
Loading of the Spine in Low Back Pain Patients Does Not Induce MRI Changes in Modic Lesions: A Prospective Clinical Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. Magnetic Resonance Imaging
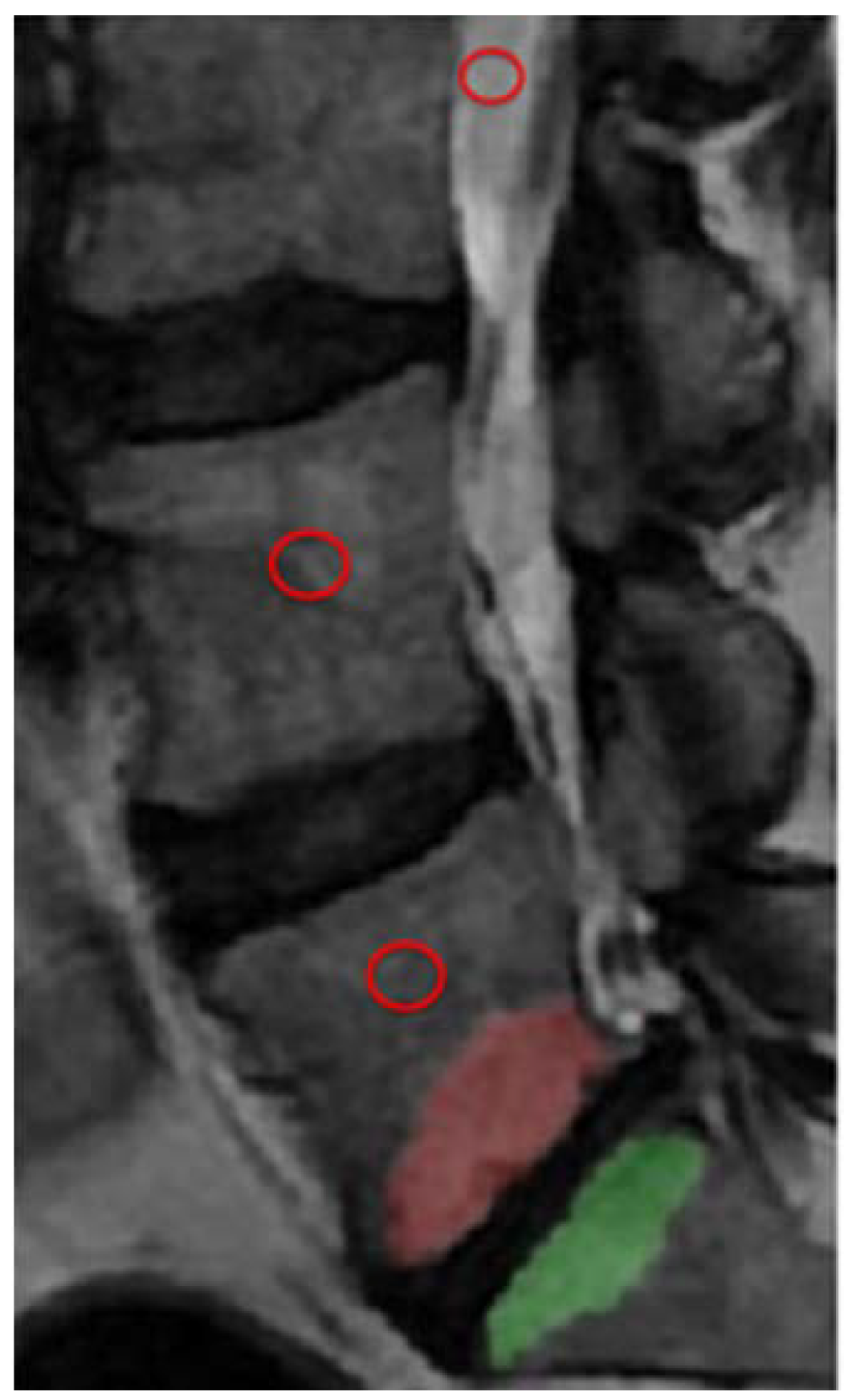
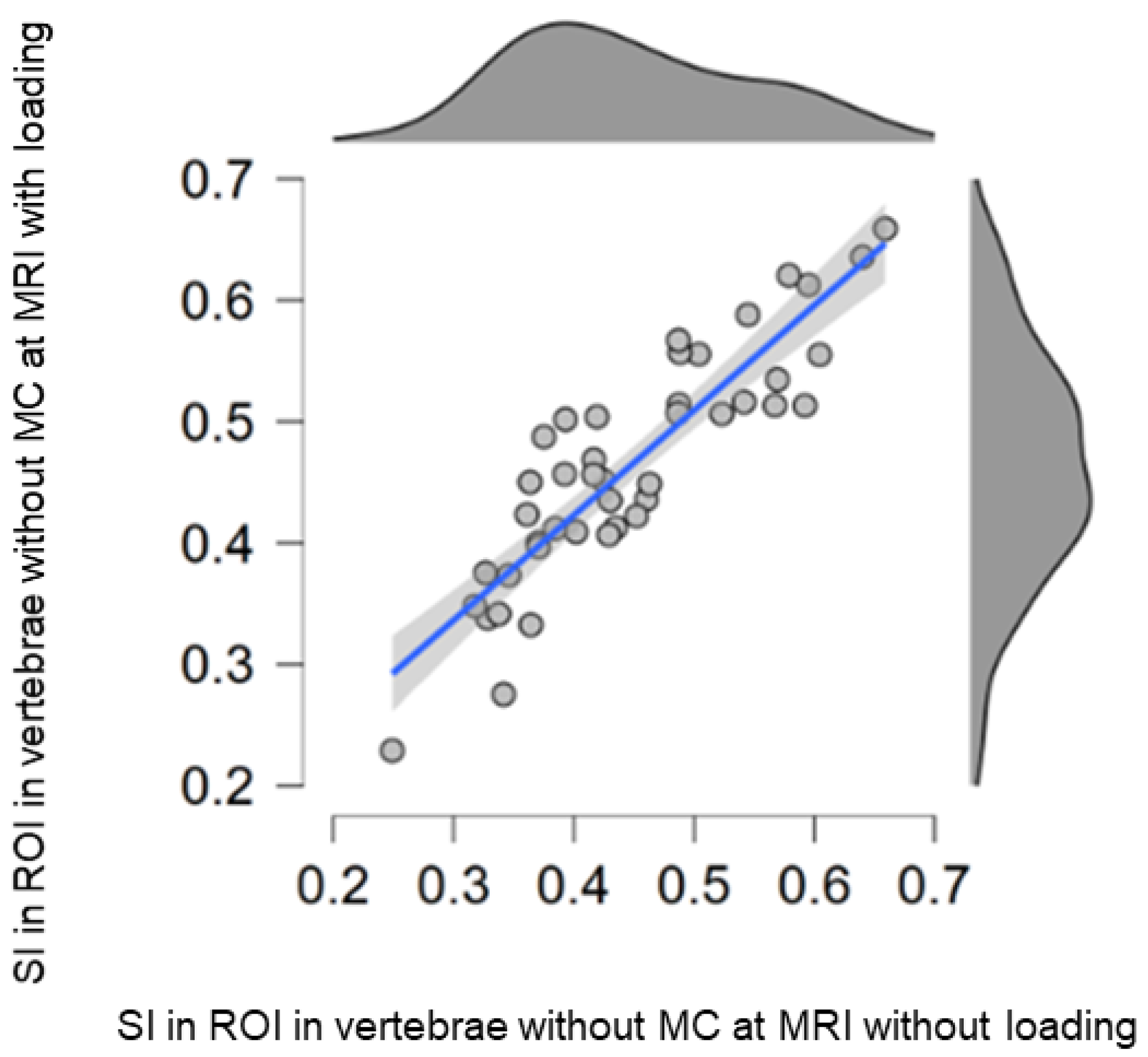
2.3. Measurements
2.4. Statistics
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dudli, S.; Fields, A.J.; Samartzis, D.; Karppinen, J.; Lotz, J.C. Pathobiology of Modic changes. Eur. Spine J. 2016, 25, 3723–3734. [Google Scholar] [CrossRef]
- Modic, M.T.; Masaryk, T.J.; Ross, J.; Carter, J.R. Imaging of degenerative disk disease. Radiology 1988, 168, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Modic, M.; Steinberg, P.; Ross, J.; Masaryk, T.; Carter, J. Degenerative disk disease: Assessment of changes in vertebral body marrow with MR imaging. Radiology 1988, 166, 193–199. [Google Scholar] [CrossRef]
- Mera, Y.; Teraguchi, M.; Hashizume, H.; Oka, H.; Muraki, S.; Akune, T.; Kawaguchi, H.; Nakamura, K.; Tamai, H.; Tanaka, S. Association between types of Modic changes in the lumbar region and low back pain in a large cohort: The Wakayama spine study. Eur. Spine J. 2020, 30, 1011–1017. [Google Scholar] [CrossRef]
- Karppinen, J.; Koivisto, K.; Ketola, J.; Haapea, M.; Paananen, M.; Herzig, K.-H.; Alini, M.; Lotz, J.; Dudli, S.; Samartzis, D. Serum biomarkers for Modic changes in patients with chronic low back pain. Eur. Spine J. 2021, 30, 1018–1027. [Google Scholar] [CrossRef]
- Dudli, S.; Liebenberg, E.; Magnitsky, S.; Miller, S.; Demir-Deviren, S.; Lotz, J.C. Propionibacterium acnes infected intervertebral discs cause vertebral bone marrow lesions consistent with Modic changes. J. Orthop. Res. 2016, 34, 1447–1455. [Google Scholar] [CrossRef] [Green Version]
- Jensen, T.; Karppinen, J.; Sorensen, J.; Niinimäki, J.; Leboeuf-Yde, C. Prevalence of vertebral endplate signal (Modic) changes and their association with non-specific low back pain—A systematic literature review. Eur. Spine J. 2008, 17, 1407–1422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crockett, M.T.; Kelly, B.S.; van Baarsel, S.; Kavanagh, E.C. Modic type 1 vertebral endplate changes: Injury, inflammation, or infection? Am. J. Roentgenol. 2017, 209, 167–170. [Google Scholar] [CrossRef] [PubMed]
