
Developing a Simple Score for Diagnosis of Acute Cholecystitis at the Emergency Department
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Selection of Participants
2.2. Data Collection
2.3. Confirmation of Cases
2.4. Statistical Analysis and Sample Size Estimation
2.5. Model Development and Internal Validation
2.6. Score Derivation and Validation
3. Results
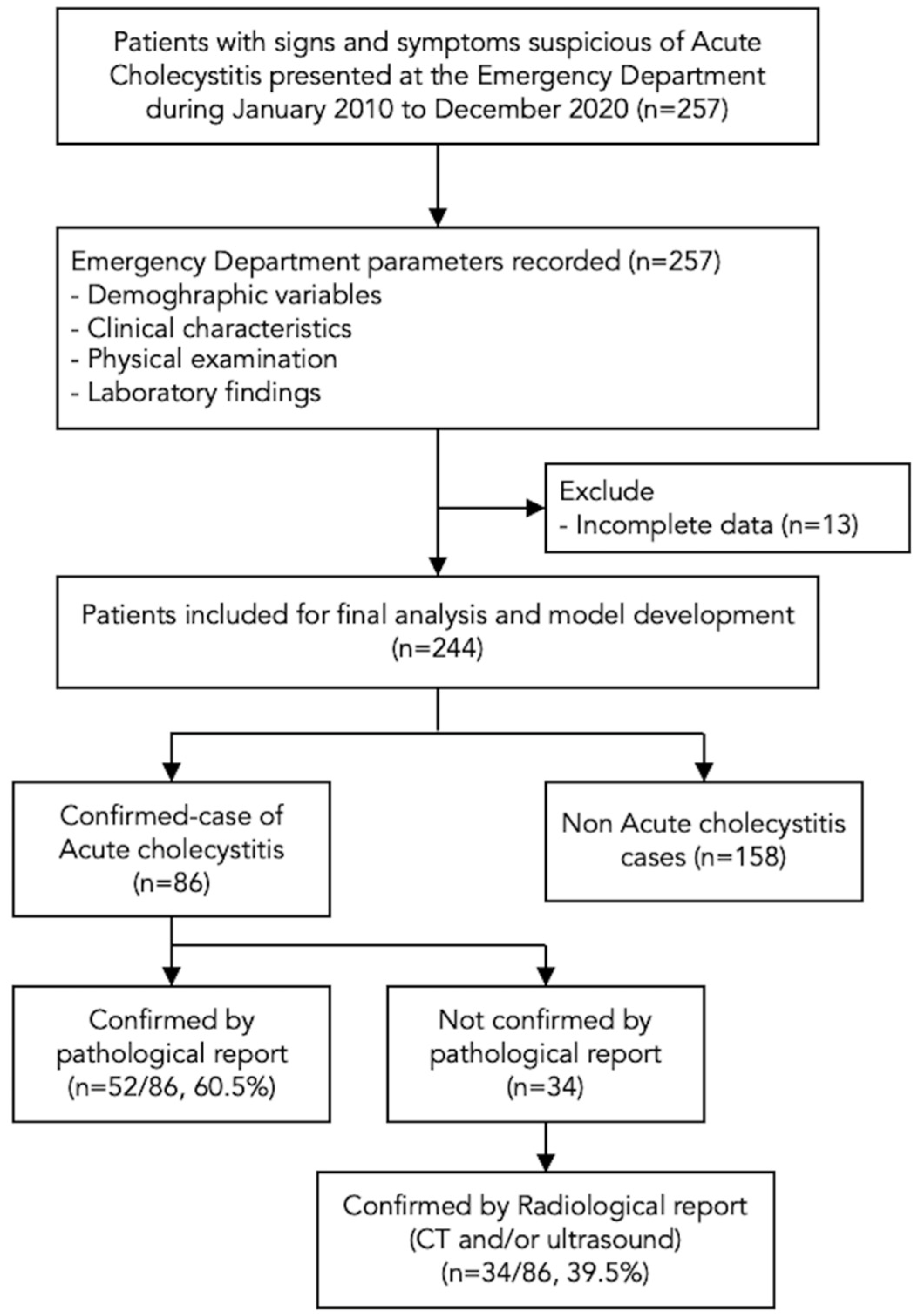
3.1. Participants
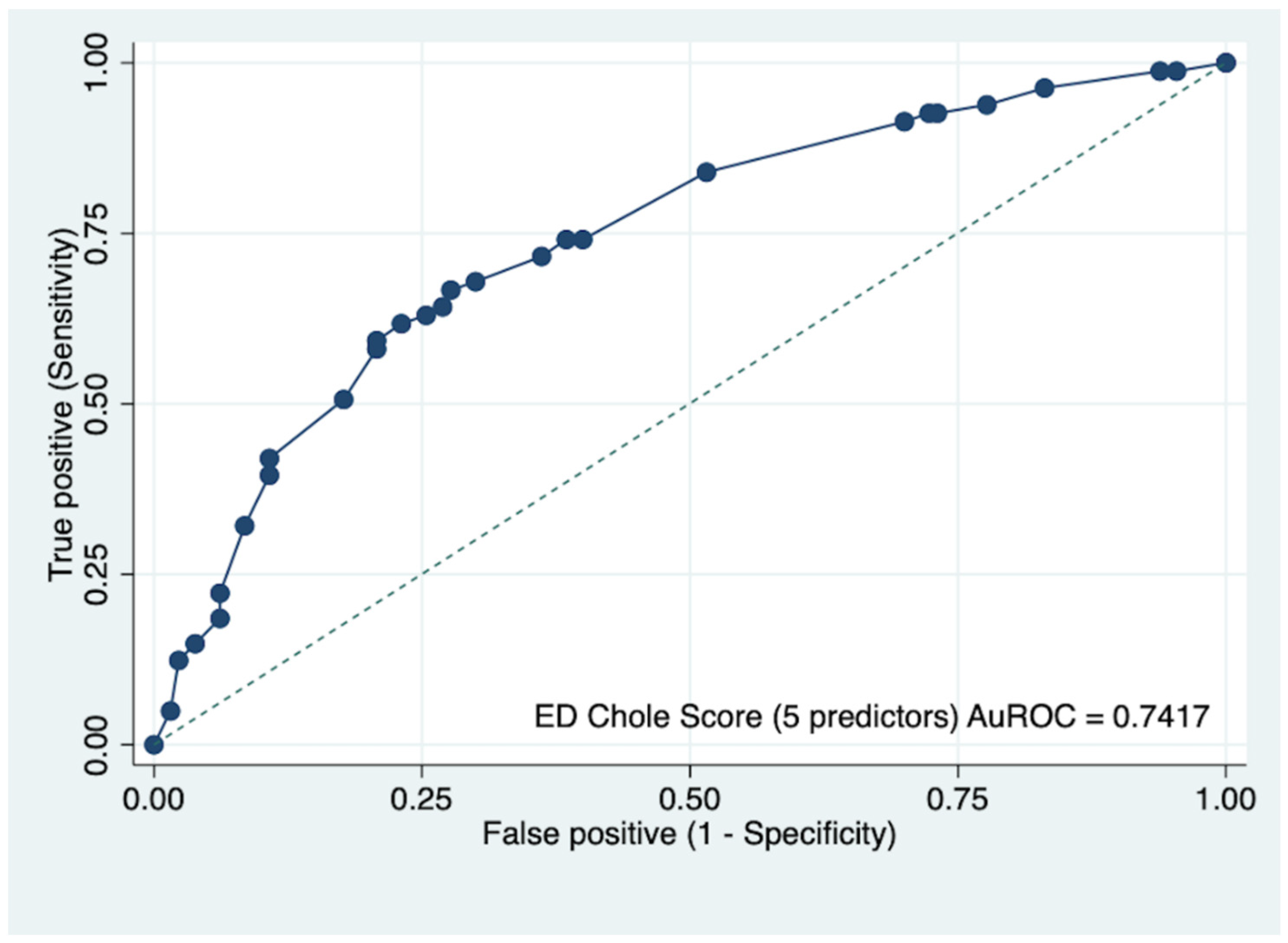
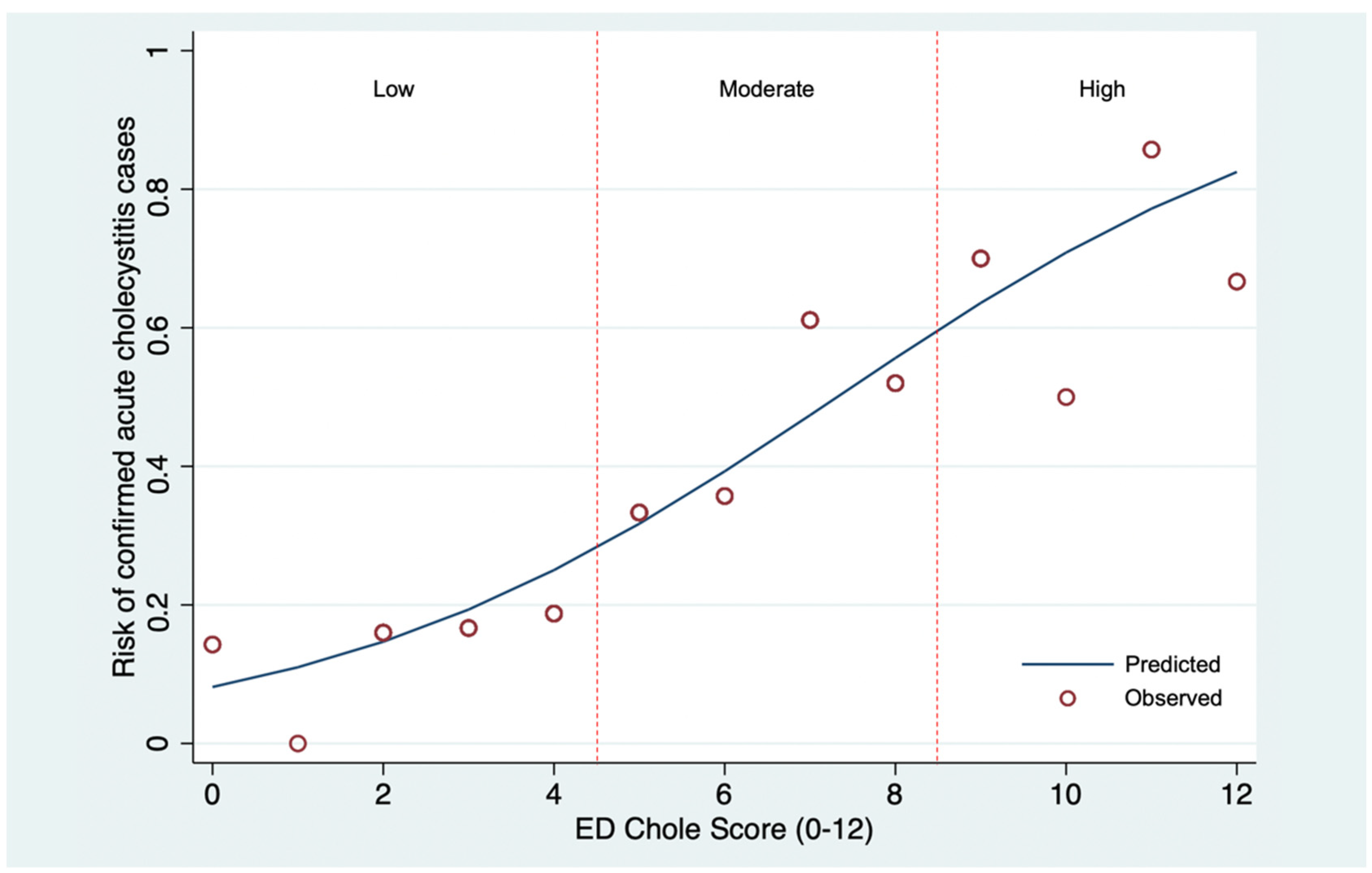
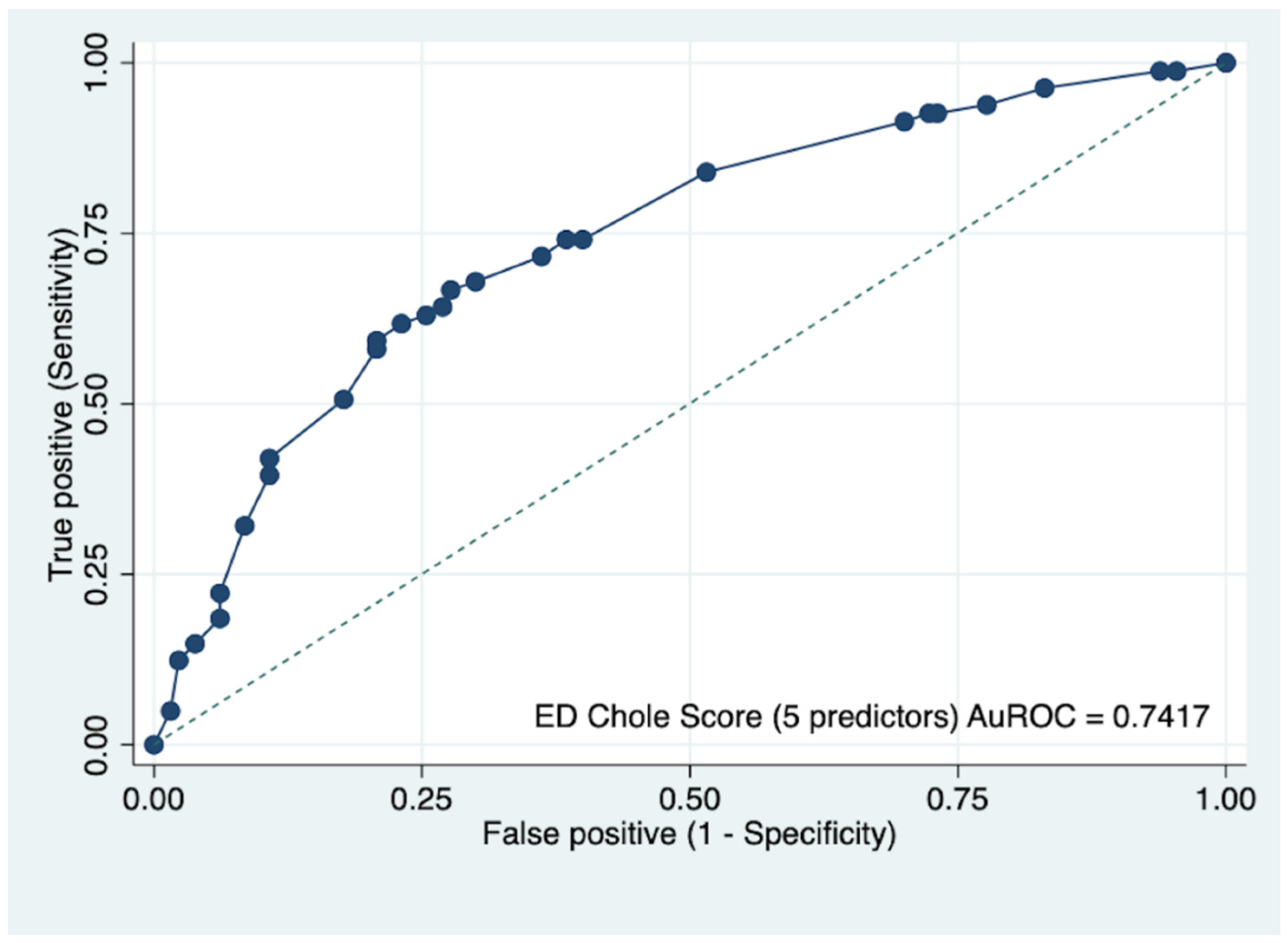
3.2. Model Development and Validation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jain, A.; Mehta, N.; Secko, M.; Schechter, J.; Papanagnou, D.; Pandya, S.; Sinert, R. History, Physical Examination, Laboratory Testing, and Emergency Department Ultrasonography for the Diagnosis of Acute Cholecystitis. Acad. Emerg. Med. 2017, 24, 281–297. [Google Scholar] [CrossRef] [PubMed]
- Yeh, D.D.; Chang, Y.; Tabrizi, M.B.; Yu, L.; Cropano, C.; Fagenholz, P.; King, D.R.; Kaafarani, H.M.A.; de Moya, M.; Velmahos, G. Derivation and Validation of a Practical Bedside Score for the Diagnosis of Cholecystitis. Am. J. Emerg. Med. 2019, 37, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Hiatt, K.D.; Ou, J.J.; Childs, D.D. Role of Ultrasound and CT in the Workup of Right Upper Quadrant Pain in Adults in the Emergency Department: A Retrospective Review of More Than 2800 Cases. Am. J. Roentgenol. 2020, 214, 1305–1310. [Google Scholar] [CrossRef] [PubMed]
- Marasco, G.; Verardi, F.M.; Eusebi, L.H.; Guarino, S.; Romiti, A.; Vestito, A.; Bazzoli, F.; Cavazza, M.; Zagari, R.M. Diagnostic Imaging for Acute Abdominal Pain in an Emergency Department in Italy. Intern. Emerg. Med. 2019, 14, 1147–1153. [Google Scholar] [CrossRef]
- Takada, T.; Kawarada, Y.; Nimura, Y.; Yoshida, M.; Mayumi, T.; Sekimoto, M.; Miura, F.; Wada, K.; Hirota, M.; Yamashita, Y.; et al. Background: Tokyo Guidelines for the Management of Acute Cholangitis and Cholecystitis. J. Hepato-Biliary-Pancreat. Surg. 2007, 14, 1–10. [Google Scholar] [CrossRef]
