
Prognosis Associated with Glycolytic Activity in Regional Lymph Nodes of Patients with Previously Untreated Metastatic Breast Cancer: A Preliminary Study


Abstract
:1. Introduction
2. Materials and Methods
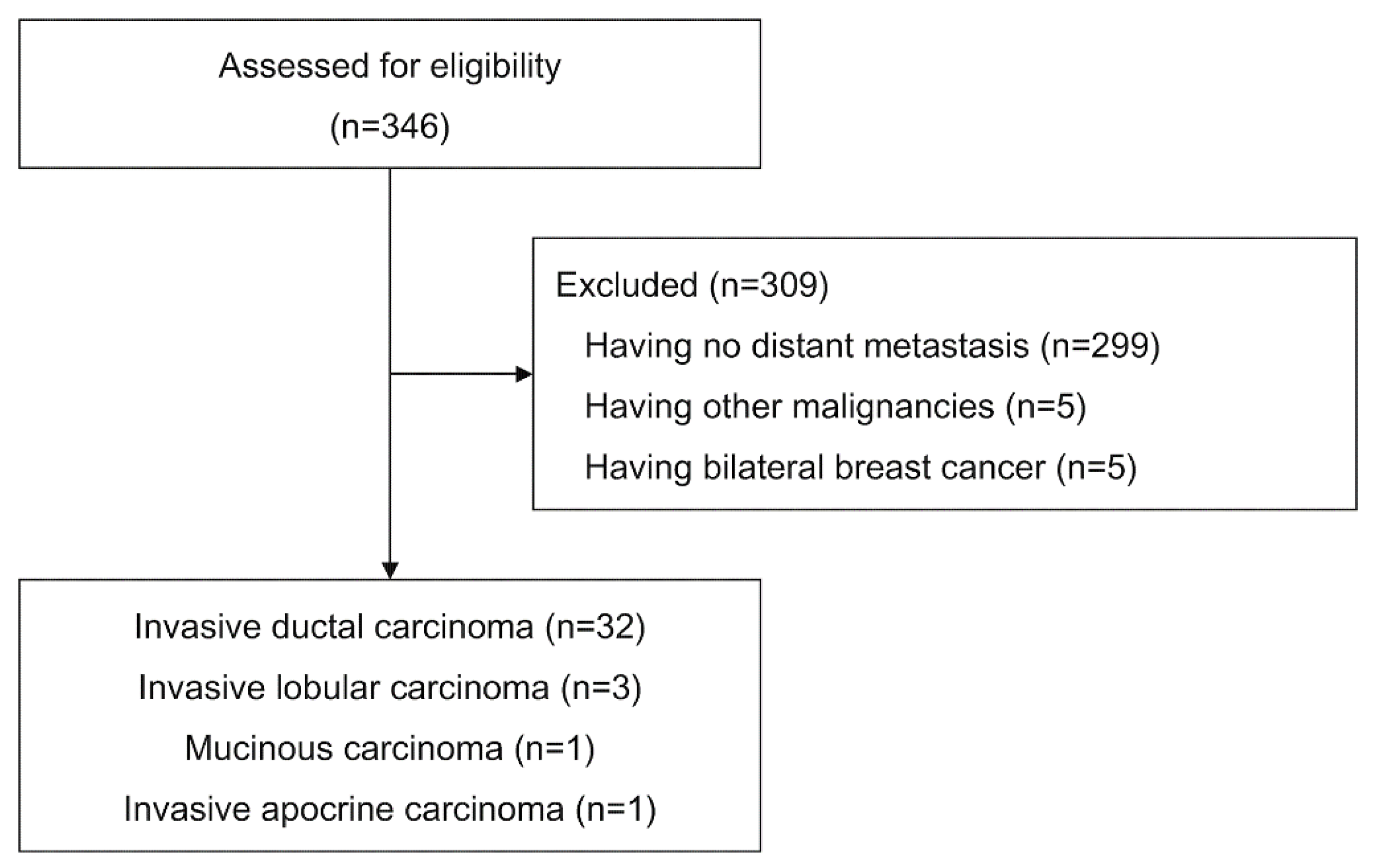
2.1. Patients
2.2. PET/CT Imaging
2.3. Image Analysis
2.4. Statistical Analysis
3. Results
3.1. Image Analysis
3.2. Analysis of Prognostic Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chung, C.T.; Carlson, R.W. Goals and objectives in the management of metastatic breast cancer. Oncologist 2003, 8, 514–520. [Google Scholar] [CrossRef]
- Dawood, S.; Broglio, K.; Gonzalez-Angulo, A.M.; Buzdar, A.U.; Hortobagyi, G.N.; Giordano, S.H. Trends in survival over the past two decades among white and black patients with newly diagnosed stage IV breast cancer. J. Clin. Oncol. 2008, 26, 4891–4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chia, S.K.; Speers, C.H.; D’Yachkova, Y.; Kang, A.; Malfair-Taylor, S.; Barnett, J.; Coldman, A.; Gelmon, K.A.; O’Reilly, S.E.; Olivotto, I.A. The impact of new chemotherapeutic and hormone agents on survival in a population-based cohort of women with metastatic breast cancer. Cancer 2007, 110, 973–979. [Google Scholar] [CrossRef]
- Gennari, A.; Conte, P.; Rosso, R.; Orlandini, C.; Bruzzi, P. Survival of metastatic breast carcinoma patients over a 20-year period: A retrospective analysis based on individual patient data from six consecutive studies. Cancer 2005, 104, 1742–1750. [Google Scholar] [CrossRef]
- Falkson, G.; Holcroft, C.; Gelman, R.S.; Tormey, D.C.; Wolter, J.M.; Cummings, F.J. Ten-year follow-up study of premenopausal women with metastatic breast cancer: An Eastern Cooperative Oncology Group study. J. Clin. Oncol. 1995, 13, 1453–1458. [Google Scholar] [CrossRef]
- Greenberg, P.A.; Hortobagyi, G.N.; Smith, T.L.; Ziegler, L.D.; Frye, D.K.; Buzdar, A.U. Long-term follow-up of patients with complete remission following combination chemotherapy for metastatic breast cancer. J. Clin. Oncol. 1996, 14, 2197–2205. [Google Scholar] [CrossRef]
- Eubank, W.B.; Mankoff, D.A. Evolving role of positron emission tomography in breast cancer imaging. Semin. Nucl. Med. 2005, 35, 84–99. [Google Scholar] [CrossRef] [PubMed]
- Gradishar, W.J.; Moran, M.S.; Abraham, J.; Aft, R.; Agnese, D.; Allison, K.H.; Anderson, B.; Burstein, H.J.; Chew, H.; Dang, C.; et al. Breast Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2022, 20, 691–722. [Google Scholar] [CrossRef] [PubMed]
