
Cytology and High-Risk Human Papillomavirus Test for Cervical Cancer Screening Assessment

 ,
, 
 ,
,
Abstract
:1. Introduction
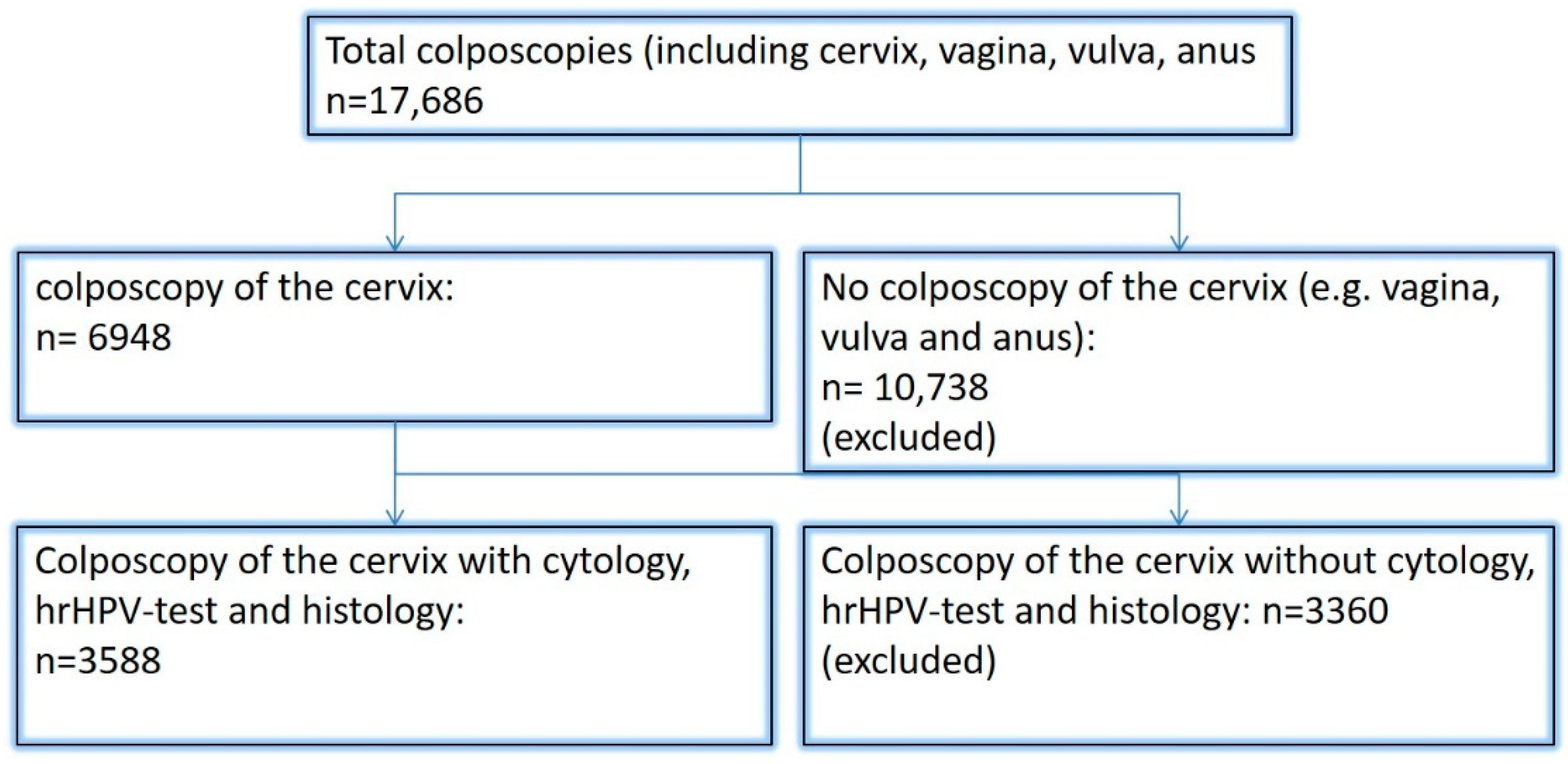
2. Materials and Methods
Statistics
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- Bootstrap Estimation:
References
- Barnes, B.; Kraywinkel, K.; Nowossadeck, E.; Schönfeld, I.; Starker, A.; Wienecke, A.; Wolf, U. RKI Bericht zum Krebsgeschehen in Deutschland 2016. 2016. Available online: https://www.krebsdaten.de/Krebs/DE/Content/Publikationen/Krebsgeschehen/Krebsgeschehen_node.html (accessed on 2 August 2020).