- Yokoe, M.; Takada, T.; Strasberg, S.M.; Solomkin, J.S.; Mayumi, T.; Gomi, H.; Pitt, H.A.; Garden, O.J.; Kiriyama, S.; Hata, J.; et al. TG13 Diagnostic Criteria and Severity Grading of Acute Cholecystitis (with Videos). J. Hepato-Biliary-Pancreat. Sci. 2013, 20, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Yokoe, M.; Hata, J.; Takada, T.; Strasberg, S.M.; Asbun, H.J.; Wakabayashi, G.; Kozaka, K.; Endo, I.; Deziel, D.J.; Miura, F.; et al. Tokyo Guidelines 2018: Diagnostic Criteria and Severity Grading of Acute Cholecystitis (with Videos). J. Hepato-Biliary-Pancreat. Sci. 2018, 25, 41–54. [Google Scholar] [CrossRef]
- Parker, L.J.; Vukov, L.F.; Wollan, P.C. Emergency Department Evaluation of Geriatric Patients with Acute Cholecystitis. Acad. Emerg. Med. 1997, 4, 51–55. [Google Scholar] [CrossRef]
- MacDonald, A.; Harman, R. Bedside Ultrasonography by Surgeons: A New Diagnostic Adjunct for Cholecystitis and Gallstone Disease. ANZ J. Surg. 2019, 89, 460–461. [Google Scholar] [CrossRef]
- Tourghabe, J.T.; Arabikhan, H.R.; Alamdaran, A.; Moghadam, H.Z. Emergency Medicine Resident versus Radiologist in Detecting the Ultrasonographic Signs of Acute Cholecystitis; a Diagnostic Accuracy Study. Emergency 2018, 6, e19. [Google Scholar]
- Takada, T.; Strasberg, S.M.; Solomkin, J.S.; Pitt, H.A.; Gomi, H.; Yoshida, M.; Mayumi, T.; Miura, F.; Gouma, D.J.; Garden, O.J.; et al. TG13: Updated Tokyo Guidelines for the Management of Acute Cholangitis and Cholecystitis. J. Hepato-Biliary-Pancreat. Sci. 2013, 20, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G.M. Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD): The Tripod Statement. J. Clin. Epidemiol. 2015, 68, 112–121. [Google Scholar] [CrossRef] [PubMed]