- Gennari, A.; Andre, F.; Barrios, C.H.; Cortes, J.; de Azambuja, E.; DeMichele, A.; Dent, R.; Fenlon, D.; Gligorov, J.; Hurvitz, S.A.; et al. ESMO Clinical Practice Guideline for the diagnosis, staging and treatment of patients with metastatic breast cancer. Ann. Oncol. 2021, 32, 1475–1495. [Google Scholar] [CrossRef] [PubMed]
- Couturier, O.; Jerusalem, G.; N’Guyen, J.M.; Hustinx, R. Sequential positron emission tomography using [18F]fluorodeoxyglucose for monitoring response to chemotherapy in metastatic breast cancer. Clin. Cancer Res. 2006, 12, 6437–6443. [Google Scholar] [CrossRef] [Green Version]
- Dose Schwarz, J.; Bader, M.; Jenicke, L.; Hemminger, G.; Janicke, F.; Avril, N. Early prediction of response to chemotherapy in metastatic breast cancer using sequential 18F-FDG PET. J. Nucl. Med. 2005, 46, 1144–1150. [Google Scholar] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Weber, W.A.; Ziegler, S.I.; Thodtmann, R.; Hanauske, A.R.; Schwaiger, M. Reproducibility of metabolic measurements in malignant tumors using FDG PET. J. Nucl. Med. 1999, 40, 1771–1777. [Google Scholar]
- Schoenfeld, D. Partial residuals for the proportional hazards regression model. Biometrika 1982, 69, 239–241. [Google Scholar] [CrossRef]
- Akaike, H. Information theory and an extension of the maximum likelihood principle. In Proceedings of the 2nd International Symposium on Information Theory, Budapest, Hungary, 2–8 September 1973; pp. 267–281. [Google Scholar]
- Simmons, C.; Miller, N.; Geddie, W.; Gianfelice, D.; Oldfield, M.; Dranitsaris, G.; Clemons, M.J. Does confirmatory tumor biopsy alter the management of breast cancer patients with distant metastases? Ann. Oncol. 2009, 20, 1499–1504. [Google Scholar] [CrossRef] [PubMed]
- Amir, E.; Clemons, M. Should a biopsy be recommended to confirm metastatic disease in women with breast cancer? Lancet Oncol. 2009, 10, 933–935. [Google Scholar] [CrossRef]
- Symmans, W.F.; Liu, J.; Knowles, D.M.; Inghirami, G. Breast cancer heterogeneity: Evaluation of clonality in primary and metastatic lesions. Hum. Pathol. 1995, 26, 210–216. [Google Scholar] [CrossRef]
- Kuukasjarvi, T.; Karhu, R.; Tanner, M.; Kahkonen, M.; Schaffer, A.; Nupponen, N.; Pennanen, S.; Kallioniemi, A.; Kallioniemi, O.P.; Isola, J. Genetic heterogeneity and clonal evolution underlying development of asynchronous metastasis in human breast cancer. Cancer Res. 1997, 57, 1597–1604. [Google Scholar]
- Giuliano, A.E.; Edge, S.B.; Hortobagyi, G.N. Eighth Edition of the AJCC Cancer Staging Manual: Breast Cancer. Ann. Surg. Oncol. 2018, 25, 1783–1785. [Google Scholar] [CrossRef] [PubMed]
