
Diagnosis of Pulmonary Embolism during Pregnancy


Abstract
:1. Introduction
Epidemiological Data
2. Diagnostic Management of Pregnant Women with Suspected Pulmonary Embolism
2.1. Assessing the Pre-Test Clinical Probability of PE in Pregnant Women
2.2. Safety and Usefulness of D-Dimer to Exclude PE during Pregnancy
2.3. The Diagnostic Yield of Lower Limb Compression Ultrasound in Pregnant Women with Suspected PE
2.4. Thoracic Imaging in Pregnant Women with Suspected PE
2.5. Scientific Societies’ Recommendations for PE Diagnosis during Pregnancy
- -
- formal diagnostic assessment with validated methods (Class I, level B)
- -
- D-dimer measurement and clinical prediction rules to rule out PE (Class IIa, level B)
- -
- venous CUS to avoid unnecessary irradiation (Class IIa, level B)
- -
- and in terms of imaging test: perfusion scintigraphy or CTPA (with a low-radiation dose protocol); CTPA as the first-line option if chest X-ray is abnormal (Class IIa, level C) recommendation.
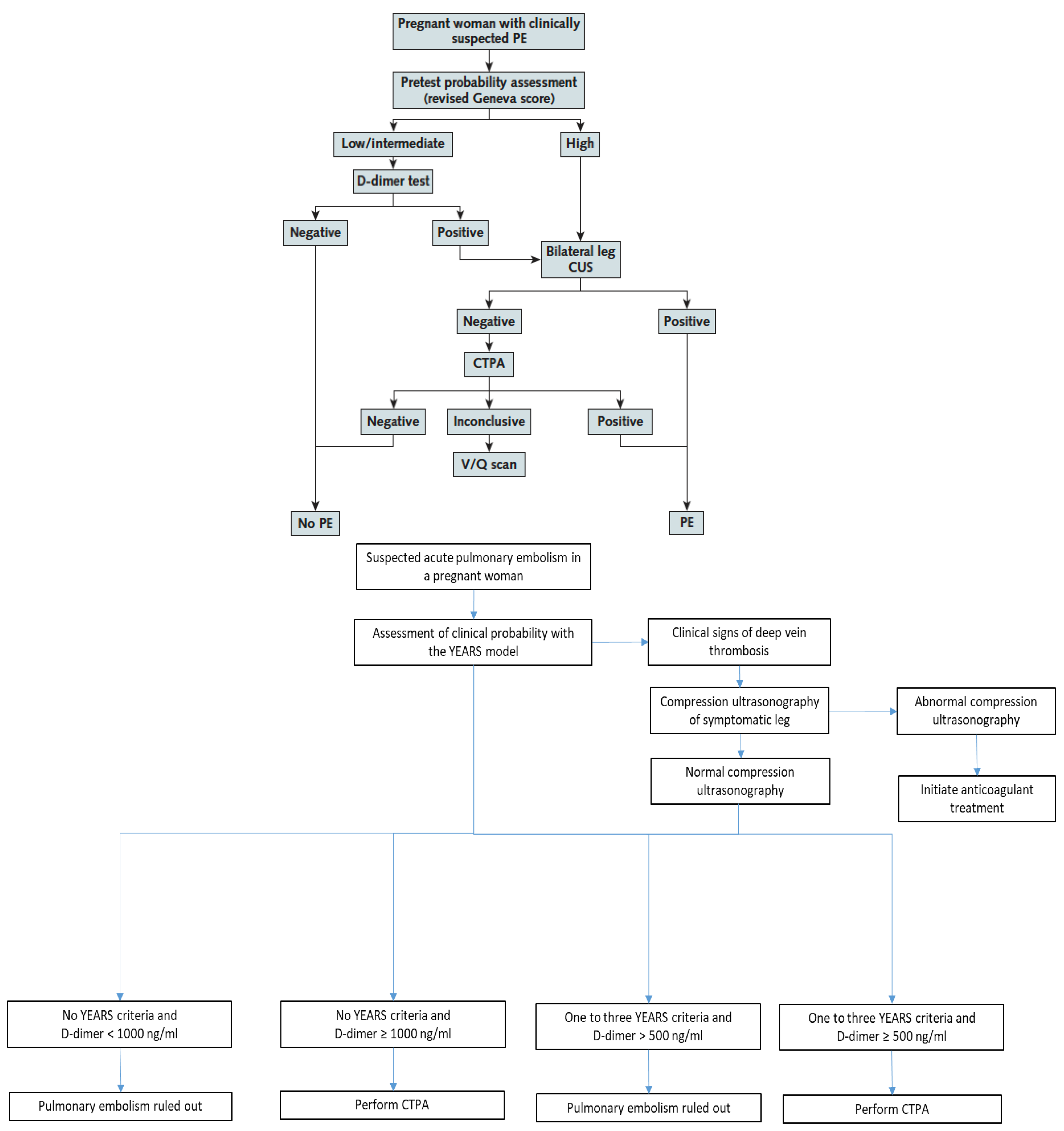
3. Recently Validated Diagnostic Algorithms in Pregnant Women with Suspected PE
3.1. The CT-PE Pregnancy Study
3.2. The ARTEMIS Study
4. Remaining Controversies and Future Perspectives
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cantwell, R.; Clutton-Brock, T.; Cooper, G.; Dawson, A.; Drife, J.; Garrod, D.; Harper, A.; Hulbert, D.; Lucas, S.; McClure, J.; et al. Saving Mothers’ Lives: Reviewing maternal deaths to make motherhood safer: 2006–2008. The Eighth Report of the Confidential Enquiries into Maternal Deaths in the United Kingdom. BJOG 2011, 118 (Suppl. 1), 1–203. [Google Scholar]
- Heit, J.A.; Kobbervig, C.E.; James, A.H.; Petterson, T.M.; Bailey, K.R.; Melton, L.J., 3rd. Trends in the incidence of venous thromboembolism during pregnancy or postpartum: A 30-year population-based study. Ann. Intern. Med. 2005, 143, 697–706. [Google Scholar] [CrossRef]
- Kamel, H.; Navi, B.B.; Sriram, N.; Hovsepian, D.A.; Devereux, R.B.; Elkind, M.S. Risk of a thrombotic event after the 6-week postpartum period. N. Engl. J. Med. 2014, 370, 1307–1315. [Google Scholar] [CrossRef] [Green Version]
- Chan, W.S.; Ray, J.G.; Murray, S.; Coady, G.E.; Coates, G.; Ginsberg, J.S. Suspected pulmonary embolism in pregnancy: Clinical presentation, results of lung scanning, and subsequent maternal and pediatric outcomes. Arch. Intern. Med. 2002, 162, 1170–1175. [Google Scholar] [CrossRef]