- Facciorusso, A.; di Maso, M.; Serviddio, G.; Vendemiale, G.; Spada, C.; Costamagna, G.; Muscatiello, N. Factors Associated with Recurrence of Advanced Colorectal Adenoma after Endoscopic Resection. Clin. Gastroenterol. Hepatol. 2016, 14, 1148–1154.e4. [Google Scholar] [CrossRef] [PubMed]
- Moons, K.G.M.; Altman, D.G.; Reitsma, J.B.; Ioannidis, J.P.A.; Macaskill, P.; Steyerberg, E.W.; Vickers, A.J.; Ransohoff, D.F.; Collins, G.S. Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD): Explanation and Elaboration. Ann. Intern. Med. 2015, 162, W1–W73. [Google Scholar] [CrossRef]
- Gomes, C.A.; Junior, C.S.; Di Saveiro, S.; Sartelli, M.; Kelly, M.D.; Gomes, C.C.; Gomes, F.C.; Correa, L.D.; Alves, C.B.; de Fádel Guimarães, S. Acute Calculous Cholecystitis: Review of Current Best Practices. World J. Gastrointest. Surg. 2017, 9, 118. [Google Scholar] [CrossRef]
- Hosmer, D.W.; Lemeshow, S.; Sturdivant, R.X. Applied Logistic Regression; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2013; ISBN 9780470582473. [Google Scholar]
- Hirota, M.; Takada, T.; Kawarada, Y.; Nimura, Y.; Miura, F.; Hirata, K.; Mayumi, T.; Yoshida, M.; Strasberg, S.; Pitt, H.; et al. Diagnostic Criteria and Severity Assessment of Acute Cholecystitis: Tokyo Guidelines. J. Hepato-Biliary-Pancreat. Surg. 2007, 14, 78–82. [Google Scholar] [CrossRef]
- Cho, J.Y.; Han, H.S.; Yoon, Y.S.; Ahn, K.S. Risk Factors for Acute Cholecystitis and a Complicated Clinical Course in Patients with Symptomatic Cholelithiasis. Arch. Surg. 2010, 145, 329–333. [Google Scholar] [CrossRef]
- Feldman, I.; Feldman, L.; Shapiro, D.S.; Munter, G.; Yinnon, A.M.; Friedman, R. Characteristics and Outcome of Elderly Patients Admitted for Acute Cholecystitis to Medical or Surgical Wards. Isr. J. Health Policy Res. 2020, 9, 23. [Google Scholar] [CrossRef]
- Kaye, A.D.; Baluch, A.; Scott, J.T. Pain Management in the Elderly Population: A Review. Ochsner J. 2010, 10, 179–187. [Google Scholar]