- Lonning, P.E. Breast cancer prognostication and prediction: Are we making progress? Ann. Oncol. 2007, 18 (Suppl. S8), viii3–viii7. [Google Scholar] [CrossRef] [PubMed]
- Warburg, O.; Dickens, F.; Kaiser-Wilhelm-Institut für Biologie. The Metabolism of Tumours, Investigations from the Kaiser Wilhelm Institute for Biology, Berlin-Dahlem; Constable & Co., Ltd.: London, UK, 1930. [Google Scholar]
- Sun, R.C.; Fadia, M.; Dahlstrom, J.E.; Parish, C.R.; Board, P.G.; Blackburn, A.C. Reversal of the glycolytic phenotype by dichloroacetate inhibits metastatic breast cancer cell growth in vitro and in vivo. Breast Cancer Res. Treat. 2010, 120, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Funasaka, T.; Hogan, V.; Raz, A. Phosphoglucose isomerase/autocrine motility factor mediates epithelial and mesenchymal phenotype conversions in breast cancer. Cancer Res. 2009, 69, 5349–5356. [Google Scholar] [CrossRef] [Green Version]
- Oshida, M.; Uno, K.; Suzuki, M.; Nagashima, T.; Hashimoto, H.; Yagata, H.; Shishikura, T.; Imazeki, K.; Nakajima, N. Predicting the prognoses of breast carcinoma patients with positron emission tomography using 2-deoxy-2-fluoro[18F]-D-glucose. Cancer 1998, 82, 2227–2234. [Google Scholar] [CrossRef] [Green Version]
- Crippa, F.; Seregni, E.; Agresti, R.; Chiesa, C.; Pascali, C.; Bogni, A.; Decise, D.; De Sanctis, V.; Greco, M.; Daidone, M.G.; et al. Association between [18F]fluorodeoxyglucose uptake and postoperative histopathology, hormone receptor status, thymidine labelling index and p53 in primary breast cancer: A preliminary observation. Eur. J. Nucl. Med. 1998, 25, 1429–1434. [Google Scholar] [CrossRef]
- Avril, N.; Menzel, M.; Dose, J.; Schelling, M.; Weber, W.; Janicke, F.; Nathrath, W.; Schwaiger, M. Glucose metabolism of breast cancer assessed by 18F-FDG PET: Histologic and immunohistochemical tissue analysis. J. Nucl. Med. 2001, 42, 9–16. [Google Scholar] [PubMed]
- Buck, A.; Schirrmeister, H.; Kuhn, T.; Shen, C.; Kalker, T.; Kotzerke, J.; Dankerl, A.; Glatting, G.; Reske, S.; Mattfeldt, T. FDG uptake in breast cancer: Correlation with biological and clinical prognostic parameters. Eur. J. Nucl. Med. Mol. Imaging 2002, 29, 1317–1323. [Google Scholar] [CrossRef] [PubMed]
- Gil-Rendo, A.; Martinez-Regueira, F.; Zornoza, G.; Garcia-Velloso, M.J.; Beorlegui, C.; Rodriguez-Spiteri, N. Association between [18F]fluorodeoxyglucose uptake and prognostic parameters in breast cancer. Br. J. Surg. 2009, 96, 166–170. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.S.; Leung, J.Y.; Fisher, S.J.; Frey, K.A.; Ethier, S.P.; Wahl, R.L. Intratumoral distribution of tritiated-FDG in breast carcinoma: Correlation between Glut-1 expression and FDG uptake. J. Nucl. Med. 1996, 37, 1042–1047. [Google Scholar]