- Chan, W.S.; Lee, A.; Spencer, F.A.; Crowther, M.; Rodger, M.; Ramsay, T.; Ginsberg, J.S. Predicting deep venous thrombosis in pregnancy: Out in “LEFt” field? Ann. Intern. Med. 2009, 151, 85–92. [Google Scholar] [CrossRef]
- Gibson, P.S.; Powrie, R.; Peipert, J. Prevalence of syncope and recurrent presyncope during pregnancy. Obstet. Gynecol. 2001, 97, S41–S42. [Google Scholar]
- Bourjeily, G.; Paidas, M.; Khalil, H.; Rosene-Montella, K.; Rodger, M. Pulmonary embolism in pregnancy. Lancet 2010, 375, 500–512. [Google Scholar] [CrossRef] [Green Version]
- Righini, M.; Robert-Ebadi, H.; Elias, A.; Sanchez, O.; Le Moigne, E.; Schmidt, J.; Le Gall, C.; Cornuz, J.; Aujesky, D.; Roy, P.-M.; et al. Diagnosis of Pulmonary Embolism during Pregnancy: A Multicenter Prospective Management Outcome Study. Ann. Intern. Med. 2018, 169, 766–773. [Google Scholar] [CrossRef]
- van der Pol, L.M.; Tromeur, C.; Bistervels, I.M.; Ni Ainle, F.; van Bemmel, T.; Bertoletti, L.; Couturaud, F.; van Dooren, Y.P.; Elias, A.; Faber, L.M.; et al. Pregnancy-Adapted YEARS Algorithm for Diagnosis of Suspected Pulmonary Embolism. N. Engl. J. Med. 2019, 380, 1139–1149. [Google Scholar] [CrossRef]
- Righini, M.; Van Es, J.; Den Exter, P.L.; Roy, P.M.; Verschuren, F.; Ghuysen, A.; Rutschmann, O.T.; Sanchez, O.; Jaffrelot, M.; Trinh-Duc, A.; et al. Age-adjusted D-dimer cutoff levels to rule out pulmonary embolism: The ADJUST-PE study. JAMA 2014, 311, 1117–1124. [Google Scholar] [CrossRef] [PubMed]
- van der Hulle, T.; Cheung, W.Y.; Kooij, S.; Beenen, L.F.M.; van Bemmel, T.; van Es, J.; Faber, L.M.; Hazelaar, G.M.; Heringhaus, C.; Hofstee, H.; et al. Simplified diagnostic management of suspected pulmonary embolism (the YEARS study): A prospective, multicentre, cohort study. Lancet 2017, 390, 289–297. [Google Scholar] [CrossRef]
- Le Gal, G.; Kercret, G.; Ben Yahmed, K.; Bressollette, L.; Robert-Ebadi, H.; Riberdy, L.; Louis, P.; Delluc, A.; Labalette, M.; Baba-Ahmed, M.; et al. Diagnostic value of single complete compression ultrasonography in pregnant and postpartum women with suspected deep vein thrombosis: Prospective study. BMJ 2012, 344, e2635. [Google Scholar] [CrossRef] [Green Version]
- Dronkers, C.E.A.; van der Hulle, T.; Le Gal, G.; Kyrle, P.A.; Huisman, M.V.; Cannegieter, S.C.; Klok, F.A.; Disease, T.S. Towards a tailored diagnostic standard for future diagnostic studies in pulmonary embolism: Communication from the SSC of the ISTH. J. Thromb. Haemost. 2017, 15, 1040–1043. [Google Scholar] [CrossRef]