- Stuebs, F.A.; Schulmeyer, C.E.; Mehlhorn, G.; Gass, P.; Kehl, S.; Renner, S.K.; Renner, S.P.; Geppert, C.; Adler, W.; Hartmann, A.; et al. Accuracy of colposcopy-directed biopsy in detecting early cervical neoplasia: A retrospective study. Arch. Gynecol. Obstet. 2019, 299, 525–532. [Google Scholar] [CrossRef]
- Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, Deutsche Krebshilfe, AWMF): S3-Leitlinie Diagnostik, Therapie und Nachsorge der Patientin mit Zervixkarzinom, Langversion, 2.1, 2021, AWMF-Registernummer: 032/033OL. Available online: https://www.leitlinienprogramm-onkologie.de/leitlinien/zervixkarzinom/ (accessed on 1 December 2021).
- Walboomers, J.M.; Jacobs, M.V.; Manos, M.M.; Bosch, F.X.; Kummer, J.A.; Shah, K.V.; Snijders, P.J.; Peto, J.; Meijer, C.J.; Muñoz, N. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J. Pathol. 1999, 189, 12–19. [Google Scholar] [CrossRef]
- Siegler, E.; Shiner, M.; Segev, Y.; Mackuli, L.; Lahat, N.; Lavie, O. Prevalence and Genotype Distribution of HPV Types in Women at Risk for Cervical Neoplasia in Israel. Isr. Med. Assoc. J. 2017, 19, 635–639. [Google Scholar]
- Friebe, K.; Klapdor, R.; Hillemanns, P.; Jentschke, M. The Value of Partial HPV Genotyping After Conization of Cervical Dysplasias. Geburtshilfe Frauenheilkd 2017, 77, 887–893. [Google Scholar] [CrossRef] [Green Version]
- zur Hausen, H. Papillomaviruses and cancer: From basic studies to clinical application. Nat. Rev. Cancer 2002, 2, 342–350. [Google Scholar] [CrossRef]
- Bosch, F.X.; Manos, M.M.; Muñoz, N.; Sherman, M.; Jansen, A.M.; Peto, J.; Schiffman, M.H.; Moreno, V.; Kurman, R.; Shan, K.V.; et al. Prevalence of Human Papillomavirus in Cervical Cancer: A Worldwide Perspective. J. Natl. Cancer Inst. 1995, 87, 796–802. [Google Scholar] [CrossRef]
- De Sanjose, S.; Quint, W.G.; Alemany, L.; Geraets, D.T.; Klaustermeier, J.E.; Lloveras, B.; Tous, S.; Felix, A.; Bravo, L.E.; Shin, H.-R.; et al. Human papillomavirus genotype attribution in invasive cervical cancer: A retrospective cross-sectional worldwide study. Lancet Oncol. 2010, 11, 1048–1056. [Google Scholar] [CrossRef]
- Wang, Z.; Li, Z.; Li, J.; Wang, C.; Wang, W.; Hao, M.; Zhao, C. Prevalence and Distribution of HPV Genotypes in 1387 Women with Cervical Intraepithelial Neoplasia 2/3 in Shanxi Province, China. J. Cancer 2018, 9, 2802–2806. [Google Scholar] [CrossRef]
- Beschluss des Gemeinsamen Bundesausschusses über eine Änderung der Krebsfrüherkennungs-Richtlinie und eine Änderung der Richtlinie für Organisierte Krebsfrüherkennungsprogramme: Programm zur Früherkennung von Zervixkarzinomen 2018. 22 November 2018. Available online: https://www.g-ba.de/downloads/39-261-3597/2018-11-22_oKFE-RL_Zervixkarzinom.pdf (accessed on 2 August 2020).