- Rajasekaran, S.; Babu, J.N.; Arun, R.; Armstrong, B.R.W.; Shetty, A.P.; Murugan, S. ISSLS prize winner: A study of diffusion in human lumbar discs: A serial magnetic resonance imaging study documenting the influence of the endplate on diffusion in normal and degenerate discs. Spine 2004, 29, 2654–2667. [Google Scholar] [CrossRef] [PubMed]
- Muftuler, L.T.; Jarman, J.P.; Hon, J.Y.; Gardner, V.O.; Maiman, D.J.; Arpinar, V.E. Association between intervertebral disc degeneration and endplate perfusion studied by DCE-MRI. Eur. Spine J. 2015, 24, 679–685. [Google Scholar] [CrossRef] [PubMed]
- Roberts, S.; Urban, J.P.; Evans, H.; Eisenstein, S.M. Transport properties of the human cartilage endplate in relation to its composition and calcification. Spine 1996, 21, 415–420. [Google Scholar] [CrossRef]
- Yoganandan, N.; Larson, S.J.; Gallagher, M.; Pintar, F.A.; Reinartz, J.; Droese, K. Correlation of microtrauma in the lumbar spine with intraosseous pressures. Spine 1994, 19, 435–440. [Google Scholar] [CrossRef]
- Ferguson, S.J.; Ito, K.; Nolte, L.-P. Fluid flow and convective transport of solutes within the intervertebral disc. J. Biomech. 2004, 37, 213–221. [Google Scholar] [CrossRef]
- Lotz, J.C.; Ulrich, J.A. Innervation, inflammation, and hypermobility may characterize pathologic disc degeneration: Review of animal model data. JBJS 2006, 88, 76–82. [Google Scholar] [CrossRef]
- Splendiani, A.; Bruno, F.; Marsecano, C.; Arrigoni, F.; Di Cesare, E.; Barile, A.; Masciocchi, C. Modic I changes size increase from supine to standing MRI correlates with increase in pain intensity in standing position: Uncovering the “biomechanical stress” and “active discopathy” theories in low back pain. Eur. Spine J. 2019, 28, 983–992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Splendiani, A.; Perri, M.; Grattacaso, G.; Di Tunno, V.; Marsecano, C.; Panebianco, L.; Gennarelli, A.; Felli, V.; Varrassi, M.; Barile, A.; et al. Magnetic resonance imaging (MRI) of the lumbar spine with dedicated G-scan machine in the upright position: A retrospective study and our experience in 10 years with 4305 patients. Radiol. Med. 2016, 121, 38–44. [Google Scholar] [CrossRef]
