
Network Analysis for Better Understanding the Complex Psycho-Biological Mechanisms behind Fibromyalgia Syndrome

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
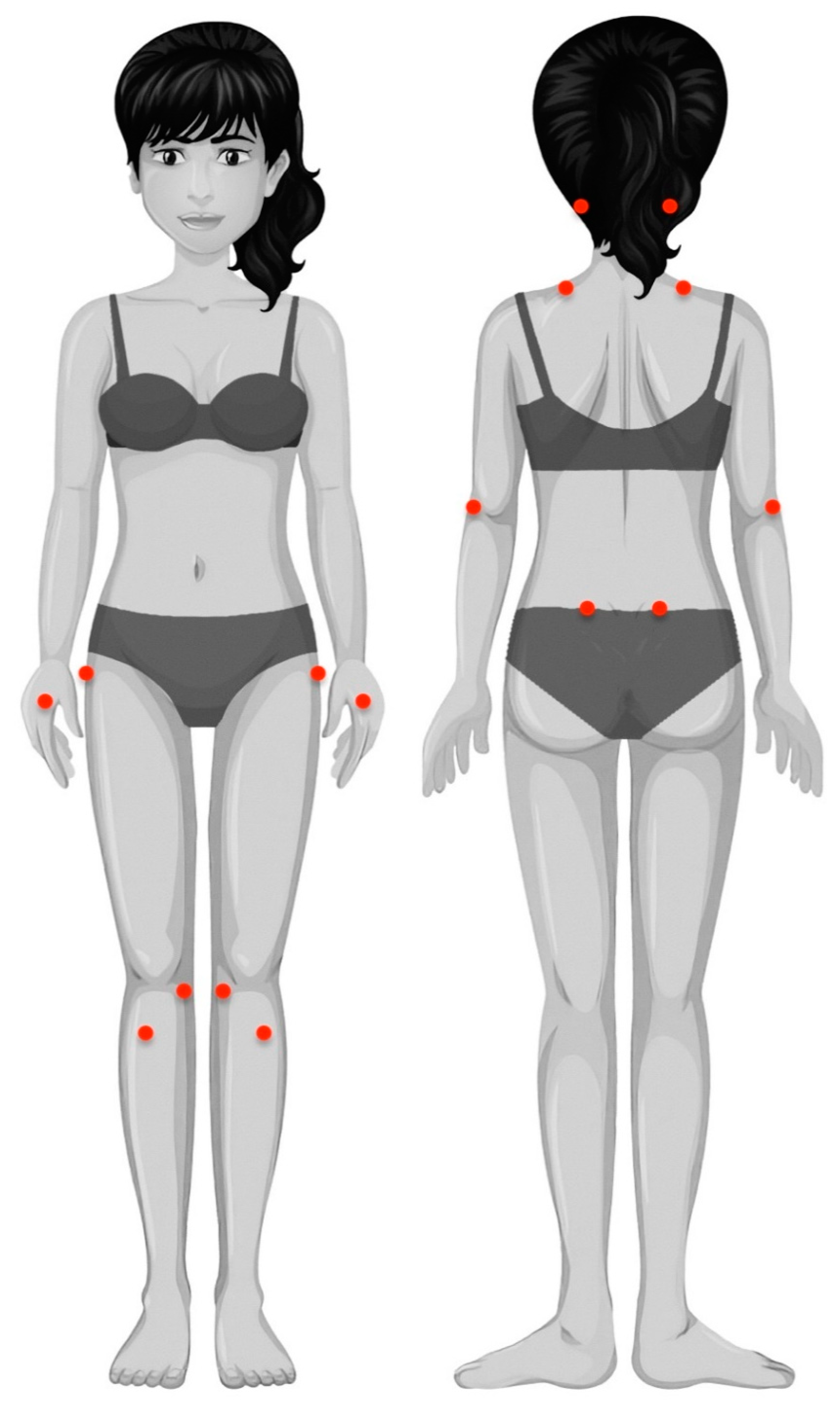
2.2. Clinical Variables
2.3. Psycho-Physical Variables
2.4. Psychological/Cognitive Variables
2.5. Health-Related Variables
2.6. Physical Variables
2.7. Approach to Network Analysis
2.7.1. Software and Packages
2.7.2. Missing Value Imputation
2.7.3. Network Estimation
2.7.4. Node Centrality
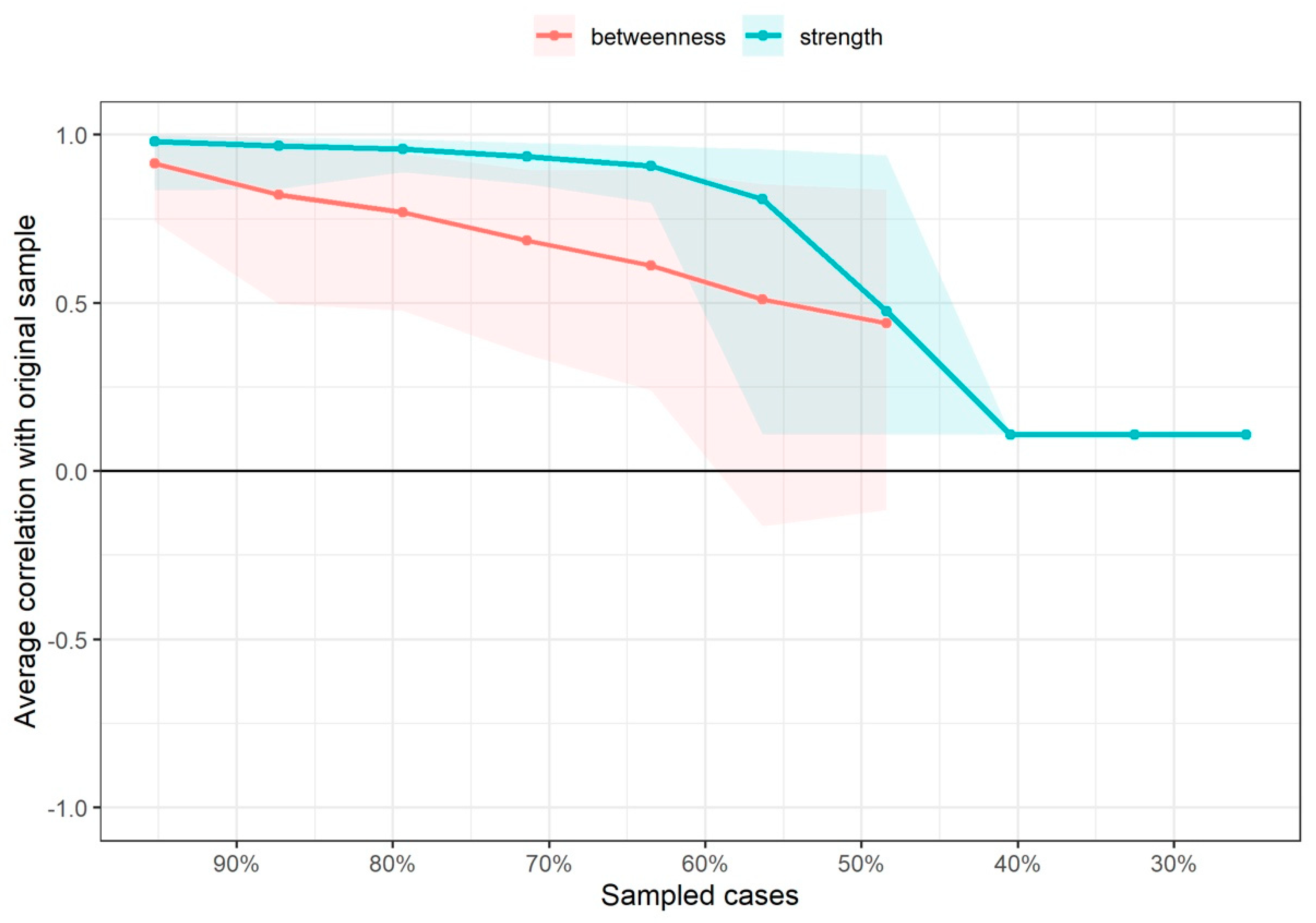
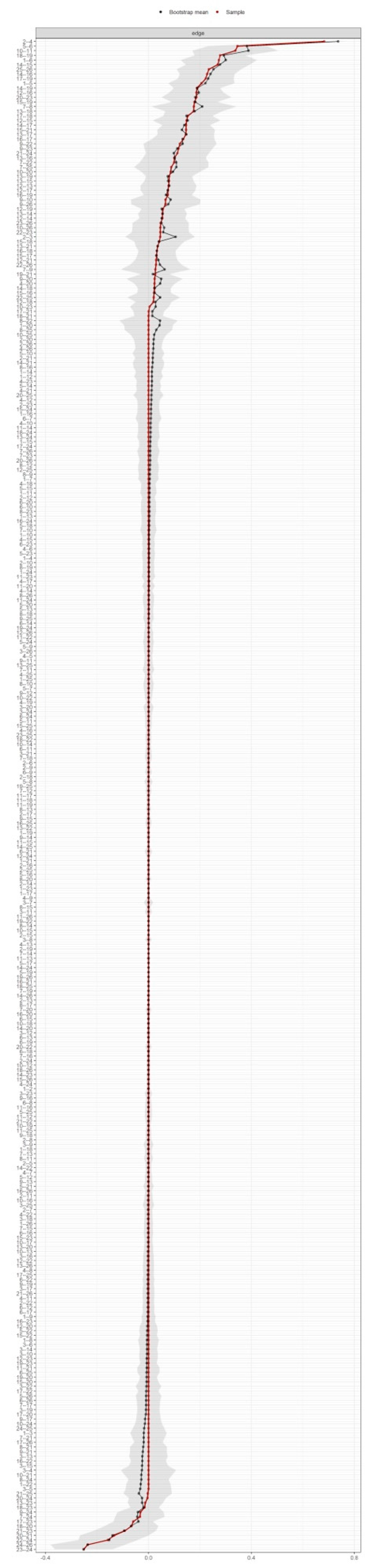
2.7.5. Network Edge and Node Centrality Variability
2.7.6. Community Detection
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cabo-Meseguer, A.; Cerdá-Olmedo, G.; Trillo-Mata, J.L. Fibromyalgia: Prevalence, epidemiologic profiles and economic costs. Fibromialgia: Prevalencia, perfiles epidemiológicos y costes económicos. Med. Clin. 2017, 149, 441–448. [Google Scholar] [CrossRef]
- Gostine, M.; Davis, F.; Roberts, B.A.; Risko, R.; Asmus, M.; Cappelleri, J.C.; Sadosky, A. Clinical Characteristics of fibromyalgia in a chronic pain population. Pain Pract. 2018, 18, 67–78. [Google Scholar] [CrossRef] [PubMed]
- Boomershine, C.S. Fibromyalgia: The prototypical central sensitivity syndrome. Curr. Rheumatol. Rev. 2015, 11, 131–145. [Google Scholar] [CrossRef]
- Kosek, E.; Clauw, D.; Nijs, J.; Baron, R.; Gilron, I.; Harris, R.E.; Mico, J.A.; Rice, A.; Sterling, M. Chronic nociplastic pain affecting the musculoskeletal system: Clinical criteria and grading system. Pain 2021, 162, 2629–2634. [Google Scholar] [CrossRef]
- Meeus, M.; Nijs, J. Central sensitization: A biopsychosocial explanation for chronic widespread pain in patients with fibromyalgia and chronic fatigue syndrome. Clin. Rheumatol. 2007, 26, 465–473. [Google Scholar] [CrossRef] [Green Version]
