185–188. [Google Scholar] [CrossRef]
- Nikolaou, M.; Kourea, H.P.; Antonopoulos, K.; Geronatsiou, K.; Adonakis, G.; Decavalas, G. Spontaneous uterine rupture in a primigravid woman in the early third trimester attributed to adenomyosis: A case report and review of the literature. J. Obstet. Gynaecol. Res. 2013, 39, 727. [Google Scholar] [CrossRef]
- Indraccolo, U.; Iannicco, A.; Micucci, G. A novel case of an adenomyosis-related uterine rupture in pregnancy. Clin. Exp. Obstet. Gynecol. 2015, 42, 810–811. [Google Scholar] [CrossRef]
- Li, X.; Li, C.; Sun, M.; Li, H.; Cao, Y.; Wei, Z. Spontaneous unscarred uterine rupture in a twin pregnancy complicated by adenomyosis. Medicine 2021, 100, e24048. [Google Scholar] [CrossRef]
- Sun, H.D.; Su, W.H.; Chang, W.H.; Wen, L.; Huang, B.S.; Wang, P.H. Rupture of a pregnant unscarred uterus in an early secondary trimester: A case report and brief review. J. Obstet. Gynaecol. Res. 2012, 38, 442. [Google Scholar] [CrossRef]
- Chen, L.H.; Tan, K.H.; Yeo, G.S. A ten-year review of uterine rupture in modern obstetric practice. Ann. Acad. Med. Singap. 1995, 24, 830–835. [Google Scholar]
- Wu, X.; Jiang, W.; Xu, H.; Ye, X.; Xu, C. Characteristics of uterine rupture after laparoscopic surgery of the uterus: Clinical analysis of 10 cases and literature review. J. Int. Med. Res. 2018, 46, 3630–3639. [Google Scholar] [CrossRef] [Green Version]
- Signorile, P.G.; Cassano, M.; Viceconte, R.; Spyrou, M.; Marcattilj, V.; Baldi, A. Endometriosis: A Retrospective Analysis on Diagnostic Data in a Cohort of 4,401 Patients. Vivo 2021, 36, 430–438. [Google Scholar] [CrossRef]
- Van den Bosch, T.; de Bruijn, A.M.; de Leeuw, R.A.; Dueholm, M.; Exacoustos, C.; Valentin, L.; Bourne, T.; Timmerman, D.; Huirne, J.A.F. Sonographic classification and reporting system for diagnosing adenomyosis. Ultrasound Obstet. Gynecol. 2019, 53, 576–582. [Google Scholar] [CrossRef]
- Harmsen, M.J.; Bosch, T.V.D.; de Leeuw, R.A.; Dueholm, M.; Exacoustos, C.; Valentin, L.; Hehenkamp, W.; Groenman, F.; De Bruyn, C.; Rasmussen, C.; et al. Consensus on revised definitions of morphological uterus sonographic assessment (MUSA) features of adenomyosis: Results of a modified Delphi procedure. Ultrasound Obstet. Gynecol. 2021. [Google Scholar] [CrossRef]
- Vimercati, A.; Dellino, M.; Crupano, F.M.; Gargano, G.; Cicinelli, E. Ultrasonic assessment of cesarean section scar to vesicovaginal fold distance: An instrument to estimate pre-labor uterine rupture risk. J. Matern. Fetal Neonatal Med. 2021, 1–5. [Google Scholar] [CrossRef]
- Buonomo, B.; Massarotti, C.; Dellino, M.; Anserini, P.; Ferrari, A.; Campanella, M.; Magnotti, M.; De Stefano, C.; Peccatori, F.A.; Lambertini, M. Reproductive issues in carriers of germline pathogenic variants in the BRCA1/2 genes: An expert meeting. BMC Med. 2021, 19, 205. [Google Scholar] [CrossRef]
- Dellino, M.; Silvestris, E.; Loizzi, V.; Paradiso, A.; Loiacono, R.; Minoia, C.; Daniele, A.; Cormio, G. Germinal ovarian tumors in reproductive age women: Fertility-sparing and outcome. Medicine 2020, 99, e22146. [Google Scholar] [CrossRef]
- Silvestris, E.; Cormio, G.; Skrypets, T.; Dellino, M.; Paradiso, A.V.; Guarini, A.; Minoia, C. Novel aspects on gonadotoxicity and fertility preservation in lymphoproliferative neoplasms. Crit. Rev. Oncol. 2020, 151, 102981. [Google Scholar] [CrossRef]
- Silvestris, E.; Dellino, M.; Cafforio, P.; Paradiso, A.V.; Cormio, G.; D’Oronzo, S. Breast cancer: An update on treatment-related infertility. J. Cancer Res. Clin. Oncol. 2020, 146, 647–657. [Google Scholar] [CrossRef]
- Silvestris, E.; D’Oronzo, S.; Cafforio, P.; Kardhashi, A.; Dellino, M.; Cormio, G. In Vitro Generation of Oocytes from Ovarian Stem Cells (OSCs): In Search of Major Evidence. Int. J. Mol. Sci. 2019, 20, 6225. [Google Scholar] [CrossRef] [Green Version]
- Dellino, M.; Carriero, C.; Silvestris, E.; Capursi, T.; Paradiso, A.; Cormio, G. Primary Vaginal Carcinoma Arising on Cystocele Mimicking Vulvar Cancer. J. Obstet Gynaecol Can. 2020, 42, 1543–1545. [Google Scholar] [CrossRef]