- Lagerstrand, K.; Hebelka, H.; Brisby, H. Low back pain patients and controls display functional differences in endplates and vertebrae measured with T2-mapping. Eur. Spine J. 2019, 28, 234–240. [Google Scholar] [CrossRef] [Green Version]
- Hebelka, H.; Miron, A.; Kasperska, I.; Brisby, H.; Lagerstrand, K. Axial loading during MRI induces significant T2 value changes in vertebral endplates—A feasibility study on patients with low back pain. J. Orthop. Surg. Res. 2018, 13, 18. [Google Scholar] [CrossRef] [Green Version]
- Hebelka, H.; Torén, L.; Lagerstrand, K.; Brisby, H. Axial loading during MRI reveals deviant characteristics within posterior IVD regions between low back pain patients and controls. Eur. Spine J. 2018, 27, 2840–2846. [Google Scholar] [CrossRef] [PubMed]
- Lagerstrand, K.; Brisby, H.; Hebelka, H. Associations between high-intensity zones, endplate, and Modic changes and their effect on T2-mapping with and without spinal load. J. Orthop. Res.® 2021, 39, 2703–2710. [Google Scholar] [CrossRef]
- Willen, J.; Danielson, B. The diagnostic effect from axial loading of the lumbar spine during computed tomography and magnetic resonance imaging in patients with degenerative disorders. Spine 2001, 26, 2607–2614. [Google Scholar] [CrossRef]
- Charoensuk, J.; Laothamatas, J.; Sungkarat, W.; Worapruekjaru, L.; Hooncharoen, B.; Chousangsuntorn, K. Axial loading during supine MRI for improved assessment of lumbar spine: Comparison with standing MRI. Acta Radiol. 2021, 02841851211068148. [Google Scholar] [CrossRef]
- Yushkevich, P.A.; Piven, J.; Hazlett, H.C.; Smith, R.G.; Ho, S.; Gee, J.C.; Gerig, G. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. Neuroimage 2006, 31, 1116–1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420. [Google Scholar] [CrossRef]
- Perilli, E.; Parkinson, I.H.; Truong, L.-H.; Chong, K.C.; Fazzalari, N.L.; Osti, O.L. Modic (endplate) changes in the lumbar spine: Bone micro-architecture and remodelling. Eur. Spine J. 2015, 24, 1926–1934. [Google Scholar] [CrossRef] [Green Version]