- Singer, A.J.; McCracken, G.; Henry, M.C.; Thode, J.; Cabahug, C.J. Correlation among Clinical, Laboratory, and Hepatobiliary Scanning Findings in Patients with Suspected Acute Cholecystitis. Ann. Emerg. Med. 1996, 28, 267–272. [Google Scholar] [CrossRef]
- Look, N.; Acute, S.D. Color Velocity Imaging and Power Doppler Sonography of the GallbladderWall: A New Look at Sonographic Diagnosisof Acute ChoIecystitis. Am. J. Roentgenol. 1998, 171, 183–188. [Google Scholar]
- Bree, R.L. Further Observations on the Usefulness of the Sonographic Murphy Sign in the Evaluation of Suspected Acute Cholecystitis. J. Clin. Ultrasound 1995, 23, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Serban, D.; Balasescu, S.; Alius, C.; Balalau, C.; Sabau, A.; Badiu, C.; Socea, B.; Trotea, A.; Dascalu, A.; Motofei, I.; et al. Clinical and Therapeutic Features of Acute Cholecystitis in Diabetic Patients. Exp. Med. 2021, 22, 758. [Google Scholar] [CrossRef]
- King, N.K.K.; Siriwardana, H.P.P.; Siriwardena, A.K. Cholecystitis after Cholecystectomy. J. R. Soc. Med. 2002, 95, 138–139. [Google Scholar] [CrossRef] [PubMed]
- Romano, L.; Lazzarin, G.; Varrassi, M.; di Sibio, A.; Vicentini, V.; Schietroma, M.; Carlei, F.; Giuliani, A. Haemobilia Secondary to a Cystic Artery Pseudoaneurysm as Complication of VLC. Acta Biomed. 2021, 92, e2021125. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.P.; Sanders, T.K.; Prakash, P.; Law, J.; Alvencar, S.; Choi, A.; Shah, J.; Patel, K.; Srivoleti, P.; Chauhan, K.; et al. Gastrointestinal Manifestations of Coronavirus Disease 2019 across the United States: A Multi-Center Cohort Study. Gastro Hep Adv. 2022, 1, 909–915. [Google Scholar] [CrossRef] [PubMed]
- Hwaiz, R.; Merza, M.; Hamad, B.; HamaSalih, S.; Mohammed, M.; Hama, H. Evaluation of Hepatic Enzymes Activities in COVID-19 Patients. Int. Immunopharmacol. 2021, 97, 107701. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Variables | Missing Data, n (%) | Confirmed Cases, n (%) (n = 86) | Non-Cases, n (%) (n = 158) | Crude OR (95% CI) | p-Value | AuROC (95% CI) |