- Bujan Rivera, J.; Klug, S.J. Cervical cancer screening in Germany. Bundesgesundheitsblatt Gesundh. Gesundh. 2018, 61, 1528–1535. [Google Scholar] [CrossRef]
- Hillemanns, P.; Mallmann, P.; Beckmann, M.W.; Gynecology Oncology Working Group. New Screening Proposals: The Federal Joint Commission Defines the Parameters for Cervical Cancer Screening from 2018: Statement of the Gynecology Oncology Working Group (AGO). Geburtshilfe Frauenheilkd 2016, 76, 145–146. [Google Scholar]
- Hillemanns, P.; Friese, K.; Dannecker, C.; Klug, S.; Seifert, U.; Iftner, T.; Hädicke, J.; Löning, T.; Horn, L.; Schmidt, D.; et al. Prevention of Cervical Cancer: Guideline of the DGGG and the DKG (S3 Level, AWMF Register Number 015/027OL, December 2017)—Part 2 on Triage, Treatment and Follow-up. Geburtshilfe Frauenheilkd 2019, 79, 160–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hillemanns, P.; Friese, K.; Dannecker, C.; Klug, S.; Seifert, U.; Iftner, T.; Hädicke, J.; Löning, T.; Horn, L.; Schmidt, D.; et al. Prevention of Cervical Cancer: Guideline of the DGGG and the DKG (S3 Level, AWMF Register Number 015/027OL, December 2017)—Part 1 with Introduction, Screening and the Pathology of Cervical Dysplasia. Geburtshilfe Frauenheilkd 2019, 79, 148–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hillemanns, P.; Tempfer, C.; Beckmann, M.W.; Küppers, V.; Quaas, J. Statement of the AGO and AG-CPC on the Aftercare/Follow-up for Surgical Procedures of the Lower Genital Tract after the Introduction of a New Cancer Screening Guideline. Geburtshilfe Frauenheilkd 2020, 80, 809–812. [Google Scholar] [CrossRef] [PubMed]
- Schröer-Günther, M.; Fechtelpeter, D.; Zschorlich, B.; Wegmann, M.; Keller, S.; Schürmann, C.; Lampert, U.; Seidl, A.; Janßen, I.; Koch, K. Development of Decision Aids for Organized Cervical Carcinoma Screening in Germany. Gesundheitswesen 2019, 83, 128–134. [Google Scholar]
- Nayar, R.; Wilbur, D.C. The Pap test and Bethesda 2014. Cancer Cytopathol. 2015, 123, 271–281. [Google Scholar] [CrossRef]
- Cirkel, C.; Barop, C.; Beyer, D.A. Method comparison between Munich II and III nomenclature for Pap smear samples. J. Turk. Gynecol. Assoc. 2015, 16, 203–207. [Google Scholar] [CrossRef]
- Münchner Nomenklatur III für die Gynäkologische Zytodiagnostik der Zervix ab 1. July 2014. Available online: http://www.azaed.de/tl_files/azaed/downloads/Verschiedenes/Muenchner%20Nomenklatur%20III.pdf (accessed on 17 January 2021).
- Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, Deutsche Krebshilfe, AWMF): Prävention des Zervixkarzinoms, Langversion 1.1, 2020, AWMF Registernummer: 015/027OL. Available online: http://www.leitlinienprogrammonkologie.de/leitlinien/zervixkarzinom-praevention/ (accessed on 14 July 2021).