- Cagnie, B.; Coppieters, I.; Denecker, S.; Six, J.; Danneels, L.; Meeus, M. Central sensitization in fibromyalgia? A systematic review on structural and functional brain MRI. Semin. Arthritis Rheum. 2014, 44, 68–75. [Google Scholar] [CrossRef]
- Clauw, D.J. Fibromyalgia: A clinical review. JAMA 2014, 311, 1547–1555. [Google Scholar] [CrossRef]
- Estévez-López, F.; Álvarez-Gallardo, I.C.; Segura-Jiménez, V.; Soriano-Maldonado, A.; Borges-Cosic, M.; Pulido-Martos, M.; Aparicio, V.A.; Carbonell-Baeza, A.; Delgado-Fernández, M.; Geenen, R. The discordance between subjectively and objectively measured physical function in women with fibromyalgia: Association with catastrophizing and self-efficacy cognitions: The al-Ándalus project. Disabil. Rehabil. 2018, 40, 329–337. [Google Scholar] [CrossRef]
- Larsson, A.; Palstam, A.; Bjersing, J.; Löfgren, M.; Ernberg, M.; Kosek, E.; Gerdle, B.; Mannerkorpi, K. Controlled, cross-sectional, multi-center study of physical capacity and associated factors in women with fibromyalgia. BMC Musculoskelet. Disord. 2018, 19, 121. [Google Scholar] [CrossRef] [Green Version]
- Sempere-Rubio, N.; Aguilar-Rodríguez, M.; Inglés, M.; Izquierdo-Alventosa, R.; Serra-Añó, P. Physical condition factors that predict a better quality of life in women with fibromyalgia. Int. J. Environ. Res. Public Health 2019, 16, 3173. [Google Scholar] [CrossRef] [Green Version]
- Larsson, A.; Palstam, A.; Löfgren, M.; Ernberg, M.; Bjersing, J.; Bileviciute-Ljungar, I.; Gerdle, B.; Kosek, E.; Mannerkorpi, K. Pain and fear avoidance partially mediate change in muscle strength during resistance exercise in women with fibromyalgia. J. Rehabil. Med. 2017, 49, 744–750. [Google Scholar] [CrossRef] [Green Version]