|---|---|---|---|---|---|---|
| Demographic data | ||||||
| Male | 0 (0) | 48 (55.8) | 88 (55.7) | 1.00 (0.59–1.71) | 0.99 | 50.06 (43.51–56.61) |
| Age, years (mean ± SD) | 0 (0) | 47.9 ± 15.9 | 53.4 ± 19.2 | 0.98 (0.97–1.00) | 0.03 | 42.10 (34.86–49.35) |
| Age < 60 years old | 67 (77.9) | 101 (63.9) | 1.99 (1.09–3.64) | 0.03 | 56.99 (51.20–62.78) | |
| Clinical characteristics | ||||||
| Fever | 0 (0) | 14 (16.3) | 41 (26.0) | 0.55 (0.28–1.09) | 0.09 | 45.16 (39.95–50.38) |
| Nausea/vomiting | 0 (0) | 44 (51.2) | 48 (30.4) | 2.40 (1.40–4.13) | 0.002 | 60.39 (53.98–66.81) |
| Jaundice | 0 (0) | 13 (51.1) | 20 (12.7) | 1.23 (0.58–2.61) | 0.59 | 51.23 (46.62–55.84) |
| RUQ pain | 0 (0) | 70 (81.4) | 107 (67.7) | 2.09 (1.10–3.94) | 0.02 | 56.84 (51.32–62.36) |
| Physical examinations | ||||||
| Body temperature, °C (mean ± SD) | 29 (11.9) | 36.9 ± 0.9 | 37.1 ± 1.0 | 0.80 (0.60–1.08) | 0.14 | 43.96 (37.98–49.94) |
| <36 °C | 9 (37.5) | 15 (62.5) | 0.95 (0.39–2.31) | 0.91 | ||
| 36–38 °C | 60 (38.7) | 95 (61.3) | Ref | Ref | ||
| >38 °C | 7 (19.4) | 29 (80.6) | 0.38 (0.16–0.93) | 0.03 | ||
| Pulse rate, per mins (mean ± SD) | 7 (2.9) | 85.9 ± 21.0 | 89.3 ± 18.7 | 0.99 (0.98–1.00) | 0.20 | 48.71 (42.78–54.64) |
| >60 bpm | 6 (54.6) | 5 (45.5) | 2.18 (0.64–7.45) | 0.21 | ||
| 60–100 bpm | 61 (35.5) | 111 (64.5) | Ref | Ref | ||
| >100 bpm | 16 (29.6) | 38 (70.4) | 0.77 (0.40–1.49) | 0.43 | ||
| SBP, mmHg (mean ± SD) | 8 (3.3) | 128.7 ± 25.4 | 131.6 ± 23.8 | 1.00 (0.98–1.01) | 0.38 | 52.36 (49.26–55.46) |
| ≥90 mmHg | 76 (33.6) | 150 (66.4) | Ref | Ref | ||
| <90 mmHg | 6 (60.0) | 4 (40.0) | 2.96 (0.81–10.81) | 0.10 | ||
| DBP, mmHg (mean ± SD) | 8 (3.3) | 77.1 ± 18.5 | 78.5 ± 16.7 | 1.00 (0.98–1.01) | 0.54 | 53.34 (48.59–58.10) |
| ≥60 mmHg | 68 (82.9) | 138 (89.6) | Ref | Ref | ||
| <60 mmHg | 14 (17.1) | 16 (10.4) | 1.78 (0.82–3.85) | 0.15 | ||
| Respiratory rate, per mins (mean ± SD) | 23 (9.4) | 20.7 ± 4.4 | 20.3 ± 4.6 | 1.02 (0.96–1.08) | 0.53 | 49.17 (46.30–52.04) |