- Ronco, G.; Giorgi-Rossi, P.; Carozzi, F.; Confortini, M.; Palma, P.D.; Del Mistro, A.; Ghiringhello, B.; Girlando, S.; Gillio-Tos, A.; De Marco, L.; et al. Efficacy of human papillomavirus testing for the detection of invasive cervical cancers and cervical intraepithelial neoplasia: A randomised controlled trial. Lancet Oncol. 2010, 11, 249–257. [Google Scholar] [CrossRef]
- Kitchener, H.; Almonte, M.; Gilham, C.; Dowie, R.; Stoykova, B.; Sargent, A.; Roberts, C.; Desai, M.; Peto, J. ARTISTIC: A randomised trial of human papillomavirus (HPV) testing in primary cervical screening. Health Technol. Assess. 2009, 13, 1–150, iii–iv. [Google Scholar] [CrossRef] [Green Version]
- Leinonen, M.K.; Nieminen, P.; Lönnberg, S.; Malila, N.; Hakama, M.; Pokhrel, A.; Laurila, P.; Tarkkanen, J.; Anttila, A. Detection rates of precancerous and cancerous cervical lesions within one screening round of primary human papillomavirus DNA testing: Prospective randomised trial in Finland. BMJ 2012, 345, e7789. [Google Scholar] [CrossRef] [Green Version]
- Rijkaart, D.C.; Berkhof, J.; Rozendaal, L.; van Kemenade, F.J.; Bulkmans, N.W.; Heideman, D.A.; Kenter, G.G.; Cuzick, J.; Snijders, P.J.; Meijer, C.J. Human papillomavirus testing for the detection of high-grade cervical intraepithelial neoplasia and cancer: Final results of the POBASCAM randomised controlled trial. Lancet Oncol. 2012, 13, 78–88. [Google Scholar] [CrossRef]
- Naucler, P.; Ryd, W.; Törnberg, S.; Strand, A.; Wadell, G.; Elfgren, K.; Rådberg, T.; Strander, B.; Johansson, B.; Forslund, O.; et al. Human Papillomavirus and Papanicolaou Tests to Screen for Cervical Cancer. N. Engl. J. Med. 2007, 357, 1589–1597. [Google Scholar] [CrossRef] [PubMed]
- Jentschke, M.; Soergel, P.; Hillemanns, P. Importance of HPV Genotyping for the Screening, Therapy and Management of Cervical Neoplasias. Geburtshilfe Frauenheilkd 2012, 72, 507–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luyten, A.; Buttmann-Schweiger, N.; Luyten, K.; Mauritz, C.; Reinecke-Lüthge, A.; Pietralla, M.; Meijer, C.J.; Petry, K.U. Early detection of CIN3 and cervical cancer during long-term follow-up using HPV/Pap smear co-testing and risk-adapted follow-up in a locally organised screening programme. Int. J. Cancer 2014, 135, 1408–1416. [Google Scholar] [CrossRef] [PubMed]
- Katki, H.A.; Schiffman, M.; Castle, P.E.; Fetterman, B.; Poitras, N.E.; Lorey, T.; Cheung, L.; Raine-Bennett, T.; Gage, J.C.; Kinney, W.K. Five-Year Risks of CIN 3+ and Cervical Cancer Among Women with HPV Testing of ASC-US Pap Results. J. Low. Genit. Tract Dis. 2013, 17 (Suppl. 1), S36–S42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, T.C., Jr.; Behrens, C.M.; Ranger-Moore, J.; Rehm, S.; Sharma, A.; Stoler, M.H.; Ridder, R. Triaging HPV-positive women with p16/Ki-67 dual-stained cytology: Results from a sub-study nested into the ATHENA trial. Gynecol. Oncol. 2017, 144, 51–56. [Google Scholar] [CrossRef]