- Bos, R.; van Der Hoeven, J.J.; van Der Wall, E.; van Der Groep, P.; van Diest, P.J.; Comans, E.F.; Joshi, U.; Semenza, G.L.; Hoekstra, O.S.; Lammertsma, A.A.; et al. Biologic correlates of (18)fluorodeoxyglucose uptake in human breast cancer measured by positron emission tomography. J. Clin. Oncol. 2002, 20, 379–387. [Google Scholar] [CrossRef]
- Song, B.I.; Kim, H.W.; Won, K.S. Predictive Value of (18)F-FDG PET/CT for Axillary Lymph Node Metastasis in Invasive Ductal Breast Cancer. Ann. Surg. Oncol. 2017, 24, 2174–2181. [Google Scholar] [CrossRef]
- Kim, Y.I.; Kim, Y.J.; Paeng, J.C.; Cheon, G.J.; Lee, D.S.; Chung, J.K.; Kang, K.W. Prediction of breast cancer recurrence using lymph node metabolic and volumetric parameters from (18)F-FDG PET/CT in operable triple-negative breast cancer. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1787–1795. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Kim, S.H.; Park, H.S.; Kim, J.H.; Kim, D.; Cho, H.; Yun, M. The Prognostic Value of 18F-FDG Uptake in the Supraclavicular Lymph Node (N3c) on PET/CT in Patients with Locally Advanced Breast Cancer with Clinical N3c. Clin. Nucl. Med. 2019, 44, e6–e12. [Google Scholar] [CrossRef]
- Ulaner, G.A.; Eaton, A.; Morris, P.G.; Lilienstein, J.; Jhaveri, K.; Patil, S.; Fazio, M.; Larson, S.; Hudis, C.A.; Jochelson, M.S. Prognostic value of quantitative fluorodeoxyglucose measurements in newly diagnosed metastatic breast cancer. Cancer Med. 2013, 2, 725–733. [Google Scholar] [CrossRef] [PubMed]
- Satoh, Y.; Nambu, A.; Ichikawa, T.; Onishi, H. Whole-body total lesion glycolysis measured on fluorodeoxyglucose positron emission tomography/computed tomography as a prognostic variable in metastatic breast cancer. BMC Cancer 2014, 14, 525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marinelli, B.; Espinet-Col, C.; Ulaner, G.A.; McArthur, H.L.; Gonen, M.; Jochelson, M.; Weber, W.A. Prognostic value of FDG PET/CT-based metabolic tumor volumes in metastatic triple negative breast cancer patients. Am. J. Nucl. Med. Mol. Imaging 2016, 6, 120–127. [Google Scholar]
- Fisher, B.; Bauer, M.; Wickerham, D.L.; Redmond, C.K.; Fisher, E.R.; Cruz, A.B.; Foster, R.; Gardner, B.; Lerner, H.; Margolese, R.; et al. Relation of number of positive axillary nodes to the prognosis of patients with primary breast cancer. An NSABP update. Cancer 1983, 52, 1551–1557. [Google Scholar] [CrossRef]