| <30 per mins | 74 (96.1) | 136 (94.4) | Ref | Ref | ||
| ≥30 per mins | 3 (3.9) | 8 (5.6) | 0.69 (0.18–2.68) | 0.59 | ||
| Rebound tenderness at RUQ | 0 (0) | 7 (8.1) | 7 (4.4) | 1.91 (0.65–5.64) | 0.24 | 51.85 (48.53–55.18) |
| Positive Murphy’s sign | 0 (0) | 38 (44.2) | 57 (36.1) | 1.40 (0.82–2.40) | 0.22 | 54.06 (47.58–60.53) |
| Laboratory findings | ||||||
| WBC/μL (median, IQR) | 13 (5.3) | 11,021 (8,000–15,560) | 11,170 (8,180–14,025) | 1.00 (1.00–1.00) | 0.28 | 51.61 (44.90–58.32) |
| <12,000/μ | 45 (54.2) | 85 (57.4) | Ref | Ref | ||
| ≥12,000/μ | 38 (45.8) | 63 (42.3) | 1.14 (0.66–1.96) | 0.64 | ||
| Neutrophil, % (mean ± SD) | 13 (5.3) | 75.2 ± 13.2 | 72.4 ± 14.7 | 1.01 (0.00–1.03) | 0.16 | 51.21 (44.67–57.75) |
| Neutrophil count ≥ 80% | 38 (44.2) | 66 (41.8) | 1.10 (0.65–1.88) | 0.72 | ||
| Absolute neutrophil count/μL (median, IQR) | 13 (5.3) | 8,257.4 (1,055.7–22,070.1) | 7,831.7 (4,477.9–10,795.7) | 1.00 (1.00–1.00) | 0.11 | 55.20 (47.62–62.78) |
| Platelet/μL (median, IQR) | 15 (6.1) | 242,000 (192,000–297,000) | 245,000 (192,000–313,000) | 1.00 (1.00–1.00) | 0.37 | 47.62 (39.93–55.33) |
| AST (median, IQR) | 33 (13.5) | 58 (21–136) | 28 (19–64) | 1.00 (1.00–1.01) | 0.003 | 64.84 (58.43–71.26) |
| <2xULN | 42 (51.9) | 106 (81.5) | Ref | Ref | ||
| ≥2xULN | 39 (48.2) | 24 (18.5) | 4.10 (2.20–7.64) | <0.001 | ||
| ALT (median, IQR) | 32 (13.1) | 38 (21–141) | 27 (17–53) | 1.00 (1.00–1.01) | 0.004 | 57.51 (51.36–63.65) |
| <2xULN | 54 (66.7) | 107 (81.7) | Ref | Ref | ||
| ≥2xULN | 27 (33.3) | 24 (18.3) | 2.23 (1.18–4.23) | 0.01 | ||
| Alkaline phosphatase (median, IQR) | 36 (14.8) | 98 (70–169) | 92 (67–148) | 1.00 (1.00–1.00) | 0.39 | 49.93 (44.38–55.49) |
| <2xULN | 61 (81.3) | 108 (81.2) | Ref | Ref | ||
| ≥2xULN | 14 (18.7) | 25 (18.8) | 0.99 (0.48–2.05) | 0.98 | ||
| Total bilirubin (median, IQR) | 31 (12.7) | 1.02 (0.55–2.48) | 0.68 (0.40–1.42) | 1.02 (0.95–1.10) | 0.54 | 57.01 (50.74–63.28) |