- Luyten, A.; Petry, K.U. Relevance of HPV Screening for Triaging Equivocal Cytology Findings in the Pap II-p, Pap III and Pap IIID Groups—Results of Two Long-Term Studies. Geburtshilfe Frauenheilkd 2015, 75, 1058–1062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katki, H.A.; Schiffman, M.; Castle, P.E.; Fetterman, B.; Poitras, N.E.; Lorey, T.; Cheung, L.C.; Raine-Bennett, T.; Gage, J.C.; Kinney, W.K. Five-Year Risks of CIN 2+ and CIN 3+ Among Women With HPV-Positive and HPV-Negative LSIL Pap Results. J. Low. Genit. Tract Dis. 2013, 17 (Suppl. 1), S43–S49. [Google Scholar] [CrossRef] [Green Version]
- Arbyn, M.; Roelens, J.; Simoens, C.; Buntinx, F.; Paraskevaidis, E.; Martin-Hirsch, P.P.; Prendiville, W.J. Human papillomavirus testing versus repeat cytology for triage of minor cytological cervical lesions. Cochrane Database Syst. Rev. 2013, 2023, CD008054. [Google Scholar]
- Arbyn, M.; Verdoodt, F.; Snijders, P.J.F.; Verhoef, V.M.J.; Suonio, E.; Dillner, L.; Minozzi, S.; Bellisario, C.; Banzi, R.; Zhao, F.-H.; et al. Accuracy of human papillomavirus testing on self-collected versus clinician-collected samples: A meta-analysis. Lancet Oncol. 2014, 15, 172–183. [Google Scholar] [CrossRef]
- Beckmann, M.W.; Quaas, J.; Bischofberger, A.; Kämmerle, A.; Lux, M.P.; Wesselmann, S. Establishment of the Certification System “Gynaecological Dysplasia” in Germany. Geburtshilfe Frauenheilkd 2014, 74, 860–867. [Google Scholar] [CrossRef] [Green Version]
- Seidel, D.; Becker, N.; Rohrmann, S.; Nimptsch, K.; Linseisen, J. Socio-demographic characteristics of participation in the opportunistic German cervical cancer screening programme: Results from the EPIC-Heidelberg cohort. J. Cancer Res. Clin. Oncol. 2009, 135, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Poljak, M.; Oštrbenk, A.; Seme, K.; Šterbenc, A.; Jančar, N.; Bokal, E.V. Three-year longitudinal data on the clinical performance of the Abbott RealTime High Risk HPV test in a cervical cancer screening setting. J. Clin. Virol. 2016, 76 (Suppl. 1), S29–S39. [Google Scholar] [CrossRef] [PubMed]
- Mongia, A.; Pompeo, G.; Sani, C.; Burroni, E.; Fantacci, G.; Bisanzi, S.; Cellai, F.; Ventura, L.; Bottari, F.; Carozzi, F. Hybrid capture 2 and cobas® 4800: Comparison of performance of two clinically validated tests for human papillomavirus primary screening of cervical cancer. J. Med Screen. 2021, 28, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Carozzi, F.M.; Burroni, E.; Bisanzi, S.; Puliti, D.; Confortini, M.; Giorgi Rossi, P.; Sani, C.; Scalisi, A.; Chini, F. Comparison of clinical performance of Abbott RealTime High Risk HPV test with that of hybrid capture 2 assay in a screening setting. J. Clin. Microbiol. 2011, 49, 1446–1451. [Google Scholar] [CrossRef] [Green Version]
- Team, R.C. A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.R-project.org/ (accessed on 1 April 2021).