- Carter, C.L.; Allen, C.; Henson, D.E. Relation of tumor size, lymph node status, and survival in 24,740 breast cancer cases. Cancer 1989, 63, 181–187. [Google Scholar] [CrossRef]
- Early Breast Cancer Trialists’ Collaborative Group. Tamoxifen for early breast cancer: An overview of the randomised trials. Lancet 1998, 351, 1451–1467. [Google Scholar] [CrossRef]
- Early Breast Cancer Trialists’ Collaborative Group. Polychemotherapy for early breast cancer: An overview of the randomised trials. Lancet 1998, 352, 930–942. [Google Scholar] [CrossRef]
- Yang, J.H.; Slack, N.H.; Nemoto, T. Effect of axillary nodal status on the long-term survival following mastectomy for breast carcinoma: Nodal metastases may not always suggest systemic disease. J. Surg. Oncol. 1987, 36, 243–248. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | All Patients (n = 32) |
|---|---|
| Age at diagnosis—years | |
| Median | 52.5 |
| Range | 34–75 |
| Menopausal status—no. (%) | |
| Premenopausal | 15 (46.9) |
| Postmenopausal | 17 (53.1) |
| ECOG performance status—no. (%) | |
| 0 | 16 (50.0) |
| 1 | 13 (40.6) |
| 2 | 3 (9.4) |
| Estrogen-receptor and progesterone-receptor status—no. (%) | |
| Positive for either | 23 (71.9) |
| Negative for both | 9 (28.1) |
| HER2 status—no. (%) | |
| Positive | 12 (37.5) |
| Negative | 20 (62.5) |
| Tumor stage—no. (%) | |
| T1 | 4 (12.5) |
| T2 | 15 (46.9) |
| T3 | 4 (12.5) |
| T4 | 9 (28.1) |
| Nodal stage—no. (%) | |
| N0 | 1 (3.1) |
| N1 | 15 (46.9) |
| N2 | 0 (0.0) |
| N3 | 16 (50.0) |
| Extent of disease—no. (%) | |
| <3 sites | 9 (28.1) |
| ≥3 sites | 23 (71.9) |
| Sites of metastasis—no. (%) | |
| Visceral | 21 (65.6) |
| Non-visceral only | 11 (34.4) |
| Type of therapy—no. (%) | |
| Hormone therapy, immunotherapy, or both | 3 (9.4) |
| Chemotherapy alone or combined with other therapy | 29 (90.6) |
| Variable | Progression-Free Survival | Overall Survival | ||
|---|---|---|---|---|
| Hazard Ratio (95% CI) | p Value | Hazard Ratio (95% CI) | p Value | |
| Age at diagnosis—years * | 1.02 (0.98–1.06) | 0.34 | 1.03 (0.96–1.09) | 0.45 |
| Menopausal status | ||||
| Premenopausal | 0.80 (0.36–1.77) | 0.58 | 0.78 (0.24–2.57) | 0.69 |
| Postmenopausal | 1.00 | 1.00 | ||
| ECOG performance status | ||||
| 0 | 1.00 | 1.00 | ||
| 1 | 1.89 (0.80–4.44) | 0.15 | 1.00 (0.27–3.73) | 1.00 |
| 2 | 3.41 (0.91–12.78) | 0.07 | 4.54 (0.85–24.16) | 0.08 |