- Umeda, M.; Corbin, L.W.; Maluf, K.S. Pain mediates the association between physical activity and the impact of fibromyalgia on daily function. Clin. Rheumatol. 2015, 34, 143–149. [Google Scholar] [CrossRef]
- Epskamp, S.; Fried, E.I. A tutorial on regularized partial correlation networks. Psychol. Methods 2018, 23, 617–634. [Google Scholar] [CrossRef] [Green Version]
- Schmittmann, V.D.; Cramer, A.O.J.; Waldorp, L.J.; Epskamp, S.; Kievit, R.A.; Borsboom, D. Deconstructing the construct: A network perspective on psychological phenomena. N. Ideas Psychol. 2013, 31, 43–53. [Google Scholar] [CrossRef]
- Valente, T.W. Network Interventions. Science 2012, 337, 49. [Google Scholar] [CrossRef]
- Gómez Penedo, J.M.; Rubel, J.A.; Blättler, L.; Schmidt, S.J.; Stewart, J.; Egloff, N.; Grosse Holtforth, M. The complex interplay of pain, depression, and anxiety symptoms in patients with chronic pain: A Network Approach. Clin. J. Pain 2020, 36, 249–259. [Google Scholar] [CrossRef]
- Åkerblom, S.; Cervin, M.; Perrin, S.; Rivano Fischer, M.; Gerdle, B.; McCracken, L.M. A network analysis of clinical variables in chronic pain: A Study from the Swedish Quality Registry for Pain Rehabilitation (SQRP). Pain Med. 2021, 22, 1591–1602. [Google Scholar] [CrossRef]
- Kumbhare, D.; Tesio, L. A theoretical framework to improve the construct for chronic pain disorders using fibromyalgia as an example. Ther. Adv. Musculoskelet. Dis. 2021, 13, 1759720X20966490. [Google Scholar] [CrossRef]
- Segura-Jiménez, V.; Aparicio, V.A.; Álvarez-Gallardo, I.C.; Soriano-Maldonado, A.; Estévez-López, F.; Delgado-Fernández, M.; Carbonell-Baeza, A. Validation of the modified 2010 American College of Rheumatology diagnostic criteria for fibromyalgia in a Spanish population. Rheumatology 2014, 53, 1803–1811. [Google Scholar] [CrossRef] [Green Version]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin. Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Cheatham, S.W.; Kolber, M.J.; Mokha, M.; Hanney, W.J. Concurrent validity of pain scales in individuals with myofascial pain and fibromyalgia. J. Bodyw. Mov. Ther. 2018, 22, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Barbero, M.; Moresi, F.; Leoni, D.; Gatti, R.; Egloff, M.; Falla, D. Test-retest reliability of pain extent and pain location using a novel method for pain drawing analysis. Eur. J. Pain 2015, 19, 1129–1138. [Google Scholar] [CrossRef] [PubMed]
- Úbeda-D’Ocasar, E.; Valera-Calero, J.A.; Hervás-Pérez, J.P.; Caballero-Corella, M.; Ojedo-Martín, C.; Gallego-Sendarrubias, G.M. Pain Intensity and Sensory Perception of Tender Points in Female Patients with Fibromyalgia: A Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 1461. [Google Scholar] [CrossRef]
- Cheatham, S.W.; Kolber, M.J.; Mokha, G.M.; Hanney, W.J. Concurrent validation of a pressure pain threshold scale for individuals with myofascial pain syndrome and fibromyalgia. J. Man. Manip. Ther. 2018, 26, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Pilar Martínez, M.; Miró, E.; Sánchez, A.I.; Lami, M.J.; Prados, G.; Ávila, D. Spanish version of the Pain Vigilance and Awareness Questionnaire: Psychometric properties in a sample of women with fibromyalgia. Span. J. Psychol. 2015, 17, E105. [Google Scholar] [CrossRef] [PubMed]
- García Campayo, J.; Rodero, B.; Alda, M.; Sobradiel, N.; Montero, J.; Moreno, S. Validation of the Spanish version of the Pain Catastrophizing Scale in fibromyalgia. Med. Clin. 2008, 131, 487–492. [Google Scholar] [CrossRef]