- Marquardt, K.; Kossowski, I.; Pfandzelter, R. Münchner Nomenklatur III—Bundesweite Jahresstatistik nach der Nomenklaturreform. Frauenarzt 2017 [Cited No. 9 17.01.2021]. Available online: https://www.ag-cpc.de/wp-content/uploads/2018/07/FA-2017-9_BERUF_Jahresstatistik_Zervix-Zytologie-1.pdf (accessed on 17 January 2021).
- Marquardt, K.; Kossowski, I.; Hantschke-Zerbich, H.; Michel, F. An der Schwelle zum organisierten Zervixkarzinomscreening. Der Gynäkologe 2019, 52, 622–627. [Google Scholar] [CrossRef]
- Meijer, C.J.; Berkhof, J.; Castle, P.E.; Hesselink, A.T.; Franco, E.L.; Ronco, G.; Arbyn, M.; Bosch, F.X.; Cuzick, J.; Dillner, J.; et al. Guidelines for human papillomavirus DNA test requirements for primary cervical cancer screening in women 30 years and older. Int. J. Cancer 2009, 124, 516–520. [Google Scholar] [CrossRef] [Green Version]
- Stoler, M.H.; Castle, P.E.; Solomon, D.; Schiffman, M. The expanded use of HPV testing in gynecologic practice per ASCCP-guided management requires the use of well-validated assays. Am. J. Clin. Pathol. 2007, 127, 335–337. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Subdivision | Munich III | Bethesda |
|---|---|---|
| Benign | I; | NILM |
| II-a; | NILM | |
| II-g | AGC endocervical NOS | |
| II-p | ASC-US | |
| LSIL | IIID1 | LSIL |
| HSIL+ | IIID2 | HSIL |
| IVa-p | HSIL | |
| IVa-g | AIS | |
| IVb-p | HSIL with features suspicious for invasion | |
| IVb-g | AIS with features suspicious for invasion | |
| V-e | endometrial adenocarcinoma | |
| V-g | endocervical adenocarcinoma | |
| V-p | squamous cell carcinoma | |
| V-x | other malignant neoplasms | |
| Unspecific | III-e | AGC endometrial |
| III-g | AGC endocervical favoring neoplasia | |
| III-p | ASC-H | |
| III-x | AGC favoring neoplasia |
| Pap Smears with Histology (n = 3588) (3118 Women) | Bethesda System | hrHPV-Positive (n = 2369) | hrHPV-Negative (n = 1219) | Benign (n = 597) | CIN 1/LSIL (n = 964) | CIN 2/HSIL (n = 442) | CIN 3/AIS/HSIL (n = 1452) | Carcinoma (n = 133) |
|---|---|---|---|---|---|---|---|---|
| 0 (n = 10) | Unsatisfactory for evaluation | 5 (50%) | 1 (20%) | 3 (60%) | 0 | 1 (20%) | 0 | |
| 0 | Unsatisfactory for evaluation | 5 (50%) | 3 (60%) | 2 (40%) | 0 | 0 | 0 | |
| I (n = 297) | NILM | 40 (13.5%) | 25 (62.5%) | 12 (30%) | 2 (5%) | 1 (2.5%) | 0 | |
| I | NILM | 257 (86.5%) | 165 (64.2%) | 89 (34.6%) | 3 (1.2%) | 0 | 0 | |
| II-a (n = 246) | NILM | 54 (21.9%) | 16 (29.6%) | 29 (53.7%) | 6 (11.1%) | 3 (5.6%) | 0 | |
| II-a | NILM | 192 (78.0%) | 72 (37.5%) | 111 (57.8%) | 4 (2.1%) | 4 (2.1%) | 1 (0.5%) | |
| II-g (n = 6) | AGC endocervical NOS | 2 (33.3%) | 0 | 0 | 0 | 1 (50%) | 1 (50%) | |
| II-g | AGC endocervical NOS | 4 (66.6%) | 2 (50%) | 2 (50%) | 0 | 0 | 0 | |
| II-p (n = 144) | ASC-US | 49 (34.1%) | 13 (26.5%) | 18 (36.7%) | 7 (14.3%) | 11 (22.4%) | 0 | |
| II-p | ASC-US | 95 (65.9%) | 53 (55.8%) | 33 (34.7%) | 8 (8.4%) | 1 (1.1%) | 0 | |
| IIID1 (n = 663) | LSIL | 325 (49.1%) | 42 (12.9%) | 175 (53.8%) | 62 (19.1%) | 46 (14.1%) | 0 | |