| Estrogen-receptor and progesterone-receptor status | ||||
| Positive for either | 1.00 | 1.00 | ||
| Negative for both | 1.16 (0.48–2.78) | 0.74 | 2.81 (0.81–9.72) | 0.10 |
| HER2 status | ||||
| Positive | 1.00 | 1.00 | ||
| Negative | 0.97 (0.43–2.15) | 0.93 | 0.68 (0.20–2.36) | 0.55 |
| Tumor stage | ||||
| T1 | 1.00 | 1.00 | ||
| T2 | 0.99 (0.28–3.56) | 0.99 | 1.30 (0.15–11.22) | 0.81 |
| T3 | 1.44 (0.29–7.19) | 0.66 | 1.18 (0.07–18.96) | 0.91 |
| T4 | 2.32 (0.61–8.89) | 0.22 | 1.64 (0.18–14.97) | 0.66 |
| Nodal stage | ||||
| N0 or N1 | 1.00 | 1.00 | ||
| N2 or N3 | 2.64 (1.14–6.10) | 0.02 | 3.40 (0.90–12.89) | 0.07 |
| Extent of disease | ||||
| <3 sites | 1.00 | 1.00 | ||
| ≥3 sites | 1.32 (0.52–3.34) | 0.55 | 3.45 (0.44–27.24) | 0.24 |
| Sites of metastasis | ||||
| Visceral | 1.91 (0.79–4.61) | 0.15 | 5.56 (0.70–44.09) | 0.11 |
| Non-visceral only | 1.00 | 1.00 | ||
| Type of therapy | ||||
| Hormone therapy, immunotherapy, or both | 1.00 | 1.00 | ||
| Chemotherapy alone or combined with other therapy | 0.51 (0.15–1.77) | 0.29 | NE † | 0.56 |
| Maximum standardized uptake value | ||||
| Primary tumors | 1.08 (1.00–1.15) | 0.04 | 1.07 (0.98–1.17) | 0.14 |
| Regional lymph nodes | 1.10 (1.02–1.20) | 0.02 | 1.22 (1.07–1.40) | 0.004 |
| Total lesion glycolysis | ||||
| Primary tumors | 1.00 (1.00–1.00) | 0.57 | 1.00 (1.00–1.00) | 0.80 |
| Regional lymph nodes | 1.01 (1.00–1.02) | 0.04 | 1.02 (1.01–1.03) | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, H.; Cho, A.; Kang, W.J. Prognosis Associated with Glycolytic Activity in Regional Lymph Nodes of Patients with Previously Untreated Metastatic Breast Cancer: A Preliminary Study. Diagnostics 2022, 12, 1809. https://doi.org/10.3390/diagnostics12081809
Cho H, Cho A, Kang WJ. Prognosis Associated with Glycolytic Activity in Regional Lymph Nodes of Patients with Previously Untreated Metastatic Breast Cancer: A Preliminary Study. Diagnostics. 2022; 12(8):1809. https://doi.org/10.3390/diagnostics12081809
Chicago/Turabian StyleCho, Hojin, Arthur Cho, and Won Jun Kang. 2022. "Prognosis Associated with Glycolytic Activity in Regional Lymph Nodes of Patients with Previously Untreated Metastatic Breast Cancer: A Preliminary Study" Diagnostics 12, no. 8: 1809. https://doi.org/10.3390/diagnostics12081809
APA StyleCho, H., Cho, A., & Kang, W. J. (2022). Prognosis Associated with Glycolytic Activity in Regional Lymph Nodes of Patients with Previously Untreated Metastatic Breast Cancer: A Preliminary Study. Diagnostics, 12(8), 1809. https://doi.org/10.3390/diagnostics12081809