- Järvinen, J.; Niinimäki, J.; Karppinen, J.; Takalo, R.; Haapea, M.; Tervonen, O. Does bone scintigraphy show Modic changes associated with increased bone turnover? Eur. J. Radiol. Open 2020, 7, 100222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, C.; Jousse, M.; Poiraudeau, S.; Feydy, A.; Rannou, F. Intervertebral disc and vertebral endplate subchondral changes associated with Modic 1 changes of the lumbar spine: A cross-sectional study. BMC Musculoskelet. Disord. 2017, 18, 1–7. [Google Scholar]
- Hebelka, H.; Brisby, H.; Hansson, T. Comparison between pain at discography and morphological disc changes at axial loaded MRI in patients with low back pain. Eur. Spine J. 2014, 23, 2075–2082. [Google Scholar] [CrossRef]
- Torén, L.; Lagerstrand, K.; Waldenberg, C.; Brisby, H.; Hebelka, H. MRI during Spinal Loading Reveals Intervertebral Disc Behavior Corresponding to Discogram Findings of Annular Fissures and Pain Provocation. Spine 2020, 45, E1500–E1506. [Google Scholar] [CrossRef]
- Waldenberg, C.; Hebelka, H.; Brisby, H.; Lagerstrand, K.M. Differences in IVD characteristics between low back pain patients and controls associated with HIZ as revealed with quantitative MRI. PLoS ONE 2019, 14, e0220952. [Google Scholar] [CrossRef] [Green Version]
- Berg, B.C.V.; Lecouvet, F.E.; Galant, C.; Simoni, P.; Malghem, J. Normal Variants of the Bone Marrow at MR Imaging of the Spine. In Seminars in Musculoskeletal Radiology; Thieme Medical Publishers: Leipzig, Germany, 2009; pp. 87–96. [Google Scholar]
- Karampinos, D.C.; Ruschke, S.; Dieckmeyer, M.; Diefenbach, M.; Franz, D.; Gersing, A.S.; Krug, R.; Baum, T. Quantitative MRI and spectroscopy of bone marrow. J. Magn. Reson. Imaging 2018, 47, 332–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krug, R.; Joseph, G.B.; Han, M.; Fields, A.; Cheung, J.; Mundada, M.; Bailey, J.; Rochette, A.; Ballatori, A.; McCulloch, C.E. Associations between vertebral body fat fraction and intervertebral disc biochemical composition as assessed by quantitative MRI. J. Magn. Reson. Imaging 2019, 50, 1219–1226. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Orientation/Sequence | TR (ms) | TE (ms) | FOV (mm) | Aqusition Matrix | Slice (mm) |