| IIID1 | LSIL | 338 (50.9%) | 74 (21.9%) | 213 (63.0%) | 39 (11.5%) | 12 (3.6%) | 0 | |
| IIID2 (n = 508) | HSIL | 401 (78.9%) | 27 (6.7%) | 79 (19.7%) | 136 (33.9%) | 157 (39.2%) | 2 (0.5%) | |
| IIID2 | HSIL | 107 (21.1%) | 17 (15.9%) | 46 (43%) | 34 (31.8%) | 10 (9.3%) | 0 | |
| III-e (n = 1) | AGC endometrial | 0 | 0 | 0 | 0 | 0 | 0 | |
| III-e | AGC endometrial | 1 (100%) | 1 (100%) | 0 | 0 | 0 | 0 | |
| III-g (n = 63) | AGC endocervical favoring neoplasia | 42 (66.7%) | 7 (16.6%) | 9 (21.4%) | 7 (16.6%) | 14 (33.3%) | 5 (11.9%) | |
| III-g | AGC endocervical favoring neoplasia | 21 (33.3%) | 11 (52.4%) | 7 (33.3%) | 3 (14.3%) | 0 | 0 | |
| III-p (n = 258) | ASC-H | 168 (65.1%) | 20 (11.9%) | 25 (14.9%) | 18 (10.7%) | 102 (60.7%) | 3 (1.8%) | |
| III-p | ASC-H | 90 (34.9%) | 13 (14.4%) | 49 (54.4%) | 16 (17.8%) | 12 (13.3%) | 0 | |
| III-x (n = 3) | AGC favoring neoplasia | 0 | 0 | 0 | 0 | 0 | 0 | |
| III-x | AGC favoring neoplasia | 3 (100%) | 2 (66.6%) | 1 (33.3%) | 0 | 0 | 0 | |
| IVa-p (n = 1120) | HSIL | 1032 (92.1%) | 20 (1.9%) | 40 (3.9%) | 81 (7.8%) | 865 (83.8%) | 26 (2.5%) | |
| IVa-p | HSIL | 88 (7.9%) | 9 (10.2%) | 13 (14.8%) | 10 (11.4%) | 53 (60.2%) | 3 (3.4%) | |
| IVa-g (n = 17) | AIS | 15 (88.2%) | 2 (11.8%) | 2 (11.8%) | 0 | 9 (52.9%) | 2 (11.8%) | |
| IVa-g | AIS | 2 (11.8%) | 1 (50%) | 1 (50%) | ||||
| IVb-p (n = 142) | HSIL with features suspicious for invasion | 132 (92.9%) | 1 (0.8%) | 4 (3.0%) | 5 (3.8%) | 111 (84.1%) | 11 (8.3%) | |
| IVb-p | HSIL with features suspicious for invasion | 10 (7.0%) | 0 | 1 (10%) | 0 | 7 (70%) | 2 (20%) | |
| IVb-g (n = 9) | AIS with features suspicious for invasion | 8 (88.9%) | 0 | 0 | 0 | 5 (62.5%) | 3 (37.5%) | |
| IVb-g | AIS with features suspicious for invasion | 1 (11.1%) | 0 | 0 | 0 | 1 (100%) | 0 | |
| V-p (n = 86) | Squamous cell carcinoma | 81 (94.2%) | 0 | 0 | 1 (1.2%) | 24 (27.9%) | 56 (65.1%) | |
| V-p | Squamous cell carcinoma | 5 (5.8%) | 0 | 0 | 0 | 1 (20%) | 4 (80%) | |
| V-g (n = 12) | Endocervical adenocarcinoma | 12 (100%) | 0 | 0 | 0 | 1 (8.3%) | 11 (91.7) | |
| V-g | Endocervical adenocarcinoma | 0 | 0 | 0 | 0 | 0 | 0 | |
| V-e (n = 1) | Endometrial adenocarcinoma | 1 (100%) | 0 | 0 | 0 | 0 | 1 (100%) | |
| V-e | Endometrial adenocarcinoma | 0 | 0 | 0 | 0 | 0 | 0 | |
| V-x (n = 2) | Other malignant neoplasms | 2 (100%) | 0 | 0 | 0 | 0 | 2 (100%) | |
| V-x | Other malignant neoplasms | 0 | 0 | 0 | 0 | 0 | 0 |
| Pap Smear (n = 1409) | hrHPV-Positive (n = 1137) | hrHPV-Negative (n = 272) | Benign (n = 108) | CIN 1 (n = 311) | CIN 2 (n = 222) | CIN 3/AIS (n = 753) | Carcinoma (n = 15) |
|---|---|---|---|---|---|---|---|
| Pap IIID1 (n = 347) | 195 (56.2%) | 28 (14.6%) | 103 (52.8%) | 37 (19.0%) | 27 (13.8%) | 0 | |
| Pap IIID1 | 152 (43.8%) | 25 (16.4%) | 93 (61.2%) | 25 (16.4%) | 9 (5.9%) | 0 | |
| Pap IIID2 (n = 286) | 239 (83.6%) | 14 (5.6%) | 58 (24.3%) | 80 (33.5%) | 85 (35.6%) | 2 (0.8%) | |
| Pap IIID2 | 47 (16.4%) | 12 (25.5%) | 11 (23.4%) | 18 (38.3%) | 6 (12.8%) | 0 | |