- Rivera, J.; González, T. The Fibromyalgia Impact Questionnaire: A validated Spanish version to assess the health status in women with fibromyalgia. Clin. Exp. Rheumatol. 2004, 22, 554–560. [Google Scholar]
- Wolfe, F.; Hawley, D.J.; Goldenberg, D.L.; Russell, I.J.; Buskila, D.; Neumann, L. The assessment of functional impairment in fibromyalgia (FM): Rasch analyses of 5 functional scales and the development of the FM Health Assessment Questionnaire. J. Rheumatol. 2000, 27, 1989–1999. [Google Scholar] [PubMed]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Van Hout, B.; Janssen, M.F.; Feng, Y.J.; Kohlmann, T.; Busschbach, J.; Golicki, D.; Lloyd, A.; Scalone, L.; Kind, P.; Pickard, A.S. Interim scoring for the EQ-5D-5L: Mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Health 2012, 15, 708–715. [Google Scholar] [CrossRef] [Green Version]
- Carbonell-Baeza, A.; Álvarez-Gallardo, I.C.; Segura-Jiménez, V.; Castro-Piñero, J.; Ruiz, J.R.; Delgado-Fernández, M.; Aparicio, V.A. Reliability and feasibility of physical fitness tests in female fibromyalgia patients. Int. J. Sports Med. 2015, 36, 157–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barry, E.; Galvin, R.; Keogh, C.; Horgan, F.; Fahey, T. Is the Timed Up and Go test a useful predictor of risk of falls in community dwelling older adults: A systematic review and meta-analysis. BMC Geriatr. 2014, 14, 14. [Google Scholar] [CrossRef]
- Collado-Mateo, D.; Domínguez-Muñoz, F.J.; Adsuar, J.C.; Merellano-Navarro, E.; Olivares, P.R.; Gusi, N. Reliability of the Timed Up and Go Test in Fibromyalgia. Rehabil. Nurs. 2018, 43, 35–39. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R. A Language and Environment for Statistical Computing. In R Foundation for Statistical Computing, R Core Team: Viena, Austria. 2020. Available online: http://wwwR-projectorg/ (accessed on 15 July 2022).