| <2 mg/dL | 52 (65.8) | 107 (79.9) | Ref | Ref | ||
| ≥2 mg/dL | 27 (34.2) | 27 (20.2) | 2.06 (1.10–3.86) | 0.02 | ||
| Direct bilirubin (median, IQR) | 30 (12.3) | 0.47 (0.20-.1.22) | 0.24 (0.16–0.64) | 1.03 (0.91–1.17) | 0.63 | 53.16 (47.73–58.60) |
| <1.5 mg/dL | 63 (78.8) | 114 (85.1) | Ref | Ref | ||
| ≥1.5 mg/dL | 17 (21.2) | 20 (14.9) | 1.54 (0.75–3.15) | 0.24 |
| Variables | Full Model mOR | 95% CI | p-Value | Reduced Model mOR | 95% CI | p-Value |
|---|---|---|---|---|---|---|
| Demographic data | ||||||
| Male | 0.87 | 0.39–1.95 | 0.74 | |||
| Age, years | 0.97 | 0.94–1.01 | 0.14 | |||
| Age < 60 years old | 0.78 | 0.18–3.40 | 0.74 | 2.02 | 1.00–4.06 | 0.05 |
| Clinical characteristics | ||||||
| Fever | 0.77 | 0.24–2.50 | 0.66 | |||
| Nausea/vomiting | 1.49 | 0.66–3.37 | 0.34 | 2.66 | 1.42–4.99 | 0.002 |
| Jaundice | 0.76 | 0.16–3.66 | 0.73 | |||
| RUQ pain | 1.17 | 0.42–3.21 | 0.77 | 1.85 | 0.84–4.05 | 0.13 |
| Physical examinations | ||||||
| Body temperature, °C | 0.81 | 0.48–1.36 | 0.43 | |||
| Pulse rate, per mins | 0.98 | 0.96–1.01 | 0.22 | |||
| SBP, mmHg | 0.99 | 0.97–1.01 | 0.38 | |||
| DBP, mmHg | 1.00 | 0.98–1.03 | 0.83 | |||
| Respiratory rate, per mins | 1.04 | 0.93–1.15 | 0.50 | |||
| Rebound tenderness at RUQ | 0.76 | 0.15–3.88 | 0.75 | |||
| Positive Murphy’s sign | 1.49 | 0.62–3.58 | 0.37 | 1.12 | 0.58–2.14 | 0.74 |
| Laboratory findings | ||||||
| WBC/μL | 1.00 | 1.00–1.00 | 0.92 | |||
| Neutrophil, % | 1.04 | 0.97–1.11 | 0.26 | |||
| Absolute neutrophil count/μL | 1.00 | 1.00–1.00 | 0.73 | |||
| Platelet/μL | 1.00 | 1.00–1.00 | 0.34 | |||
| AST | 1.00 | 1.00–1.00 | 0.83 | |||
| AST ≥ 2xULN | 8.28 | 3.20–31.14 | 0.002 | 4.21 | 2.19–8.08 | <0.001 |
| ALT ≥ 2xULN | 0.84 | 0.23–3.10 | 0.79 | |||
| Alkaline phosphatase | 1.00 | 1.00–1.00 | 0.10 | |||
| Total bilirubin | 0.95 | 0.67–1.34 | 0.77 | |||
| Direct bilirubin | 1.03 | 0.58–1.83 | 0.92 | |||
| Constant (intercept) | 3715.24 | 0.09 |