| Pap III-p (n = 100) | 77 (77%) | 5 (6.5%) | 9 (11.7%) | 7 (9.1%) | 55 (71.4%) | 1 (1.3%) | |
| Pap III-p | 23 (23%) | 3 (13.0%) | 9 (39.1%) | 6 (26.1%) | 5 (21.7%) | 0 | |
| Pap IVa-p (n = 676) | 626 (92.6%) | 14 (2.2%) | 19 (3.0%) | 45 (7.2%) | 538 (85.9%) | 10 (1.6%) | |
| Pap IVa-p | 50 (7.4%) | 7 (14.0%) | 9 (18.0%) | 4 (8.0%) | 28 (58%) | 2 (4.0%) |
| Pap Smear (n = 1140) | hrHPV-Positive (n = 789) | hrHPV-Negative (n = 351) | Benign (n = 114) | CIN I (n = 329) | CIN II (n = 174) | CIN III/AIS (n = 504) | Carcinoma (n = 19) |
|---|---|---|---|---|---|---|---|
| Pap IIID1 (n = 316) | 130 (41.1%) | 14 (10.8%) | 72 (55.4%) | 25 (19.2%) | 19 (14.6%) | 0 | |
| Pap IIID1 | 186 (58.9%) | 49 (26.3%) | 120 (64.5%) | 14 (7.5%) | 3 (1.6%) | 0 | |
| Pap IIID2 (n = 222) | 162 (73.0%) | 13 (8.0%) | 21 (9.5%) | 56 (25.2%) | 72 (32.4%) | 0 | |
| Pap IIID2 | 60 (27%) | 5 (8.3%) | 35 (58.3%) | 16 (26.7%) | 4 (6.7%) | 0 | |
| Pap III-p (n = 158) | 91 (57.6%) | 15 (9.5%) | 16 (17.6%) | 11 (12.1%) | 47 (51.6%) | 2 (2.2%) | |
| Pap III-p | 67 (42.4%) | 10 (14.9%) | 40 (59.7%) | 10 (14.9%) | 7 (10.4%) | 0 | |
| Pap IVa-p (n = 444) | 406 (91.4%) | 6 (1.5%) | 21 (5.2%) | 36 (8.1%) | 327 (80.5%) | 16 (3.9%) | |
| Pap IVa-p | 38 (8.6%) | 2 (5.3%) | 4 (10.5%) | 6 (15.8%) | 25 (65.8%) | 1 (2.6%) |
| Pap (Reference Benign) | OR | 95% CI | p |
|---|---|---|---|
| LSIL | 2.52 | 1.765; 3.604 | <0.001 |
| HSIL+ | 34.27 | 24.629; 47.671 | <0.001 |
| Unspecific | 9.24 | 6.346; 13.46 | <0.001 |
| HPV (reference: negative HPV co-test) | |||
| Positive HPV co-test | 5.07 | 4.068; 6.329 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stuebs, F.A.; Koch, M.C.; Dietl, A.K.; Adler, W.; Geppert, C.; Hartmann, A.; Knöll, A.; Beckmann, M.W.; Mehlhorn, G.; Schulmeyer, C.E.; et al. Cytology and High-Risk Human Papillomavirus Test for Cervical Cancer Screening Assessment. Diagnostics 2022, 12, 1748. https://doi.org/10.3390/diagnostics12071748
Stuebs FA, Koch MC, Dietl AK, Adler W, Geppert C, Hartmann A, Knöll A, Beckmann MW, Mehlhorn G, Schulmeyer CE, et al. Cytology and High-Risk Human Papillomavirus Test for Cervical Cancer Screening Assessment. Diagnostics. 2022; 12(7):1748. https://doi.org/10.3390/diagnostics12071748
Chicago/Turabian StyleStuebs, Frederik A., Martin C. Koch, Anna K. Dietl, Werner Adler, Carol Geppert, Arndt Hartmann, Antje Knöll, Matthias W. Beckmann, Grit Mehlhorn, Carla E. Schulmeyer, and et al. 2022. "Cytology and High-Risk Human Papillomavirus Test for Cervical Cancer Screening Assessment" Diagnostics 12, no. 7: 1748. https://doi.org/10.3390/diagnostics12071748
APA StyleStuebs, F. A., Koch, M. C., Dietl, A. K., Adler, W., Geppert, C., Hartmann, A., Knöll, A., Beckmann, M. W., Mehlhorn, G., Schulmeyer, C. E., & Gass, P. (2022). Cytology and High-Risk Human Papillomavirus Test for Cervical Cancer Screening Assessment. Diagnostics, 12(7), 1748. https://doi.org/10.3390/diagnostics12071748