- Epskamp, S.; Cramer, A.O.J.; Waldorp, L.J.; Schmittmann, V.D.; Borsboom, D. qgraph: Network visualizations of relationships in psychometric data. J. Stat. Softw. 2012, 1, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Friedman, J.; Hastie, T.; Tibshirani, R. glasso: Graphical lasso estimation of Gaussian graphical models. R Package Version 2014, 1, 8. [Google Scholar]
- Ashtiani, M.; Mirzaie, M.; Jafari, M. CINNA: An R/CRAN package to decipher Central Informative Nodes in Network Analysis. Bioinformatics 2019, 35, 1436–1437. [Google Scholar] [CrossRef]
- Rahiminejad, S.; Maurya, M.R.; Subramaniam, S. Topological and functional comparison of community detection algorithms in biological networks. BMC Bioinform. 2019, 20, 212. [Google Scholar] [CrossRef]
- Liu, H.; Lafferty, J.; Wasserman, L. The nonparanormal: Semiparametric estimation of high dimensional undirected graphs. J. Mach. Learn. Res. 2009, 10, 2295–2328. [Google Scholar]
- Stekhoven, D.J.; Bühlmann, P. MissForest: Non-parametric missing value imputation for mixed-type data. Bioinformatics 2012, 28, 112–118. [Google Scholar] [CrossRef] [Green Version]
- Lauritzen, S.L.; Wermuth, N. Graphical models for associations between variables, some of which are qualitative and some quantitative. Ann. Stat. 1989, 17, 31–57. [Google Scholar] [CrossRef]
- Penone, C.; Davidson, A.D.; Shoemaker, K.T.; Di Marco, M.; Rondinini, C.; Brooks, T.M.; Young, B.E.; Graham, C.H.; Costa, G.C. Imputation of missing data in life-history trait datasets: Which approach performs the best? Methods Ecol. Evol. 2014, 5, 961–970. [Google Scholar] [CrossRef]
- Van Buuren, S.; Groothuis-Oudshoorn, K. Mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef] [Green Version]
- Hong, S.; Lynn, H.S. Accuracy of random-forest-based imputation of missing data in the presence of non-normality, non-linearity, and interaction. BMC Med. Res. Methodol. 2020, 20, 199. [Google Scholar] [CrossRef]
- Waljee, A.K.; Mukherjee, A.; Singal, A.G.; Zhang, Y.; Warren, J.; Balis, U.; Marrero, J.; Zhu, J.; Higgins, P.D. Comparison of imputation methods for missing laboratory data in medicine. BMJ Open 2013, 3, e002847. [Google Scholar] [CrossRef]
- Costantini, G.; Epskamp, S.; Borsboom, D.; Perugini, M.; Mõttus, R.; Waldorp, L.J.; Cramer, A.O.J. State of the aRt personality research: A tutorial on network analysis of personality data in R. J. Res. Pers. 2015, 54, 13–29. [Google Scholar] [CrossRef]
- Borgatti, S.P. Centrality and network flow. Soc. Netw. 2005, 27, 55–71. [Google Scholar] [CrossRef]
- Freeman, L.C. Centrality in social networks conceptual clarification. Soc. Netw. 1978, 1, 215–239. [Google Scholar] [CrossRef] [Green Version]
- Newman, M.E.J. Analysis of weighted networks. Phys. Rev. 2004, 70, 056131. [Google Scholar] [CrossRef] [Green Version]
- Opsahl, T.; Agneessens, F.; Skvoretz, J. Node centrality in weighted networks: Generalizing degree and shortest paths. Soc. Netw. 2010, 32, 245–251. [Google Scholar] [CrossRef]
- Rochat, Y. Closeness centrality extended to unconnected graphs: The harmonic centrality index. Inprocredings 2009, 10755931. Available online: https://infoscience.epfl.ch/record/200525 (accessed on 15 July 2022).