| Predictors | mOR | 95% CI | p-Value | Score |
|---|---|---|---|---|
| Age < 60 years old | 2.02 | 1.00–4.06 | 0.05 | 2 |
| Nausea/vomiting | 2.66 | 1.42–4.99 | 0.002 | 3 |
| RUQ pain | 1.85 | 0.84–4.05 | 0.13 | 2 |
| Positive Murphy’s sign | 1.12 | 0.58–2.14 | 0.74 | 1 |
| AST ≥ 2xULN | 4.21 | 2.19–8.08 | <0.001 | 4 |
| Constant | 0.09 |
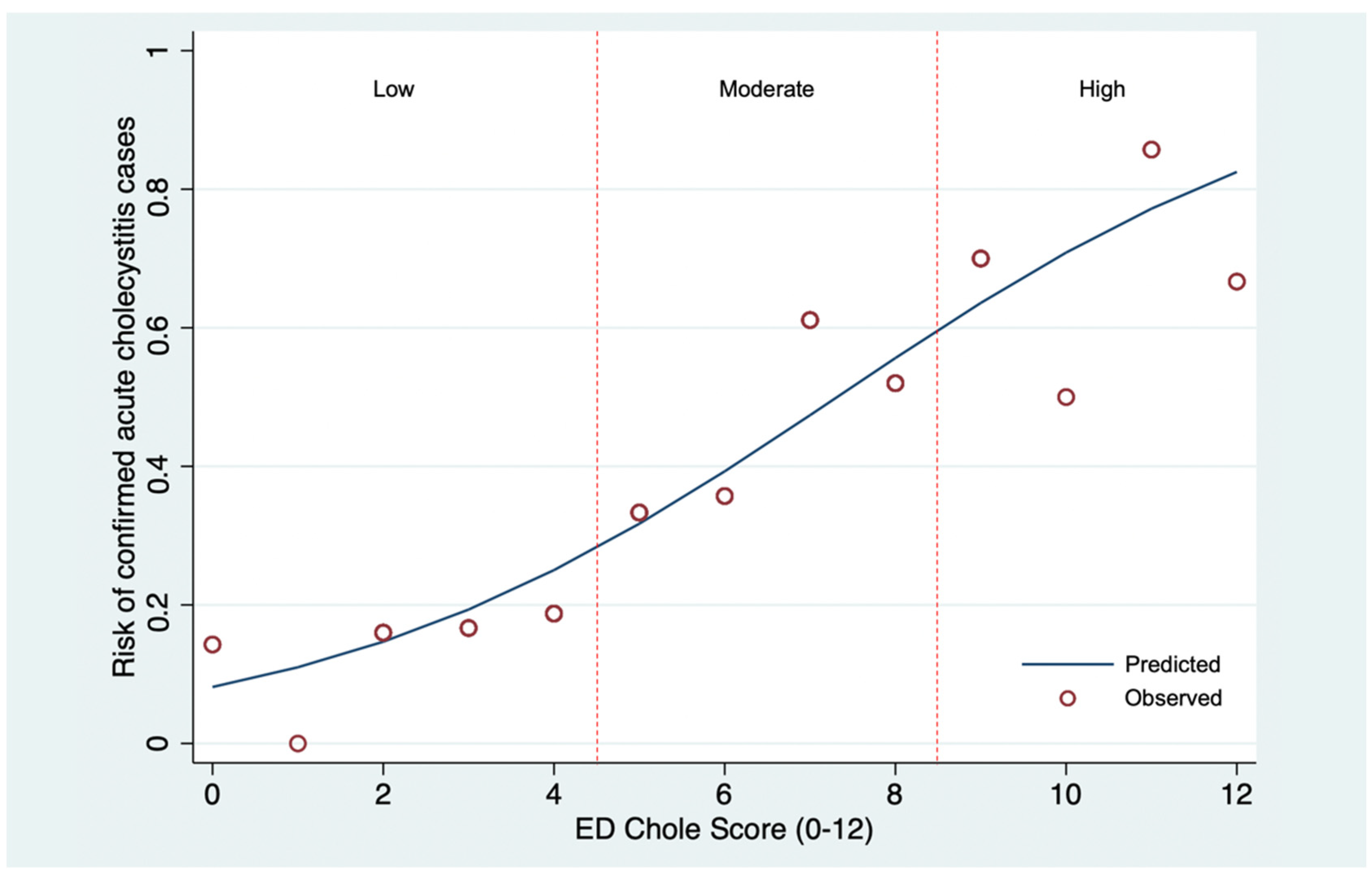
| Probable Categories | Score | Confirmed Cases, n (%) (n = 81) | Non-Cases, n (%) (n = 130) | LHR+ | (95% CI) | p-Value |
|---|---|---|---|---|---|---|
| ED Chole Score | ||||||
| Low | 0–4 | 13 (16.0) | 65 (50.0) | 0.32 | 0.15–0.64 | <0.001 |
| Moderate | 5–8 | 42 (51.9) | 54 (41.5) | 1.25 | 0.74–2.09 | 0.37 |
| High | 9–12 | 26 (32.1) | 11 (8.5) | 3.79 | 1.69–8.94 | <0.001 |
| Mean ± SD | 7.1 ± 2.7 | 4.7 ± 2.6 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faikhongngoen, S.; Chenthanakij, B.; Wittayachamnankul, B.; Phinyo, P.; Wongtanasarasin, W. Developing a Simple Score for Diagnosis of Acute Cholecystitis at the Emergency Department. Diagnostics 2022, 12, 2246. https://doi.org/10.3390/diagnostics12092246
Faikhongngoen S, Chenthanakij B, Wittayachamnankul B, Phinyo P, Wongtanasarasin W. Developing a Simple Score for Diagnosis of Acute Cholecystitis at the Emergency Department. Diagnostics. 2022; 12(9):2246. https://doi.org/10.3390/diagnostics12092246
Chicago/Turabian StyleFaikhongngoen, Saowaluck, Boriboon Chenthanakij, Borwon Wittayachamnankul, Phichayut Phinyo, and Wachira Wongtanasarasin. 2022. "Developing a Simple Score for Diagnosis of Acute Cholecystitis at the Emergency Department" Diagnostics 12, no. 9: 2246. https://doi.org/10.3390/diagnostics12092246
APA StyleFaikhongngoen, S., Chenthanakij, B., Wittayachamnankul, B., Phinyo, P., & Wongtanasarasin, W. (2022). Developing a Simple Score for Diagnosis of Acute Cholecystitis at the Emergency Department. Diagnostics, 12(9), 2246. https://doi.org/10.3390/diagnostics12092246