- Leung, A.N.; Bull, T.M.; Jaeschke, R.; Lockwood, C.J.; Boiselle, P.M.; Hurwitz, L.M.; James, A.H.; McCullough, L.B.; Menda, Y.; Paidas, M.J.; et al. An official American Thoracic Society/Society of Thoracic Radiology clinical practice guideline: Evaluation of suspected pulmonary embolism in pregnancy. Am. J. Respir. Crit. Care Med. 2011, 184, 1200–1208. [Google Scholar] [CrossRef]
- Investigators, P. Value of the ventilation/perfusion scan in acute pulmonary embolism. Results of the prospective investigation of pulmonary embolism diagnosis (PIOPED). JAMA 1990, 263, 2753–2759. [Google Scholar]
- Roy, P.-M.; Meyer, G.; Carpentier, F.; Leveau, P.; The EMDEPU Study Group; Vielle, B.; Le Gall, C.; Verschuren, F.; Furber, A. Appropriateness of diagnostic management and outcomes of suspected pulmonary embolism. Ann. Intern. Med. 2006, 144, 157–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.J.; Harjola, V.-P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jiménez, D.; et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur. Heart, J. 2020, 41, 543–603. [Google Scholar] [CrossRef] [Green Version]
- Lim, W.; Le Gal, G.; Bates, S.M.; Righini, M.; Haramati, L.B.; Lang, E.; Kline, J.A.; Chasteen, S.; Snyder, M.; Patel, P.; et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: Diagnosis of venous thromboembolism. Blood Adv. 2018, 2, 3226–3256. [Google Scholar] [CrossRef] [PubMed]
- Chan, W.S. Can pregnancy-adapted algorithms avoid diagnostic imaging for pulmonary embolism? Hematol. Am. Soc. Hematol. Educ. Program 2020, 2020, 184–189. [Google Scholar] [CrossRef]
- Langlois, E.; Cusson-Dufour, C.; Moumneh, T.; Elias, A.; Meyer, G.; Lacut, K.; Schmidt, J.; Le Gall, C.; Chauleur, C.; Glauser, F.; et al. Could the YEARS algorithm be used to exclude pulmonary embolism during pregnancy? Data from the CT-PE-pregnancy study. J. Thromb. Haemost. 2019, 17, 1329–1334. [Google Scholar] [CrossRef] [PubMed]
- Robert-Ebadi, H.; Elias, A.; Sanchez, O.; Le Moigne, E.; Schmidt, J.; Le Gall, C.; Aujesky, D.; Roy, P.; Moumneh, T.; Chauleur, C.; et al. Assessing the clinical probability of pulmonary embolism during pregnancy: The Pregnancy-Adapted Geneva (PAG) score. J. Thromb. Haemost. 2021, 19, 3044–3050. [Google Scholar] [CrossRef]
- Goodacre, S.; Horspool, K.; Nelson-Piercy, C.; Knight, M.; Shephard, N.; Lecky, F.; Thomas, S.; Hunt, B.J.; Fuller, G.W. The DiPEP study: An observational study of the diagnostic accuracy of clinical assessment, D-dimer and chest x-ray for suspected pulmonary embolism in pregnancy and postpartum. BJOG 2019, 126, 383–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robert-Ebadi, H.; Robin, P.; Hugli, O.; Verschuren, F.; Trinh-Duc, A.; Roy, P.M.; Schmidt, J.; Fumeaux, T.; Meyer, G.; Hayoz, D.; et al. Impact of the Age-Adjusted D-Dimer Cutoff to Exclude Pulmonary Embolism: A Multinational Prospective Real-Life Study (the RELAX-PE Study). Circulation 2021, 143, 1828–1830. [Google Scholar] [CrossRef]