|---|---|---|---|---|---|
| sagittal T1 weighted | 573 | 7.7 | 280 × 280 | 352 × 260 | 3.5 |
| sagittal T2 weighted | 3680 | 108 | 280 × 280 | 352 × 288 | 3.5 |
| Load-Induced Change (MRI without Load-MRI with Load) | ||||
|---|---|---|---|---|
| MC Signal Intensity | MC Volume (cm3) | ROI Vertebra w MC Signal Intensity | ROI Vertebra w/o MC Signal Intensity | |
| N | 94 | 94 | 94 | 43 |
| Mean | 0.020 | 0.046 | (−)0.025 | (−)0.016 |
| SD | 0.187 | 0.387 | 0.07 | 0.09 |
| 95% CI lower | (−)0.019 | (−)0.033 | (−) 0.039 | (−)0.064 |
| 95% CI upper | 0.058 | 0.125 | (−) 0.007 | (−) 0.047 |
| Load-Induced Change (MRI without Load-MRI with Load) | |||||
|---|---|---|---|---|---|
| Modic Change Signal Intensity | Modic Change Volume (cm3) | ||||
| Modic Type | N | Mean | SD | Mean | SD |
| I | 34 | (−)0.004 | 0.176 | (−)0.026 | 0.316 |
| II | 55 | 0.039 | 0.198 | 0.099 | 0.433 |
| III | 5 | (−)0.033 | 0.121 | 0.205 | 0.416 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hebelka, H.; Brisby, H.; Erkmar, A.; Lagerstrand, K. Loading of the Spine in Low Back Pain Patients Does Not Induce MRI Changes in Modic Lesions: A Prospective Clinical Study. Diagnostics 2022, 12, 1815. https://doi.org/10.3390/diagnostics12081815
Hebelka H, Brisby H, Erkmar A, Lagerstrand K. Loading of the Spine in Low Back Pain Patients Does Not Induce MRI Changes in Modic Lesions: A Prospective Clinical Study. Diagnostics. 2022; 12(8):1815. https://doi.org/10.3390/diagnostics12081815
Chicago/Turabian StyleHebelka, Hanna, Helena Brisby, Alfred Erkmar, and Kerstin Lagerstrand. 2022. "Loading of the Spine in Low Back Pain Patients Does Not Induce MRI Changes in Modic Lesions: A Prospective Clinical Study" Diagnostics 12, no. 8: 1815. https://doi.org/10.3390/diagnostics12081815
APA StyleHebelka, H., Brisby, H., Erkmar, A., & Lagerstrand, K. (2022). Loading of the Spine in Low Back Pain Patients Does Not Induce MRI Changes in Modic Lesions: A Prospective Clinical Study. Diagnostics, 12(8), 1815. https://doi.org/10.3390/diagnostics12081815