- Fernández-de-Las-Peñas, C.; Palacios-Ceña, M.; Valera-Calero, J.A.; Cuadrado, M.L.; Guerrero-Peral, A.; Pareja, J.A.; Arendt-Nielsen, L.; Varol, U. Understanding the interaction between clinical, emotional and psychophysical outcomes underlying tension-type headache: A network analysis approach. J. Neurol. 2022, 269, 4525–4534. [Google Scholar] [CrossRef]
- Epskamp, S.; Borsboom, D.; Fried, E.I. Estimating psychological networks and their accuracy: A tutorial paper. Behav. Res. Methods 2018, 50, 195–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacMahon, M.; Garlaschelli, D. Community detection for correlation matrices. Phys. Rev. 2015, 4, 021006. [Google Scholar] [CrossRef] [Green Version]
- Blondel, V.D.; Guillaume, J.L.; Lambiotte, R.; Lefebvre, E. Fast unfolding of communities in large networks. J. Stat. Mech. 2008, 10, P10008. [Google Scholar] [CrossRef] [Green Version]
- Hübscher, M.; Moloney, N.; Leaver, A.; Rebbeck, T.; McAuley, J.H.; Refshauge, K.M. Relationship between quantitative sensory testing and pain or disability in people with spinal pain-a systematic review and meta-analysis. Pain 2013, 154, 1497–1504. [Google Scholar] [CrossRef]
- Belavy, D.L.; Van Oosterwijck, J.; Clarkson, M.; Dhondt, E.; Mundell, N.L.; Miller, C.T.; Owen, P.J. Pain sensitivity is reduced by exercise training: Evidence from a systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2021, 120, 100–108. [Google Scholar] [CrossRef]
- Estévez-López, F.; Maestre-Cascales, C.; Russell, D.; Álvarez-Gallardo, I.C.; Rodriguez-Ayllon, M.; Hughes, C.M.; Davison, G.W.; Sañudo, B.; McVeigh, J.G. Effectiveness of exercise on fatigue and sleep quality in fibromyalgia: A systematic review and meta-analysis of randomized trials. Arch. Phys. Med. Rehabil. 2021, 102, 752–761. [Google Scholar] [CrossRef]
- Ferro Moura Franco, K.; Lenoir, D.; Dos Santos Franco, Y.R.; Jandre Reis, F.J.; Nunes Cabral, C.M.; Meeus, M. Prescription of exercises for the treatment of chronic pain along the continuum of nociplastic pain: A systematic review with meta-analysis. Eur. J. Pain 2021, 25, 51–70. [Google Scholar] [CrossRef]
- Othman, R.; Jayakaran, P.; Swain, N.; Dassanayake, S.; Tumilty, S.; Mani, R. Relationships between psychological, sleep, and physical activity measures and somatosensory function in people with peripheral joint pain: A systematic review and meta-analysis. Pain Pract. 2021, 21, 226–261. [Google Scholar] [CrossRef]
- Palstam, A.; Larsson, A.; Löfgren, M.; Ernberg, M.; Bjersing, J.; Bileviciute-Ljungar, I.; Gerdle, B.; Kosek, E.; Mannerkorpi, K. Decrease of fear avoidance beliefs following person-centered progressive resistance exercise contributes to reduced pain disability in women with fibromyalgia: Secondary exploratory analyses from a randomized controlled trial. Arthritis Res. Ther. 2016, 18, 116. [Google Scholar] [CrossRef] [Green Version]