- Carrier, M.; Righini, M.; Djurabi, R.K.; Huisman, M.V.; Perrier, A.; Wells, P.S.; Rodger, M.; Wuillemin, M.A.; Le Gal, G. VIDAS D-dimer in combination with clinical pre-test probability to rule out pulmonary embolism. A systematic review of management outcome studies. Thromb. Haemost. 2009, 101, 886–892. [Google Scholar] [CrossRef] [PubMed]
- Bellesini, M.; Robert-Ebadi, H.; Combescure, C.; Dedionigi, C.; Le Gal, G.; Righini, M. D-dimer to rule out venous thromboembolism during pregnancy: A systematic review and meta-analysis. J. Thromb. Haemost. 2021, 19, 2454–2467. [Google Scholar] [CrossRef] [PubMed]
- Chabloz, P.; Reber, G.; Boehlen, F.; Hohlfeld, P.; de Moerloose, P. TAFI antigen and D-dimer levels during normal pregnancy and at delivery. Br. J. Haematol. 2001, 115, 150–152. [Google Scholar] [CrossRef]
- Murphy, N.; Broadhurst, D.I.; Khashan, A.S.; Gilligan, O.; Kenny, L.C.; O’Donoghue, K. Gestation-specific D-dimer reference ranges: A cross-sectional study. BJOG 2015, 122, 395–400. [Google Scholar] [CrossRef]
- Wan, T.; Skeith, L.; Karovitch, A.; Rodger, M.; Le Gal, G. Guidance for the diagnosis of pulmonary embolism during pregnancy: Consensus and controversies. Thromb. Res. 2017, 157, 23–28. [Google Scholar] [CrossRef]
- Robert-Ebadi, H.; Le Gal, G.; Righini, M. Evolving imaging techniques in diagnostic strategies of pulmonary embolism. Expert Rev. Cardiovasc. Ther. 2016, 14, 495–503. [Google Scholar] [CrossRef] [PubMed]
- Tromeur, C.; van der Pol, L.M.; Le Roux, P.-Y.; Ende-Verhaar, Y.; Salaun, P.-Y.; Leroyer, C.; Couturaud, F.; Kroft, L.J.; Huisman, M.V.; Klok, F.A. Computed tomography pulmonary angiography versus ventilation-perfusion lung scanning for diagnosing pulmonary embolism during pregnancy: A systematic review and meta-analysis. Haematologica 2019, 104, 176–188. [Google Scholar] [CrossRef] [Green Version]
- McLintock, C.; Brighton, T.; Chunilal, S.; Dekker, G.; McDonnell, N.; McRae, S.; Muller, P.; Tran, H.; Walters, B.N.; Young, L. Recommendations for the diagnosis and treatment of deep venous thrombosis and pulmonary embolism in pregnancy and the postpartum period. Aust. N. Z. J. Obstet. Gynaecol. 2012, 52, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Ridge, C.A.; Mhuircheartaigh, J.N.; Dodd, J.D.; Skehan, S.J. Pulmonary CT angiography protocol adapted to the hemodynamic effects of pregnancy. AJR Am. J. Roentgenol. 2011, 197, 1058–1063. [Google Scholar] [CrossRef] [PubMed]