- Dellino, M.; Minoia, C.; Paradiso, A.V.; De Palo, R.; Silvestris, E. Fertility Preservation in Cancer Patients During the Coronavirus (COVID-19) Pandemic. Front. Oncol. 2020, 10, 1009. [Google Scholar] [CrossRef]
- Date, S.; Murthy, B.; Magdum, A. Post B-Lynch Uterine Rupture: Case Report and Review of Literature. J. Obstet. Gynecol. India 2013, 64, 362–363. [Google Scholar] [CrossRef] [Green Version]
- Dellino, M.; Crupano, F.M.; Rossi, A.C.; Xuemin, H.; Tinelli, R.; Cicinelli, E.; Vimercati, A. Relationship between prelabour uterine rupture and previous placenta previa diagnosis: Case reports and review of literature. Ital. J. Gynaecol. Obstet. 2022, 34, 48–53. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Author | N° | Age | Gravida/Para | Dysmenorrhea | Endometriosis /Adenomyosis | Infertility | Gestational Age | Labor | FHR | Fetus | Apgar | Transfusion | Hysterectomy | Prognosis |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Azziz (1986) [5] | 1 | 41 | NA/P 10 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| 1 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | |
| 1 | 25 | NA/P0 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | |
| 1 | 38 | NA/P1 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | |
| 1 | 33 | NA/P0 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | |
| 1 | 25 | NA/P1 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | |
| 1 | 36 | NA/P3 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | |
| Bensaid et al. (1996) [6] | 1 | 22 | G1/P1 | NA | NA | No | Term | Yes | Severe bradycardia | 3000 g | 0/2 | NA | No | Newborn demise at 3 days |
| Mueller et al. (1996) [7] | 1 | 30 | G1/P0 | NA | No | Yes | 18 | No | NA | NA | NA | NA | Total hysterectomy | Good |
| Pafumi et al. (2001) [8] | 1 | 30 | G3/P2 | NA | No | No | 37 | Yes | NA | 2750 | 8/10 | NA | Total hysterectomy | Good |
| Villa et al. (2008) [9] | 1 | 30 | G1/P1 | Yes | Rectovaginal septum endometriosis | NA | 37 w + 5 d | Yes | Normal | 2600 | Alive | NA | Rupture 6h postpartum, total hysterectomy | Good |
| Nikolaou et al. (2013) [12] | 1 | 33 | G1/P1 | Yes | Ovarian endometriosis | Yes | 28 | No | Decelerations | 1310 g | 6/6 | 6RBC e 3FFP | Subtotal hysterectomy | Good |
| Indraccolo et al. (2015) [13] | 1 | 37 | G2/P0 | Yes | Laparoscopy with adhesiolysis for chronic pelvic pain- nodule of the uterine posterior wall and diagnosing an adenomyosis | NA | 36 | No | Decelerations | NA | 9/10 | No | No | Good |
| Li et al. (2021) [14] | 1 | 32 | G1/P0- twin pregnancy | Yes | Yes | Yes | 29 | No | NA | Fetus 1—1440 g Fetus 2—1310 g | Fetus 1:3 /8 5/7 | 2RBC | No | Good |
| Present case | 1 | 27 | G0/P0 | Yes | Yes | No | 21 w | No | Severe bradycardia | 460 g | Alive | 2RBC | Total hysterectomy | Good |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vimercati, A.; Dellino, M.; Suma, C.; Damiani, G.R.; Malvasi, A.; Cazzato, G.; Cascardi, E.; Resta, L.; Cicinelli, E. Spontaneous Uterine Rupture and Adenomyosis, a Rare but Possible Correlation: Case Report and Literature Review. Diagnostics 2022, 12, 1574. https://doi.org/10.3390/diagnostics12071574
Vimercati A, Dellino M, Suma C, Damiani GR, Malvasi A, Cazzato G, Cascardi E, Resta L, Cicinelli E. Spontaneous Uterine Rupture and Adenomyosis, a Rare but Possible Correlation: Case Report and Literature Review. Diagnostics. 2022; 12(7):1574. https://doi.org/10.3390/diagnostics12071574
Chicago/Turabian StyleVimercati, Antonella, Miriam Dellino, Cosimina Suma, Gianluca Raffaello Damiani, Antonio Malvasi, Gerardo Cazzato, Eliano Cascardi, Leonardo Resta, and Ettore Cicinelli. 2022. "Spontaneous Uterine Rupture and Adenomyosis, a Rare but Possible Correlation: Case Report and Literature Review" Diagnostics 12, no. 7: 1574. https://doi.org/10.3390/diagnostics12071574
APA StyleVimercati, A., Dellino, M., Suma, C., Damiani, G. R., Malvasi, A., Cazzato, G., Cascardi, E., Resta, L., & Cicinelli, E. (2022). Spontaneous Uterine Rupture and Adenomyosis, a Rare but Possible Correlation: Case Report and Literature Review. Diagnostics, 12(7), 1574. https://doi.org/10.3390/diagnostics12071574