- Macfarlane, G.J.; Kronisch, C.; Dean, L.E.; Atzeni, F.; Häuser, W.; Fluß, E.; Choy, E.; Kosek, E.; Amris, K.; Branco, J.; et al. EULAR revised recommendations for the management of fibromyalgia. Ann. Rheum. Dis. 2017, 76, 318–328. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Pre-Imputation Statistics | Missing Values (n; %) | Post-Imputation Statistics |
|---|---|---|---|
| Age (years) | 52.2 ± 10.7 | 1; 0.79 | 52.2 ± 10.7 |
| Weight (kg) | 71.4 ± 16.6 | 1; 0.79 | 71.4 ± 16.5 |
| Height (cm) | 1.6 ± 0.1 | 3; 2.38 | 1.6 ± 0.1 |
| BMI (kg/cm2) | 27.5 ± 6.2 | 3; 2.38 | 27.5 ± 6.1 |
| Years with pain | 20.1 ± 15.3 | 6; 4.76 | 20.4 ± 14.6 |
| Years with diagnosis | 10.2 ± 8.9 | 3; 2.38 | 10.1 ± 8.8 |
| Mean pain (NPRS, 0–10) | 6.4 ± 1.7 | 2; 1.58 | 6.4 ± 1.6 |
| Worst pain (NPRS, 0–10) | 7.3 ± 2.2 | 2; 1.58 | 7.3 ± 2.1 |
| Pain with activity (NPRS, 0–10) | 8.1 ± 1.9 | 3; 2.38 | 8.1 ± 1.8 |
| Pain extent dorsal (%) | 31.4 ± 26.3 | 0; 0 | 31.4 ± 26.3 |
| Pain extent ventral (%) | 26.6 ± 25.0 | 1; 0.79 | 26.8 ± 25.1 |
| PPT mastoid (kPa) | 151.2 ± 90.8 | 2; 1.59 | 150.8 ± 90.1 |
| PPT trapezius (kPa) | 125.6 ± 60.4 | 2; 1.59 | 126.1 ± 60.1 |
| PPT elbow (kPa) | 149.0 ± 87.1 | 2; 1.59 | 148.7 ± 86.5 |
| PPT hand (kPa) | 120.2 ± 59.1 | 1; 0.79 | 120.3 ± 58.9 |
| PPT posterior iliac crest (kPa) | 233.9 ± 130.7 | 1; 0.79 | 233.5 ± 130.3 |
| PPT greater trochanter (kPa) | 257.7 ± 123.9 | 1; 0.79 | 257.8 ± 123.4 |
| PPT knee (kPa) | 148.1 ± 107.1 | 2; 1.59 | 149.1 ± 106.8 |
| PPT tibialis anterior (kPa) | 187 ± 108.7 | 3; 2.38 | 187.9 ± 107.6 |
| Test Up and Go (TUG, s) | 12.4 ± 4.9 | 0; 0 | 12.4 ± 4.9 |
| Hand grip (kg) | 16.7 ± 6.2 | 9; 7.14 | 16.1 ± 5.7 |
| FIQ (0–100) | 64.8 ± 12.7 | 0; 0 | 64.8 ± 12.7 |
| FHAQ (0–3) | 1.3 ± 0.6 | 0; 0 | 1.3 ± 0.6 |
| EQ5DL (0–1) | 0.4 ± 0.3 | 0; 0 | 0.4 ± 0.3 |
| PVAQ (0–45) | 27 ± 8.2 | 0; 0 | 27 ± 8.2 |
| PCS (0–52) | 22.5 ± 12.3 | 0; 0 | 22.5 ± 12.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valera-Calero, J.A.; Arendt-Nielsen, L.; Cigarán-Méndez, M.; Fernández-de-las-Peñas, C.; Varol, U. Network Analysis for Better Understanding the Complex Psycho-Biological Mechanisms behind Fibromyalgia Syndrome. Diagnostics 2022, 12, 1845. https://doi.org/10.3390/diagnostics12081845
Valera-Calero JA, Arendt-Nielsen L, Cigarán-Méndez M, Fernández-de-las-Peñas C, Varol U. Network Analysis for Better Understanding the Complex Psycho-Biological Mechanisms behind Fibromyalgia Syndrome. Diagnostics. 2022; 12(8):1845. https://doi.org/10.3390/diagnostics12081845
Chicago/Turabian StyleValera-Calero, Juan Antonio, Lars Arendt-Nielsen, Margarita Cigarán-Méndez, César Fernández-de-las-Peñas, and Umut Varol. 2022. "Network Analysis for Better Understanding the Complex Psycho-Biological Mechanisms behind Fibromyalgia Syndrome" Diagnostics 12, no. 8: 1845. https://doi.org/10.3390/diagnostics12081845
APA StyleValera-Calero, J. A., Arendt-Nielsen, L., Cigarán-Méndez, M., Fernández-de-las-Peñas, C., & Varol, U. (2022). Network Analysis for Better Understanding the Complex Psycho-Biological Mechanisms behind Fibromyalgia Syndrome. Diagnostics, 12(8), 1845. https://doi.org/10.3390/diagnostics12081845