- Hunt, B.J.; Parmar, K.; Horspool, K.; Shephard, N.; Nelson-Piercy, C.; Goodacre, S.; The DiPEP Research Group. The DiPEP (Diagnosis of PE in Pregnancy) biomarker study: An observational cohort study augmented with additional cases to determine the diagnostic utility of biomarkers for suspected venous thromboembolism during pregnancy and puerperium. Br. J. Haematol. 2018, 180, 694–704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burton, K.R.; Park, A.L.; Fralick, M.; Ray, J.G. Risk of early-onset breast cancer among women exposed to thoracic computed tomography in pregnancy or early postpartum. J. Thromb. Haemost. 2018, 16, 876–885. [Google Scholar] [CrossRef] [Green Version]
- Gillespie, C.; Foley, S.; Rowan, M.; Ewins, K.; NiAinle, F.; MacMahon, P. The OPTICA study (Optimised Computed Tomography Pulmonary Angiography in Pregnancy Quality and Safety study): Rationale and design of a prospective trial assessing the quality and safety of an optimised CTPA protocol in pregnancy. Thromb. Res. 2019, 177, 172–179. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| The Pregnancy-Adapted Geneva Score | |||
|---|---|---|---|
| ITEM | POINTS | ||
| Age 40 years and older | +1 | ||
| Surgery (under GA) or lower limb fracture in past month | +2 | ||
| Previous DVT or PE | +3 | ||
| Unilateral lower limb pain | +3 | ||
| Hemoptysis | +2 | ||
| Pain on lower limb palpation and unilateral oedema | +4 | ||
| Heart rate > 110 bpm | +5 | ||
| Maximal point number | 20 | ||
| Points | PTP Category | PE Prevalence in Development Cohort | 95% CI |
| 0–1 | Low | 2.3% | 1.0–4.9% |
| 2–6 | Intermediate | 11.6% | 6.9–18.9% |
| ≥7 | High | 61.5% | 35.5–82.2% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Robert-Ebadi, H.; Moumneh, T.; Le Gal, G.; Righini, M. Diagnosis of Pulmonary Embolism during Pregnancy. Diagnostics 2022, 12, 1875. https://doi.org/10.3390/diagnostics12081875
Robert-Ebadi H, Moumneh T, Le Gal G, Righini M. Diagnosis of Pulmonary Embolism during Pregnancy. Diagnostics. 2022; 12(8):1875. https://doi.org/10.3390/diagnostics12081875
Chicago/Turabian StyleRobert-Ebadi, Helia, Thomas Moumneh, Grégoire Le Gal, and Marc Righini. 2022. "Diagnosis of Pulmonary Embolism during Pregnancy" Diagnostics 12, no. 8: 1875. https://doi.org/10.3390/diagnostics12081875